
Hospitalisation for Drug Infusion Did Not Increase Levels of Anxiety and the Risk of Disease Relapse in Patients with Inflammatory Bowel Disease during COVID-19 Outbreak

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
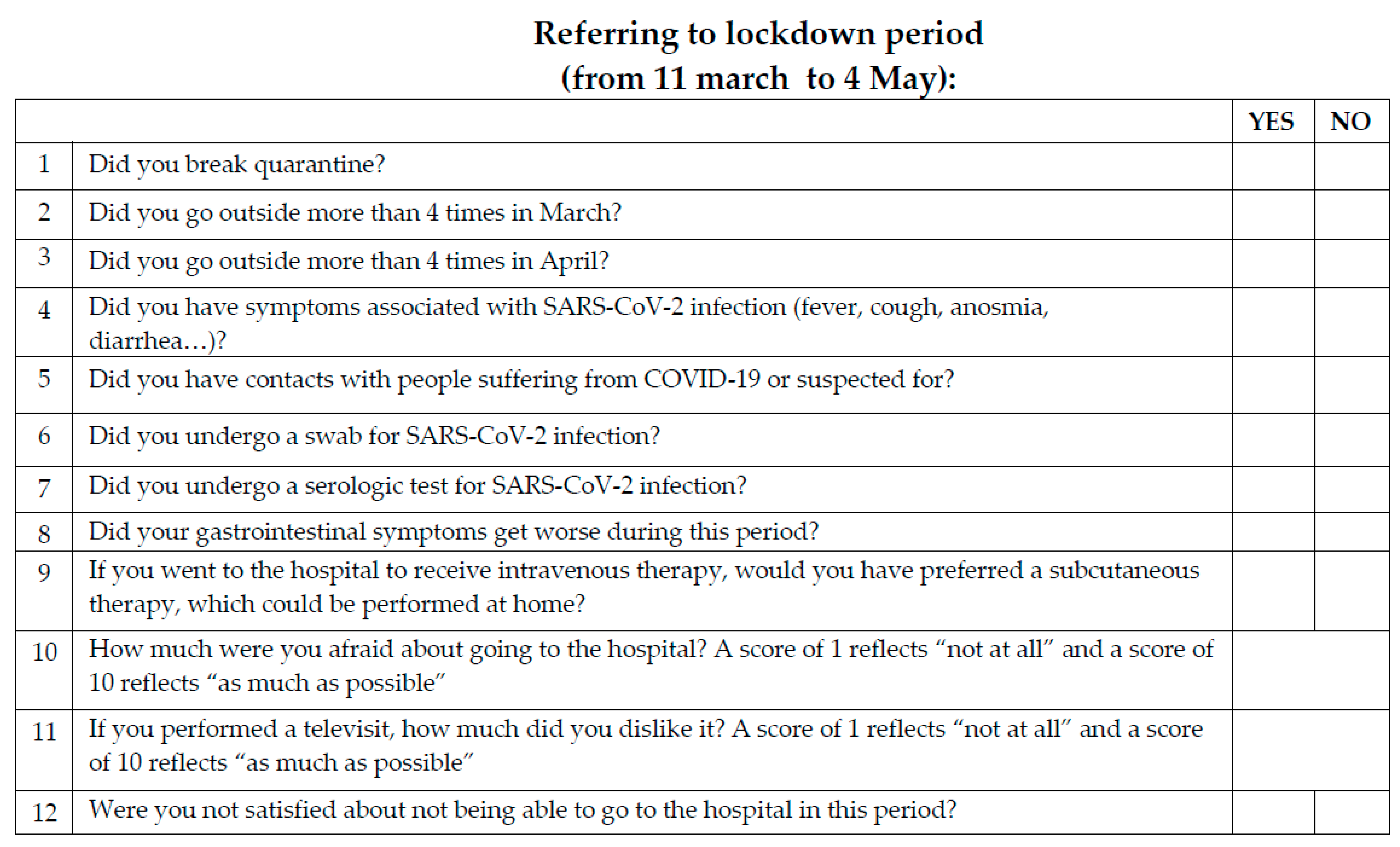
2.1. Patients and Study Protocol
2.2. Statistical Analysis
2.3. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coronavirus Resource Center. Coronavirus COVID-19 Global Cases. Available online: https://coronavirus.jhu.edu/map.html (accessed on 15 March 2021).
