Comparison of the Efficacy and Safety of Trabeculectomy with Mitomycin C According to Concentration: A Prospective Randomized Clinical Trial

 ,
, 
Abstract
:1. Introduction
2. Experimental Section
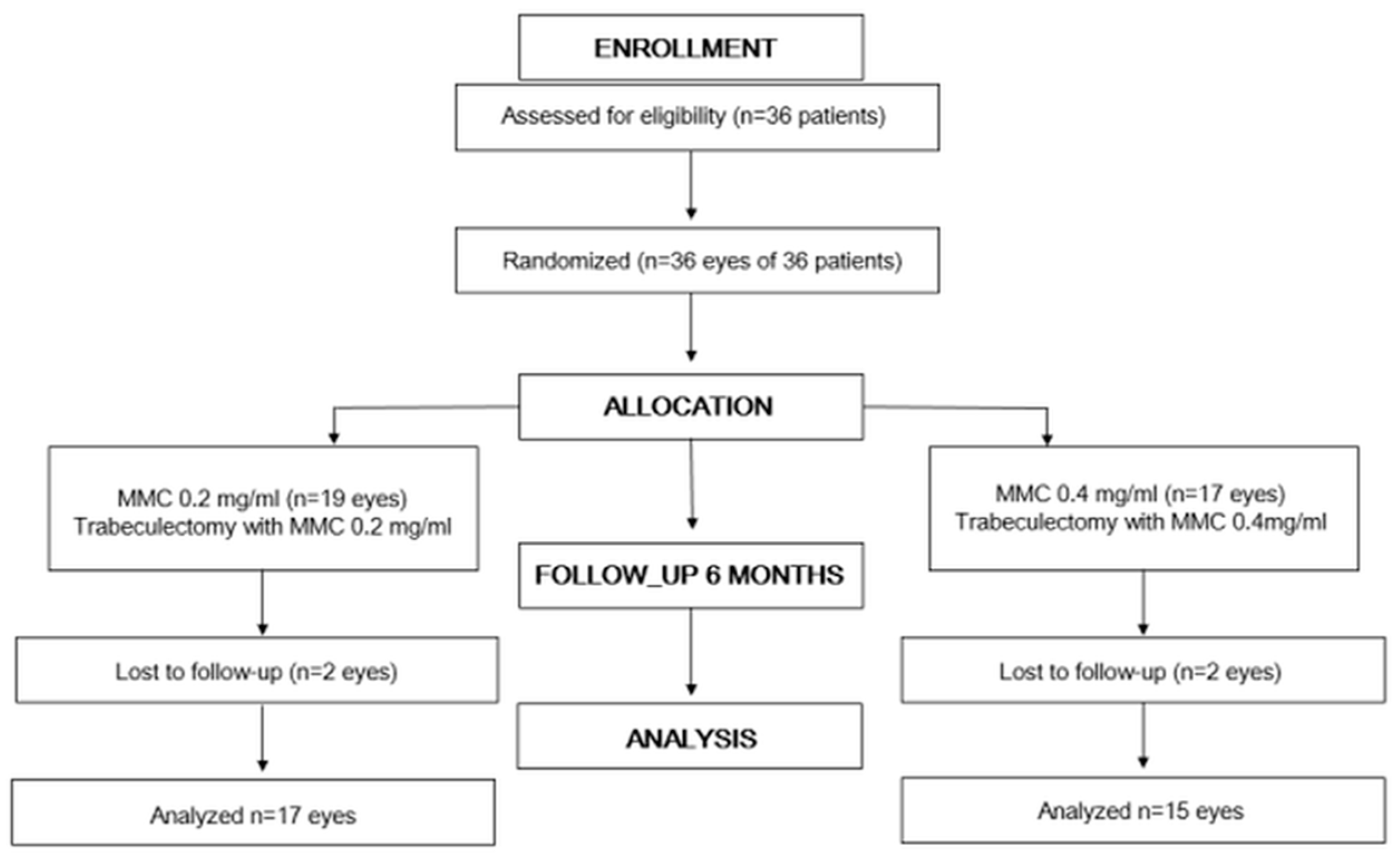
2.1. Study Design
2.2. Subjects
2.3. Preoperative Assessment
2.4. Randomization
2.5. Surgical Procedure
2.6. Postoperative Assessment
2.7. Experimental Procedures
2.8. Outcome Evaluations
2.9. Statistics
2.10. Sample Size
3. Results
3.1. Subjects
3.2. Changes of Intraocular Pressure and Number of Glaucoma Medications
3.3. Success Rates and the Predictive Factors for Surgical Failure
3.4. Bleb Morphology
3.5. Complications and Additional Procedures
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Addicks, E.M.; Quigley, H.A.; Green, W.R.; Robin, A.L. Histologic characteristics of filtering blebs in glaucomatous eyes. Arch. Ophthalmol. 1983, 101, 795–798. [Google Scholar] [CrossRef]
- Van Buskirk, E.M. Cysts of Tenon’s capsule following filtration surgery. Am. J. Ophthalmol. 1982, 94, 522–527. [Google Scholar] [CrossRef]
- Costa, V.P.; Moster, M.R.; Wilson, R.P.; Schmidt, C.M.; Gandham, S.; Smith, M. Effects of topical mitomycin C on primary trabeculectomies and combined procedures. Br. J. Ophthalmol. 1993, 77, 693–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, V.P.; Spaeth, G.L.; Eiferman, R.A.; Orengo-Nania, S. Wound healing modulation in glaucoma filtration surgery. Ophthalmic. Surg. 1993, 24, 152–170. [Google Scholar] [PubMed]
- Wilkins, M.; Indar, A.; Wormald, R. Intra-operative mitomycin C for glaucoma surgery. Cochrane Database Syst. Rev. 2001, 2005, CD002897. [Google Scholar]
- Jampel, H.D.; Solus, J.F.; Tracey, P.A.; Gilbert, D.L.; Loyd, T.L.; Jefferys, J.L.; Quigley, H.A. Outcomes and bleb-related complications of trabeculectomy. Ophthalmology 2012, 119, 712–722. [Google Scholar] [CrossRef]
- Lee, S.J.; Paranhos, A.; Shields, M.B. Does titration of mitomycin C as an adjunct to trabeculectomy significantly influence the intraocular pressure outcome? Clin. Ophthalmol. 2009, 3, 81–87. [Google Scholar]
- Al Habash, A.; Aljasim, L.A.; Owaidhah, O.; Edward, D.P. A review of the efficacy of mitomycin C in glaucoma filtration surgery. Clin. Ophthalmol. 2015, 9, 1945–1951. [Google Scholar]
