
Role of Annual Influenza Vaccination against Lung Cancer in Type 2 Diabetic Patients from a Population-Based Cohort Study


 ,
, 

Abstract
1. Introduction
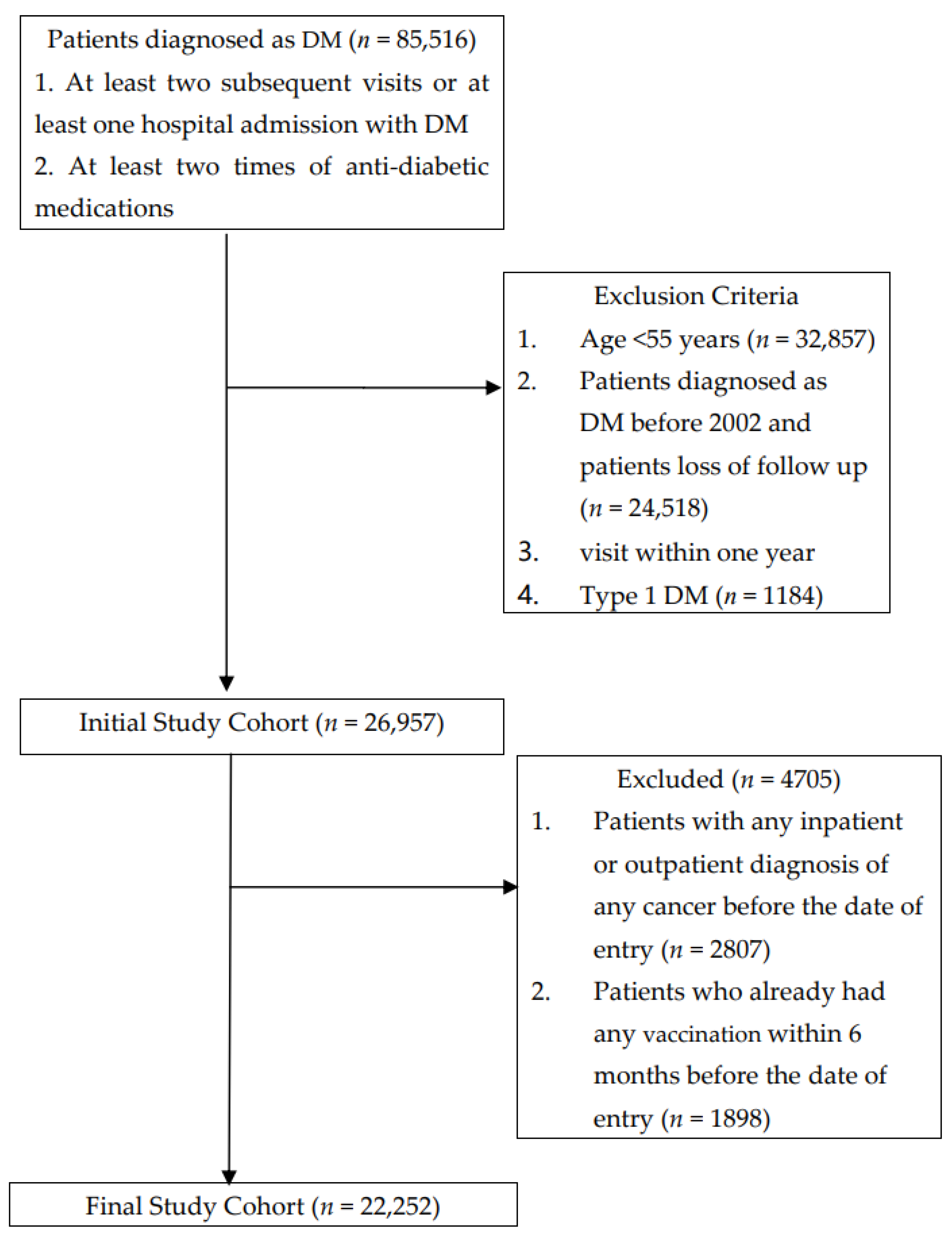
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Song, S.; Wang, B.; Zhang, X.; Hao, L.; Hu, X.; Li, Z.; Sun, S. Long-Term Diabetes Mellitus Is Associated with an Increased Risk of Pancreatic Cancer: A Meta-Analysis. PLoS ONE 2015, 10, e0134321. [Google Scholar] [CrossRef] [PubMed]
- Sasazuki, S.; Charvat, H.; Hara, A.; Wakai, K.; Nagata, C.; Nakamura, K.; Tsuji, I.; Sugawara, Y.; Tamakoshi, A.; Matsuo, K.; et al. Diabetes mellitus and cancer risk: Pooled analysis of eight cohort studies in Japan. Cancer Sci. 2013, 104, 1499–1507. [Google Scholar] [CrossRef]
- Hope, C.; Robertshaw, A.; Cheung, K.L.; Idris, I.; English, E. Relationship between HbA1c and cancer in people with or without diabetes: A systematic review. Diabet. Med. 2016, 33, 1013–1025. [Google Scholar] [CrossRef] [PubMed]
- Agache, A.; Mustatea, P.; Mihalache, O.; Bobirca, F.T.; Georgescu, D.E.; Jauca, C.M.; Birligea, A.; Doran, H.; Patrascu, T. Diabetes Mellitus as a Risk-factor for Colorectal Cancer Literature Review-Current Situation and Future Perspectives. Chirurgia 2018, 113, 603–610. [Google Scholar] [CrossRef]
- Kuriki, K.; Hirose, K.; Tajima, K. Diabetes and cancer risk for all and specific sites among Japanese men and women. Eur. J. Cancer Prev. 2007, 16, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Chlebowski, R.; Wactawski-Wende, J.; Schlecht, N.F.; Tinker, L.; Margolis, K.L. Diabetes and lung cancer among postmenopausal women. Diabet. Care 2012, 35, 1485–1491. [Google Scholar] [CrossRef]
- Jee, S.H.; Ohrr, H.; Sull, J.W.; Yun, J.E.; Ji, M.; Samet, J.M. Fasting serum glucose level and cancer risk in Korean men and women. JAMA 2005, 293, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Pallis, A.G.; Syrigos, K.N. Lung cancer in never smokers: Disease characteristics and risk factors. Crit. Rev. Oncol. Hematol. 2013, 88, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Argiles, J.M.; Lopez-Soriano, F.J. Insulin and cancer (Review). Int. J. Oncol. 2001, 18, 683–687. [Google Scholar] [CrossRef]
- Strickler, H.D.; Wylie-Rosett, J.; Rohan, T.; Hoover, D.R.; Smoller, S.; Burk, R.D.; Yu, H. The relation of type 2 diabetes and cancer. Diabetes. Technol. Ther. 2001, 3, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Forgiarini, L.A., Jr.; Kretzmann, N.A.; Porawski, M.; Dias, A.S.; Marroni, N.A. Experimental diabetes mellitus: Oxidative stress and changes in lung structure. J. Bras. Pneumol. 2009, 35, 788–791. [Google Scholar] [CrossRef]