- Giusti, L.; Salza, A.; Mammarella, S.; Bianco, D.; Ussorio, D.; Casacchia, M.; Roncone, R. #Everything Will Be Fine. Duration of Home Confinement and “All-or-Nothing” Cognitive Thinking Style as Predictors of Traumatic Distress in Young University Students on a Digital Platform during the COVID-19 Italian Lockdown. Front. Psychiatry 2020, 11, 574812. [Google Scholar] [CrossRef]
- Tuccori, M.; Convertino, I.; Ferraro, S.; Cappello, E.; Valdiserra, G.; Focosi, D.; Blandizzi, C. The Impact of the COVID-19 “Infodemic” on Drug-Utilization Behaviors: Implications for Pharmacovigilance. Drug Saf. 2020, 43, 699–709. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Ungaro, R.; Mehandru, S.; Allen, P.B.; Peyrin-Biroulet, L.; Colombel, J.F. Ulcerative colitis. Lancet 2017, 389, 1756–1770. [Google Scholar] [CrossRef]
- Barberio, B.; Zamani, M.; Black, C.J.; Savarino, E.V.; Ford, A.C. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2021. [Google Scholar] [CrossRef]
- Marinelli, C.; Savarino, E.; Inferrera, M.; Lorenzon, G.; Rigo, A.; Ghisa, M.; Facchin, S.; D’Inca, R.; Zingone, F. Factors Influencing Disability and Quality of Life during Treatment: A Cross-Sectional Study on IBD Patients. Gastroenterol. Res. Pract. 2019, 2019, 5354320. [Google Scholar] [CrossRef]
- Sun, Y.; Li, L.; Xie, R.; Wang, B.; Jiang, K.; Cao, H. Stress Triggers Flare of Inflammatory Bowel Disease in Children and Adults. Front. Pediatr. 2019, 7, 432. [Google Scholar] [CrossRef]
- Wintjens, D.S.J.; de Jong, M.J.; van der Meulen-de Jong, A.E.; Romberg-Camps, M.J.; Becx, M.C.; Maljaars, J.P.; van Bodegraven, A.A.; Mahmmod, N.; Markus, T.; Haans, J.; et al. Novel Perceived Stress and Life Events Precede Flares of Inflammatory Bowel Disease: A Prospective 12-Month Follow-Up Study. J. Crohn’s Colitis 2019, 13, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Barberio, B.; Segal, J.P.; Quraishi, M.N.; Black, C.J.; Savarino, E.V.; Ford, A.C. Efficacy of Oral, Topical, or Combined Oral and Topical 5-Aminosalicylates, in Ulcerative Colitis: Systematic Review and Network Meta-Analysis. J. Crohn’s Colitis 2021. [Google Scholar] [CrossRef] [PubMed]
- Beaugerie, L.; Kirchgesner, J. Balancing Benefit vs. Risk of Immunosuppressive Therapy for Individual Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2019, 17, 370–379. [Google Scholar] [CrossRef]
- Long, M.D.; Martin, C.; Sandler, R.S.; Kappelman, M.D. Increased risk of pneumonia among patients with inflammatory bowel disease. Am. J. Gastroenterol. 2013, 108, 240–248. [Google Scholar] [CrossRef] [Green Version]
- Barberio, B.; Zingone, F.; D’Inca, R.; Rovigo, L.; Bertani, L.; Bodini, G.; Ghisa, M.; Gubbiotti, A.; Massimi, D.; Lorenzon, G.; et al. Infliximab Originator, Infliximab Biosimilar, and Adalimumab Are More Effective in Crohn’s Disease Than Ulcerative Colitis: A Real-Life Cohort Study. Clin. Transl. Gastroenterol. 2020, 11, e00177. [Google Scholar] [CrossRef]
- Zingone, F.; Siniscalchi, M.; Savarino, E.V.; Barberio, B.; Cingolani, L.; D’Inca, R.; De Filippo, F.R.; Camera, S.; Ciacci, C. Perception of the COVID-19 Pandemic among Patients With Inflammatory Bowel Disease in the Time of Telemedicine: Cross-Sectional Questionnaire Study. J. Med. Internet Res. 2020, 22, e19574. [Google Scholar] [CrossRef]
- D’Amico, F.; Danese, S.; Peyrin-Biroulet, L.; taskforce, E.C. Inflammatory Bowel Disease Management during the Coronavirus-19 Outbreak: A Survey from the European Crohn’s and Colitis Organization. Gastroenterology 2020, 159, 14–19.e13. [Google Scholar] [CrossRef]
- Danese, S.; Cecconi, M.; Spinelli, A. Management of IBD during the COVID-19 outbreak: Resetting clinical priorities. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 253–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, P.; Ji, M.; Ren, H.; Su, J.; Ding, N.S.; Kang, J.; Yin, A.; Zhou, Q.; Shen, L.; Zhao, L.; et al. Prevention of COVID-19 in patients with inflammatory bowel disease in Wuhan, China. Lancet Gastroenterol. Hepatol. 2020, 5, 525–527. [Google Scholar] [CrossRef]
- Hanzel, J.; Ma, C.; Marshall, J.K.; Feagan, B.G.; Jairath, V. Managing Inflammatory Bowel Disease during COVID-19: Summary of Recommendations from Gastrointestinal Societies. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2020, 18, 2143–2146. [Google Scholar] [CrossRef] [PubMed]
- Ferreira de Abreu, C.M. 1st Interview COVID-19 ECCO Taskforce, Published 13 March 2020. Available online: https://www.ecco-ibd.eu/publications/covid-19.html (accessed on 29 June 2021).
