
Prone Positioning Is Safe and May Reduce the Rate of Intubation in Selected COVID-19 Patients Receiving High-Flow Nasal Oxygen Therapy

 ,
, 
 , and
, and
Abstract
:1. Introduction
2. Methods
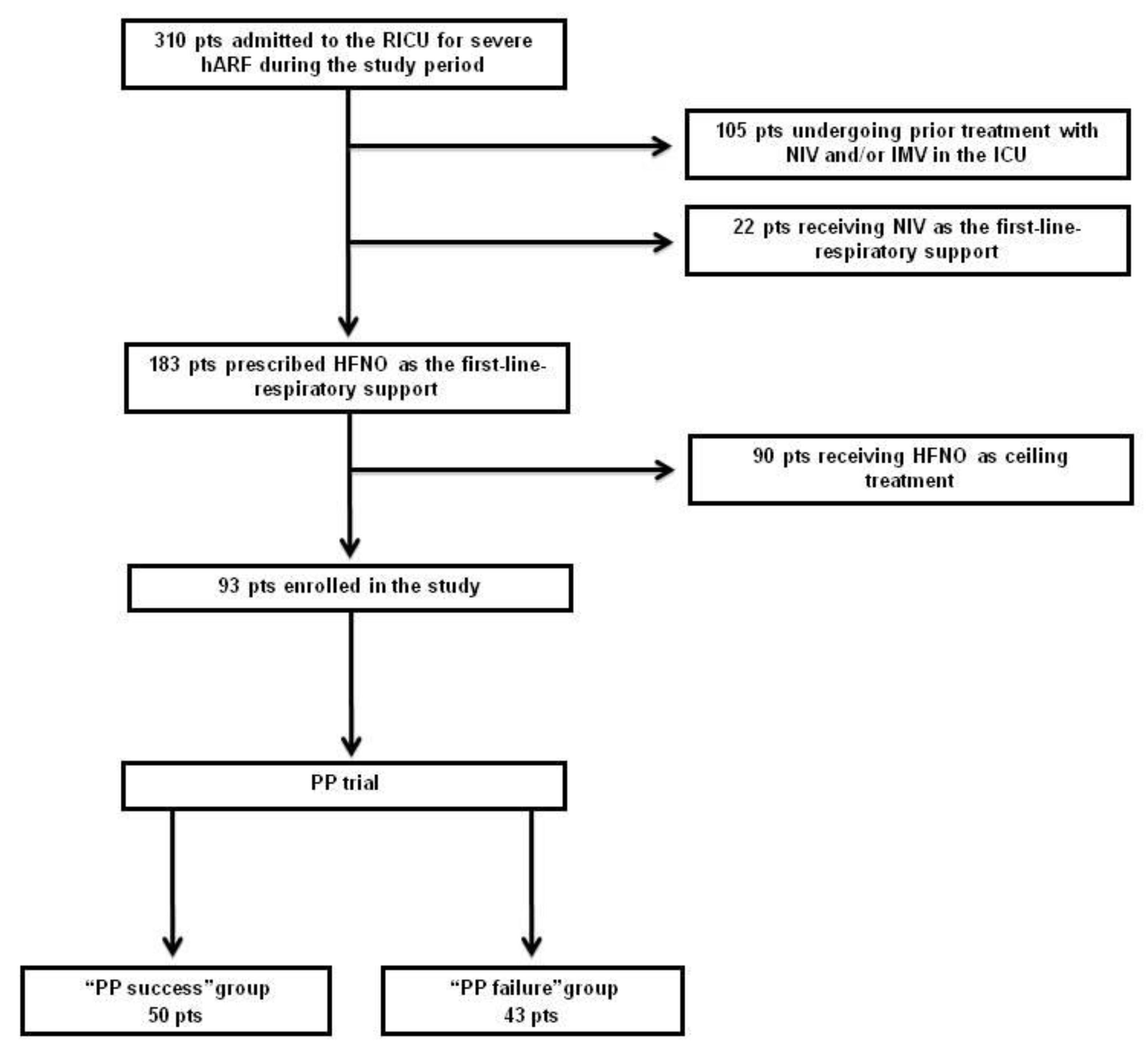
2.1. Patients
2.2. Interventions
2.3. Outcome Measures and Statistical Analysis
3. Results
3.1. Feasibility
3.2. Safety
3.3. Efficacy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease Is Suspected: Interim Guidance, 13 March 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Nasa, P.; Azoulay, E.; Khanna, A.K.; Jain, R.; Gupta, S.; Javeri, Y.; Juneja, D.; Rangappa, P.; Sundararajan, K.; Alhazzani, W.; et al. Expert consensus statements for the management of COVID-19-related acute respira-tory failure using a Delphi method. Crit. Care 2021, 25, 106. [Google Scholar] [CrossRef]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med. 2020, 46, 854–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarantonello, F.; Andreatta, G.; Sella, N.; Navalesi, P. Prone position and lung ventilation and perfusion matching in acute res-piratory failure due to COVID-19. Am. J. Respir. Crit. Care Med. 2020, 202, 278–279. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Qiu, H.; Huang, M.; Yang, Y. Lower mortality of COVID-19 by early recognition and intervention: Experience from Jiangsu Province. Ann. Intensive Care 2020, 10, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Q.; Wang, T.; Qin, X.; Jie, Y.; Zha, L.; Lu, W. Early awake prone position combined with high-flow nasal oxygen therapy in severe COVID-19: A case series. Crit. Care 2020, 24, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Ng, Z.; Tay, W.C.; Ho, C.H.B. Rationale and significance of patient selection in awake prone positioning for COVID-19 pneu-monia. Eur. Respir. J. 2020, 56, 2002571. [Google Scholar] [CrossRef] [PubMed]
- Hallifax, R.J.; Porter, B.M.; Elder, P.J.; Evans, S.B.; Turnbull, C.D.; Hynes, G.; Lardner, R.; Archer, K.; Bettinson, H.V.; Nickol, A.H.; et al. Successful awake proning is associated with improved clinical outcomes in patients with COVID-19: Single-centre high-dependency unit experience. BMJ Open Respir. Res. 2020, 7, e000678. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Roca, O.; Messika, J.; Caralt, B.; García-de-Acilu, M.; Sztrymf, B.; Ricard, J.D.; Masclans, J.R. Predicting success of highflow nasal cannula in pneumonia patients with hypoxemic res-piratory failure: The utility of the ROX index. J. Crit. Care 2016, 35, 200–205. [Google Scholar] [CrossRef]
- Vincent, J.L.; De Mendonça, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M.; Sprung, C.L.; Colardyn, F.; Blecher, S. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: Results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Giraudo, C.; Cavaliere, A.; Fichera, G.; Weber, M.; Motta, R.; Pelloso, M.; Tosato, F.; Lupi, A.; Calabrese, F.; Carretta, G.; et al. Validation of a composed COVID-19 chest radiography score: The CARE project. ERJ Open Res. 2020, 6, 00359–02020. [Google Scholar] [CrossRef] [PubMed]
