
Limited Liver or Lung Colorectal Cancer Metastases. Systemic Treatment, Surgery, Ablation or SBRT

 , , , , ,
, , , , ,
Abstract
:- Percutaneous ablation and stereotactic body radiotherapy of colorectal cancer liver and lung metastases.
- Systemic treatment of patients with colorectal cancer resectable liver metastases.
- Systemic treatment of patients with colorectal cancer potentially resectable liver metastases.
1. Percutaneous Ablation and Stereotactic Body Radiotherapy of Liver and Lung Metastases from Colorectal Cancer
- The size and localization of the metastases and therefore, access regarding selection of the best treatment method;
- The local control rates achieved (with greater local control for surgery than for the remaining options);
- The invasiveness of the technique;
- The non-tumor-related prognostic considerations and patient-relevant factors as well as patient preferences;
- The local expertise regarding the use of each ablative treatment method;
- Consideration of patient frailty and life expectancy [2].
1.1. Percutaneous Ablation
1.1.1. Types of Percutaneous Ablation
1.1.2. Lung Metastases Ablation
1.1.3. Liver Metastases Ablation
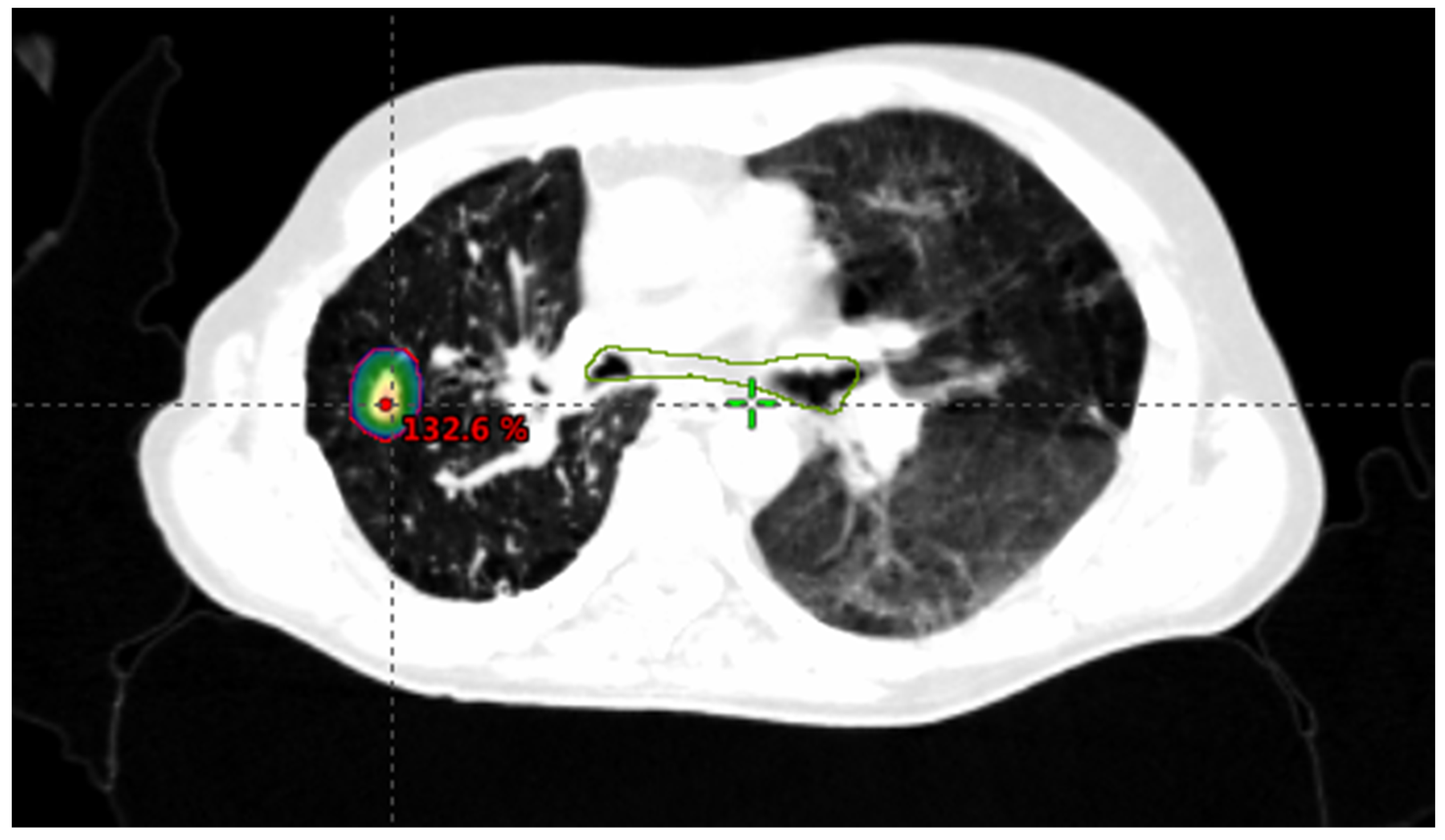
1.2. Stereotactic Body Radiotherapy (SBRT)
1.2.1. SBRT Technique
1.2.2. SBRT Dose
1.2.3. Criteria for Determining SBRT Suitability
1.2.4. SBRT Outcomes
- -
- Evaluate these patients with a multidisciplinary team of experts in colorectal cancer.
