
Diagnostic Performance of Extracellular Volume Quantified by Dual-Layer Dual-Energy CT for Detection of Acute Myocarditis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
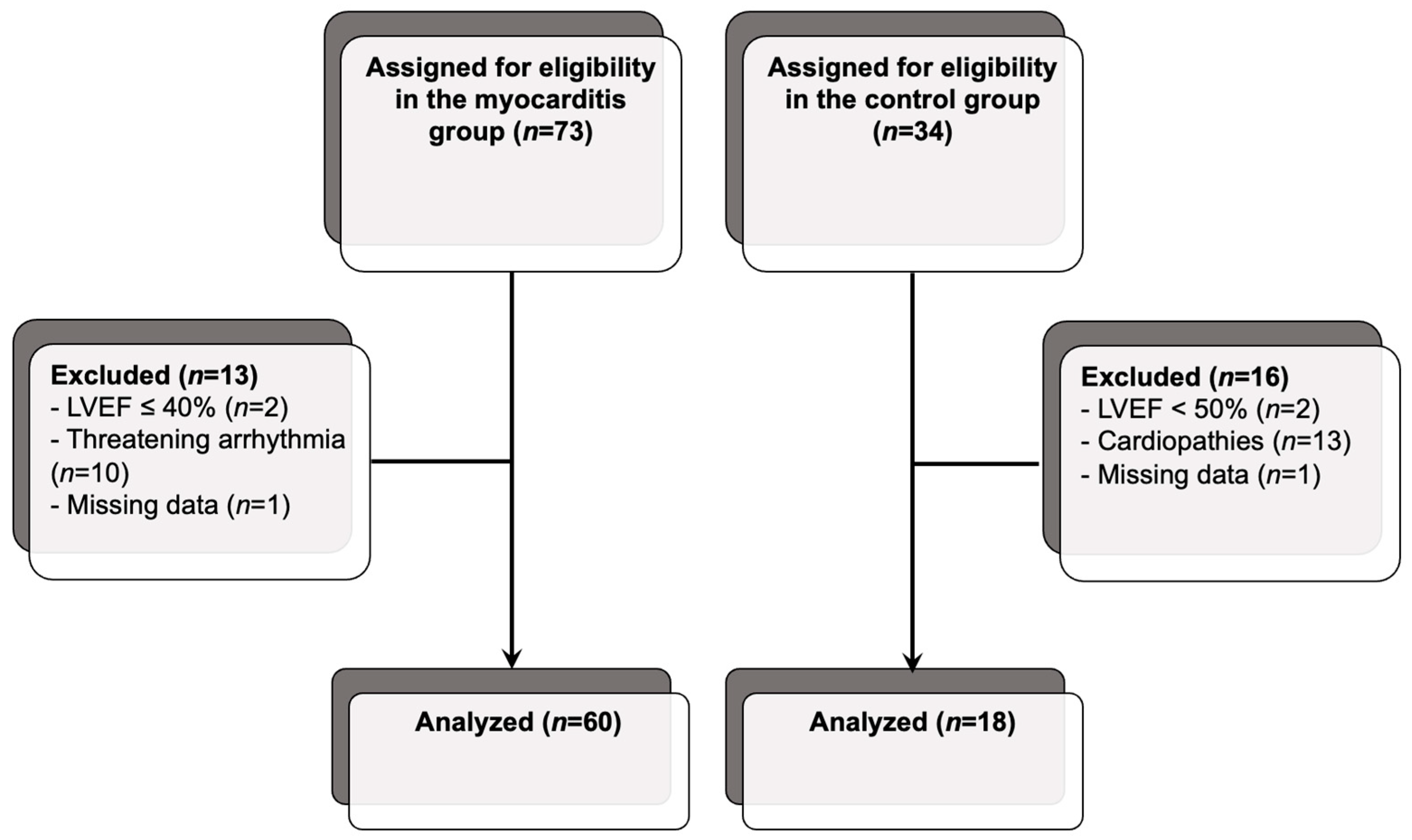
2.2. Population
2.3. Data Registration
2.4. DECT Imaging Protocol
2.4.1. Injection Protocol
2.4.2. Image Acquisition
2.4.3. Reconstruction Protocol
2.4.4. Image Analysis
2.5. Radiation Dose
2.6. Statistical Analyses
3. Results
3.1. Characteristics of the Population
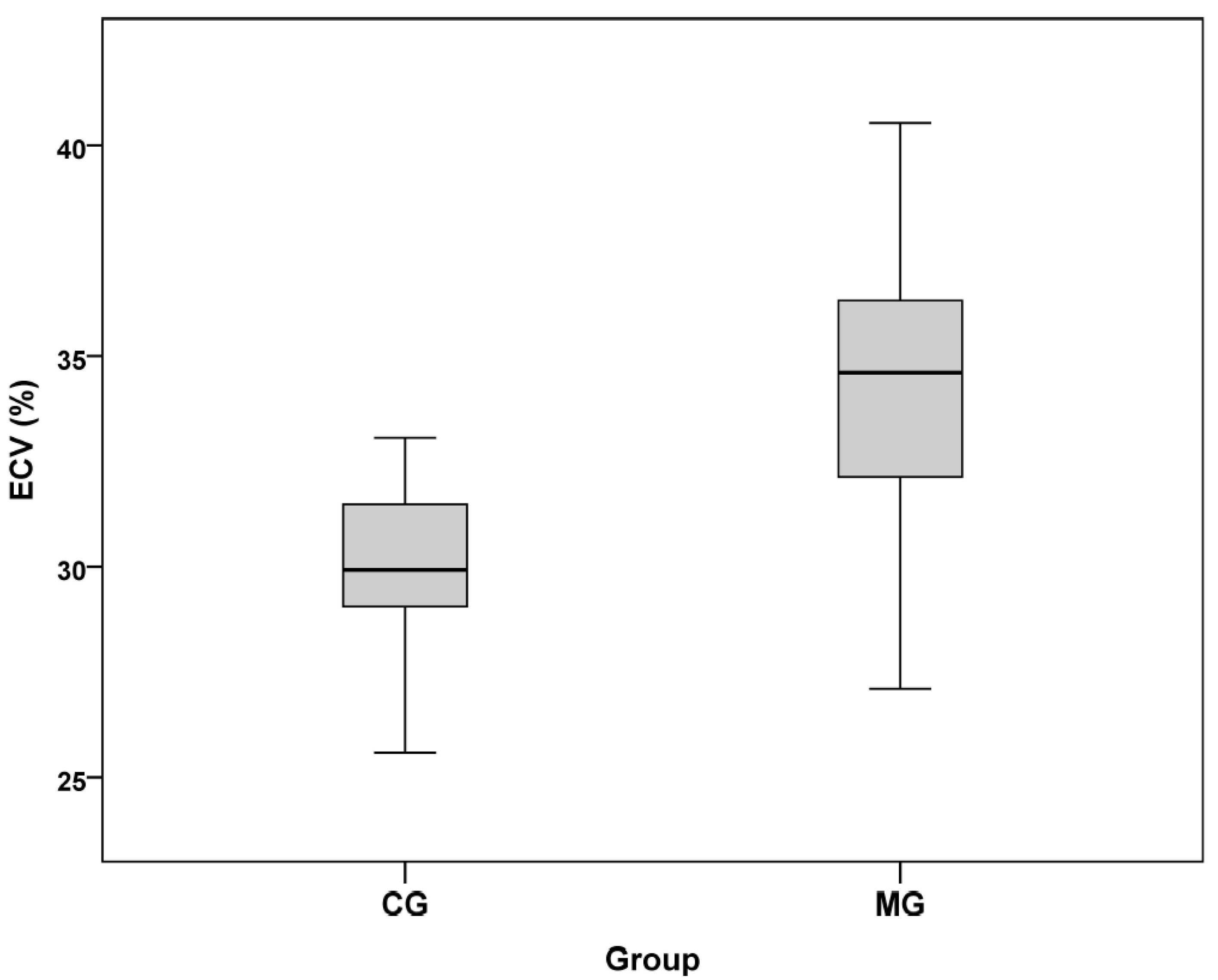
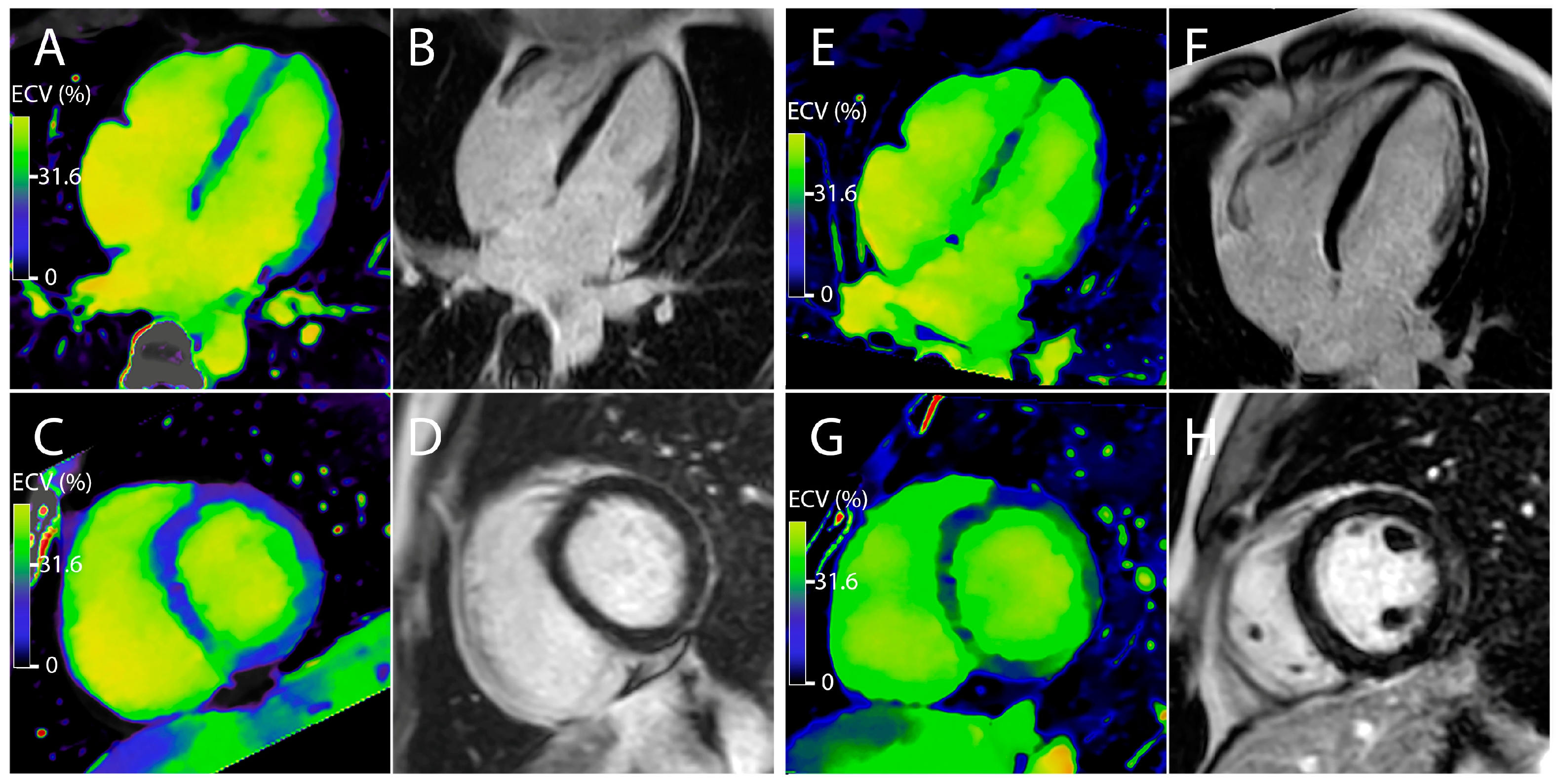
3.2. Measurement of the Myocardial Inflammation
3.3. Correlation between ECV and the Different Parameters
3.4. Measurement of the ECV Cut-Off Value
3.5. Radiation Dose Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Golpour, A.; Patriki, D.; Hanson, P.J.; McManus, B.; Heidecker, B. Epidemiological Impact of Myocarditis. J. Clin. Med. 2021, 10, 603. [Google Scholar] [CrossRef]
- Cooper, L.T. Myocarditis. N. Engl. J. Med. 2009, 360, 1526–1538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caforio, A.L.P.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2648a–2648d. [Google Scholar] [CrossRef]
- Bozkurt, B.; Colvin, M.; Cook, J.; Cooper, L.T.; Deswal, A.; Fonarow, G.C.; Francis, G.S.; Lenihan, D.; Lewis, E.F.; McNamara, D.M.; et al. Current Diagnostic and Treatment Strategies for Specific Dilated Cardiomyopathies: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e579–e646. [Google Scholar] [CrossRef]