- Lee, G.; Walser, T.C.; Dubinett, S.M. Chronic inflammation, chronic obstructive pulmonary disease, and lung cancer. Curr. Opin. Pulm. Med. 2009, 15, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Jeon, I.; Lee, J.M.; Yoon, J.M.; Park, S.M. Diabetes mellitus as an independent risk factor for lung cancer: A meta-analysis of observational studies. Eur. J. Cancer 2013, 49, 2411–2423. [Google Scholar] [CrossRef]
- Zhu, L.; Cao, H.; Zhang, T.; Shen, H.; Dong, W.; Wang, L.; Du, J. The Effect of Diabetes Mellitus on Lung Cancer Prognosis: A PRISMA-compliant Meta-analysis of Cohort Studies. Medicine 2016, 95, e3528. [Google Scholar] [CrossRef]
- Chan, T.C.; Fu, Y.C.; Wang, D.W.; Chuang, J.H. Determinants of receiving the pandemic (H1N1) 2009 vaccine and intention to receive the seasonal influenza vaccine in Taiwan. PLoS ONE 2014, 9, e101083. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.Y.; Wu, S.M.; Liu, J.C.; Lee, K.Y. Effect of annual influenza vaccination on reducing lung cancer in patients with chronic obstructive pulmonary disease from a population-based cohort study. Medicine 2019, 98, e18035. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, R.B., Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Allard, R.; Leclerc, P.; Tremblay, C.; Tannenbaum, T.N. Diabetes and the severity of pandemic influenza A (H1N1) infection. Diabetes Care 2010, 33, 1491–1493. [Google Scholar] [CrossRef] [PubMed]
- Wilking, H.; Buda, S.; von der Lippe, E.; Altmann, D.; Krause, G.; Eckmanns, T.; Haas, W. Mortality of 2009 pandemic influenza A(H1N1) in Germany. Euro. Surveill. 2010, 15, 19741. [Google Scholar] [CrossRef]
- Nojima, I.; Eikawa, S.; Tomonobu, N.; Hada, Y.; Kajitani, N.; Teshigawara, S.; Miyamoto, S.; Tone, A.; Uchida, H.A.; Nakatsuka, A.; et al. Dysfunction of CD8 + PD-1 + T cells in type 2 diabetes caused by the impairment of metabolism-immune axis. Sci. Rep. 2020, 10, 14928. [Google Scholar] [CrossRef]
- Sheridan, P.A.; Paich, H.A.; Handy, J.; Karlsson, E.A.; Schultz-Cherry, S.; Hudgens, M.; Weir, S.; Noah, T.; Beck, M.A. The antibody response to influenza vaccination is not impaired in type 2 diabetics. Vaccine 2015, 33, 3306–3313. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.B.; Baek, J.H.; Lee, J.; Song, J.Y.; Lee, J.S.; Cheong, H.J.; Kim, W.J. Long-Term Immunogenicity and Safety of a Conventional Influenza Vaccine in Patients with Type 2 Diabetes. Clin. Vaccine Immunol. 2015, 22, 1160–1165. [Google Scholar] [CrossRef] [PubMed]
