
Intranasal Dexmedetomidine Compared to a Combination of Intranasal Dexmedetomidine with Ketamine for Sedation of Children Requiring Dental Treatment: A Randomized Clinical Trial

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Setting
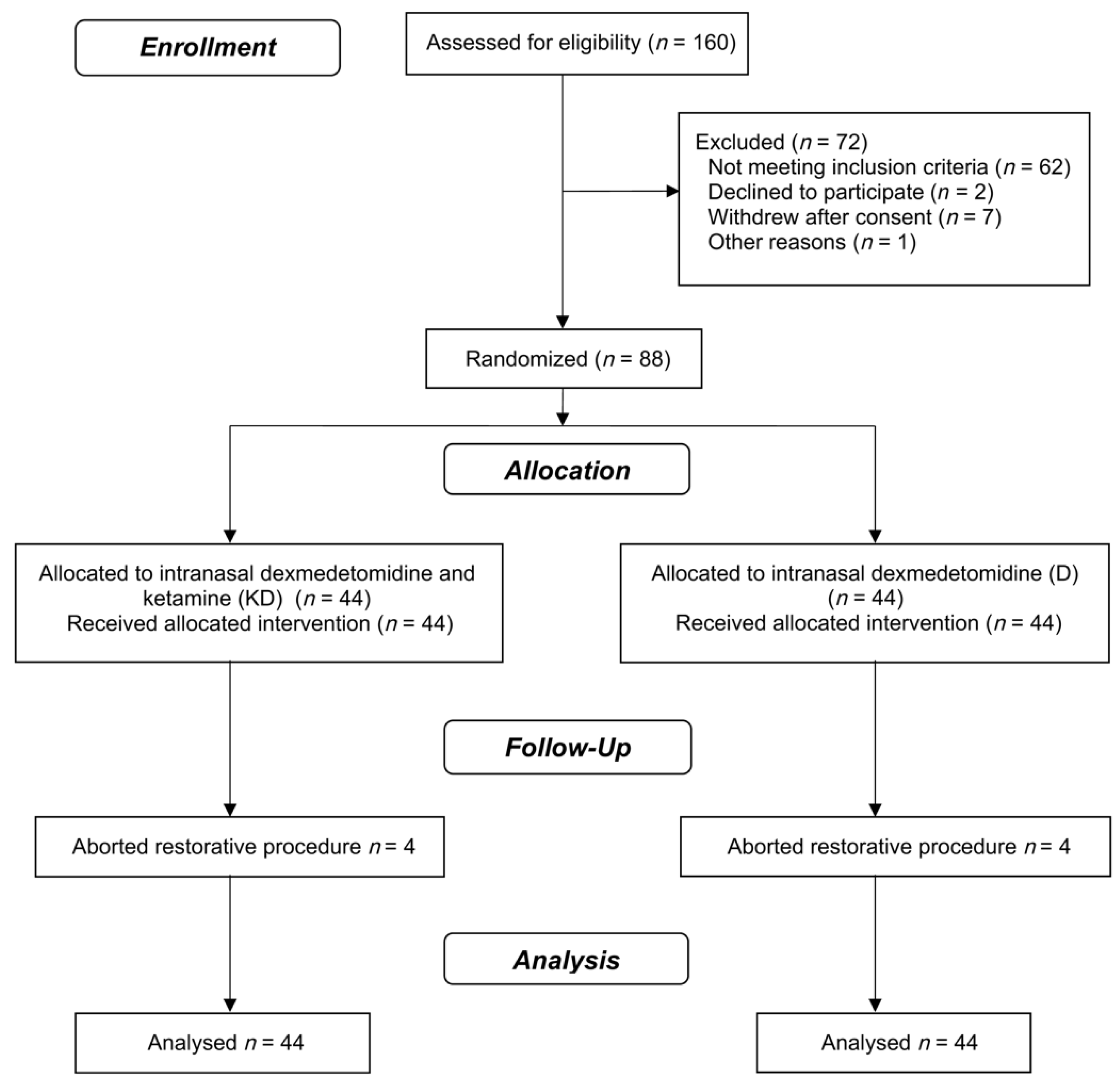
2.2. Randomization and Blinding
2.3. Interventions
2.4. Outcomes
2.4.1. Primary Outcome—Children’s Behavior
2.4.2. Secondary Outcomes—Parents’ and Dentists’ Satisfaction; Adverse Events and Recovery Time
2.5. Sample Size
2.6. Statistical Analysis
3. Results
3.1. Child Behavior
3.2. Parents and Operator Satisfaction during the Procedure
3.3. Adverse Events (AEs)
3.4. Recovery Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grisolia, B.M.; dos Santos, A.P.P.; D’Hyppolito, I.M.; Buchanan, H.; Hill, K.; Oliveira, B.H. Prevalence of dental anxiety in children and adolescents globally: A systematic review with meta-analyses. Int. J. Paediatr. Dent. 2021, 31, 168–183. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatric Dentistry. Behavior Guidance for the Pediatric Dental Patient. In The Reference Manual of Pediatric Dentistry; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2020; pp. 292–310. [Google Scholar]
- Rafique, S.; Banerjee, A.; Fiske, J. Management of the petrified dental patient. Dent. Update 2008, 35, 196–198. [Google Scholar] [CrossRef]
- Krauss, B.; Green, S.M. Procedural sedation and analgesia in children. Lancet 2006, 367, 766–780. [Google Scholar] [CrossRef]
- Chen, Z.; Lin, M.; Huang, Z.; Zeng, L.; Huang, L.; Yu, D.; Zhang, L. Efficacy of chloral hydrate oral solution for sedation in pediatrics: A systematic review and meta-analysis. Drug Des. Dev. Ther. 2019, 13, 2643–2653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashley, P.F.; Chaudhary, M.; Lourenço-Matharu, L. Sedation of children undergoing dental treatment. Cochrane Database Syst. Rev. 2018, 12, CD003877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCormack, L.; Chen, J.W.; Trapp, L.; Job, A. A comparison of sedation-related events for two multiagent oral sedation regimens in pediatric dental patients. Pediatr. Dent. 2014, 36, 302–308. [Google Scholar]
- Olacke, B.; Nelson, T.; Sarvas, E.; Scott, J.M. A retrospective study of dosing weight and outcomes for one pediatric dental sedation regimen. Pediatr Dent. 2018, 40, 346–351. [Google Scholar]
- Huang, A.; Tanbonliong, T. Oral sedation postdischarge adverse events in pediatric dental patients. Anesth. Prog. 2015, 62, 91–99. [Google Scholar] [CrossRef] [Green Version]
- Song, S.; Han, M.; Kim, J. Safety of chloral hydrate sedation in dental practice for children: An overview. J. Dent. Anesth. Pain Med. 2020, 20, 107–118. [Google Scholar] [CrossRef]