- -
- Local ablative treatments or SBRT must be considered to treat limited lung and liver CRC M1 smaller than or equal to 5 cm.
- -
- RFA is preferred in CRC M1 smaller than 3 cm. MWA could be considered in CRC M1 ≤ 5 cm.
- -
- There is no maximum limit on the number of lesions to treat with ablative treatments or SBRT, but the consensus from most studies recommends a maximum of 5 lesions.
- -
- Consider SBRT to treat lung and liver M1 close to vascular, biliary, or gastrointestinal structures;, laparoscopic ablative treatments also could be considered.
- -
- Take into account clinical and molecular tumor prognostic factors, patient preferences, patient comorbidities, and center experience.
2. Treatment of Patients with Resectable Liver Colorectal Metastases (Liver M1: Number <4 and Size <5 cm)
- -
- A perioperative schedule with FOLFOX is recommended in this population of patients.
- -
- Combinations of FOLFOX with bevacizumab or anti-EGFR cannot be recommended based on RCTs.
- -
- Stratification criteria in prospective RCTs should consider the number of liver nodules (1 vs. 2–4) and the DFI (disease free interval) <12 vs. >12 months.
- -
- In elderly and frail patients, consider SBRT or local ablative treatments alone or in combination with surgery. Take into account center experience and patient preferences.
- -
- Evaluate all of these patients with a multidisciplinary team of experts in colorectal cancer.
3. Treatment of Potentially Resectable Liver Metastases from Colorectal Cancer (Liver M1: Number >4 or Size >5 cm)
- -
- A highly active regimen in terms of ORR and tumor shrinkage is recommended for patients with potentially resectable CRC liver metastases.
- -
- For RAS wild-type patients, an anti-EGFR combination schedule is recommended regardless of sidedness, if conversion is the goal.
- -
- For RAS mutant patients, a bevacizumab combination-schedule is recommended regardless of sidedness, if conversion is the goal. For fit patients, FOLFIRINOX-bevacizumab is the preferred schedule.
- -
- In elderly and frail patients consider SBRT or local ablative treatments alone or in combination with surgery if good response is achieved with systemic treatment. Consider patient preferences and center experience.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aguilar, E.A.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Andersen, I.R.; Thorup, K.; Jepsen, B.N.; Mortensen, F.V.; Nielsen, D.T.; Rasmussen, F. Dynamic contrast-enhanced computed tomography in the treatment evaluation of patients with colorectal liver metastases treated with ablation: A feasibility study. Acta Radiol. 2019, 60, 936–945. [Google Scholar] [CrossRef] [PubMed]
- Palussière, J.; Catena, V.; Buy, X. Percutaneous thermal ablation of lung tumors–Radiofrequency, microwave and cryotherapy: Where are we going? Diagn. Interv. Imaging 2017, 98, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; Liu, Z.; Afzal, K.S.; Weeks, D.; Lobo, S.M.; Kruskal, J.B.; Lenkinski, R.E.; Goldberg, S.N. Radiofrequency Ablation: Effect of Surrounding Tissue Composition on Coagulation Necrosis in a Canine Tumor Model. Radiology 2004, 230, 761–767. [Google Scholar] [CrossRef]
- Ihara, H.; Gobara, H.; Hiraki, T.; Mitsuhashi, T.; Iguchi, T.; Fujiwara, H.; Matsui, Y.; Soh, J.; Toyooka, S.; Kanazawa, S. Radiofrequency Ablation of Lung Tumors Using a Multitined Expandable Electrode: Impact of the Electrode Array Diameter on Local Tumor Progression. J. Vasc. Interv. Radiol. 2016, 27, 87–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, A.S.; Sampson, L.A.; Warner, T.F.; Mahvi, D.M.; Lee, J.F.T. Radiofrequency versus Microwave Ablation in a Hepatic Porcine Model. Radiology 2005, 236, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Iida, T.; Nomori, H.; Shiba, M.; Nakajima, J.; Okumura, S.; Horio, H.; Haruhisa, M.; Norihiko, I.; Ichiro, Y.; Yuichi, O.; et al. Prognostic factors after pulmonary metastasectomy for colorectal cancer and rationale for determining surgical indications: A retrospective analysis. Ann. Surg. 2013, 257, 1059–1064. [Google Scholar] [CrossRef]