- Hauck, A.J.; Kearney, D.L.; Edwards, W.D. Evaluation of postmortem endomyocardial biopsy specimens from 38 patients with lymphocytic myocarditis: Implications for role of sampling error. Mayo Clin. Proc. 1989, 64, 1235–1245. [Google Scholar] [CrossRef]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J. Am. Coll. Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef]
- Friedrich, M.G.; Sechtem, U.; Schulz-Menger, J.; Holmvang, G.; Alakija, P.; Cooper, L.T.; White, J.A.; Abdel-Aty, H.; Gutberlet, M.; Prasad, S.; et al. Cardiovascular Magnetic Resonance in Myocarditis: A JACC White Paper. J. Am. Coll. Cardiol. 2009, 53, 1475–1487. [Google Scholar] [CrossRef] [Green Version]
- Scully, P.R.; Bastarrika, G.; Moon, J.C.; Treibel, T.A. Myocardial Extracellular Volume Quantification by Cardiovascular Magnetic Resonance and Computed Tomography. Curr. Cardiol. Rep. 2018, 20, 15. [Google Scholar] [CrossRef] [Green Version]
- Nacif, M.S.; Kawel, N.; Lee, J.J.; Chen, X.; Yao, J.; Zavodni, A.; Sibley, C.T.; Lima, J.A.C.; Liu, S.; Bluemke, D.A. Interstitial myocardial fibrosis assessed as extracellular volume fraction with low-radiation-dose cardiac CT. Radiology 2012, 264, 876–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandula, S.; White, S.K.; Flett, A.S.; Lawrence, D.; Pugliese, F.; Ashworth, M.T.; Punwani, S.; Taylor, S.A.; Moon, J.C. Measurement of myocardial extracellular volume fraction by using equilibrium contrast-enhanced CT: Validation against histologic findings. Radiology 2013, 269, 396–403. [Google Scholar] [CrossRef]