- Grissinger, M. Chloral hydrate: Is it still being used? Are there safer alternatives? Pharm. Ther. 2019, 44, 444–459. [Google Scholar]
- Ghajari, M.F.; Ansari, G.; Soleymani, A.A.; Shayeghi, S.; Ardakani, F.F. Comparison of Oral and Intranasal Midazolam/Ketamine Sedation in 3–6-year-old Uncooperative Dental Patients. J. Dent. Res. Dent. Clin. Dent. Prospect. 2015, 9, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Sado-Filho, J.; Viana, K.A.; Corrêa-Faria, P.; Costa, L.R.; Costa, P.S. Randomized clinical trial on the efficacy of intranasal or oral ketamine-midazolam combinations compared to oral midazolam for outpatient pediatric sedation. PLoS ONE 2019, 14, e0213074. [Google Scholar] [CrossRef]
- Oh, S.; Kingsley, K. Efficacy of ketamine in pediatric sedation dentistry: A systematic review. Compend. Contin. Educ. Dent. 2018, 39, e1–e4. [Google Scholar]
- Surendar, M.N.; Pandey, R.K.; Saksena, A.K.; Kumar, R.; Chandra, G. A comparative evaluation of intranasal dexmedetomidine, midazolam and ketamine for their sedative and analgesic properties: A triple blind randomized study. J. Clin. Pediatr. Dent. 2014, 38, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Krauss, B.; Green, S.M. Sedation and analgesia for procedures in children. N. Engl. J. Med. 2000, 342, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Green, S.M.; Roback, M.G.; Kennedy, R.M.; Krauss, B. Clinical Practice Guideline for Emergency Department Ketamine Dissociative Sedation: 2011 Update. Ann. Emerg. Med. 2011, 57, 449–461. [Google Scholar] [CrossRef]
- Kuga, S.; Maeda, T.; Ihara, K. Pediatric procedural sedation in Japan: A single-facility study of 1436 cases. Pediatr. Int. 2020, 62, 1346–1350. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.L.; Tham, L.P. Incidence and predictors of respiratory adverse events in children undergoing procedural sedation with intramuscular ketamine in a paediatric emergency department. Singap. Med. J. 2020. [Google Scholar] [CrossRef]
- Tobias, J.D. Dexmedetomidine and ketamine: An effective alternative for procedural sedation? Pediatr. Crit. Care Med. 2012, 13, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Qian, B.; Zheng, W.; Shi, J.; Chen, Z.; Guo, Y.; Yao, Y. Ketamine enhances intranasal dexmedetomidine-induced sedation in children: A randomized, double-blind trial. Drug Des. Dev. Ther. 2020, 14, 3559–3565. [Google Scholar] [CrossRef]