- Kim, Y.Y.; Sexton, R.M.; Shin, D.H.; Kim, C.; Ginde, S.A.; Ren, J.; Lee, D.; Kupin, T.H. Outcomes of primary phakic trabeculectomies without versus with 0.5- to 1-minute versus 3- to 5-minute mitomycin C. Am. J. Ophthalmol. 1998, 126, 755–762. [Google Scholar] [CrossRef]
- Robin, A.L.; Ramakrishnan, R.; Krishnadas, R.; Smith, S.D.; Katz, J.D.; Selvaraj, S.; Skuta, G.L.; Bhantnagar, R. A long-term dose-response study of mitomycin in glaucoma filtration surgery. Arch. Ophthalmol. 1997, 115, 969–974. [Google Scholar] [CrossRef]
- Sihota, R.; Angmo, D.; Chandra, A.; Gupta, V.; Sharma, A.; Pandey, R.M. Evaluating the long-term efficacy of short-duration 0.1 mg/ml and 0.2 mg/ml MMC in primary trabeculectomy for primary adult glaucoma. Graefes Arch. Clin. Exp. Ophthalmol. 2015, 253, 1153–1159. [Google Scholar] [CrossRef] [PubMed]
- Maquet, J.A.; Dios, E.; Aragón, J.; Bailez, C.; Ussa, F.; Laguna, N. Protocol for mitomycin C use in glaucoma surgery. Acta Ophthalmol. Scand. 2005, 83, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Park, K.H.; Youn, D.H. The effect of low-and high-dose adjunctive mitomycin C in trabeculectomy. Korean J. Ophthalmol. 1996, 10, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Sanders, S.P.; Cantor, L.B.; Dobler, A.A.; Hoop, J.S. Mitomycin C in higher risk trabeculectomy: A prospective comparison of 0.2- to 0.4-mg/cc doses. J. Glaucoma. 1999, 8, 193–198. [Google Scholar] [CrossRef]
- Jampel, H.D.; McGuigan, L.J.; Dunkelberger, G.R.; L’Hernault, N.L.; Quigley, H.A. Cellular proliferation after experimental glaucoma filtration surgery. Arch. Ophthalmol. 1988, 106, 89–94. [Google Scholar] [CrossRef]
- Kawashima, Y.; Saika, S.; Yamanaka, O.; Okada, Y.; Ohkawa, K.; Ohnishi, Y. Immunolocalization of matrix metalloproteinases and tissue inhibitors of metalloproteinases in human subconjunctival tissues. Curr. Eye Res. 1998, 17, 445–451. [Google Scholar] [CrossRef]
- Mathalone, N.; Marmor, S.; Rahat, M.A.; Lahat, N.; Oron, Y.; Geyer, O. MMP expression in leaking filtering blebs and tears after glaucoma filtering surgery. Graefes Arch. Clin. Exp. Ophthalmol. 2011, 249, 1047–1055. [Google Scholar] [CrossRef]
- Seo, J.H.; Park, K.H.; Kim, Y.J.; Yoo, Y.C.; Kang, S.H.; Kim, D.M. Differences in the histopathology and matrix metalloproteinase expression in Tenon’s tissue of primary open-angle glaucoma and primary angle-closure glaucoma. Korean J. Ophthalmol. 2008, 22, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Automated Static Perimetry, 2nd ed.; Mosby: St. Louis, MO, USA, 1999.
