
Find Me If You Can: First Clinical Experience Using the Novel CARTOFINDER Algorithm in a Routine Workflow for Atrial Fibrillation Ablation

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. CARTOFINDER Analysis
2.2. Ablation Procedure
2.3. Ultra High Density Mapping
2.4. Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Procedural Data
3.3. Ablation Effect and Stability of ROIs over Time
3.4. Follow-Up Data and Complications
4. Discussion
4.1. Major Findings
4.2. Benefits of CARTOFINDER Mapping in Persistent AF
4.3. Regions of Interest—New Targets for AF Ablation
4.4. Can CARTOFINDER Mapping Identify Responder to LAA Isolation?
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Watkins, C.L. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart. J. 2021, 42, 373–498. [Google Scholar] [PubMed]
- Marrouche, N.F.; Wilber, D.; Hindricks, G.; Jais, P.; Akoum, N.; Marchlinski, F.; Brachmann, J. Association of atrial tissue fibrosis identified by delayed enhancement MRI and atrial fibrillation catheter ablation: The DECAAF study. JAMA 2014, 311, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Sohns, C.; Zintl, K.; Zhao, Y.; Dagher, L.; Andresen, D.; Siebels, J.; Wegscheider, K.; Sehner, S.; Boersma, L.; Merkely, B.; et al. Impact of left ventricular function and heart failure symptoms on outcomes post ablation of atrial fibrillation in heart failure: CASTLE-AF trial. Circ. Arrhythm. Electrophysiol. 2020, 13, e008461. [Google Scholar] [CrossRef] [PubMed]
- Nattel, S.; Sager, P.; Huser, J.; Heijman, J.; Dobrev, D. Why translation from basic discoveries to clinical applications is so difficult for atrial fibrillation and possible approaches to improving it. Cardiovasc. Res. 2021, 7, 1609–1611. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.S.; Hocini, M.; Dubois, R.; Denis, A.; Derval, N.; Zellerhoff, S.; Yamashita, S.; Berte, B.; Mahida, S.; Komatsu, Y.; et al. Complexity and Distribution of Drivers in Relation to Duration of Persistent Atrial Fibrillation. J. Am. Coll. Cardiol. 2017, 69, 1257–1269. [Google Scholar] [CrossRef] [PubMed]
- Narayan, S.M.; Krummen, D.E.; Shivkumar, K.; Clopton, P.; Rappel, W.J.; Miller, J.M. Treatment of atrial fibrillation by the ablation of localized sources: CONFIRM (conventional ablation for atrial fibrillation with or without focal impulse and rotor modulation) trial. J. Am. Coll. Cardiol. 2012, 60, 628–636. [Google Scholar]
- Sohns, C.; Lemes, C.; Metzner, A.; Fink, T.; Chmelevsky, M.; Maurer, T.; Budanova, M.; Solntsev, V.; Schulze, W.H.; Staab, W.; et al. First-in-man analysis of the relationship between electrical rotors from noninvasive panoramic mapping and atrial fibrosis from magnetic resonance imaging in patients with persistent atrial fibrillation. Circ. Arrhythm. Electrophysiol. 2017, 10, e0004419. [Google Scholar] [CrossRef] [PubMed]