- Lee, H.-J.; Im, D.J.; Youn, J.-C.; Chang, S.; Suh, Y.J.; Hong, Y.J.; Kim, Y.J.; Hur, J.; Choi, B.W. Myocardial Extracellular Volume Fraction with Dual-Energy Equilibrium Contrast-enhanced Cardiac CT in Nonischemic Cardiomyopathy: A Prospective Comparison with Cardiac MR Imaging. Radiology 2016, 280, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Kurita, Y.; Kitagawa, K.; Kurobe, Y.; Nakamori, S.; Nakajima, H.; Dohi, K.; Ito, M.; Sakuma, H. Estimation of myocardial extracellular volume fraction with cardiac CT in subjects without clinical coronary artery disease: A feasibility study. J. Cardiovasc. Comput. Tomogr. 2016, 10, 237–241. [Google Scholar] [CrossRef]
- Nacif, M.S.; Liu, Y.; Yao, J.; Liu, S.; Sibley, C.T.; Summers, R.M.; Bluemke, D.A. 3D left ventricular extracellular volume fraction by low-radiation dose cardiac CT: Assessment of interstitial myocardial fibrosis. J. Cardiovasc. Comput. Tomogr. 2013, 7, 51–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubourg, B.; Dacher, J.-N.; Durand, E.; Caudron, J.; Bauer, F.; Bubenheim, M.; Eltchaninoff, H.; Serfaty, J.-M. Single-source dual energy CT to assess myocardial extracellular volume fraction in aortic stenosis before transcatheter aortic valve implantation (TAVI). Diagn. Interv. Imaging 2021. [Google Scholar] [CrossRef] [PubMed]