- Dotan, I.; Panaccione, R.; Kaplan, G.G.; O’Morain, C.; Lindsay, J.O.; Abreu, M.T. Best Practice Guidance for Adult Infusion Centres during the COVID-19 Pandemic: Report from the COVID-19 International Organization for the Study of IBD [IOIBD] Task Force. J. Crohn’s Colitis 2020, 14, S785–S790. [Google Scholar] [CrossRef]
- Fantini, M.C.; Biancone, L.; Dragoni, G.; Bezzio, C.; Miranda, A.; Ribaldone, D.G.; Bertani, A.; Bossa, F.; Allocca, M.; Buda, A.; et al. Telemedicine and Remote Screening for COVID-19 in Inflammatory Bowel Disease Patients: Results from the SoCOVID-19 Survey. Inflamm. Bowel Dis. 2020, 26, e134–e136. [Google Scholar] [CrossRef]
- Saibeni, S.; Scucchi, L.; Dragoni, G.; Bezzio, C.; Miranda, A.; Ribaldone, D.G.; Bertani, A.; Bossa, F.; Allocca, M.; Buda, A.; et al. Activities related to inflammatory bowel disease management during and after the coronavirus disease 2019 lockdown in Italy: How to maintain standards of care. United Eur. Gastroenterol. J. 2020, 8, 1228–1235. [Google Scholar] [CrossRef] [PubMed]
- Bertani, L.; Mumolo, M.G.; Tapete, G.; Albano, E.; Baiano Svizzero, G.; Zanzi, F.; Ceccarelli, L.; Bellini, M.; Marchi, S.; Costa, F. Fecal calprotectin: Current and future perspectives for inflammatory bowel disease treatment. Eur. J. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef]
- Snaith, R.P.; Zigmond, A.S. The hospital anxiety and depression scale. Br. Med. J. (Clin. Res. Ed.) 1986, 292, 344. [Google Scholar] [CrossRef] [Green Version]
- Magro, F.; Abreu, C.; Rahier, J.F. The daily impact of COVID-19 in gastroenterology. United Eur. Gastroenterol. J. 2020, 8, 520–527. [Google Scholar] [CrossRef]
- Mao, R.; Liang, J.; Shen, J.; Ghosh, S.; Zhu, L.R.; Yang, H.; Wu, K.C.; Chen, M.H.; Chinese Society of IBD; Chinese Elite IBD Union. Implications of COVID-19 for patients with pre-existing digestive diseases. Lancet Gastroenterol. Hepatol. 2020, 5, 425–427. [Google Scholar] [CrossRef]
- Gubatan, J.; Levitte, S.; Balabanis, T.; Patel, A.; Sharma, A.; Habtezion, A. SARS-CoV-2 Testing, Prevalence, and Predictors of COVID-19 in Patients with Inflammatory Bowel Disease in Northern California. Gastroenterology 2020, 159, 1141–1144.e1142. [Google Scholar] [CrossRef] [PubMed]
- Allocca, M.; Fiorino, G.; Zallot, C.; Furfaro, F.; Gilardi, D.; Radice, S.; Danese, S.; Peyrin-Biroulet, L. Incidence and Patterns of COVID-19 among Inflammatory Bowel Disease Patients from the Nancy and Milan Cohorts. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2020, 18, 2134–2135. [Google Scholar] [CrossRef]
- Ferro, F.; Elefante, E.; Baldini, C.; Bartoloni, E.; Puxeddu, I.; Talarico, R.; Mosca, M.; Bombardieri, S. COVID-19: The new challenge for rheumatologists. Clin. Exp. Rheumatol. 2020, 38, 175–180. [Google Scholar]
- Scribano, M.L. Why Do Immunosuppressed Patients with Inflammatory Bowel Disease Not Seem to Be at a Higher Risk of COVID-19? Dig. Dis. Sci. 2020. [Google Scholar] [CrossRef] [PubMed]
- Papa, A.; Gasbarrini, A.; Tursi, A. Epidemiology and the Impact of Therapies on the Outcome of COVID-19 in Patients with Inflammatory Bowel Disease. Am. J. Gastroenterol. 2020, 115, 1722–1724. [Google Scholar] [CrossRef]