- Quintanilla, J.G.; Shpun, S.; Jalife, J.; Filgueiras-Rama, D. Novel approaches to mechanism-based atrial fibrillation ablation. Cardiovasc. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Knecht, S.; Sohal, M.; Deisenhofer, I.; Albenque, J.P.; Arentz, T.; Neumann, T.; Cauchemez, B.; Duytschaever, M.; Ramoul, K.; Verbeet, T.; et al. Multicentre evaluation of non-invasive biatrial mapping for persistent atrial fibrillation ablation: The AFACART study. Europace 2017, 19, 1302–1309. [Google Scholar] [CrossRef] [PubMed]
- Cochet, H.; Dubois, R.; Yamashita, S.; Al Jefairi, N.; Berte, B.; Sellal, J.M.; Hooks, D.; Frontera, A.; Amraoui, S.; Zemoura, A.; et al. Relationship between fibrosis detected on late gadolinium-enhanced cardiac magnetic resonance and re-entrant activity assessed with electrocardiographic imaging in human persistent atrial fibrillation. JACC Clin. Electrophysiol. 2018, 4, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Honarbakhsh, S.; Schilling, R.J.; Dhillon, G.; Ullah, W.; Keating, E.; Providencia, R.; Chow, A.; Earley, M.J.; Hunter, R.J. A novel mapping system for panoramic mapping of the left atrium: Application to detect and characterize localized sources maintaining atrial fibrillation. JACC Clin. Electrophysiol. 2018, 4, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Honarbakhsh, S.; Schilling, R.J.; Providencia, R.; Keating, E.; Sporton, S.; Lowe, M.; Lambiase, P.D.; Chow, A.; Earley, M.J.; Hunter, R.J. Automated detection of repetitive focal activations in persistent atrial fibrillation: Validation of a novel detection algorithm and application through panoramic and sequential mapping. J. Cardiovasc. Electrophysiol. 2019, 30, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Daoud, E.G.; Zeidan, Z.; Hummel, J.D.; Weiss, R.; Houmsse, M.; Augostini, R.; Kalbfleisch, S.J. Identification of repetitive activation patterns using novel computational analysis of multielectrode recordings during atrial fibrillation and flutter in humans. JACC Clin. Electrophysiol. 2017, 3, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Baykaner, T.; Rogers, A.J.; Meckler, G.L.; Zaman, J.; Navara, R.; Rodrigo, M.; Alhusseini, M.; Kowalewski, C.A.B.; Viswanathan, M.N.; Narayan, S.M.; et al. Clinical implications of ablation of drivers for atrial fibrillation: A systematic review and meta-analysis. Circ. Arrhythm. Electrophysiol. 2018, 11, e006119. [Google Scholar] [CrossRef] [PubMed]