- Pfannschmidt, J.; Hoffmann, H.; Dienemann, H. Reported Outcome Factors for Pulmonary Resection in Metastatic Colorectal Cancer. J. Thorac. Oncol. 2010, 5, S172–S178. [Google Scholar] [CrossRef]
- Baba, Y.; Watanabe, M.; Yoshida, N.; Kawanaka, K.; Yamashita, Y.; Baba, H. Radiofrequency Ablation for Pulmonary Metastases from Gastrointestinal Cancers. Ann. Thorac. Cardiovasc. Surg. 2014, 20, 99–105. [Google Scholar] [CrossRef] [Green Version]
- De Baère, T.; Aupérin, A.; Deschamps, F.; Chevallier, P.; Gaubert, Y.; Boige, V.; Fonck, M.; Escudier, B.; Palussiére, J. Radiofrequency ablation is a valid treatment option for lung metastases: Experience in 566 patients with 1037 metastases. Ann. Oncol. 2015, 26, 987–991. [Google Scholar] [CrossRef] [PubMed]
- Vogl, T.J.; Eckert, R.; Naguib, N.N.N.; Beeres, M.; Gruber-Rouh, T.; Nour-Eldin, N.-E.A. Thermal Ablation of Colorectal Lung Metastases: Retrospective Comparison among Laser-Induced Thermotherapy, Radiofrequency Ablation, and Microwave Ablation. Am. J. Roentgenol. 2016, 207, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
- De Baere, T.; Tselikas, L.; Woodrum, D.; Abtin, F.; Littrup, P.; Deschamps, F.; Suh, R.; Aoun, H.D.; Callstrom, M. Evaluating cryoablation of metastatic lung tumors in patients-safety and efficacy the ECLIPSE trial-interim analysis at 1 year. J. Thorac. Oncol. 2015, 10, 1468–1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, T.D.; King, J.; Sjarif, A.; Glenn, D.; Steinke, K.; Morris, D.L. Percutaneous Radiofrequency Ablation of Pulmonary Metastases from Colorectal Carcinoma: Prognostic Determinants for Survival. Ann. Surg. Oncol. 2006, 13, 1529–1537. [Google Scholar] [CrossRef] [PubMed]
- Stoltz, A.; Gagnière, J.; Dupré, A.; Rivoire, M. Radiofrequency ablation for colorectal liver metastases. J. Visc. Surg. 2014, 151, S33–S44. [Google Scholar] [CrossRef]
- Gurusamy, K.; Corrigan, N.; Croft, J.; Twiddy, M.; Morris, S.; Woodward, N.; Bandula, S.; Hochhauser, D.; Napp, V.; Pullan, A.; et al. Liver resection surgery versus thermal ablation for colorectal LiVer MetAstases (LAVA): Study protocol for a randomised controlled trial. Trials 2018, 19, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puijk, R.S.; COLLISION Trial Group; Ruarus, A.H.; Vroomen, L.G.P.H.; Van Tilborg, A.A.J.M.; Scheffer, H.J.; Nielsen, K.; De Jong, M.C.; De Vries, J.J.J.; Zonderhuis, B.M.; et al. Colorectal liver metastases: Surgery versus thermal ablation (COLLISION)–a phase III single-blind prospective randomized controlled trial. BMC Cancer 2018, 18, 821. [Google Scholar] [CrossRef]
- Abdalla, E.K.; Vauthey, J.-N.; Ellis, L.M.; Ellis, V.; Pollock, R.; Broglio, K.R.; Hess, K.; Curley, S.A. Recurrence and Outcomes Following Hepatic Resection, Radiofrequency Ablation, and Combined Resection/Ablation for Colorectal Liver Metastases. Ann. Surg. 2004, 239, 818–827. [Google Scholar] [CrossRef]
- Liang, P.; Wang, Y.; Yu, X.; Dong, B. Malignant Liver Tumors: Treatment with Percutaneous Microwave Ablation—Complications among Cohort of 1136 Patients. Radiology 2009, 251, 933–940. [Google Scholar] [CrossRef]
- Shady, W.; Petre, E.N.; Gonen, M.; Erinjeri, J.P.; Brown, K.T.; Covey, A.M.; Alago, W.; Durack, J.C.; Maybody, M.; Brody, L.A.; et al. Percutaneous Radiofrequency Ablation of Colorectal Cancer Liver Metastases: Factors Affecting Outcomes—A 10-year Experience at a Single Center. Radiology 2016, 278, 601–611. [Google Scholar] [CrossRef] [Green Version]
