
Neurosurgical Considerations Regarding Decompressive Craniectomy for Intracerebral Hemorrhage after SARS-CoV-2-Vaccination in Vaccine Induced Thrombotic Thrombocytopenia—VITT

 ,
,  ,
,  , , ,
, , , 
Abstract
:1. Introduction
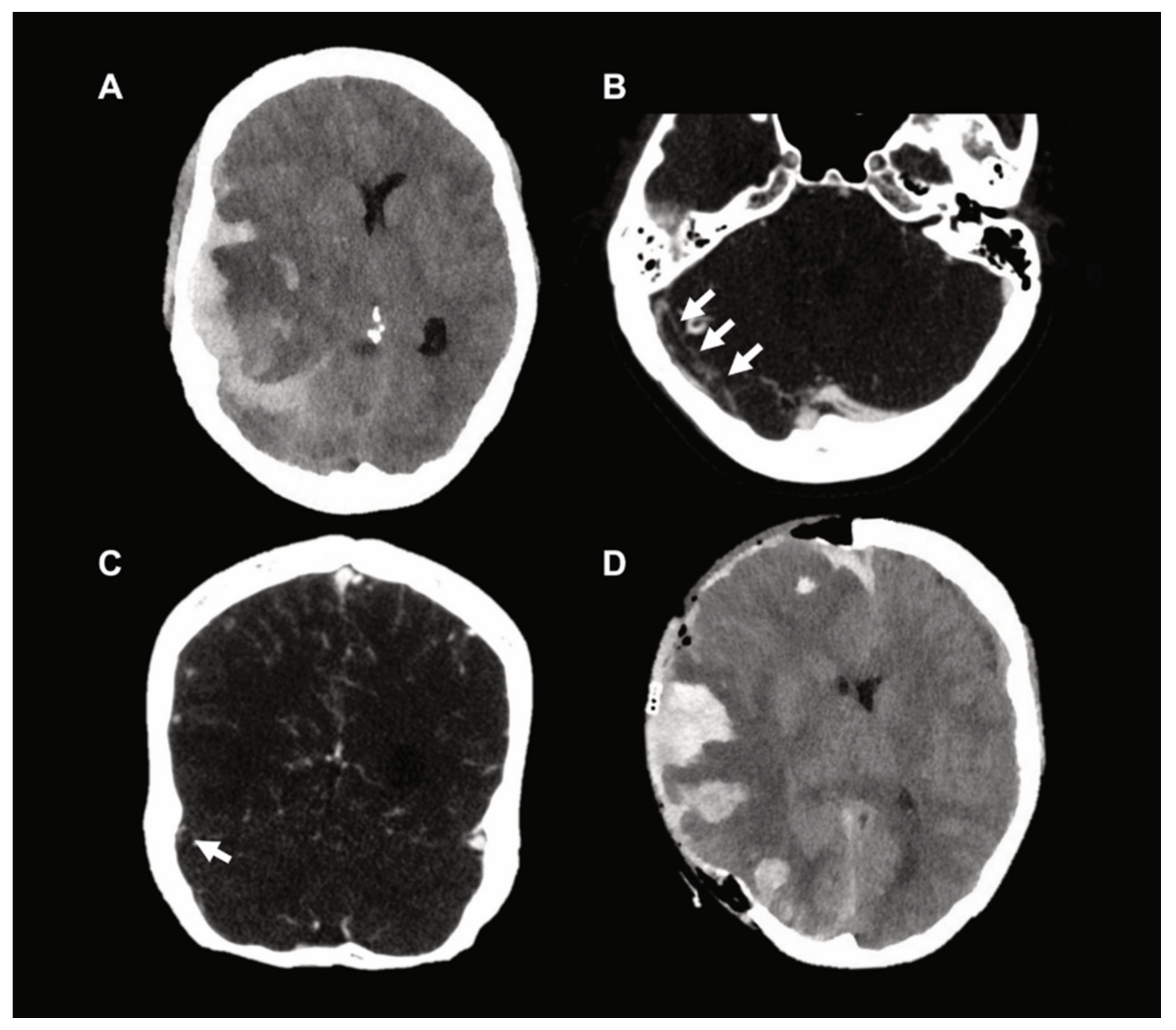
2. Exemplary Case Presentation
3. Discussion
3.1. Neurosurgical Considerations
3.2. Hematological Considerations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coutinho, J.M.; Zuurbier, S.M.; Aramideh, M.; Stam, J. The incidence of cerebral venous thrombosis: A cross-sectional study. Stroke 2012, 43, 3375–3377. [Google Scholar] [CrossRef] [Green Version]
- Amoozegar, F.; Ronksley, P.E.; Sauve, R.; Menon, B.K. Hormonal contraceptives and cerebral venous thrombosis risk: A systematic review and meta-analysis. Front. Neurol. 2015, 6, 7. [Google Scholar] [CrossRef] [Green Version]
- Gessler, F.; Bruder, M.; Duetzmann, S.; Tritt, S.; Bernstock, J.D.; Seifert, V.; Senft, C. Risk factors governing the development of cerebral vein and dural sinus thrombosis after craniotomy in patients with intracranial tumors. J. Neurosurg. 2018, 128, 373–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stam, J. Thrombosis of the cerebral veins and sinuses. N. Engl. J. Med. 2005, 352, 1791–1798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuss, P.; Bode, C.; Borger, V.; Coch, C.; Guresir, A.; Hadjiathanasiou, A.; Hamed, M.; Kuchelmeister, K.; Lehmann, F.; Muller, M.; et al. MR-Imaging and Histopathological Diagnostic Work-Up of Patients with Spontaneous Lobar Intracerebral Hemorrhage: Results of an Institutional Prospective Registry Study. Diagnostics (Basel) 2021, 11, 368. [Google Scholar] [CrossRef]
- Carli, G.; Nichele, I.; Ruggeri, M.; Barra, S.; Tosetto, A. Deep vein thrombosis (DVT) occurring shortly after the second dose of mRNA SARS-CoV-2 vaccine. Intern. Emerg. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.J.; Cines, D.B.; Gernsheimer, T.; Kessler, C.; Michel, M.; Tarantino, M.D.; Semple, J.W.; Arnold, D.M.; Godeau, B.; Lambert, M.P.; et al. Thrombocytopenia following Pfizer and Moderna SARS-CoV-2 vaccination. Am. J. Hematol. 2021. [Google Scholar] [CrossRef]
- Tarawneh, O.; Tarawneh, H. Immune thrombocytopenia in a 22-year-old post Covid-19 vaccine. Am. J. Hematol. 2021. [Google Scholar] [CrossRef]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Scully, M.; Singh, D.; Lown, R.; Poles, A.; Solomon, T.; Levi, M.; Goldblatt, D.; Kotoucek, P.; Thomas, W.; Lester, W. Pathologic Antibodies to Platelet Factor 4 after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Schultz, N.H.; Sorvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.H.; Skattor, T.H.; Tjonnfjord, G.E.; et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2124–2130. [Google Scholar] [CrossRef]