- Abadia, A.F.; van Assen, M.; Martin, S.S.; Vingiani, V.; Griffith, L.P.; Giovagnoli, D.A.; Bauer, M.J.; Schoepf, U.J. Myocardial extracellular volume fraction to differentiate healthy from cardiomyopathic myocardium using dual-source dual-energy CT. J. Cardiovasc. Comput. Tomogr. 2020, 14, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Si-Mohamed, S.; Dupuis, N.; Tatard-Leitman, V.; Rotzinger, D.; Boccalini, S.; Dion, M.; Vlassenbroek, A.; Coulon, P.; Yagil, Y.; Shapira, N.; et al. Virtual versus true non-contrast dual-energy CT imaging for the diagnosis of aortic intramural hematoma. Eur. Radiol. 2019. [Google Scholar] [CrossRef]
- Rotzinger, D.C.; Si-Mohamed, S.A.; Shapira, N.; Douek, P.C.; Meuli, R.A.; Boussel, L. “Dark-blood” dual-energy computed tomography angiography for thoracic aortic wall imaging. Eur. Radiol. 2020, 30, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Rotzinger, D.C.; Si-Mohamed, S.A.; Yerly, J.; Boccalini, S.; Becce, F.; Boussel, L.; Meuli, R.A.; Qanadli, S.D.; Douek, P.C. Reduced-iodine-dose dual-energy coronary CT angiography: Qualitative and quantitative comparison between virtual monochromatic and polychromatic CT images. Eur. Radiol. 2021. [Google Scholar] [CrossRef]
- Bongartz, G.; Golding, S.J.; Jurik, A.G.; Leonardi, M.; van Meerten, E.v.P. European Guidelines on Quality Criteria for Computed Tomography. Available online: http://www.drs.dk/guidelines/ct/quality/htmlindex.htm (accessed on 26 March 2020).