- Wells, A.P.; Crowston, J.G.; Marks, J.; Kirwan, J.F.; Smith, G.; Clarke, J.C.K.; Shah, R.; Vieira, J.; Bunce, C.; Murdoch, I.; et al. A pilot study of a system for grading of drainage blebs after glaucoma surgery. J. Glaucoma 2004, 13, 454–460. [Google Scholar] [CrossRef]
- Johnstone, M.A. Hypotony: What is it? How should we manage it? J. Glaucoma 2000, 9, 131–133. [Google Scholar] [CrossRef]
- Fine, H.F.; Biscette, O.; Chang, S.; Schiff, W.M. Ocular hypotony: A review. Compr. Ophthalmol. Update 2007, 8, 29–37. [Google Scholar] [PubMed]
- Akkan, J.U.; Cilsim, S. Role of subconjunctival bevacizumab as an adjuvant to primary trabeculectomy: A prospective randomized comparative 1-year follow-up study. J. Glaucoma 2015, 24, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fontana, H.; Nouri-Mahdavi, K.; Caprioli, J. Trabeculectomy with mitomycin C in pseudophakic patients with open-angle glaucoma: Outcomes and risk factors for failure. Am. J. Ophthalmol. 2006, 141, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Fontana, H.; Nouri-Mahdavi, K.; Lumba, J.; Ralli, M.; Caprioli, J. Trabeculectomy with mitomycin C: Outcomes and risk factors for failure in phakic open-angle glaucoma. Ophthalmology 2006, 113, 930–936. [Google Scholar] [CrossRef]
- Mietz, H.; Krieglstein, G.K. Three-year follow-up of trabeculectomies performed with different concentrations of mitomycin-C. Ophthalmic Surg. Lasers 1998, 29, 628–634. [Google Scholar]
- Kitazawa, Y.; Suemori-Matsushita, H.; Yamamoto, T.; Kawase, K. Low-dose and high-dose mitomycin trabeculectomy as an initial surgery in primary open-angle glaucoma. Ophthalmology 1993, 100, 1624–1628. [Google Scholar] [CrossRef]
- Watson, P.G.; Grierson, I. The place of trabeculectomy in the treatment of glaucoma. Ophthalmology 1981, 88, 175–196. [Google Scholar] [CrossRef]
- Lochhead, J.; Casson, R.J.; Salmon, J.F. Long term effect on intraocular pressure of phacotrabeculectomy compared to trabeculectomy. Br. J. Ophthalmol. 2003, 87, 850–852. [Google Scholar] [CrossRef]
- Helin-Toiviainen, M.; Ronkko, S.; Puustjarvi, T.; Rekonen, P.; Ollikainen, M.; Uusitalo, H. Conjunctival matrix metalloproteinases and their inhibitors in glaucoma patients. Acta Ophthalmol. 2015, 93, 165–171. [Google Scholar] [CrossRef] [Green Version]
- Terai, N.; Schlotzer-Schrehardt, U.; Lampel, J.; Bohm, A.G.; Rummelt, C.; Schmidt, E.; Pillunat, L.E. Effect of latanoprost and timolol on the histopathology of the human conjunctiva. Br. J. Ophthalmol. 2009, 93, 219–224. [Google Scholar] [CrossRef] [Green Version]