- Bezzio, C.; Saibeni, S.; Variola, A.; Allocca, M.; Massari, A.; Gerardi, V.; Casini, V.; Ricci, C.; Zingone, F.; Amato, A.; et al. Outcomes of COVID-19 in 79 patients with IBD in Italy: An IG-IBD study. Gut 2020, 69, 1213–1217. [Google Scholar] [CrossRef] [PubMed]
- Gianfrancesco, M.; Hyrich, K.L.; Al-Adely, S.; Carmona, L.; Danila, M.I.; Gossec, L.; Izadi, Z.; Jacobsohn, L.; Katz, P.; Lawson-Tovey, S.; et al. Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: Data from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann. Rheum. Dis. 2020, 79, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Veenstra, J.; Buechler, C.R.; Robinson, G.; Chapman, S.; Adelman, M.; Tisack, A.; Dimitrion, P.; Todter, E.; Kohen, L.; Lim, H.W. Antecedent immunosuppressive therapy for immune-mediated inflammatory diseases in the setting of a COVID-19 outbreak. J. Am. Acad. Dermatol. 2020, 83, 1696–1703. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Passavanti, M.; Argentieri, A.; Barbieri, D.M.; Lou, B.; Wijayaratna, K.; Foroutan Mirhosseini, A.S.; Wang, F.; Naseri, S.; Qamhia, I.; Tangeras, M.; et al. The psychological impact of COVID-19 and restrictive measures in the world. J. Affect. Disord. 2021, 283, 36–51. [Google Scholar] [CrossRef] [PubMed]
- Fornili, M.; Petri, D.; Berrocal, C.; Fiorentino, G.; Ricceri, F.; Macciotta, A.; Bruno, A.; Farinella, D.; Baccini, M.; Severi, G.; et al. Psychological distress in the academic population and its association with socio-demographic and lifestyle characteristics during COVID-19 pandemic lockdown: Results from a large multicenter Italian study. PLoS ONE 2021, 16, e0248370. [Google Scholar] [CrossRef]
- Geldsetzer, P. Knowledge and Perceptions of COVID-19 among the General Public in the United States and the United Kingdom: A Cross-Sectional Online Survey. Ann. Intern. Med. 2020, 173, 157–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Otmani, H.; El Bidaoui, Z.; Amzil, R.; Bellakhdar, S.; El Moutawakil, B.; Abdoh Rafai, M. No impact of confinement during COVID-19 pandemic on anxiety and depression in Parkinsonian patients. Rev. Neurol. 2021. [Google Scholar] [CrossRef]
- Chiaravalloti, N.D.; Amato, M.P.; Brichetto, G.; Chataway, J.; Dalgas, U.; DeLuca, J.; Meza, C.; Moore, N.B.; Feys, P.; Filippi, M.; et al. The emotional impact of the COVID-19 pandemic on individuals with progressive multiple sclerosis. J. Neurol. 2020. [Google Scholar] [CrossRef]
- Barberio, B.; Zingone, F.; Bertani, L.; Savarino, E. The Adherence to Infusible Biologic Therapies in Inflammatory Bowel Disease Patients During COVID-19 Pandemic: Is It Really a Problem? Gastroenterology 2020. [Google Scholar] [CrossRef]
- Khan, N.; Patel, D.; Xie, D.; Pernes, T.; Lewis, J.; Yang, Y.X. Adherence of Infusible Biologics During the Time of COVID-19 Among Patients With Inflammatory Bowel Disease: A Nationwide Veterans Affairs Cohort Study. Gastroenterology 2020, 159, 1592–1594. [Google Scholar] [CrossRef]