- Hammill, C.W.; Billingsley, K.G.; Cassera, M.A.; Wolf, R.F.; Ujiki, M.B.; Hansen, P.D. Outcome After Laparoscopic Radiofrequency Ablation of Technically Resectable Colorectal Liver Metastases. Ann. Surg. Oncol. 2011, 18, 1947–1954. [Google Scholar] [CrossRef]
- Gillams, A.; Goldberg, N.; Ahmed, M.; Bale, R.; Breen, D.; Callstrom, M.; Chen, M.H.; Choi, B.I.; De Baere, T.; Dupuy, D.; et al. Thermal ablation of colorectal liver metastases: A position paper by an international panel of ablation experts, the interventional oncology sans frontières meeting 2013. Eur. Radiol. 2015, 25, 3438–3454. [Google Scholar] [CrossRef]
- Ruers, T.; Van Coevorden, F.; Punt, C.J.A.; Pierie, J.-P.E.N.; Borel-Rinkes, I.; Ledermann, J.A.; Poston, G.; Bechstein, W.; Lentz, M.-A.; Mauer, M.; et al. Local Treatment of Unresectable Colorectal Liver Metastases: Results of a Randomized Phase II Trial. J. Natl. Cancer Inst. 2017, 109, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Potters, L.; Kavanagh, B.; Galvin, J.M.; Hevezi, J.M.; Janjan, N.A.; Larson, D.A.; Mehta, M.P.; Ryu, S.; Steinberg, M.; Timmerman, R.; et al. American Society for Therapeutic Radiology and Oncology (ASTRO) and American College of Radiology (ACR) Practice Guideline for the Performance of Stereotactic Body Radiation Therapy. Int. J. Radiat. Oncol. 2010, 76, 326–332. [Google Scholar] [CrossRef]
- Timmerman, R.D. An Overview of Hypofractionation and Introduction to This Issue of Seminars in Radiation Oncology. Semin. Radiat. Oncol. 2008, 18, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Benedict, S.H.; Yenice, K.M.; Followill, D.; Galvin, J.M.; Hinson, W.; Kavanagh, B.; Keall, P.; Lovelock, M.; Meeks, S.; Papiez, L.; et al. Stereotactic body radiation therapy: The report of AAPM Task Group 101. Med Phys. 2010, 37, 4078–4101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanna, G.; Murray, L.; Patel, R.; Jain, S.; Aitken, K.; Franks, K.; van As, N.; Tree, A.; Hatfield, P.; Harrow, S.; et al. UK Consensus on Normal Tissue Dose Constraints for Stereotactic Radiotherapy. Clin. Oncol. 2018, 30, 5–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klement, R.J.; Abbasi-Senger, N.; Adebahr, S.; Alheid, H.; Allgaeuer, M.; Becker, G.; Blanck, O.; Boda-Heggemann, J.; Brunner, T.; Duma, M.; et al. The impact of local control on overall survival after stereotactic body radiotherapy for liver and lung metastases from colorectal cancer: A combined analysis of 388 patients with 500 metastases. BMC Cancer 2019, 19, 173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McPartlin, A.; Swaminath, A.; Wang, R.; Pintilie, M.; Brierley, J.; Kim, J.; Ringash, J.; Wong, R.; Dinniwell, R.; Craig, T.; et al. Long-Term Outcomes of Phase 1 and 2 Studies of SBRT for Hepatic Colorectal Metastases. Int. J. Radiat. Oncol. 2017, 99, 388–395. [Google Scholar] [CrossRef]
- Scorsetti, M.; Comito, T.; Tozzi, A.; Navarria, P.; Fogliata, A.; Clerici, E.; Mancosu, P.; Reggiori, G.; Rimassa, L.; Torzilli, G.; et al. Final results of a phase II trial for stereotactic body radiation therapy for patients with inoperable liver metastases from colorectal cancer. J. Cancer Res. Clin. Oncol. 2015, 141, 543–553. [Google Scholar] [CrossRef]
- Tree, A.C.; Khoo, V.S.; Eeles, R.A.; Ahmed, M.; Dearnaley, D.P.; Hawkins, M.A.; Huddart, R.A.; Nutting, C.M.; Ostler, P.J.; van As, N.J. Stereotactic body radiotherapy for oligometastases. Lancet Oncol. 2013, 14, e28–e37. [Google Scholar] [CrossRef]
- Huang, F.; Wu, G.; Yang, K. Oligometastasis and oligo-recurrence: More than a mirage. Radiat. Oncol. 2014, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Aitken, K.; Tree, A.; Thomas, K.; Nutting, C.; Hawkins, M.; Tait, D.; Mandeville, H.; Ahmed, M.; Lalondrelle, S.; Miah, A.; et al. Initial UK Experience of Stereotactic Body Radiotherapy for Extracranial Oligometastases: Can We Change the Therapeutic Paradigm? Clin. Oncol. 2015, 27, 411–419. [Google Scholar] [CrossRef]