- Soltau, J.B.; Rothman, R.F.; Budenz, D.L.; Greenfield, D.S.; Feuer, W.; Liebmann, J.M.; Ritch, R. Risk factors for glaucoma filtering bleb infections. Arch. Ophthalmol. 2000, 118, 338–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeBry, P.W.; Perkins, T.W.; Heatley, G.; Kaufman, P.; Brumback, L.C. Incidence of late-onset bleb-related complications following trabeculectomy with mitomycin. Arch. Ophthalmol. 2002, 120, 297–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bashford, K.P.; Shafranov, G.; Shields, M.B. Bleb revision for hypotony maculopathy after trabeculectomy. J. Glaucoma 2004, 13, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Broadway, D.C.; Bloom, P.A.; Bunce, C.; Thiagarajan, M.; Khaw, P.T. Needle revision of failing and failed trabeculectomy blebs with adjunctive 5-fluorouracil: Survival analysis. Ophthalmology 2004, 111, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Ciancaglini, M.; Carpineto, P.; Agnifili, L.; Nubile, M.; Lanzini, M.; Fasanella, V.; Mastropasqua, L. Filtering bleb functionality: A clinical, anterior segment optical coherence tomography and in vivo confocal microscopy study. J. Glaucoma 2008, 17, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Tominaga, A.; Miki, A.; Yamazaki, Y.; Matsushita, K.; Otori, Y. The assessment of the filtering bleb function with anterior segment optical coherence tomography. J. Glaucoma 2010, 19, 551–555. [Google Scholar] [CrossRef]
- Singh, M.; Chew, P.T.; Friedman, D.S.; Nolan, W.P.; See, J.L.; Smith, S.D.; Zheng, C.; Foster, P.J.; Aung, T. Imaging of trabeculectomy blebs using anterior segment optical coherence tomography. Ophthalmology 2007, 114, 47–53. [Google Scholar] [CrossRef]
- Narita, A.; Morizane, Y.; Miyake, T.; Seguchi, J.; Baba, T.; Shiraga, F. Characteristics of successful filtering blebs at 1 year after trabeculectomy using swept-source three-dimensional anterior segment optical coherence tomography. Jpn. J. Ophthalmol. 2017, 61, 253–259. [Google Scholar] [CrossRef]
- Skuta, G.L.; Beeson, C.C.; Higginbotham, E.J.; Lichter, P.R.; Musch, D.C.; Bergstrom, T.J.; Klein, T.B.; Falck, Y. Intraoperative mitomycin versus postoperative 5-fluorouracil in high-risk glaucoma filtering surgery. Ophthalmology 1992, 99, 438–444. [Google Scholar] [CrossRef]
- Stamper, R.L.; McMenemy, M.G.; Lieberman, M.F. Hypotonous maculopathy after trabeculectomy with subconjunctival 5-fluorouracil. Am. J. Ophthalmol. 1992, 114, 544–553. [Google Scholar] [CrossRef]
- Costa, V.P.; Wilson, R.P.; Moster, M.R.; Schmidt, C.M.; Gandham, S. Hypotony maculopathy following the use of topical mitomycin C in glaucoma filtration surgery. Ophthalmic Surg. 1993, 24, 389–394. [Google Scholar] [PubMed]
- Shields, M.B.; Scroggs, M.W.; Sloop, C.M.; Simmons, R.B. Clinical and histopathologic observations concerning hypotony after trabeculectomy with adjunctive mitomycin C. Am. J. Ophthalmol. 1993, 116, 673–683. [Google Scholar] [CrossRef]
- Zacharia, P.T.; Deppermann, S.R.; Schuman, J.S. Ocular hypotony after trabeculectomy with mitomycin C. Am. J. Ophthalmol. 1993, 116, 314–326. [Google Scholar] [CrossRef]
- Suner, I.J.; Greenfield, D.S.; Miller, M.P.; Nicolela, M.T.; Palmberg, P.F. Hypotony maculopathy after filtering surgery with mitomycin C. Incidence and treatment. Ophthalmology 1997, 104, 207–214. [Google Scholar] [CrossRef]