- Makris, M.; Pavord, S.; Lester, W.; Scully, M.; Hunt, B. Vaccineinduced Immune Thrombocytopenia and Thrombosis (VITT). Res. Pr. Thromb Haemost Res. Pract. Thromb. Haemost. 2021, 5, e12529. [Google Scholar]
- Einhaupl, K.M.; Villringer, A.; Meister, W.; Mehraein, S.; Garner, C.; Pellkofer, M.; Haberl, R.L.; Pfister, H.W.; Schmiedek, P. Heparin treatment in sinus venous thrombosis. Lancet 1991, 338, 597–600. [Google Scholar] [CrossRef]
- Barnwell, S.L.; Higashida, R.T.; Halbach, V.V.; Dowd, C.F.; Hieshima, G.B. Direct endovascular thrombolytic therapy for dural sinus thrombosis. Neurosurgery 1991, 28, 135–142. [Google Scholar] [CrossRef] [PubMed]
- de Bruijn, S.F.; Stam, J. Randomized, placebo-controlled trial of anticoagulant treatment with low-molecular-weight heparin for cerebral sinus thrombosis. Stroke 1999, 30, 484–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coutinho, J.M.; Majoie, C.B.; Coert, B.A.; Stam, J. Decompressive hemicraniectomy in cerebral sinus thrombosis: Consecutive case series and review of the literature. Stroke 2009, 40, 2233–2235. [Google Scholar] [CrossRef] [Green Version]
- Neunert, C.; Terrell, D.R.; Arnold, D.M.; Buchanan, G.; Cines, D.B.; Cooper, N.; Cuker, A.; Despotovic, J.M.; George, J.N.; Grace, R.F.; et al. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv. 2019, 3, 3829–3866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warkentin, T.E. High-dose intravenous immunoglobulin for the treatment and prevention of heparin-induced thrombocytopenia: A review. Expert Rev. Hematol. 2019, 12, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.; Ness, P.M.; Takemoto, C.M.; Krishnamurti, L.; King, K.E.; Tobian, A.A. Platelet transfusions in platelet consumptive disorders are associated with arterial thrombosis and in-hospital mortality. Blood 2015, 125, 1470–1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, S.; Makris, M. The reversal of anticoagulation in clinical practice. Clin. Med. (Lond.) 2018, 18, 314–319. [Google Scholar] [CrossRef]
- Kuramatsu, J.B.; Sembill, J.A.; Gerner, S.T.; Sprugel, M.I.; Hagen, M.; Roeder, S.S.; Endres, M.; Haeusler, K.G.; Sobesky, J.; Schurig, J.; et al. Management of therapeutic anticoagulation in patients with intracerebral haemorrhage and mechanical heart valves. Eur. Heart J. 2018, 39, 1709–1723. [Google Scholar] [CrossRef] [PubMed]
