
Impact on Visual Acuity in Neovascular Age Related Macular Degeneration (nAMD) in Europe Due to COVID-19 Pandemic Lockdown

 ,
,  ,
,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Data Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wong, R.L.; Lai, K.H.; Huang, S.S.; Jonas, J.B.; Lam, D.S. COVID-19 Pandemic: Ways Forward. Asia-Pac. J. Ophthalmol. 2020, 9, 59–60. [Google Scholar] [CrossRef]
- Situation Report -51 WHOC Disease 2019 (COVID-19). S. No. Available online: https://www.who.int/docs/defaultsource/coronaviruse/situation-reports/20200311-Sitrep-51-Covid-19.pdf?Sfvrsn¼1ba62e57_10 (accessed on 19 May 2020).
- Toro, M.D.; Brézin, A.P.; Burdon, M.; Cummings, A.B.; Kemer, O.E.; Malyugin, B.E.; Prieto, I.; Teus, M.A.; Tognetto, D.; Törnblom, R.; et al. Early Impact of COVID-19 Outbreak on Eye Care: Insights from EUROCOVCAT Group. Eur. J. Ophthalmol. 2021, 31, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Tognetto, D.; Brézin, A.P.; Cummings, A.B.; Malyugin, B.E.; Kemer, O.E.; Prieto, I.; Rejdak, R.; Teus, M.A.; Törnblom, R.; Toro, M.D.; et al. Rethinking Elective Cataract Surgery Diagnostics, Assessments, and Tools After the COVID-19 Pandemic Experience and Beyond: Insights from the EUROCOVCAT Group. Diagnostics 2020, 10, 1035. [Google Scholar] [CrossRef] [PubMed]
- Toro, M.; Choragiewicz, T.; Posarelli, C.; Figus, M.; Rejdak, R.; European COVID-19 Cataract Group (#EUROCOVCAT). Early Impact of COVID-19 Outbreak on the Availability of Cornea Donors: Warnings and Recommendations. Clin. Ophthalmol. 2020, 14, 2879–2882. [Google Scholar] [CrossRef]
- Ferrara, M.; Romano, V.; Steel, D.H.; Gupta, R.; Iovino, C.; van Dijk, E.H.C.; Rocha-De-Lossada, C.; Bali, E.; Valldeperas, X.; Romano, D.; et al. Reshaping Ophthalmology Training After COVID-19 Pandemic. Eye 2020, 34, 2089–2097. [Google Scholar] [CrossRef] [PubMed]
- Corradetti, G.; Corvi, F.; Nguyen, T.V.; Sadda, S.R. Management of neovascular age-related macular degeneration during the COVID-19 pandemia. Ophthalmol. Retina 2020. [Google Scholar] [CrossRef] [PubMed]
- Shmueli, O.; Chowers, I.; Levy, J. Current Safety Preferences for Intravitreal Injection During COVID-19 Pandemic. Eye 2020, 34, 1165–1167. [Google Scholar] [CrossRef] [PubMed]
- Li, J.-P.O.; Shantha, J.; Wong, T.Y.; Wong, E.Y.; Mehta, J.; Lin, H.; Lin, X.; Strouthidis, N.G.; Park, K.H.; Fung, A.T.; et al. Preparedness Among Ophthalmologists: During and Beyond the COVID-19 Pandemic. Ophthalmology 2020, 127, 569–572. [Google Scholar] [CrossRef]
- Recommendations for Urgent and Nonurgent Patient Care. American Academy of Ophthalmology. Published 18 March 2020. Available online: https://www.aao.org/headline/New-Recommendations-Urgent-Nonurgent-Patient-Care (accessed on 15 July 2020).
- HPI CoronaVirus Statement 1-30-20.pdf. American Optometric Association. Published 24 March 2020. Available online: https://www.aoa.org/documents/HPI/HPI%20CoronaVirus%20Statement%201-30-20.Pdf (accessed on 15 July 2020).
- American Academy of Ophthalmology. Important Coronavirus Updates for Ophthalmologists. 2020. Available online: https://www.aao.org/headline/Alert-Important-Coronavirus-Context (accessed on 31 March 2020).