- Wang, R.; Liu, X.; Schoepf, U.J.; van Assen, M.; Alimohamed, I.; Griffith, L.P.; Luo, T.; Sun, Z.; Fan, Z.; Xu, L. Extracellular volume quantitation using dual-energy CT in patients with heart failure: Comparison with 3T cardiac MR. Int. J. Cardiol. 2018, 268, 236–240. [Google Scholar] [CrossRef] [Green Version]
- Scully, P.R.; Patel, K.P.; Saberwal, B.; Klotz, E.; Augusto, J.B.; Thornton, G.D.; Hughes, R.K.; Manisty, C.; Lloyd, G.; Newton, J.D.; et al. Identifying Cardiac Amyloid in Aortic Stenosis. JACC Cardiovasc. Imaging 2020, 13, 2177–2189. [Google Scholar] [CrossRef]
- Esposito, A.; Palmisano, A.; Barbera, M.; Vignale, D.; Benedetti, G.; Spoladore, R.; Ancona, M.B.; Giannini, F.; Oppizzi, M.; Del Maschio, A.; et al. Cardiac Computed Tomography in Troponin-Positive Chest Pain: Sometimes the Answer Lies in the Late Iodine Enhancement or Extracellular Volume Fraction Map. JACC. Cardiovasc. Imaging 2019, 12, 745–748. [Google Scholar] [CrossRef] [PubMed]
- Si-Mohamed, S.A.; Douek, P.C.; Boussel, L. Spectral CT: Dual energy CT towards multienergy CT. J. Imag. Diagn. Interv. 2019, 2, 32–45. [Google Scholar] [CrossRef]
- Si-Mohamed, S.; Bar-Ness, D.; Sigovan, M.; Cormode, D.P.; Coulon, P.; Coche, E.; Vlassenbroek, A.; Normand, G.; Boussel, L.; Douek, P. Review of an initial experience with an experimental spectral photon-counting computed tomography system. Nucl. Instrum. Methods Phys. Res. Sect. A Accel. Spectrometers Detect. Assoc. Equip. 2017, 873, 27–35. [Google Scholar] [CrossRef]
- Si-Mohamed, S.; Moreau-Triby, C.; Tylski, P.; Tatard-Leitman, V.; Wdowik, Q.; Boccalini, S.; Dessouky, R.; Douek, P.; Boussel, L. Head-to-head comparison of lung perfusion with dual-energy CT and SPECT-CT. Diagn. Interv. Imaging 2020, 101, 299–310. [Google Scholar] [CrossRef]
- Gräni, C.; Bière, L.; Eichhorn, C.; Kaneko, K.; Agarwal, V.; Aghayev, A.; Steigner, M.; Blankstein, R.; Jerosch-Herold, M.; Kwong, R.Y. Incremental value of extracellular volume assessment by cardiovascular magnetic resonance imaging in risk stratifying patients with suspected myocarditis. Int. J. Cardiovasc. Imaging 2019, 35, 1067–1078. [Google Scholar] [CrossRef] [PubMed]
- Nadjiri, J.; Nieberler, H.; Hendrich, E.; Greiser, A.; Will, A.; Martinoff, S.; Hadamitzky, M. Performance of native and contrast-enhanced T1 mapping to detect myocardial damage in patients with suspected myocarditis: A head-to-head comparison of different cardiovascular magnetic resonance techniques. Int. J. Cardiovasc. Imaging 2017, 33, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Luetkens, J.A.; Doerner, J.; Thomas, D.K.; Dabir, D.; Gieseke, J.; Sprinkart, A.M.; Fimmers, R.; Stehning, C.; Homsi, R.; Schwab, J.O.; et al. Acute myocarditis: Multiparametric cardiac MR imaging. Radiology 2014, 273, 383–392. [Google Scholar] [CrossRef] [Green Version]