- Guresir, E.; Vatter, H.; Schuss, P.; Oszvald, A.; Raabe, A.; Seifert, V.; Beck, J. Rapid closure technique in decompressive craniectomy. J. Neurosurg. 2011, 114, 954–960. [Google Scholar] [CrossRef] [PubMed]
- Jabbarli, R.; He, S.Q.; Darkwah Oppong, M.; Herten, A.; Chihi, M.; Pierscianek, D.; Dammann, P.; Sure, U.; Wrede, K.H. Size does matter: The role of decompressive craniectomy extent for outcome after aneurysmal subarachnoid hemorrhage. Eur. J. Neurol. 2021. [Google Scholar] [CrossRef]
- Borger, V.; Schuss, P.; Kinfe, T.M.; Vatter, H.; Guresir, E. Decompressive Craniectomy for Stroke: Early Cranioplasty Is a Predictor for Postoperative Complications. World Neurosurg. 2016, 92, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Schuss, P.; Vatter, H.; Marquardt, G.; Imohl, L.; Ulrich, C.T.; Seifert, V.; Guresir, E. Cranioplasty after decompressive craniectomy: The effect of timing on postoperative complications. J. Neurotrauma 2012, 29, 1090–1095. [Google Scholar] [CrossRef]
- Yun, S.H.; Sim, E.H.; Goh, R.Y.; Park, J.I.; Han, J.Y. Platelet Activation: The Mechanisms and Potential Biomarkers. Biomed. Res. Int. 2016, 2016, 9060143. [Google Scholar] [CrossRef] [Green Version]
- Vayne, C.; Rollin, J.; Gruel, Y.; Pouplard, C.; Galinat, H.; Huet, O.; Memier, V.; Geeraerts, T.; Marlu, R.; Pernod, G.; et al. PF4 Immunoassays in Vaccine-Induced Thrombotic Thrombocytopenia. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Platton, S.; Bartlett, A.; MacCallum, P.; Makris, M.; McDonald, V.; Singh, D.; Scully, M.; Pavord, S. Evaluation of laboratory assays for anti-Platelet Factor 4 antibodies after ChAdOx1 nCOV-19 vaccination. J. Thromb. Haemost. 2021. [Google Scholar] [CrossRef] [PubMed]
- Oldenburg, J.; Klamroth, R.; Langer, F.; Albisetti, M.; von Auer, C.; Ay, C.; Korte, W.; Scharf, R.E.; Potzsch, B.; Greinacher, A. Diagnosis and Management of Vaccine-Related Thrombosis following AstraZeneca COVID-19 Vaccination: Guidance Statement from the GTH. Hamostaseologie 2021. [Google Scholar] [CrossRef]
- American Heart Association/American Stroke Association Stroke Council, L. Diagnosis and Management of Cerebral Venous Sinus Thrombosis with Vaccine-Induced Thrombotic Thrombocytopenia. Stroke 2021. [Google Scholar] [CrossRef]
- Nagrebetsky, A.; Al-Samkari, H.; Davis, N.M.; Kuter, D.J.; Wiener-Kronish, J.P. Perioperative thrombocytopenia: Evidence, evaluation, and emerging therapies. Br. J. Anaesth. 2019, 122, 19–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Patient No. 1 | Patient No. 2 | Patient No. 3 | |
|---|---|---|---|
| SARS-CoV2-vaccine | ChAdOx1 nCoV-19 | ChAdOx1 nCoV-19 | Ad26.COV2.S |