- Société Françaised’Ophtalmologie. Quelle Conduite à Tenir Adopter Vis à Vis des Injections Intravitréennes (IVT) dans Cettepérioded’Épidémie au Covid-19—SARS-CoV-2. Available online: https://www.sfo.asso.fr/files/files/FPHUNG/epidemie_au_covid-19_-_ivt.pdf (accessed on 31 March 2020).
- Deutsche Opthalmologische Gesellschaft. Coronavirus COVID-19. 2020. Available online: https://www.dog.org/?Cat=288 (accessed on 31 March 2020).
- The Royal College of Ophthalmologists. COVID-19 Clinical Guidance for Ophthalmologists. 2020. Available online: https://www.rcophth.ac.uk/2020/03/Covid-19-Update-and-Resources-for-ophthalmologists/ (accessed on 31 March 2020).
- The Royal College of Ophthalmologists. Medical Retinal Management Plans During COVID-19. 2020. Available online: https://www.rcophth.ac.uk/Wp-content/uploads/2020/03/Medical-Retinal-Management-Planduring-COVID-19-UPDATED-300320-1-2.Pdf (accessed on 2 April 2020).
- Wong, T.; Chakravarthy, U.; Klein, R.; Mitchell, P.; Zlateva, G.; Buggage, R.; Fahrbach, K.; Probst, C.; Sledge, I. The Natural History and Prognosis of Neovascular Age-Related Macular Degeneration: A Systematic Review of the Literature and Meta-Analysis. Ophthalmology 2008, 115, 116–126.e1. [Google Scholar] [CrossRef]
- Haensli, C.; Sugiura, Y.; Freund, K.B.; Zweifel, S.A. Correlation of Outer Retinal Tubulations and Choriocapillaris Flow Signal Deficits Surrounding Geographic Atrophy. Retina 2021. [Google Scholar] [CrossRef]
- Plyukhova, A.A.; Budzinskaya, M.V.; Starostin, K.M.; Rejdak, R.; Bucolo, C.; Reibaldi, M.; Toro, M.D. Comparative Safety of Bevacizumab, Ranibizumab, and Aflibercept for Treatment of Neovascular Age-Related Macular Degeneration (AMD): A Systematic Review and Network Meta-Analysis of Direct Comparative Studies. J. Clin. Med. 2020, 9, 1522. [Google Scholar] [CrossRef]
- Takahashi, H.; Ohkubo, Y.; Sato, A.; Takezawa, M.; Fujino, Y.; Yanagi, Y.; Kawashima, H. Relationship Between Visual Prognosis and Delay of Intravi-Treal Injection of Ranibizumab When Treating Age-Related Macular Degeneration. Retina 2015, 35, 1331–1338. [Google Scholar] [CrossRef]
- Real, J.P.; Granero, G.E.; De Santis, M.O.; Juárez, C.P.; Palma, S.D.; Kelly, S.P.; Luna, J.D. Rate of Vision Loss in Neovascular Age-Related Macular Degeneration Explored. Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 253, 1859–1865. [Google Scholar] [CrossRef]