- Lehrer, E.J.; Singh, R.; Wang, M.; Chinchilli, V.M.; Trifiletti, D.M.; Ost, P.; Siva, S.; Meng, M.; Tchelebi, L.; Zaorsky, N.G. Safety and Survival Rates Associated with Ablative Stereotactic Radiotherapy for Patients with Oligometastatic Cancer: A Systematic Review and Meta-analysis. JAMA Oncol. 2021, 7, 92–106. [Google Scholar] [CrossRef] [PubMed]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): A randomised, phase 2, open-label trial. Lancet 2019, 393, 2051–2058. [Google Scholar] [CrossRef]
- Petrelli, F.; Comito, T.; Barni, S.; Pancera, G.; Scorsetti, M.; Ghidini, A. Stereotactic body radiotherapy for colorectal cancer liver metastases: A systematic review. Radiother. Oncol. 2018, 129, 427–434. [Google Scholar] [CrossRef]
- Langer, B.; Bleiberg, H.; Labianca, R.; Shepherd, L.; Nitti, D.; Marsoni, S.; Tu, D.; Sargeant, A.M.F.A. Fluorouracil (FU) plus leucovorin (I-LV) versus observation after potentially curative resection of liver or lung metastases from colorectal cancer (CRC): Results of the ENG (EORTC/NCIC/CTG/GIVIO) randomized trial. Proc. Am. Clin. Oncol. 2002, 21, 149a. [Google Scholar]
- Portier, G.; Elias, D.; Bouche, O.; Rougier, P.; Bosset, J.-F.; Saric, J.; Belghiti, J.; Piedbois, P.; Guimbaud, R.; Nordlinger, B.; et al. Multicenter Randomized Trial of Adjuvant Fluorouracil and Folinic Acid Compared With Surgery Alone After Resection of Colorectal Liver Metastases: FFCD ACHBTH AURC 9002 Trial. J. Clin. Oncol. 2006, 24, 4976–4982. [Google Scholar] [CrossRef]
- Mitry, E.; Fields, A.L.; Bleiberg, H.; Labianca, R.; Portier, G.; Tu, D.; Nitti, D.; Torri, V.; Elias, D.; O’Callaghan, C.; et al. Adjuvant Chemotherapy After Potentially Curative Resection of Metastases From Colorectal Cancer: A Pooled Analysis of Two Randomized Trials. J. Clin. Oncol. 2008, 26, 4906–4911. [Google Scholar] [CrossRef]
- Kobayashi, A.; Hasegawa, K.; Saiura, A.; Takayama, T.; Miyagawa, S.; Yamamoto, J.; Bandai, Y.; Teruya, M.; Yoshimi, F.; Kawasaki, S.; et al. A randomized controlled trial evaluating efficacy of adjuvant oral uracil-tegafur (UFT) with leucovorin (LV) after resection of colorectal cancer liver metastases: The UFT/LV study. J. Clin. Oncol. 2014. [Google Scholar] [CrossRef]
- Kanemitsu, Y.; Shimizu, Y.; Mizusawa, J.; Inaba, Y.; Hamaguchi, T.; Shida, D.; Ohue, M.; Komori, K.; Shiomi, A.; Shiozawa, M.; et al. A randomized phase II/III trial comparing hepatectomy followed by mFOLFOX6 with hepatectomy alone for liver metastasis from colorectal cancer: JCOG0603 study. J. Clin. Oncol. 2020, 38, 4005. [Google Scholar] [CrossRef]
- Ychou, M.; Hohenberger, W.; Thezenas, S.; Navarro, M.; Maurel, J.; Bokemeyer, C.; Shacham-Shmueli, E.; Rivera, F.; Choi, C.K.-K.; Santoro, A. A randomized phase III study comparing adjuvant 5-fluorouracil/folinic acid with FOLFIRI in patients following complete resection of liver metastases from colorectal cancer. Ann. Oncol. 2009, 20, 1964–1970. [Google Scholar] [CrossRef] [PubMed]
- Kemeny, N.; Huang, Y.; Cohen, A.M.; Shi, W.; Conti, J.A.; Brennan, M.F.; Bertino, J.R.; Turnbull, A.D.M.; Sullivan, D.; Stockman, J.; et al. Hepatic Arterial Infusion of Chemotherapy After Resection of Hepatic Metastases From Colorectal Cancer. Nejm 1999, 341, 2039–2048. [Google Scholar] [CrossRef] [PubMed]
- Kemeny, N.E.; Gonen, M. Hepatic Arterial Infusion after Liver Resection. N. Engl. J. Med. 2005, 352, 734–735. [Google Scholar] [CrossRef] [PubMed]