- Poonai, N.; Spohn, J.; VanderMeer, B.; Ali, S.; Bhatt, M.; Hendrikx, S.; Trottier, E.D.; Sabhaney, V.; Shah, A.; Joubert, G.; et al. Intranasal dexmedetomidine for procedural distress in children: A systematic review. Pediatrics 2020, 145, e20191623. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, P.U.; Thakur, S.; Singhal, P.; Chauhan, D.; Jayam, C.; Sood, R.; Malhotra, Y. Comparative evaluation of dexmedetomidine and midazolam-ketamine combination as sedative agents in pediatric dentistry: A double-blinded randomized controlled trial. Contemp. Clin. Dent. 2016, 7, 186–192. [Google Scholar] [CrossRef]
- Jaikaria, A.; Thakur, S.; Singhal, P.; Chauhan, D.; Jayam, C.; Syal, K. A comparison of oral midazolam-ketamine, dexmedetomidine-fentanyl and dexmedetomidine-ketamine combinations as sedative agents in pediatric dentistry: A triple-blinded randomized controlled trial. Contemp. Clin. Dent. 2018, 9, S197–S203. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. PLoS Med. 2010, 7, e1000251. [Google Scholar] [CrossRef]
- Frankl, S.; Shiere, F.; Fogels, H. Should the parent remain with the child in the dental operatory? J. Dent. Child. 1962, 29, 150–163. [Google Scholar]
- Mallampati, S.R.; Gatt, S.P.; Gugino, L.D.; Desai, S.P.; Waraksa, B.; Freiberger, D.; Liu, P.L. A clinical sign to predict difficult tracheal intubation: A prospective study. Can. Anesth. Soc. J. 1985, 32, 426–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coté, C.J.; Wilson, S.; American Academy of Pediatric Dentistry; American Academy of Pediatrics. Guidelines for monitoring and management of pediatric patients before, during, and after sedation for diagnostic and therapeutic procedures. Pediatr. Dent. 2019, 41, 26E–52E. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, F.; Wulf, H.; Gruber, M.; Biallas, R. S-ketamine and s-norketamine plasma concentrations after nasal and i.v. administration in anesthetized children. Paediatr. Anaesth. 2004, 14, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Iirola, T.; Vilo, S.; Manner, T.; Aantaa, R.; Lahtinen, M.; Scheinin, M.; Olkkola, K.T. Bioavailability of dexmedetomidine after intranasal administration. Eur. J. Clin. Pharmacol. 2011, 67, 825–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramsay, M.A.E.; Savege, T.M.; Simpson, B.R.J.; Goodwin, R. Controlled Sedation with Alphaxalone-Alphadolone. BMJ 1974, 22, 656–659. [Google Scholar] [CrossRef] [Green Version]
- American Society of Anesthesiologists. Continuum of Depth of Sedation: Definition of General Anesthesia and Levels of Sedation/Analgesia. Available online: https://www.asahq.org/standards-and-guidelines/continuum-of-depth-of-sedation-definition-of-general-anesthesia-and-levels-of-sedationanalgesia (accessed on 25 June 2021).