- Arrigo, S.; Alvisi, P.; Banzato, C.; Bramuzzo, M.; Celano, R.; Civitelli, F.; D’Arcangelo, G.; Dilillo, A.; Dipasquale, V.; Felici, E.; et al. Impact of COVID-19 pandemic on the management of paediatric inflammatory bowel disease: An Italian multicentre study on behalf of the SIGENP IBD Group. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2021, 53, 283–288. [Google Scholar] [CrossRef]
- Cross, R.K.; Langenberg, P.; Regueiro, M.; Schwartz, D.A.; Tracy, J.K.; Collins, J.F.; Katz, J.; Ghazi, L.; Patil, S.A.; Quezada, S.M.; et al. A Randomized Controlled Trial of TELEmedicine for Patients with Inflammatory Bowel Disease (TELE-IBD). Am. J. Gastroenterol. 2019, 114, 472–482. [Google Scholar] [CrossRef]
- George, L.A.; Cross, R.K. Remote Monitoring and Telemedicine in IBD: Are We There Yet? Curr. Gastroenterol. Rep. 2020, 22, 12. [Google Scholar] [CrossRef]
- Costantino, A.; Noviello, D.; Mazza, S.; Berte, R.; Caprioli, F.; Vecchi, M. Trust in telemedicine from IBD outpatients during the COVID-19 pandemic. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2021, 53, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Lahat, A.; Shatz, Z. Telemedicine in clinical gastroenterology practice: What do patients prefer? Ther. Adv. Gastroenterol. 2021, 14, 1756284821989178. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Number of patients, n | 189 |
| Female, n (%) | 83 (44) |
| Age, years, median | 45 (19–76) |
| Crohn’s disease, n (%) | 116 (61) |
| Drug | |
| Infliximab, n (%) | 71 (38) |
| Adalimumab, n (%) | 41 (23) |
| Golimumab, n (%) | 7 (4) |
| Vedolizumab, n (%) | 39 (21) |
| Ustekinumab, n (%) | 29 (15) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertani, L.; Barberio, B.; Tricò, D.; Zanzi, F.; Maniero, D.; Ceccarelli, L.; Marsilio, I.; Coppini, F.; Lorenzon, G.; Mumolo, M.G.; et al. Hospitalisation for Drug Infusion Did Not Increase Levels of Anxiety and the Risk of Disease Relapse in Patients with Inflammatory Bowel Disease during COVID-19 Outbreak. J. Clin. Med. 2021, 10, 3270. https://doi.org/10.3390/jcm10153270
Bertani L, Barberio B, Tricò D, Zanzi F, Maniero D, Ceccarelli L, Marsilio I, Coppini F, Lorenzon G, Mumolo MG, et al. Hospitalisation for Drug Infusion Did Not Increase Levels of Anxiety and the Risk of Disease Relapse in Patients with Inflammatory Bowel Disease during COVID-19 Outbreak. Journal of Clinical Medicine. 2021; 10(15):3270. https://doi.org/10.3390/jcm10153270
Chicago/Turabian StyleBertani, Lorenzo, Brigida Barberio, Domenico Tricò, Federico Zanzi, Daria Maniero, Linda Ceccarelli, Ilaria Marsilio, Francesca Coppini, Greta Lorenzon, Maria Gloria Mumolo, and et al. 2021. "Hospitalisation for Drug Infusion Did Not Increase Levels of Anxiety and the Risk of Disease Relapse in Patients with Inflammatory Bowel Disease during COVID-19 Outbreak" Journal of Clinical Medicine 10, no. 15: 3270. https://doi.org/10.3390/jcm10153270
APA StyleBertani, L., Barberio, B., Tricò, D., Zanzi, F., Maniero, D., Ceccarelli, L., Marsilio, I., Coppini, F., Lorenzon, G., Mumolo, M. G., Zingone, F., Costa, F., & Savarino, E. V. (2021). Hospitalisation for Drug Infusion Did Not Increase Levels of Anxiety and the Risk of Disease Relapse in Patients with Inflammatory Bowel Disease during COVID-19 Outbreak. Journal of Clinical Medicine, 10(15), 3270. https://doi.org/10.3390/jcm10153270