- Muether, P.S.; Hermann, M.M.; Koch, K.; Fauser, S. Delay Between Medical Indication to Anti-VEGF Treatment in Age-Related Macular Degeneration Can Result in a Loss of Visual Acuity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2011, 249, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Starr, M.R.; Boucher, N.; Chiang, A.; Yonekawa, Y.; Klufas, M.A.; Khan, M.A.; Cohen, M.N.; Mehta, S.; Kuriyan, A.E. Real-World Vitreoretinal Practice Patterns During the 2020 COVID-19 Pandemic: A Nationwide, Aggregated Health Record Analysis. Curr. Opin. Ophthalmol. 2020, 31, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Wasser, L.M.; Weill, Y.; Brosh, K.; Magal, I.; Potter, M.; Strassman, I.; Gelman, E.; Koslowsky, M.; Zadok, D.; Hanhart, J. The Impact of COVID-19 on Intravitreal Injection Compliance. SN Compr. Clin. Med. 2020, 2, 2546–2549. [Google Scholar] [CrossRef]
- Viola, F.; Milella, P.; Giuffrida, F.P.; Ganci, S.; Invernizzi, A. Impact of Coronavirus Disease Pandemic on Intravitreal Injections Treatment for Macular Diseases: Report from a Referral Hospital in Milan. Retina 2021, 41, 701–705. [Google Scholar] [CrossRef]
- Borrelli, E.; Grosso, D.; Vella, G.; Sacconi, R.; Battista, M.; Querques, L.; Zucchiatti, I.; Prascina, F.; Bandello, F.; Querques, G. Short-Term Outcomes of Patients with Neovascular Exudative AMD: The Effect of COVID-19 Pandemic. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 2621–2628. [Google Scholar] [CrossRef] [PubMed]
- Elfalah, M.; AlRyalat, S.A.; Toro, M.D.; Rejdak, R.; Zweifel, S.; Nazzal, R.; Abu-Ameerh, M.; Ababneh, O.; Gharaibeh, A.; Sharif, Z.; et al. Delayed Intravitreal Anti-VEGF Therapy for Patients During the COVID-19 Lockdown: An Ethical Endeavor. Clin. Ophthalmol. 2021, 15, 661–669. [Google Scholar] [CrossRef]
- Song, W.; Singh, R.P.; Rachitskaya, A.V. The Effect of Delay in Care Among Patients Requiring Intravitreal Injections. Ophthalmol. Retin. 2021. [Google Scholar] [CrossRef]
- Yeter, D.; Dursun, D.; Bozali, E.; Ozec, A.; Erdogan, H. Effects of the COVID-19 Pandemic on Neovascular Age-Related Macular Degeneration and Response to Delayed Anti-VEGF Treatment. J. Fr. Ophtalmol. 2021, 44, 299–306. [Google Scholar] [CrossRef]