- American Society of Anesthesiologists. Practice guidelines for moderate procedural sedation and analgesia 2018: A report by the American Society of Anesthesiologists Task Force on Moderate Procedural Sedation and Analgesia, the American Association of Oral and Maxillofacial Surgeons, American College of Radiology, American Dental Association, American Society of Dentist Anesthesiologists, and Society of Interventional Radiology. Anesthesiology 2018, 128, 437–479. [Google Scholar] [CrossRef] [Green Version]
- Leal, S.; Bonifacio, C.; Raggio, D.; Frencken, J. Atraumatic restorative treatment: Restorative component. Monogr. Oral Sci. 2018, 27, 92–102. [Google Scholar] [CrossRef]
- Lochary, M.E.; Wilson, S.; Griffen, A.L.; Coury, D.L. Temperament as a predictor of behavior for conscious sedation in dentistry. Pediatr. Dent. 1993, 15, 348–352. [Google Scholar]
- Theriot, A.L.; Gomez, L.; Chang, C.T.; Badger, G.R.; Herbert, A.K.; Cardenas Vasquez, J.M.; Cardenas, A.D.; Chiquet, B.T. Ethnic and language influence on parents’ perception of paediatric behaviour management techniques. Int. J. Paediatr. Dent. 2019, 29, 301–309. [Google Scholar] [CrossRef]
- Rodrigues, V.B.M.; Costa, L.R.; de Faria, P.C. Parents’ satisfaction with paediatric dental treatment under sedation: A cross-sectional study. Int. J. Paediatr. Dent. 2021, 31, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Roback, M.G.; Green, S.M.; Andolfatto, G.; Leroy, P.L.; Mason, K.P. Tracking and reporting outcomes of procedural sedation (TROOPS): Standardized quality improvement and research tools from the International Committee for the Advancement of Procedural Sedation. Br. J. Anaesth. 2018, 120, 164–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, K.P.; Green, S.M.; Piacevoli, Q.; International Sedation Task Force. Adverse event reporting tool to standardize the reporting and tracking of adverse events during procedural sedation: A consensus document from the World SIVA International Sedation Task Force. Br. J. Anaesth. 2012, 108, 13–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, L.R.; Costa, P.S.; Brasileiro, S.V.; Bendo, C.B.; Viegas, C.M.; Paiva, S.M. Post-discharge adverse events following pediatric sedation with high doses of oral medication. J. Pediatr. 2012, 160, 807–813. [Google Scholar] [CrossRef]
- Zanaty, O.M.; EL Metainy, A.S. A comparative evaluation of nebulized dexmedetomidine, nebulized ketamine, and their combination as premedication for outpatient pediatric dental surgery. Anesth. Analg. 2015, 121, 167–171. [Google Scholar] [CrossRef]
- Miller, J.W.; Ding, L.; Gunter, J.B.; Lam, J.E.; Lin, E.P.; Paquin, J.R.; Li, B.L.; Spaeth, J.P.; Kreeger, R.N.; Divanovic, A.; et al. Comparison of Intranasal Dexmedetomidine and Oral Pentobarbital Sedation for Transthoracic Echocardiography in Infants and Toddlers: A Prospective, Randomized, Double-Blind Trial. Anesth. Analg. 2018, 126, 2009–2016. [Google Scholar] [CrossRef]