- Singh, K.; Mehta, K.; Shaikh, N.M.; Tsai, J.C.; Moster, M.R.; Budenz, D.L.; Greenfield, D.S.; Chen, P.P.; Cohen, J.S.; Baerveldt, G.S.; et al. Trabeculectomy with intraoperative mitomycin C versus 5-fluorouracil. Prospective randomized clinical trial. Ophthalmology 2000, 107, 2305–2309. [Google Scholar] [CrossRef]
- Bindlish, R.; Condon, G.P.; Schlosser, J.D.; D’Antonio, J.; Lauer, K.B.; Lehrer, R. Efficacy and safety of mitomycin-C in primary trabeculectomy: Five-year follow-up. Ophthalmology 2002, 109, 1336–1341. [Google Scholar] [CrossRef]
- Parrish, R.; Minckler, D. “Late endophthalmitis”—Filtering surgery time bomb? Ophthalmology 1996, 103, 1167–1168. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Total (n = 36) | Group 1 (MMC 0.2 mg/mL) (n = 19) | Group 2 (MMC 0.4 mg/mL) (n = 17) | |
|---|---|---|---|
| Age (years), mean ± SD | 58.79 ± 15.86 | 53.83 ± 15.29 | 64.33 ± 15.02 |
| Sex, n (%) | |||
| Male | 23 (63.9) | 10 (52.6) | 13 (76.5) |
| Female | 13 (36.1) | 9 (47.4) | 4 (23.5) |
| Diabetes, n (%) | 7 (19.4) | 5 (26.3) | 2 (11.8) |
| Systemic hypertension, n (%) | 15 (41.7) | 6 (31.6) | 9 (52.9) |
| Rheumatic disease, n (%) | 2 (5.6) | 1 (5.3) | 1 (5.9) |
| Surgeon, n (%) | |||
| K.H.P. | 20 (55.6) | 9 (47.4) | 11 (64.7) |
| J.W.J. | 5 (13.9) | 3 (15.8) | 2 (11.8) |
| Y.K.K. | 11 (30.6) | 7 (36.8) | 4 (23.5) |
| Type of glaucoma, n (%) | |||
| Primary open-angle glaucoma | 19 (52.8) | 11 (57.9) | 8 (47.1) |
| Primary angle-closure glaucoma | 4 (11.1) | 2 (10.5) | 2 (11.8) |
| Pseudo-exfoliation glaucoma | 4 (11.1) | 2 (10.5) | 2 (11.8) |
| Secondary glaucoma | 9 (25.0) | 4 (21.1) | 5 (29.4) |
| Previous laser history, n (%) | 7 (19.4) | 4 (21.1) | 3 (17.6) |
| Previous cataract operation history, n (%) | 7 (19.4) | 4 (21.1) | 3 (17.6) |
| Central corneal thickness (um), mean ± SD | 532.75 ± 42.34 | 529.22 ± 33.86 | 537.29 ± 52.32 |
| Axial length (mm), mean ± SD | 24.15 ± 1.77 | 23.98 ± 1.14 | 24.33 ± 2.30 |
| Preoperative BCVA, mean ± SD | 0.37 ± 0.37 | 0.38 ± 0.48 | 0.37 ± 0.21 |
| Preoperative IOP (mmHg), mean ± SD | 24.72 ± 8.64 | 26.34 ± 10.00 | 22.91 ± 6.63 |
| Preoperative medications, mean ± SD | 2.94 ± 0.92 | 3.11 ± 0.81 | 2.76 ± 1.03 |
| MD (decibel), mean ± SD | −17.65 ± 10.54 | −18.34 ± 10.41 | −16.87 ± 10.96 |
| PSD (decibel), mean ± SD | 7.56 ± 3.66 | 7.93 ± 3.34 | 7.13 ± 4.04 |
| VFI mean ± SD | 48.20 ± 34.68 | 46.58 ± 33.37 | 50.13 ± 37.19 |
| Total (n = 36) | Group 1 (MMC 0.2 mg/mL) (n = 19) | Group 2 (MMC 0.4 mg/mL) (n = 17) | p-Value | |
|---|---|---|---|---|
| IOP (mmHg), mean ± SD | ||||
| Preoperative | 24.72 ± 8.64 | 26.34 ± 10.00 | 22.91 ± 6.63 | 0.230 a |
| Postoperative 1 day | 14.01 ± 8.84 | 16.24 ± 10.45 | 11.53 ± 5.99 | 0.112 a |
| Postoperative 1 week | 12.26 ± 5.55 | 12.87 ± 6.74 | 11.59 ± 3.92 | 0.498 a |
| Postoperative 1 month | 12.47 ± 4.63 | 11.53 ± 4.50 | 13.53 ± 4.67 | 0.199 a |
| Postoperative 3 months | 12.03 ± 3.30 | 11.94 ± 4.03 | 12.12 ± 2.50 | 0.879 a |