- Spaide, R.F.; Jaffe, G.J.; Sarraf, D.; Freund, K.B.; Sadda, S.R.; Staurenghi, G.; Waheed, N.K.; Chakravarthy, U.; Rosenfeld, P.J.; Holz, F.G.; et al. Consensus Nomenclature for Reporting Neovascular Age-Related Macular Degeneration Data. Ophthalmology 2020, 127, 616–636. [Google Scholar] [CrossRef]
- Gregori, N.Z.; Feuer, W.; Rosenfeld, P.J. Novel Method for Analyzing Snellen Visual Acuity Measurements. Retina 2010, 30, 1046–1050. [Google Scholar] [CrossRef]
- Freund, K.B.; Zweifel, S.A.; Engelbert, M. Do We Need a New Classification for Choroidal Neovascularization in Age-Related Macular Degeneration? Retina 2010, 30, 1333–1349. [Google Scholar] [CrossRef]
- Colijn, J.M.; Buitendijk, G.H.S.; Prokofyeva, E.; Alves, D.; Cachulo, M.L.; Khawaja, A.P.; Cougnard-Gregoire, A.; Merle, B.M.; Korb, C.; Erke, M.G.; et al. Prevalence of Age-Related Macular Degeneration in Europe: The Past and the Future. Ophthalmology 2017, 124, 1753–1763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holz, F.G.; Tadayoni, R.; Beatty, S.; Berger, A.R.; Cereda, M.G.; Hykin, P.; Staurenghi, G.; Wittrup-Jensen, K.; Nilsson, J.; Kim, K.; et al. Determinants of Visual Acuity Outcomes in Eyes With Neovascu-Lar AMD Treated With Anti-VEGF Agents: An Instrumental Variable Analysis of the AURA Study. Eye 2016, 30, 1063–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holz, F.G.; Figueroa, M.S.; Bandello, F.; Yang, Y.; Ohji, M.; Dai, H.; Wykrota, H.; Sharma, S.; Dunger-Baldauf, C.; Lacey, S.; et al. Ranibizumab Treatment in Treatment-Naive Neovascular Age-Related Macular Degeneration: Results From LUMINOUS, a Global Real-World Study. Retina 2020, 40, 1673–1685. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.; Warwick, A.N.; Olvera-Barrios, A.; Egan, C. Estimating Excess Visual Loss in People With Neo-Vascular Age-Related Macular Degeneration During the COVID-19 Pandemic. medRxiv 2020. [Google Scholar] [CrossRef]
- Lestable, L.; Gabrielle, P.-H.; Bron, A.; Nguyen, P.; Creuzot-Garcher, C. Twelve-Month Outcomes of Intra-Vitreal Anti-VEGF Agents for Treatment-naïve Neovascular Age-Related Macular Degeneration Eyes: French Data from the Fight for Retinal Blindness! J. Fr. Ophtalmol. 2020, 43, 761–769. [Google Scholar] [CrossRef]


{kind=link}
| Country | Poland (n = 94) | Italy (n = 105) | Spain (n = 144) | Turkey (n = 82) | Russia (n = 20) | Switzerland (n = 101) | All (n = 546) | p Value |
|---|---|---|---|---|---|---|---|---|
| Age (years) | 75.94 ± 8.40 | 81.15 ± 7.02 | 79.43 ± 7.57 | 73.13 ± 9.23 | 69.55 ± 12.68 | 83.38 ± 7.43 | 79.36 ± 8.83 | 0.0001 |