- Gan, X.; Lin, H.; Chen, J.; Lin, Z.; Lin, Y.; Chen, W. Rescue sedation with intranasal dexmedetomidine for pediatric ophthalmic examination after chloral hydrate failure: A randomized, controlled trial. Clin. Ther. 2016, 38, 1522–1529. [Google Scholar] [CrossRef] [PubMed]
- Cao, Q.; Lin, Y.; Xie, Z.; Shen, W.; Chen, Y.; Gan, X.; Liu, Y. Comparison of sedation by intranasal dexmedetomidine and oral chloral hydrate for pediatric ophthalmic examination. Pediatr. Anesth. 2017, 27, 629–636. [Google Scholar] [CrossRef]
- Li, B.L.; Yuen, V.M.; Zhou, J.L.; Zhang, N.; Huang, J.X.; Tian, H.; Song, X.R. A randomized controlled trial of oral chloral hydrate vs intranasal dexmedetomidine plus buccal midazolam for auditory brainstem response testing in children. Paediatr. Anaesth. 2018, 28, 1022–1028. [Google Scholar] [CrossRef]
- Voutilainen, A.; Pitkäaho, T.; Kvist, T.; Vehviläinen-Julkunen, K. How to ask about patient satisfaction? The visual analogue scale is less vulnerable to confounding factors and ceiling effect than a symmetric Likert scale. J. Adv. Nurs. 2016, 72, 946–957. [Google Scholar] [CrossRef] [PubMed]
- Hagan, P.P.; Hagan, J.P.; Fields, H.W., Jr.; Machen, J.B. The legal status of informed consent for behavior management techniques in pediatric dentistry. Pediatr. Dent. 1984, 6, 204–208. [Google Scholar]
- Yee, R.; Jones, L.M.; Hosey, M.T. What the child “SAID” to the dentist: A UK randomized controlled trial. Child. Care Health Dev. 2017, 43, 926–932. [Google Scholar] [CrossRef] [PubMed]
- Poonai, N.; Canton, K.; Ali, S.; Hendrikx, S.; Shah, A.; Miller, M.; Joubert, G.; Rieder, M.; Hartling, L. Intranasal ketamine for procedural sedation and analgesia in children: A systematic review. PLoS ONE 2017, 12, e0173253. [Google Scholar] [CrossRef]
- Homer, T.; Maguire, A.; Douglas, G.V.A.; Innes, N.P.; Clarkson, J.E.; Wilson, N.; Ryan, V.; McColl, E.; Robertson, M.; Vale, L. Cost-effectiveness of child caries management: A randomised controlled trial (FiCTION trial). BMC Oral Health 2020, 20, 1–8. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Treatment Group | |
|---|---|---|
| Dexmedetomidine-Ketamine | Dexmedetomidine | |
| Participants | ||
| Sex n = 88; n (%) | ||
| Male | 24 (48.0) | 26 (52.0) |
| Female | 20 (52.6) | 18 (47.4) |
| Age (months) n = 88; median (25th percentile; 75th percentile) | 36.5 (27.2–51.2) | 48.0 (31.2–55.7) |
| Weight (kg) n = 88; median (25th percentile; 75th percentile) | 14.5 (13.0–16.4) | 16.3 (13.6–18.8) |
| ASA* n = 88; n (%) | ||
| I | 42 (50.0%) | 42 (50.0%) |
| II | 2 (50.0%) | 2 (50.0%) |
| Heart rate n = 88; median (25th percentile; 75th percentile) | 113.0 (99.0–124.0) | 111.5 (99.2–119.7) |
| Oxygen saturation n = 88; median (25th percentile; 75th percentile) | 98.0 (97.0–99.0) | 98.0 (97.0–99.0) |
| Oral condition and treatment | ||
| Caries experience n = 88; mean (standard deviation) | 7.5 (3.5) | 8.4 (3.4) |
| Physical restraint during the dental procedure, n = 80; n (%) | ||