| Postoperative 6 months | 12.88 ± 4.63 | 12.71 ± 5.69 | 13.07 ± 3.22 | 0.830 a |
| IOP reduction (mmHg), mean ± SD | ||||
| Postoperative 1 day | 10.71 ± 13.17 | 10.11 ± 15.51 | 11.38 ± 10.40 | 0.776 a |
| Postoperative 1 week | 12.46 ± 11.47 | 13.47 ± 13.40 | 11.32 ± 10.01 | 0.582 a |
| Postoperative 1 month | 12.25 ± 9.51 | 14.82 ± 10.01 | 9.38 ± 8.27 | 0.087 a |
| Postoperative 3 months | 12.62 ± 8.76 | 14.44 ± 9.96 | 10.79 ± 7.21 | 0.230 a |
| Postoperative 6 months | 12.50 ± 8.42 | 14.15 ± 9.51 | 10.63 ± 6.83 | 0.245 a |
| Percentage of IOP reduction (%), mean ± SD | ||||
| Postoperative 1 day | 34.29 ± 47.18 | 26.70 ± 53.07 | 42.77 ± 39.45 | 0.315 a |
| Postoperative 1 week | 40.05 ± 45.27 | 37.49 ± 56.10 | 42.91 ± 30.44 | 0.725 a |
| Postoperative 1 month | 43.42 ± 26.64 | 50.11 ± 23.33 | 35.93 ± 28.76 | 0.112 a |
| Postoperative 3 months | 45.39 ± 22.89 | 48.22 ± 25.39 | 42.57 ± 20.48 | 0.480 a |
| Postoperative 6 months | 44.98 ± 20.92 | 48.53 ± 20.80 | 40.93 ± 21.02 | 0.311 a |
| Number of glaucoma medications, mean ± SD | ||||
| Preoperative | 2.94 ± 0.92 | 3.11 ± 0.81 | 2.76 ± 1.03 | 0.276 a |
| Postoperative 1 day | 0.14 ± 0.42 | 0.26 ± 0.56 | 0 | 0.056 a |
| Postoperative 1 week | 0.19 ± 0.47 | 0.26 ± 0.56 | 0.12 ± 0.33 | 0.358 a |
| Postoperative 1 month | 0.33 ± 0.59 | 0.32 ± 0.58 | 0.35 ± 0.61 | 0.852 a |
| Postoperative 3 months | 0.56 ± 0.82 | 0.59 ± 0.71 | 0.53 ± 0.94 | 0.839 a |
| Postoperative_6 months | 0.53 ± 0.72 | 0.59 ± 0.71 | 0.47 ± 0.74 | 0.640 a |
| Criterion A (IOP ≤18 mmHg and ≥20%) | Criterion B (IOP ≤15 mmHg and ≥25%) | Criterion C (IOP ≤12 mmHg and ≥30%) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | |||||||||
| HR | 95% CI | p-value | HR | 95% CI | p-value | HR | 95% CI | p-value | |
| Age | 0.997 | 0.958–1.038 | 0.877 a | 1.016 | 0.980–1.052 | 0.390 a | 1.025 | 0.992–1.058 | 0.134 a |
| Sex | 0.937 | 0.234–3.752 | 0.927 a | 0.992 | 0.332–2.960 | 0.988 a | 1.340 | 0.539–3.334 | 0.529 a |
| MMC concentration | 0.883 | 0.237–3.290 | 0.853 a | 0.606 | 0.203–1.810 | 0.370 a | 0.781 | 0.314–1.942 | 0.595 a |
| Surgeon | 0.612 | 0.257–1.459 | 0.268 a | 0.711 | 0.374–1.354 | 0.299 a | 1.073 | 0.649–1.774 | 0.783 a |
| Diabetes | 1.694 | 0.490–7.866 | 0.340 a | 1.090 | 0.303–3.920 | 0.895 a | 1.175 | 0.390–3.544 | 0.775 a |
| Systemic hypertension | 0.694 | 0.173–2.774 | 0.605 a | 0.545 | 0.171–1.740 | 0.306 a | 1.029 | 0.414–2.558 | 0.952 a |
| Rheumatic disease | 0.045 | 0.000–8587.18 | 0.618 a | 1.468 | 0.192–11.243 | 0.712 a | 0.993 | 0.133–7.441 | 0.995 a |
| Type of glaucoma | 0.492 | 0.216–1.122 | 0.092 a | 0.771 | 0.485–1.224 | 0.270 a | 0.829 | 0.572–1.202 | 0.322 a |
| Previous laser treatment | 0.478 | 0.060–3.826 | 0.487 a | 0.663 | 0.148–2.964 | 0.591 a | 0.754 | 0.229–2.692 | 0.700 a |
| Previous cataract op | 1.288 | 0.267–6.208 | 0.753 a | 1.122 | 0.313–4.024 | 0.859 a | 1.429 | 0.515–3.969 | 0.493 a |