- Romero, J.; Gabr, M.; Alviz, I.; Briceno, D.; Diaz, J.C.; Rodriguez, D.; Patel, K.; Polanco, D.; Trivedi, C.; Mohanty, S.; et al. Focal impulse and rotor modulation guided ablation versus pulmonary vein isolation for atrial fibrillation: A meta-analysis of head-to-head comparative studies. J. Cardiovasc. Electrophysiol. 2021. [Google Scholar] [CrossRef]
- Hansen, B.J.; Zhao, J.; Csepe, T.A.; Moore, B.T.; Li, N.; Jayne, L.A.; Kalyanasundaram, A.; Lim, P.; Bratasz, A.; Powell, K.A.; et al. Atrial fibrillation driven by micro-anatomic intramural re-entry revealed by simultaneous sub-epicardial and sub-endocardial optical mapping in explanted human hearts. Eur. Heart J. 2015, 36, 2390–2401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahid, S.; Cochet, H.; Boyle, P.M.; Schwarz, E.L.; Whyte, K.N.; Vigmond, E.J.; Dubois, R.; Hocini, M.; Haïssaguerre, M.; Jaïs, P.; et al. Patient-derived models link re-entrant driver localization in atrial fibrillation to fibrosis spatial pattern. Cardiovasc. Res. 2016, 110, 443–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sim, I.; Razeghi, O.; Karim, R.; Chubb, H.; Whitaker, J.; O’Neill, L.; Mukherjee, R.K.; Roney, C.H.; Razavi, R.; Wright, M.; et al. Reproducibility of atrial fibrosis assessment using CMR imaging and an open source platform. JACC Cardiovasc. Imag. 2019, 12, 2076–2077. [Google Scholar] [CrossRef] [PubMed]
- Di Biase, L.; Mohanty, P.; Mohanty, S.; Santangeli, P.; Trivedi, C.; Lakkireddy, D.; Reddy, M.; Jais, P.; Themistoclakis, S.; Dello Russo, A. Ablation Versus Amiodarone for Treatment of Persistent Atrial Fibrillation in Patients with Congestive Heart Failure and an Implanted Device: Results From the AATAC Multicenter Randomized Trial. Circulation 2016, 133, 1637–1644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, Y.; Akiyoshi, K.; Sekigawa, M.; Yagishita, A.; Yamamoto, T.; Maeda, S.; Kawabata, M.; Goya, M.; Hirao, K.; Sasano, T. Endocardial contact mapping of the left atrial appendage in persistent atrial fibrillation. J. Cardiovasc. Electrophysiol. 2020, 31, 112–118. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Patients; n = 50 |
|---|---|
| Age (y) | 67 ± 11 |
| Male sex (%) | 25 (50%) |
| BMI (kg/m2) | 29.5 ± 5.4 |
| LAD (mm) | 46 ± 7 |
| AF-Duration (months) | 30 ± 25 |
| CHA2DS2-VASc-Score | 2.9 ± 1.6 |
| Hypertension (%) | 37 (74%) |
| Diabetes (%) | 7 (14%) |
| Prior stroke (%) | 10 (20%) |
| Heart failure (%) | 20 (40%) |
| LVEF (%) | 52 ± 5 |
| Drug therapy | |
| Antiarrhythmic drugs | 10 (20%) |
| Beta-blocker | 39 (78%) |
| ACE-Inhibitor | 39 (78%) |
| Statin | 22 (44%) |
| Anticoagulation | 50 (100%) |
| Phenprocoumon | 5 (10%) |
| DOAC | 45 (90%) |