- Kemeny, M.M.; Adak, S.; Gray, B.; Macdonald, J.S.; Smith, T.; Lipsitz, S.; Sigurdson, E.R.; O’Dwyer, P.J.; Benson, A.B. Combined-Modality Treatment for Resectable Metastatic Colorectal Carcinoma to the Liver: Surgical Resection of Hepatic Metastases in Combination With Continuous Infusion of Chemotherapy—An Intergroup Study. J. Clin. Oncol. 2002, 20, 1499–1505. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.; Müller, H.-H.; Schramm, H.; Gassel, H.-J.; Rau, H.-G.; Ridwelski, K.; Hauss, J.; Stieger, R.; Jauch, K.-W.; Bechstein, W.O.; et al. Randomized Trial of Surgery Versus Surgery Followed by Adjuvant Hepatic Arterial Infusion With 5-Fluorouracil and Folinic Acid for Liver Metastases of Colorectal Cancer. Ann. Surg. 1998, 228, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Nordlinger, B.; Sorbye, H.; Glimelius, B.; Poston, G.J.; Schlag, P.M.; Rougier, P.; Bechstein, W.O.; Primrose, J.N.; Walpole, E.T.; Finch-Jones, M.; et al. Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): A randomised controlled trial. Lancet 2008, 371, 1007–1016. [Google Scholar] [CrossRef] [Green Version]
- Nordlinger, B.; Sorbye, H.; Glimelius, B.; Poston, G.J.; Schlag, P.M.; Rougier, P.; Bechstein, W.O.; Primrose, J.N.; Walpole, E.T.; Finch-Jones, M.; et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): Long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2013, 14, 1208–1215. [Google Scholar] [CrossRef]
- Primrose, J.; Falk, S.; Finch-Jones, M.; Valle, J.; O’Reilly, D.; Siriwardena, A.; Hornbuckle, J.; Peterson, M.; Rees, M.; Iveson, T.; et al. Systemic chemotherapy with or without cetuximab in patients with resectable colorectal liver metastasis: The New EPOC randomised controlled trial. Lancet Oncol. 2014, 15, 601–611. [Google Scholar] [CrossRef]
- Bridgewater, J.A.; A Pugh, S.; Maishman, T.; Eminton, Z.; Mellor, J.; Whitehead, A.; Stanton, L.; Radford, M.; Corkhill, A.; Griffiths, G.O.; et al. Systemic chemotherapy with or without cetuximab in patients with resectable colorectal liver metastasis (New EPOC): Long-term results of a multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2020, 21, 398–411. [Google Scholar] [CrossRef]
- Snoeren, N.; E Voest, E.; Bergman, A.M.; Dalesio, O.; Verheul, H.M.; Tollenaar, R.A.; Van Der Sijp, J.R.; Schouten, S.B.; Rinkes, I.H.B.; Van Hillegersberg, R. A randomized two arm phase III study in patients post radical resection of liver metastases of colorectal cancer to investigate bevacizumab in combination with capecitabine plus oxaliplatin (CAPOX) vs CAPOX alone as adjuvant treatment. BMC Cancer 2010, 10, 545. [Google Scholar] [CrossRef] [Green Version]
- Adam, R.; Delvart, V.; Pascal, G.; Valeanu, A.; Castaing, D.; Azoulay, D.; Giacchetti, S.; Paule, B.; Kunstlinger, F.; Ghémard, O.; et al. Rescue surgery for unresectable colorectal liver metastases downstaged by chemotherapy: A model to predict long-term survival. Ann. Surg. 2004, 240, 644. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; De Gramont, A.; Figueras, J.; Guthrie, A.; Kokudo, N.; Kunstlinger, F.; Loyer, E.; Poston, G.; Rougier, P.; Rubbia-Brandt, L.; et al. The Oncosurgery Approach to Managing Liver Metastases from Colorectal Cancer: A Multidisciplinary International Consensus. Oncologist 2012, 17, 1225–1239. [Google Scholar] [CrossRef] [Green Version]
- Mentha, G.; Majno, P.; Andres, A.; Rubbia-Brandt, L.; Morel, P.; Roth, A. Neoadjuvant chemotherapy and resection of advanced synchronous liver metastases before treatment of the colorectal primary. BJS 2006, 93, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Folprecht, G.; Gruenberger, T.; O Bechstein, W.; Raab, H.-R.; Lordick, F.; Hartmann, J.T.; Lang, H.; Frilling, A.; Stoehlmacher, J.; Weitz, J.; et al. Tumour response and secondary resectability of colorectal liver metastases following neoadjuvant chemotherapy with cetuximab: The CELIM randomised phase 2 trial. Lancet Oncol. 2010, 11, 38–47. [Google Scholar] [CrossRef]