- Vianello, A.; Arcaro, G.; Molena, B.; Turato, C.; Sukthi, A.; Guarnieri, G.; Lugato, F.; Senna, G.; Navalesi, P. High-flow nasal cannula oxygen therapy to treat patients with hypoxemic acute res-piratory failure consequent to SARS-CoV-2 infection. Thorax 2020, 75, 998–1000. [Google Scholar] [CrossRef] [PubMed]
- McNicholas, B.; Cosgrave, D.; Giacomini, C.; Brennan, A.; Laffey, J.G. Prone positioning in COVID-19 acute respiratory failure: Just do it? Br. J. Anaesth. 2020, 125, 440–443. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, C.; Mellado-Artigas, R.; Gea, A.; Arruti, E.; Aldecoa, C.; Adalia, R.; Ramasco, F.; Monedero, P.; Maseda, E.; Tamayo, G.; et al. Awake prone positioning does not reduce the risk of intubation in COVID-19 treated with high-flow nasal oxygen therapy: A multicenter, adjusted cohort study. Crit. Care 2020, 24, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Pasin, L.; Sella, N.; Correale, C.; Boscolo, A.; Rosi, P.; Saia, M.; Mantoan, D.; Navalesi, P. Regional COVID-19 Network for Coordination of SARS-CoV-2 outbreak in Veneto, Italy. J. Cardiothorac. Vasc. Anesth. 2020, 34, 2341–2345. [Google Scholar] [CrossRef] [PubMed]
- Coppo, A.; Bellani, G.; Winterton, D.; Di Pierro, M.; Soria, A.; Faverio, P.; Cairo, M.; Mori, S.; Messinesi, G.; Contro, E.; et al. Feasibility and physiological effects of prone positioning in non-intubated patients with acute respiratory failure due to COVID-19 (PRON-COVID): A prospective cohort study. Lancet Respir. Med. 2020, 8, 765–774. [Google Scholar] [CrossRef]
- Elharrar, X.; Trigui, Y.; Dols, A.-M.; Touchon, F.; Martinez, S.; Prud’Homme, E.; Papazian, L. Use of Prone Positioning in Nonintubated Patients With COVID-19 and Hypoxemic Acute Respiratory Failure. JAMA 2020, 323, 2336–2338. [Google Scholar] [CrossRef]
- Damarla, M.; Zaeh, S.; Niedermeyer, S.; Merck, S.; Niranjan-Azadi, A.; Broderick, B.; Punjabi, N. Prone Positioning of Nonintubated Patients with COVID-19. Am. J. Respir. Crit. Care Med. 2020, 202, 604–606. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| All Cases (n = 93) | PP Success (n = 50) | PP Failure (n = 43) | p-Value | |
|---|---|---|---|---|
| Baseline demographic and clinical data | ||||
| Age (yrs), median (range) | 68(36–89) | 67 (36–89) | 69 (37–86) | 0.37 |
| Gender (M/F) | 59/34 | 33/17 | 26/17 | 0.66 |
| Smokers, N | 17 | 9 | 8 | 0.99 |
| BMI (kg/m2), median (range) | 28.0 (20.8–41.5) | 26.9 (20.8–41.5) | 28.3 (22.9–33.3) | 0.75 |
| Clinical, laboratory and blood gas data at RICU admission | ||||
| Time since symptom onset (days), median (range) | 4 (3–16) | 4 (3–10) | 4 (3–16) | 0.92 |
| Barthel index, median (range) | 50 (4–100) | 45 (10–100) | 60 (4–100) | 0.08 |
| Heart rate (beats/min), median (range) | 80 (55–126) | 80 (55–110) | 80 (60–126) | 0.29 |
| Respiratory rate (breaths/min), median (range) | 22 (13–39) | 22 (13–39) | 22 (15–32) | 0.69 |
| Pts with fever, N. (Temperature > 38 °C) | 13 | 8 | 5 | 0.76 |
| Total WBC count (×109/L), median (range) | 8.6 (1.6–23.9) | 8.3 (1.6–23.9) | 8.7 (2.4–17.2) | 0.88 |