| Amount of fibrosis * | |
| 0–10% | 2 (4%) |
| 10–20% | 2 (4%) |
| 20–30% | 17 (34%) |
| > 30% | 29 (58%) |
| Parameter | Patients; n = 50 |
|---|---|
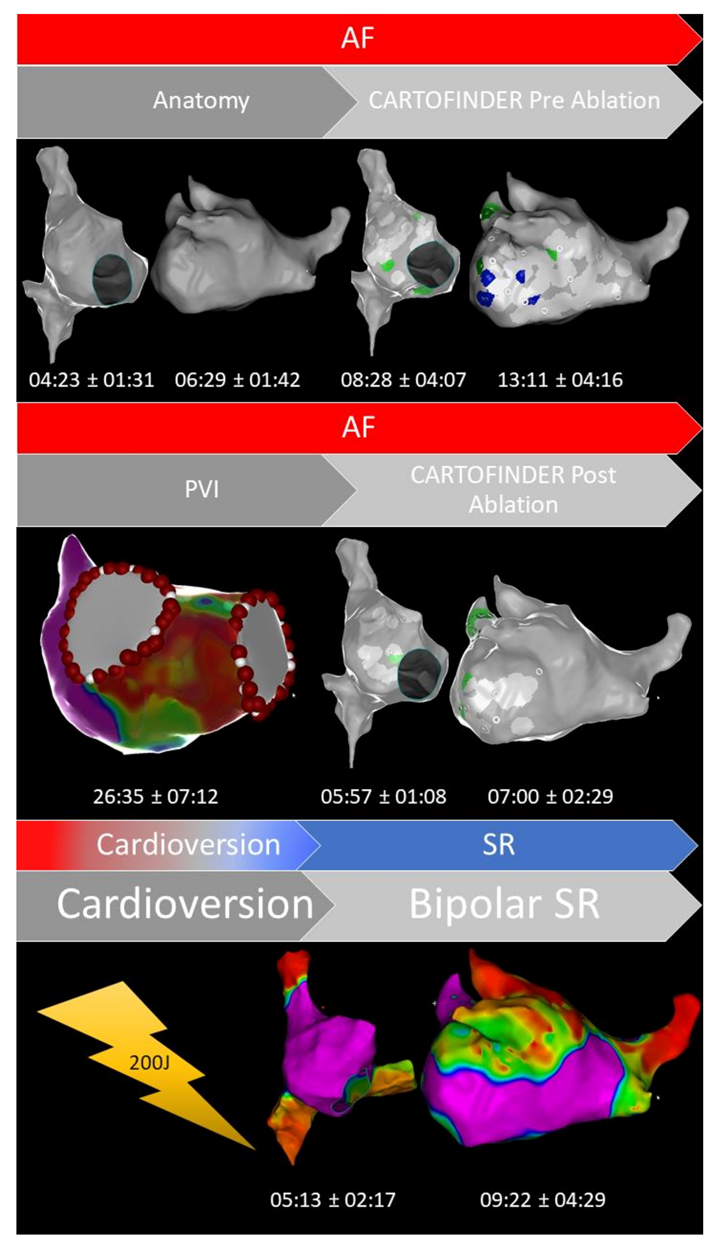
| Fluoroscopy time (min:s) | 08:34 ± 04:32 |
| Radiation dose (yGym2) | 905 ± 763 |
| Procedure time (min) | 134 ± 29 |
| Anatomical reconstruction; RA (min:s) | 04:23 ± 01:31 |
| Anatomical reconstruction; LA (min:s) | 06:29 ± 01:42 |
| CARTOFINDER mapping; RA (min:s) | 08:28 ± 04:07 |
| CARTOFINDER mapping; LA (min:s) | 13:11 ± 04:16 |
| Ablation time (min:s) | 26:35 ± 07:12 |
| Repeat CARTOFINDER mapping; RA (min:s) | 05:57 ± 01:08 |
| Repeat CARTOFINDER mapping; LA (min:s) | 07:00 ± 02:29 |
| High-density mapping bipolar voltage; RA (min:s) | 05:13 ± 02:17 |
| High-density mapping bipolar voltage; LA (min:s) | 09:22 ± 04:29 |
| ROIs from CARTOFINDER pre-ablation; LA (n) | 45 ± 33 |
| ROIs from CARTOFINDER pre-ablation; RA (n) | 32 ± 19 |
| Mapping points for bipolar voltage; LA (n) | 2156 ± 1169 |
| Mapping points for bipolar voltage; RA (n) | 1564 ± 879 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Unland, R.; Bergau, L.; El Hamriti, M.; Guckel, D.; Piran, M.; Fink, T.; Sciacca, V.; Köerperich, H.; Chmelevsky, M.; Imnadze, G.; et al. Find Me If You Can: First Clinical Experience Using the Novel CARTOFINDER Algorithm in a Routine Workflow for Atrial Fibrillation Ablation. J. Clin. Med. 2021, 10, 2979. https://doi.org/10.3390/jcm10132979
Unland R, Bergau L, El Hamriti M, Guckel D, Piran M, Fink T, Sciacca V, Köerperich H, Chmelevsky M, Imnadze G, et al. Find Me If You Can: First Clinical Experience Using the Novel CARTOFINDER Algorithm in a Routine Workflow for Atrial Fibrillation Ablation. Journal of Clinical Medicine. 2021; 10(13):2979. https://doi.org/10.3390/jcm10132979
Chicago/Turabian StyleUnland, Robin, Leonard Bergau, Mustapha El Hamriti, Denise Guckel, Misagh Piran, Thomas Fink, Vanessa Sciacca, Hermann Köerperich, Mikhail Chmelevsky, Guram Imnadze, and et al. 2021. "Find Me If You Can: First Clinical Experience Using the Novel CARTOFINDER Algorithm in a Routine Workflow for Atrial Fibrillation Ablation" Journal of Clinical Medicine 10, no. 13: 2979. https://doi.org/10.3390/jcm10132979
APA StyleUnland, R., Bergau, L., El Hamriti, M., Guckel, D., Piran, M., Fink, T., Sciacca, V., Köerperich, H., Chmelevsky, M., Imnadze, G., Khalaph, M., Braun, M., Sommer, P., & Sohns, C. (2021). Find Me If You Can: First Clinical Experience Using the Novel CARTOFINDER Algorithm in a Routine Workflow for Atrial Fibrillation Ablation. Journal of Clinical Medicine, 10(13), 2979. https://doi.org/10.3390/jcm10132979