| age (yrs) | 47 | 50 | 44 |
| sex | female | female | female |
| medical history | - | - | - |
| medication prior to ictus | - | - | - |
| platelet count (G/L) | 9 (NR 150–370) | 24 (NR 150–450) | 48 (NR 150–370) |
| time from vaccination to admission (days) | 12 days | 7 days | 10 days |
| time from admission to first brain imaging (min) | 15 min | 25 min | 21 min |
| PT | 10.7 s (NR 7.6–9.8) | - | 8.6 s (NR 7.6–9.8) |
| INR | 1.3 | 1.44 | 1.0 |
| activated partial thromboplastin time (aPTT) | 23.0 s (NR 25–35) | 28 s (NR 27–37) | 19.9 s (NR 25–35) |
| thrombin clotting time | 20.9 s (NR < 20.5) | - | 18.8 s (NR < 20.5) |
| fibrinogen | 128 mg/dL (NR 180–355) | 1.1 g/L (NR 1.8–3.5) | 294 mg/dL (NR 180–355) |
| roTEG R | 13 min (NR 8–16) | - | 12 min (NR 8–16) |
| roTEG K | >60 min (NR 3–10) | - | 10 min (NR 3–10) |
| roTEG ME | 12 (NR 80–150) | - | 52 (NR 80–150) |
| D-dimer | >35.2 mg/L (NR 0–0.5) | >35 mg/L (NR 0–0.5) | >35 mg/L (NR 0–0.5) |
| preoperative ventilator settings | APRV 18/10, 2.3 s/2.3 s, fiO2 30% | BIPAP 17/7, fiO2 50% | APRV 20/10, 2.5 s/2.5 s, fiO2 30% |
| preoperative pCO2 (mmHg) | 31.9 (NR 35–46) | 34.8 (NR 35–46) | 32.2 (NR 35–46) |
| time from admission to death (h) | 39 h | 49 h | 20 h |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gessler, F.; Schmitz, A.K.; Dubinski, D.; Bernstock, J.D.; Lehmann, F.; Won, S.-Y.; Wittstock, M.; Güresir, E.; Hadjiathanasiou, A.; Zimmermann, J.; et al. Neurosurgical Considerations Regarding Decompressive Craniectomy for Intracerebral Hemorrhage after SARS-CoV-2-Vaccination in Vaccine Induced Thrombotic Thrombocytopenia—VITT. J. Clin. Med. 2021, 10, 2777. https://doi.org/10.3390/jcm10132777
Gessler F, Schmitz AK, Dubinski D, Bernstock JD, Lehmann F, Won S-Y, Wittstock M, Güresir E, Hadjiathanasiou A, Zimmermann J, et al. Neurosurgical Considerations Regarding Decompressive Craniectomy for Intracerebral Hemorrhage after SARS-CoV-2-Vaccination in Vaccine Induced Thrombotic Thrombocytopenia—VITT. Journal of Clinical Medicine. 2021; 10(13):2777. https://doi.org/10.3390/jcm10132777
Chicago/Turabian StyleGessler, Florian, Ann Kristin Schmitz, Daniel Dubinski, Joshua D. Bernstock, Felix Lehmann, Sae-Yeon Won, Matthias Wittstock, Erdem Güresir, Alexis Hadjiathanasiou, Julian Zimmermann, and et al. 2021. "Neurosurgical Considerations Regarding Decompressive Craniectomy for Intracerebral Hemorrhage after SARS-CoV-2-Vaccination in Vaccine Induced Thrombotic Thrombocytopenia—VITT" Journal of Clinical Medicine 10, no. 13: 2777. https://doi.org/10.3390/jcm10132777