| CCT | 1.003 | 0.985–1.021 | 0.771 a | 0.997 | 0.984–1.010 | 0.634 a | 0.998 | 0.987–1.009 | 0.736 a |
| AXL | 1.088 | 0.768–1.540 | 0.636 a | 1.028 | 0.757–1.396 | 0.860 a | 0.890 | 0.634–1.249 | 0.500 a |
| Preoperative BCVA | 2.309 | 0.527–10.126 | 0.267 a | 1.507 | 0.424–5.358 | 0.527 a | 1.157 | 0.354–3.786 | 0.809 a |
| Preoperative IOP | 0.858 | 0.764–0.964 | 0.010 a | 0.910 | 0.842–0.984 | 0.018 a | 0.936 | 0.881–0.995 | 0.033 a |
| VF MD | 1.005 | 0.944–1.070 | 0.866 a | 1.005 | 0.956–1.056 | 0.852 a | 1.006 | 0.965–1.050 | 0.765 a |
| VF PSD | 0.979 | 0.820–1.170 | 0.818 a | 1.028 | 0.889–1.189 | 0.709 a | 1.033 | 0.912–1.169 | 0.611 a |
| VF VFI | 0.999 | 0.980–1.019 | 0.948 a | 1.000 | 0.985–1.016 | 0.971 a | 1.001 | 0.988–1.014 | 0.854 a |
| Laser suture lysis | 1.923 | 0.480–7.698 | 0.355 a | 3.895 | 1.081–14.036 | 0.038 a | 2.276 | 0.086–6.022 | 0.098 a |
| MMP-1 staining | 1.526 | 0.184–12.680 | 0.696 a | 2.922 | 0.373–22.871 | 0.307 a | 4.017 | 0.522–30.896 | 0.182 a |
| MMP-2 staining | 1.250 | 0.243–6.443 | 0.790 a | 2.570 | 0.553–11.935 | 0.228 a | 1.975 | 0.549–7.097 | 0.297 a |
| MMP-3 staining | 1.123 | 0.131–9.627 | 0.916 a | 2.473 | 0.313–19.558 | 0.391 a | 3.190 | 0.410–24.837 | 0.268 a |
| MMP-9 staining | 5.464 | 0.635–47.030 | 0.122 a | 5.556 | 1.147–26.922 | 0.033 a | 1.835 | 0.595–5.658 | 0.290 a |
| Multivariate Analysis | |||||||||
| Age | 1.018 | 0.984–1.053 | 0.302 b | ||||||
| Type of glaucoma | 0.521 | 0.202–1.347 | 0.179 b | ||||||
| Preoperative IOP | 0.897 | 0.776–1.036 | 0.138 b | 0.926 | 0.837–1.025 | 0.137 b | 0.936 | 0.881–0.995 | 0.033 b |
| Laser suture lysis | 2.286 | 0.844–6.192 | 0.104 b | ||||||
| MMP-9 stating | 5.464 | 0.635–47.030 | 0.122 b | 5.556 | 1.147–26.922 | 0.033 b | |||
| Total (n = 36) | Group 1 (MMC 0.2 mg/mL) (n = 19) | Group 2 (MMC 0.4 mg/mL) (n = 17) | p-Value | |
|---|---|---|---|---|
| Bleb area: central | ||||
| 1 week | 2.78 ± 1.22 | 2.79 ± 1.25 | 2.77 ± 1.24 | 0.973 a |
| 1 month | 2.73 ± 1.08 | 2.82 ± 1.25 | 2.64 ± 0.92 | 0.703 a |
| 3 months | 2.77 ± 1.02 | 2.92 ± 1.17 | 2.60 ± 0.84 | 0.469 a |
| 6 months | 2.76 ± 1.00 | 2.73 ± 1.19 | 2.80 ± 0.79 | 0.870 a |
| Bleb area: maximal | ||||
| 1 week | 3.30 ± 1.07 | 3.36 ± 1.22 | 3.23 ± 0.93 | 0.763 a |
| 1 month | 3.27 ± 0.98 | 3.18 ± 1.08 | 3.36 ± 0.92 | 0.676 a |
| 3 months | 3.32 ± 0.89 | 3.42 ± 1.08 | 3.20 ± 0.63 | 0.584 a |
| 6 months | 3.43 ± 0.81 | 3.55 ± 1.04 | 3.30 ± 0.48 | 0.502 a |
| Bleb height | ||||
| 1 week | 1.33 ± 0.48 | 1.43 ± 0.51 | 1.23 ± 0.44 | 0.291 a |
| 1 month | 1.59 ± 0.73 | 1.27 ± 0.47 | 1.91 ± 0.83 | 0.042 a |
| 3 months | 1.91 ± 1.02 | 1.67 ± 0.49 | 2.20 ± 1.40 | 0.230 a |
| 6 months | 2.05 ± 1.02 | 1.82 ± 0.75 | 2.30 ± 1.25 | 0.293 a |
| Bleb vascularity: central | ||||
| 1 week | 2.15 ± 0.86 | 2.36 ± 0.63 | 1.92 ± 1.04 | 0.198 a |
| 1 month | 1.86 ± 0.83 | 2.18 ± 0.87 | 1.55 ± 0.69 | 0.073 a |
| 3 months | 1.50 ± 0.60 | 1.58 ± 0.67 | 1.40 ± 0.52 | 0.477 a |
| 6 months | 1.52 ± 0.51 | 1.55 ± 0.52 | 1.50 ± 0.53 | 0.845 a |