| Gender (% female) | 54.26 | 54.29 | 54.86 | 52.44 | 75 | 62.07 | 55.13 | ns |
| Bilateral disease | 0% | 0% | 14.37% | 16.33% | 15.38% | 17.17% | 6.67% | ns |
| Lockdown duration | 2.5 | 2.75 | 2.75 | 2.75 | 2.5 | 1.5 | 2.51 ± 0.3 | |
| CNV type | 0.001 | |||||||
| type 1 | 89.36 | 49.52 | 68.06 | 92.68 | 80 | 49.50 | 71.53 | |
| type2 | 10.64 | 46.67 | 18.06 | 7.32 | 20 | 43.56 | 24.37 | |
| type3 | 2.86 | 13.19 | 6.93 | 3.83 | ||||
| type 1 aneurismatic | 0.95 | 0.69 | 0.27 | |||||
| Disease follow-up | 3.11 ± 0.12 | 3.07 ± 0.23 | 2.97 ± 0.18 | 2.40 ± 0.19 | 2.74 ± 0.75 | 6.91 ± 0.27 | 3.25 ± 0.09 | 0.0001 |
| Only one functional eye | 19.15 | 35.24 | 27.08 | 34.15 | 15 | 18.00 | 26.23 | ns |
| AV > 70 | 50.00% | 26.67% | 40.28% | 36.59% | 45.00% | 59.407% | 41.54% | |
| AV > 50 | 98.94% | 69.52% | 73.61% | 80.49% | 70.00% | 82.17% | 79.30% | |
| AV < 30 | 1.06% | 8.57% | 13.89% | 7.32% | 15.00% | 11.88% | 8.97% | |
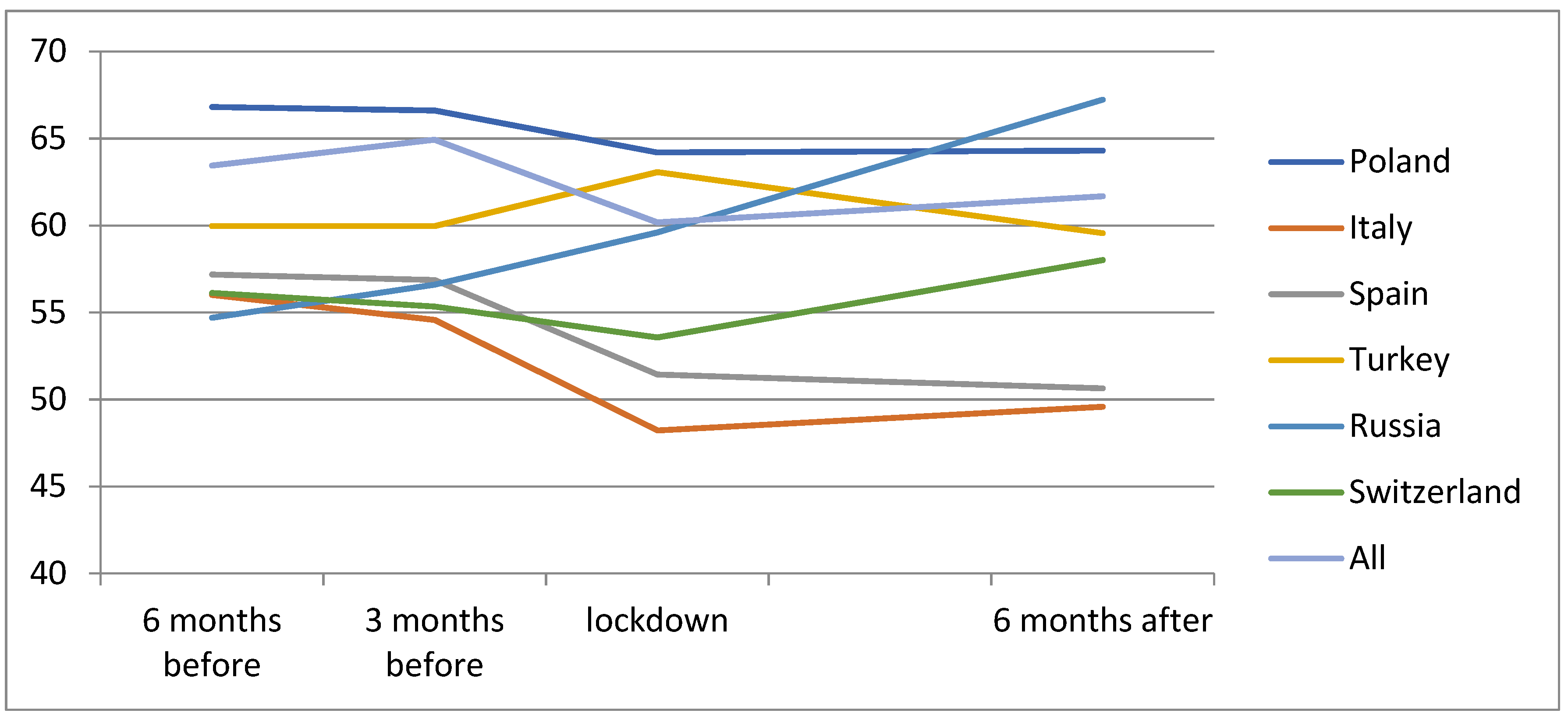
| Mean BCVA 6 months before the lockdown | 66.81 ± 10.54 | 56.01 ± 18.12 | 57.19 ± 23.14 | 59.97 ± 17.94 | 54.7 ± 25.93 | 66.36 ± 19.00 | 60.71 ± 19.34 | 0.003 |
| Mean BCVA 3 months before the lockdown | 66.60 ± 11.56 | 54.57 ± 18.74 | 56.87 ± 24.09 | 62.13 ± 18.18 | 56.6 ± 26.38 | 67.13 ± 17.91 | 60.68 ± 19.77 | 0.0001 |
| Number of visits 6 months before the lock down | 3.85 ± 0.64 | 2.08 ± 1.02 | 2.67 ± 0.88 | 3.02 ± 1.00 | 6.05 ± 3.50 | 3.67 ± 1.35 | 3.13 ± 1.45 | 0.0001 |
| Number of IVI 6 months before the lockdown | 2.94 ± 1.24 | 2.81 ± 1.48 | 2.20 ± 1.60 | 2.96 ± 1.070 | 1.9 ± 1.11 | 2.71 ± 1.83 | 2.65 ± 1.51 | 0.0001 |
| % of active CNV before the lock down | 91.49% | 76.19% | 44.44% | 28.05% | 95.00% | 77.0% | 65.17% | 0.0001 |
| % patients that discontinued the follow-up during the lockdown | 36.1% | 63.4% | 62.2% | 98.7% | 45.0% | 57.0% | 62.8% | 0.0001 |
| 6 Months before the Lockdown (n = 526) | During the Lockdown | 6 Month after the Lockdown | p Value | |
|---|---|---|---|---|
| (n = 143) | (n = 469) | |||
| Mean BCVA | 60.71 ± 19.34 | 59.18 ± 19.32 | 56.98 ± 22.59 | p = 0.001 |
| Number of IVIs | 2.65 ± 1.51 | 0.38 ± 0.57 | 1.84 ± 1.52 | p = 0.001 |
| Number of IVIs (per month) | 1.18 ± 0.78 | 0.18 ± 0.27 | 0.84 ± 0.82 | |
| Number of visits | 3.13 ± 1.45 | 0.33 ± 0.63 | 2.24 ± 1.46 | p = 0.001 |