- Folprecht, G.; Gruenberger, T.; Bechstein, W.; Raab, H.-R.; Weitz, J.; Lordick, F.; Hartmann, J.T.; Stoehlmacher-Williams, J.; Lang, H.; Trarbach, T.; et al. Survival of patients with initially unresectable colorectal liver metastases treated with FOLFOX/cetuximab or FOLFIRI/cetuximab in a multidisciplinary concept (CELIM study). Ann. Oncol. 2014, 25, 1018–1025. [Google Scholar] [CrossRef]
- Garufi, C.; Torsello, A.; Tumolo, S.; Ettorre, G.M.; Zeuli, M.; Campanella, C.; Vennarecci, G.; Mottolese, M.; Sperduti, I.; Cognetti, F. Cetuximab plus chronomodulated irinotecan, 5-fluorouracil, leucovorin and oxaliplatin as neoadjuvant chemotherapy in colorectal liver metastases: POCHER trial. Br. J. Cancer 2010, 103, 1542–1547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, L.-C.; Liu, T.-S.; Ren, L.; Wei, Y.; Zhu, D.-X.; Zai, S.-Y.; Ye, Q.-H.; Yu, Y.; Xu, B.; Qin, X.-Y.; et al. Randomized Controlled Trial of Cetuximab Plus Chemotherapy for Patients With KRAS Wild-Type Unresectable Colorectal Liver-Limited Metastases. J. Clin. Oncol. 2013, 31, 1931–1938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemeny, N.E.; Jarnagin, W.R.; Capanu, M.; Fong, Y.; Gewirtz, A.N.; DeMatteo, R.P.; D’Angelica, M.I. Randomized Phase II Trial of Adjuvant Hepatic Arterial Infusion and Systemic Chemotherapy With or Without Bevacizumab in Patients With Resected Hepatic Metastases From Colorectal Cancer. J. Clin. Oncol. 2011, 29, 884–889. [Google Scholar] [CrossRef] [Green Version]
- Gruenberger, B.; Tamandl, D.; Schueller, J.; Scheithauer, W.; Zielinski, C.; Herbst, F.; Gruenberger, T. Bevacizumab, Capecitabine, and Oxaliplatin As Neoadjuvant Therapy for Patients With Potentially Curable Metastatic Colorectal Cancer. J. Clin. Oncol. 2008, 26, 1830–1835. [Google Scholar] [CrossRef]
- Wong, R.; Cunningham, D.; Barbachano, Y.; Saffery, C.; Valle, J.; Hickish, T.; Mudan, S.; Brown, G.; Khan, A.; Wotherspoon, A.; et al. A multicentre study of capecitabine, oxaliplatin plus bevacizumab as perioperative treatment of patients with poor-risk colorectal liver-only metastases not selected for upfront resection. Ann. Oncol. 2011, 22, 2042–2048. [Google Scholar] [CrossRef]
- Gruenberger, T.; Bridgewater, J.; Chau, I.; Alfonso, P.G.; Rivoire, M.; Mudan, S.; Lasserre, S.; Hermann, F.; Waterkamp, D.; Adam, R. Bevacizumab plus mFOLFOX-6 or FOLFOXIRI in patients with initially unresectable liver metastases from colorectal cancer: The OLIVIA multinational randomised phase II trial. Ann. Oncol. 2015, 26, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Tomasello, G.; Borgonovo, K.; Ghidini, M.; Turati, L.; Dallera, P.; Passalacqua, R.; Sgroi, G.; Barni, S. Prognostic Survival Associated With Left-Sided vs Right-Sided Colon Cancer. JAMA Oncol. 2017, 3, 211–219. [Google Scholar] [CrossRef]
- Arnold, D.; Lueza, B.; Douillard, J.-Y.; Peeters, M.; Lenz, H.-J.; Venook, A.; Heinemann, V.; Van Cutsem, E.; Pignon, J.-P.; Tabernero, J.; et al. Prognostic and predictive value of primary tumour side in patients with RAS wild-type metastatic colorectal cancer treated with chemotherapy and EGFR directed antibodies in six randomized trials. Ann. Oncol. 2017, 28, 1713–1729. [Google Scholar] [CrossRef] [PubMed]
- Holch, J.W.; Ricard, I.; Stintzing, S.; Modest, D.P.; Heinemann, V. The relevance of primary tumour location in patients with metastatic colorectal cancer: A meta-analysis of first-line clinical trials. Eur. J. Cancer. 2017, 70, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Stintzing, S.; Modest, D.P.; Rossius, L.; Lerch, M.M.; von Weikersthal, L.F.; Decker, T.; Kiani, A.; Vehling-Kaiser, U.; Al-Batran, S.-E.; Heintges, T.; et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab for metastatic colorectal cancer (FIRE-3): A post-hoc analysis of tumour dynamics in the final RAS wild-type subgroup of this randomised open-label phase 3 trial. Lancet Oncol. 2016, 17, 1426–1434. [Google Scholar] [CrossRef]