| Bleb vascularity: peripheral | ||||
| 1 week | 2.89 ± 0.64 | 2.86 ± 0.66 | 2.92 ± 0.64 | 0.795 a |
| 1 month | 2.55 ± 0.80 | 2.64 ± 0.81 | 2.45 ± 0.82 | 0.606 a |
| 3 months | 2.18 ± 0.50 | 2.17 ± 0.58 | 2.20 ± 0.42 | 0.877 a |
| 6 months | 2.10 ± 0.30 | 2.09 ± 0.30 | 2.10 ± 0.32 | 0.947 a |
| Bleb vascularity: non-bleb | ||||
| 1 week | 2.30 ± 0.54 | 2.14 ± 0.54 | 2.46 ± 0.52 | 0.129 a |
| 1 month | 2.09 ± 0.68 | 2.18 ± 0.75 | 2.00 ± 0.63 | 0.546 a |
| 3 months | 1.86 ± 0.47 | 1.75 ± 0.45 | 2.00 ± 0.47 | 0.222 a |
| 6 months | 2.05 ± 0.38 | 2.00 ± 0.45 | 2.10 ± 0.32 | 0.559 a |
| Subconjunctival hemorrhage | ||||
| 1 week | 0.48 ± 0.51 | 0.36 ± 0.50 | 0.62 ± 0.51 | 0.193 a |
| 1 month | 0.05 ± 0.21 | 0.00 | 0.09 ± 0.30 | 0.329 a |
| 3 months | 0.05 ± 0.21 | 0.08 ± 0.30 | 0 | 0.339 a |
| 6 months | 0 | 0 | 0 | N/A |
| Total (n = 36) | Group 1 (MMC 0.2 mg/mL) (n = 19) | Group 2 (MMC 0.4 mg/mL) (n = 17) | p-Value | |
|---|---|---|---|---|
| Complications | ||||
| Hyphema, n (%) | 1 (2.8) | 0 | 1 (5.9) | 0.472 a |
| Hypotony, n (%) | 2 (5.6) | 2 (10.5) | 0 | 0.487 |
| Bleb leak, n (%) | 0 | 0 | 0 | N/A |
| Blebitis, n (%) | 0 | 0 | 0 | N/A |
| Endophthalmitis, n (%) | 0 | 0 | 0 | N/A |
| Choroidal detachment, n (%) | 1 (2.8) | 1 (5.3) | 0 | 1.000 a |
| Additional procedures | ||||
| Laser suture lysis, n (%) | 19 (52.8) | 12 (63.2) | 7 (41.2) | 0.316 a |
| Bleb needling, n (%) | 9 (25.0) | 5 (26.3) | 4 (23.5) | 1.000 a |
| Bleb massage, n (%) | 15 (78.9) | 10 (52.6) | 5 (29.4) | 0.192 a |
| 5 FU injection, n (%) | 2 (10.5) | 0 | 2 (11.8) | 0.216 a |
| Additional surgery, n (%)(bleb revision or secondary glaucoma surgery) | 0 | 0 | 0 | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seol, B.R.; Lee, S.Y.; Kim, Y.J.; Kim, Y.K.; Jeoung, J.W.; Park, K.H. Comparison of the Efficacy and Safety of Trabeculectomy with Mitomycin C According to Concentration: A Prospective Randomized Clinical Trial. J. Clin. Med. 2021, 10, 59. https://doi.org/10.3390/jcm10010059
Seol BR, Lee SY, Kim YJ, Kim YK, Jeoung JW, Park KH. Comparison of the Efficacy and Safety of Trabeculectomy with Mitomycin C According to Concentration: A Prospective Randomized Clinical Trial. Journal of Clinical Medicine. 2021; 10(1):59. https://doi.org/10.3390/jcm10010059
Chicago/Turabian StyleSeol, Bo Ram, Sang Yoon Lee, Yu Jeong Kim, Young Kook Kim, Jin Wook Jeoung, and Ki Ho Park. 2021. "Comparison of the Efficacy and Safety of Trabeculectomy with Mitomycin C According to Concentration: A Prospective Randomized Clinical Trial" Journal of Clinical Medicine 10, no. 1: 59. https://doi.org/10.3390/jcm10010059
APA StyleSeol, B. R., Lee, S. Y., Kim, Y. J., Kim, Y. K., Jeoung, J. W., & Park, K. H. (2021). Comparison of the Efficacy and Safety of Trabeculectomy with Mitomycin C According to Concentration: A Prospective Randomized Clinical Trial. Journal of Clinical Medicine, 10(1), 59. https://doi.org/10.3390/jcm10010059