| No | 17 (42.5%) | 16 (40.0%) |
| Yes | 23 (57.5%) | 24 (60.0%) |
| Number of teeth restored n = 80; median (25th percentile; 75th percentile) | 2 (1.2–4.7) | 2 (1.0–3.0) |
| Sedation | ||
| Time for onset of sedative action, median (25th percentile–75th percentile) | 44.0 (38.0–47.7) | 45.0 (39.0–50.0) |
| Duration of session under sedation, median (25th percentile–75th percentile) | 25.0 (14.7–41.0) | 26.0 (16.2–45.7) |
| Postanesthetic recovery time, median (25th percentile–75th percentile) | 62.5 (41.0–77.5) | 36.5 (30.0–45.5) |
| Adverse events | ||
| No | 32 (80.0%) | 34 (85.0%) |
| Yes | 8 (20.0%) | 6 (15.0%) |
| Level of sedation | ||
| Minimal sedation | 13 (29.5%) | 20 (45.5%) |
| Moderate sedation | 27 (61.4%) | 23 (52.3%) |
| Deep sedation | 4 (9.1%) | 1 (2.2%) |
| DK | D | p-Value * | p-Value ** | p-Value *** | |
|---|---|---|---|---|---|
| Mean (Standard Deviation) | |||||
| Primary outcome | |||||
| Quiet behavior (%) | 58.4 (38.1) | 55.2 (39.1) | 0.225 | 0.35 | 0.33 |
| Secondary outcomes | |||||
| Parents’ satisfaction (0–100) | 78.0 (32.2) | 72.7 (35.1) | 0.203 | 0.212 | 0.136 |
| Dentists’ satisfaction (0–100) | 62.7 (41.0) | 62.8 (40.1) | 0.339 | 0.502 | 0.503 |
| Adverse events n (%) | 0.104 | 0.273 | N/A | ||
| No | 34 (47.2) | 38 (52.8) | |||
| Yes | 10 (62.5) | 6 (37.5) | |||
| Recovery time, minutes | 61.0 (25.6) | 44.4 (23.6) | 0.012 | 0.003 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sado-Filho, J.; Corrêa-Faria, P.; Viana, K.A.; Mendes, F.M.; Mason, K.P.; Costa, L.R.; Costa, P.S. Intranasal Dexmedetomidine Compared to a Combination of Intranasal Dexmedetomidine with Ketamine for Sedation of Children Requiring Dental Treatment: A Randomized Clinical Trial. J. Clin. Med. 2021, 10, 2840. https://doi.org/10.3390/jcm10132840
Sado-Filho J, Corrêa-Faria P, Viana KA, Mendes FM, Mason KP, Costa LR, Costa PS. Intranasal Dexmedetomidine Compared to a Combination of Intranasal Dexmedetomidine with Ketamine for Sedation of Children Requiring Dental Treatment: A Randomized Clinical Trial. Journal of Clinical Medicine. 2021; 10(13):2840. https://doi.org/10.3390/jcm10132840
Chicago/Turabian StyleSado-Filho, Joji, Patrícia Corrêa-Faria, Karolline A. Viana, Fausto M. Mendes, Keira P. Mason, Luciane R. Costa, and Paulo S. Costa. 2021. "Intranasal Dexmedetomidine Compared to a Combination of Intranasal Dexmedetomidine with Ketamine for Sedation of Children Requiring Dental Treatment: A Randomized Clinical Trial" Journal of Clinical Medicine 10, no. 13: 2840. https://doi.org/10.3390/jcm10132840
APA StyleSado-Filho, J., Corrêa-Faria, P., Viana, K. A., Mendes, F. M., Mason, K. P., Costa, L. R., & Costa, P. S. (2021). Intranasal Dexmedetomidine Compared to a Combination of Intranasal Dexmedetomidine with Ketamine for Sedation of Children Requiring Dental Treatment: A Randomized Clinical Trial. Journal of Clinical Medicine, 10(13), 2840. https://doi.org/10.3390/jcm10132840