| Number of visits (per month) | 1.40 ± 0.82 | 0.12 ± 0.24 | 1.05 ± 0.87 |
| All Patients n = 546 | Discontinued Follow-Up n = 343 | Continued Follow-Up n = 203 | p Value |
|---|---|---|---|
| Age (years) | 79.93 ± 8.8 | 78.4 ± 8.7 | 0.053 |
| Gender (%female) | 53.0% | 38.8% | 0.3 |
| Only one functional eye | 25.15% | 27.72% | 0.5 |
| Duration of the disease (years) | 3.18 ± 2.22 | 3.41 ± 2.43 | 0.2 |
| Mean BCVA 6 months before lockdown | 59.02 ± 20.08 | 63.55 ± 17.68 | 0.009 |
| AV ≥ 70 letters | 38.7% | 52.6% | 0.02 |
| AV ≥ 65 letters | 51.7% | 63.5% | 0.009 |
| % of eyes with activity of the lesion before lockdown | 52.9% | 86.36% | 0.0001 |
| Lockdown duration (months) | 2.45 ± 0.43 | 2.42 ± 0.49 | 0.4 |
| Mean change in BCVA 6 months after lockdown (letters) | −3.41 ± 12.80 | −3.45 ± 14.04 | 0.9 |
| Nº of visits during the 6 months after lockdown | 2.02 ± 1.28 | 2.61 ± 1.66 | 0.0001 |
| Nº of injections during 6 months after lockdown | 1.50 ± 1.51 | 2.36 ± 1.39 | 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arruabarrena, C.; Toro, M.D.; Onen, M.; Malyugin, B.E.; Rejdak, R.; Tognetto, D.; Zweifel, S.; Giglio, R.; Teus, M.A. Impact on Visual Acuity in Neovascular Age Related Macular Degeneration (nAMD) in Europe Due to COVID-19 Pandemic Lockdown. J. Clin. Med. 2021, 10, 3281. https://doi.org/10.3390/jcm10153281
Arruabarrena C, Toro MD, Onen M, Malyugin BE, Rejdak R, Tognetto D, Zweifel S, Giglio R, Teus MA. Impact on Visual Acuity in Neovascular Age Related Macular Degeneration (nAMD) in Europe Due to COVID-19 Pandemic Lockdown. Journal of Clinical Medicine. 2021; 10(15):3281. https://doi.org/10.3390/jcm10153281
Chicago/Turabian StyleArruabarrena, Carolina, Mario Damiano Toro, Mehmet Onen, Boris E Malyugin, Robert Rejdak, Danielle Tognetto, Sandrine Zweifel, Rosa Giglio, and Miguel A Teus. 2021. "Impact on Visual Acuity in Neovascular Age Related Macular Degeneration (nAMD) in Europe Due to COVID-19 Pandemic Lockdown" Journal of Clinical Medicine 10, no. 15: 3281. https://doi.org/10.3390/jcm10153281
APA StyleArruabarrena, C., Toro, M. D., Onen, M., Malyugin, B. E., Rejdak, R., Tognetto, D., Zweifel, S., Giglio, R., & Teus, M. A. (2021). Impact on Visual Acuity in Neovascular Age Related Macular Degeneration (nAMD) in Europe Due to COVID-19 Pandemic Lockdown. Journal of Clinical Medicine, 10(15), 3281. https://doi.org/10.3390/jcm10153281