- Radunski, U.K.; Lund, G.K.; Stehning, C.; Schnackenburg, B.; Bohnen, S.; Adam, G.; Blankenberg, S.; Muellerleile, K. CMR in patients with severe myocarditis: Diagnostic value of quantitative tissue markers including extracellular volume imaging. JACC Cardiovasc. Imaging 2014, 7, 667–675. [Google Scholar] [CrossRef] [Green Version]
- Lurz, P.; Luecke, C.; Eitel, I.; Föhrenbach, F.; Frank, C.; Grothoff, M.; de Waha, S.; Rommel, K.-P.; Lurz, J.A.; Klingel, K.; et al. Comprehensive Cardiac Magnetic Resonance Imaging in Patients With Suspected Myocarditis: The MyoRacer-Trial. J. Am. Coll. Cardiol. 2016, 67, 1800–1811. [Google Scholar] [CrossRef]
- von Knobelsdorff-Brenkenhoff, F.; Schüler, J.; Dogangüzel, S.; Dieringer, M.A.; Rudolph, A.; Greiser, A.; Kellman, P.; Schulz-Menger, J. Detection and Monitoring of Acute Myocarditis Applying Quantitative Cardiovascular Magnetic Resonance. Circ. Cardiovasc. Imaging 2017, 10, e005242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, J.A.; Lee, Y.J.; Salerno, M. Diagnostic Performance of Extracellular Volume, Native T1, and T2 Mapping versus Lake Louise Criteria by CMR for Detection of Acute Myocarditis: A Meta-Analysis. Circ. Cardiovasc. Imaging 2018, 11, e007598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Si-Mohamed, S.A.; Congi, A.; Ziegler, A.; Tomasevic, D.; Tatard-Leitman, V.; Broussaud, T.; Boccalini, S.; Bensalah, M.; Rouvière, A.-S.; Bonnefoy-Cudraz, E.; et al. Early Prediction of Cardiac Complications in Acute Myocarditis by Means of Extracellular Volume Quantification With the Use of Dual-Energy Computed Tomography. JACC Cardiovasc. Imaging 2021. [Google Scholar] [CrossRef]
- Bouleti, C.; Baudry, G.; Iung, B.; Arangalage, D.; Abtan, J.; Ducrocq, G.; Steg, P.-G.; Vahanian, A.; Henry-Feugeas, M.-C.; Pasi, N.; et al. Usefulness of Late Iodine Enhancement on Spectral CT in Acute Myocarditis. JACC Cardiovasc. Imaging 2017, 10, 826–827. [Google Scholar] [CrossRef] [PubMed]
- Oda, S.; Emoto, T.; Nakaura, T.; Kidoh, M.; Utsunomiya, D.; Funama, Y.; Nagayama, Y.; Takashio, S.; Ueda, M.; Yamashita, T.; et al. Myocardial Late Iodine Enhancement and Extracellular Volume Quantification with Dual-Layer Spectral Detector Dual-Energy Cardiac CT. Radiol. Cardiothorac. Imaging 2019, 1, e180003. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Myocarditis Group | Control Group | |||||
|---|---|---|---|---|---|---|---|
| Variables | n | Mean ± MSE | Median (Min–Max) | n | Mean ± MSE | Median (Min–Max) | p |
| Sex | 60 | 49M, 11F | 18 | 11M, 7F | 0.602 | ||
| Age (years) | 60 | 32.9 ± 1.4 | 29.8 (18.0; 73.6) | 18 | 35.1 ± 3.6 | 33.0 (15.0; 68.2) | 0.731 |