| Pts with D-dimer level above the normal range, n | 38 | 22 | 16 | 0.09 |
| Serum CRP (μg/mL), median (range) | 96.0 (11.0–270.0) | 84.2 (11.0–230.0) | 99.5 (13.0–270.0) | 0.23 |
| PaO2 * (mmHg), median (range) | 68.0 (6.8–157.6) | 64.9 (6.8–157.6) | 68.8 (39.2–110.9) | 0.99 |
| PaCO2 (mmHg), median (range) | 33.4 (23.6–70.0) | 32.7 (23.6–60.0) | 34.9 (25.2–70.0) | 0.23 |
| Arterial pH, median (range) | 7.46 (7.25–7.56) | 7.46 (7.25–7.56) | 7.47 (7.32–7.53) | 0.79 |
| SaO2 (%), median (range) | 95 (84–100) | 94 (89–100) | 95 (84–100) | 0.93 |
| PaO2/FiO2, median (range) | 101.8 (6.8–300.0) | 107.2 (6.8–300.0) | 92.4 (52.4–240.9) | 0.35 |
| ROX index, median (range) | 5.65 (2.41–22.06) | 5.81 (2.41–21.50) | 4.94 (2.97–22.06) | 0.37 |
| SOFA score, median (range) | 2 (1–5) | 2 (1–5) | 2 (2–5) | 0.01 |
| Pts with co-morbidities, N | 87 | 45 | 42 | 0.21 |
| ACCI | 4 (0–13) | 4 (0–13) | 4 (0–8) | 0.82 |
| CARE score, median (range) | 18 (10–86) | 18 (12–86) | 16 (10–22) | <0.0001 |
| All Cases (n = 93) | PP Success (n = 50) | PP Failure (n = 43) | p-Value | |
|---|---|---|---|---|
| Patients receiving ETI, n (%) | 16 (17) | 4 (8) | 12 (28) | 0.014 |
| Patients escalating respiratory support, n (%) | 27 (29) | 9 (18) | 16 (37) | 0.059 |
| Death during hospitalization, n (%) | 9 (10) | 2 (4) | 7 (16) | 0.047 |
| Length of hospital stay (days), median (range) | 18 (6–75) | 17 (6–46) | 21 (7–75) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vianello, A.; Turrin, M.; Guarnieri, G.; Molena, B.; Arcaro, G.; Turato, C.; Braccioni, F.; Bertagna De Marchi, L.; Lionello, F.; Subotic, P.; et al. Prone Positioning Is Safe and May Reduce the Rate of Intubation in Selected COVID-19 Patients Receiving High-Flow Nasal Oxygen Therapy. J. Clin. Med. 2021, 10, 3404. https://doi.org/10.3390/jcm10153404
Vianello A, Turrin M, Guarnieri G, Molena B, Arcaro G, Turato C, Braccioni F, Bertagna De Marchi L, Lionello F, Subotic P, et al. Prone Positioning Is Safe and May Reduce the Rate of Intubation in Selected COVID-19 Patients Receiving High-Flow Nasal Oxygen Therapy. Journal of Clinical Medicine. 2021; 10(15):3404. https://doi.org/10.3390/jcm10153404
Chicago/Turabian StyleVianello, Andrea, Martina Turrin, Gabriella Guarnieri, Beatrice Molena, Giovanna Arcaro, Cristian Turato, Fausto Braccioni, Leonardo Bertagna De Marchi, Federico Lionello, Pavle Subotic, and et al. 2021. "Prone Positioning Is Safe and May Reduce the Rate of Intubation in Selected COVID-19 Patients Receiving High-Flow Nasal Oxygen Therapy" Journal of Clinical Medicine 10, no. 15: 3404. https://doi.org/10.3390/jcm10153404
APA StyleVianello, A., Turrin, M., Guarnieri, G., Molena, B., Arcaro, G., Turato, C., Braccioni, F., Bertagna De Marchi, L., Lionello, F., Subotic, P., Masiero, S., Giraudo, C., & Navalesi, P. (2021). Prone Positioning Is Safe and May Reduce the Rate of Intubation in Selected COVID-19 Patients Receiving High-Flow Nasal Oxygen Therapy. Journal of Clinical Medicine, 10(15), 3404. https://doi.org/10.3390/jcm10153404