- Rivera, F.; Karthaus, M.; Hecht, J.R.; Sevilla, I.; Forget, F.; Fasola, G.; Canon, J.-L.; Guan, X.; Demonty, G.; Schwartzberg, L.S. Final analysis of the randomised PEAK trial: Overall survival and tumour responses during first-line treatment with mFOLFOX6 plus either panitumumab or bevacizumab in patients with metastatic colorectal carcinoma. Int. J. Colorectal Dis. 2017, 32, 1179–1190. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Author | N | Treatments | HR PFS/OS. <0.8 | Adequate Control Arm | Any Change in Primary End-Point or Sample Size | Achieved Pre-Specified Objective | Quality of Clinical Design | ESMO. MCBS/PFS | ESMO. MCBS/OS | ESMO/MCBS 1.1 |
|---|---|---|---|---|---|---|---|---|---|---|
| Randomized clinical trials in CRC with liver limited M1 (<4 M1) | ||||||||||
| Portier, JCO 2006 | 173 | S vs. S plus 5FU/LV | 0.66/0.73/0.9 | 1 | 0 | 0 | 1 of 3 | B | A | A |
| Mitry, JCO 2008 | 278 | S vs. S plus 5FU/LV | 1.32/1.32/1 | 1 | 1 | NA | NA | B | A | A |
| Hasewaga, Plos One 2016 | 180 | S vs. S plus UFT/LV | 0.56/0.8/0,7 | 1 | 1 | 0 | 2 of 3 | A | C | A |
| Nordlinger, Lancet Oncol 2013 | 364 | S vs. S plus FOLFOX | 0.79/0.88/0.89 | 1 | 1 | 0 | 2 of 3 | B | B | B |
| Ychou, Ann Oncol 2009 | 321 | S plus FU/LV vs. S plus FOLFIRI | 0.89/1.09/0.81 | 0 | 0 | 0 | 0 of 3 | C | C | C |
| Bridgewater JA. Lancet Oncol 2020 | 257 | S plus FOLFOX vs. S plus FOLFOX/CET | 1.17/1.45/0.8 | 1 | 0 | 0 | 1 of 3 | C | C | C |
| Snoeren N. Neoplasia 2017 | 79 | S plus CAPOX vs. S plus CAPOX plus BEV | NA | 0 | 0 | 0 | 0 of 3 | C | C | C |
| Kanemitsu. ASCO 2020 | 300 | S vs. S plus FOLFOX | 0.67/1.25/0.53 | 1 | 1 | 1 | 3 of 3 | B | C | B |
| Randomized Clinical trials in CRC with liver limited M1 (≥4 M1) | ||||||||||
| Ye LC, JCO, 2013 | 138 | CHT plus S vs. CHT/CET plus S | 0.6/0.54/1.11 | 1 | NA | 1 | 1 of 3 | A | A | A |
| Gruenberger, Ann Oncol 2015 | 80 | FOLFOX/BVZ plus S vs. FOLFOXIRI/BVZ plus S | 0.43/0.35/1.22 | 0 | 1 | NA | 1 of 3 | A | NA | A |
| Adding RF or SBRT to chemo | ||||||||||
| Ruers T. JNCI 2017 | 119 | FOLFOX vs. FOLFOX plus RF ± S | 0.57/0.58/0.98 | 1 | 0 | 1 | 2 of 3 | 3 | 3 | 3 |
| Palma, Lancet 2019 | 99 | CHT vs. CHT plus SBRT | 0.47/0.57/0.82 | 1 | 1 | 1 | 2 of 3 | 3 | 4 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molla, M.; Fernandez-Plana, J.; Albiol, S.; Fondevila, C.; Vollmer, I.; Cases, C.; Garcia-Criado, A.; Capdevila, J.; Conill, C.; Fundora, Y.; et al. Limited Liver or Lung Colorectal Cancer Metastases. Systemic Treatment, Surgery, Ablation or SBRT. J. Clin. Med. 2021, 10, 2131. https://doi.org/10.3390/jcm10102131
Molla M, Fernandez-Plana J, Albiol S, Fondevila C, Vollmer I, Cases C, Garcia-Criado A, Capdevila J, Conill C, Fundora Y, et al. Limited Liver or Lung Colorectal Cancer Metastases. Systemic Treatment, Surgery, Ablation or SBRT. Journal of Clinical Medicine. 2021; 10(10):2131. https://doi.org/10.3390/jcm10102131
Chicago/Turabian StyleMolla, Meritxell, Julen Fernandez-Plana, Santiago Albiol, Constantino Fondevila, Ivan Vollmer, Carla Cases, Angeles Garcia-Criado, Jaume Capdevila, Carles Conill, Yliam Fundora, and et al. 2021. "Limited Liver or Lung Colorectal Cancer Metastases. Systemic Treatment, Surgery, Ablation or SBRT" Journal of Clinical Medicine 10, no. 10: 2131. https://doi.org/10.3390/jcm10102131
APA StyleMolla, M., Fernandez-Plana, J., Albiol, S., Fondevila, C., Vollmer, I., Cases, C., Garcia-Criado, A., Capdevila, J., Conill, C., Fundora, Y., Fernandez-Martos, C., & Pineda, E. (2021). Limited Liver or Lung Colorectal Cancer Metastases. Systemic Treatment, Surgery, Ablation or SBRT. Journal of Clinical Medicine, 10(10), 2131. https://doi.org/10.3390/jcm10102131