| Weight (kg) | 60 | 75.0 ± 1.7 | 74.0 (50.0; 110.0) | 18 | 73.8 ± 4.2 | 72.5 (39.0; 106.0) | 0.606 |
| Height (cm) | 60 | 173.4 ± 1.0 | 173.0 (158; 194) | 18 | 171.4 ± 2.3 | 172.5 (150; 185) | 0.622 |
| BMI (kg/m2) | 60 | 24.9 ± 0.5 | 24.2 (17.2; 38.4) | 18 | 24.9 ± 1.1 | 24.9 (17.3; 33.9) | 0.962 |
| LVEF (%) | 60 | 57.6 ± 1.0 | 60.0 (42.0; 74.0) | 18 | 64.2 ± 1.7 | 66.0 (55.0; 78.0) | 0.006 * |
| Creatinine (µmol/L) | 10 | 73.1 ± 4.1 | 75.0 (50.0; 88.0) | 18 | 75.4 ± 3.8 | 72.0 (52.0; 111.0) | 0.885 |
| Troponins (ng/L) | 60 | 8630.3 ± 1585.9 | 5365.0 (36.0; 62,929.0) | 18 | 822.5 ± 339.9 | 214.5 (5.0; 5159.0) | 0.001 * |
| BNP (ng/L) | 44 | 137.4 ± 45.4 | 46.5 (0.1; 1700.0) | 16 | 140.6 ± 76.0 | 35.0 (0.1; 1018.0) | 0.303 |
| Hematocrit (%) | 60 | 42.2 ± 0.5 | 42.2 (33.3; 54.0) | 18 | 42.7 ± 1.0 | 42.8 (35.4; 49.8) | 0.589 |
| ECV for MG (n = 60) | ECV for CG (n = 18) | |
|---|---|---|
| Mean | 34.18 * | 30.04 |
| Mean Standard Error | 0.43 | 0.53 |
| Median | 34.61 | 29.93 |
| Minimum | 27.10 | 24.99 |
| Maximum | 40.54 | 33.06 |
| 25% Percentile | 32.12 | 28.97 |
| 50% Percentile | 34.61 | 29.93 |
| 75% Percentile | 36.39 | 31.73 |
| Parameters | ECV MG | ECV CG | ||||
|---|---|---|---|---|---|---|
| n | Rho Spearman | p | n | Rho Spearman | p | |
| Weight | 60 | −0.033 | 0.803 | 18 | −0.423 | 0.080 |
| Height | 60 | 0.016 | 0.903 | 18 | −0.362 | 0.140 |
| BMI | 60 | −0.078 | 0.552 | 18 | −0.311 | 0.210 |
| Troponins | 60 | 0.408 | 0.001 * | 18 | −0.169 | 0.504 |
| LVEF | 60 | −0.199 | 0.128 | 18 | −0.057 | 0.822 |
| BNP | 44 | 0.455 | 0.002 * | 16 | 0.035 | 0.896 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Si-Mohamed, S.A.; Restier, L.M.; Branchu, A.; Boccalini, S.; Congi, A.; Ziegler, A.; Tomasevic, D.; Bochaton, T.; Boussel, L.; Douek, P.C. Diagnostic Performance of Extracellular Volume Quantified by Dual-Layer Dual-Energy CT for Detection of Acute Myocarditis. J. Clin. Med. 2021, 10, 3286. https://doi.org/10.3390/jcm10153286
Si-Mohamed SA, Restier LM, Branchu A, Boccalini S, Congi A, Ziegler A, Tomasevic D, Bochaton T, Boussel L, Douek PC. Diagnostic Performance of Extracellular Volume Quantified by Dual-Layer Dual-Energy CT for Detection of Acute Myocarditis. Journal of Clinical Medicine. 2021; 10(15):3286. https://doi.org/10.3390/jcm10153286
Chicago/Turabian StyleSi-Mohamed, Salim Aymeric, Lauria Marie Restier, Arthur Branchu, Sara Boccalini, Anaelle Congi, Arthur Ziegler, Danka Tomasevic, Thomas Bochaton, Loic Boussel, and Philippe Charles Douek. 2021. "Diagnostic Performance of Extracellular Volume Quantified by Dual-Layer Dual-Energy CT for Detection of Acute Myocarditis" Journal of Clinical Medicine 10, no. 15: 3286. https://doi.org/10.3390/jcm10153286