- McElhaney, J.E.; Garneau, H.; Camous, X.; Dupuis, G.; Pawelec, G.; Baehl, S.; Tessier, D.; Frost, E.H.; Frasca, D.; Larbi, A.; et al. Predictors of the antibody response to influenza vaccination in older adults with type 2 diabetes. BMJ Open. Diabetes Res. Care 2015, 3, e000140. [Google Scholar] [CrossRef]
- Newman, J.H.; Chesson, C.B.; Herzog, N.L.; Bommareddy, P.K.; Aspromonte, S.M.; Pepe, R.; Estupinian, R.; Aboelatta, M.M.; Buddhadev, S.; Tarabichi, S.; et al. Intratumoral injection of the seasonal flu shot converts immunologically cold tumors to hot and serves as an immunotherapy for cancer. Proc. Natl. Acad. Sci. USA 2020, 117, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Chang, F.C.; Sung, H.Y.; Zhu, S.H.; Chiou, S.T. Impact of the 2009 Taiwan tobacco hazards prevention act on smoking cessation. Addiction 2014, 109, 140–146. [Google Scholar] [CrossRef]
- Ozlu, T.; Bulbul, Y. Smoking and lung cancer. Tuberk. Toraks 2005, 53, 200–209. [Google Scholar] [PubMed]
- Murin, S.; Bilello, K.S. Respiratory tract infections: Another reason not to smoke. Cleve Clin. J. Med. 2005, 72, 916–920. [Google Scholar] [CrossRef]
- Feng, Y.; Kong, Y.; Barnes, P.F.; Huang, F.F.; Klucar, P.; Wang, X.; Samten, B.; Sengupta, M.; Machona, B.; Donis, R.; et al. Exposure to cigarette smoke inhibits the pulmonary T-cell response to influenza virus and Mycobacterium tuberculosis. Infect. Immun. 2011, 79, 229–237. [Google Scholar] [CrossRef]
- Epstein, M.A.; Reynaldo, S.; El-Amin, A.N. Is smoking a risk factor for influenza hospitalization and death? J. Infect. Dis. 2010, 201, 794–795. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Almirall, J.; Bolibar, I.; Serra-Prat, M.; Roig, J.; Hospital, I.; Carandell, E.; Agusti, M.; Ayuso, P.; Estela, A.; Torres, A.; et al. New evidence of risk factors for community-acquired pneumonia: A population-based study. Eur. Respir. J. 2008, 31, 1274–1284. [Google Scholar] [CrossRef] [PubMed]
- Godoy, P.; Castilla, J.; Soldevila, N.; Mayoral, J.M.; Toledo, D.; Martin, V.; Astray, J.; Egurrola, M.; Morales-Suarez-Varela, M.; Dominguez, A.; et al. Smoking may increase the risk of influenza hospitalization and reduce influenza vaccine effectiveness in the elderly. Eur J. Public Health 2018, 28, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Chambers, C.; Skowronski, D.M.; Rose, C.; Serres, G.; Winter, A.L.; Dickinson, J.A.; Jassem, A.; Gubbay, J.B.; Fonseca, K.; Drews, S.J.; et al. Should Sex Be Considered an Effect Modifier in the Evaluation of Influenza Vaccine Effectiveness? Open. Forum. Infect. Dis. 2018, 5, ofy211. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Pekosz, A. Sex-based biology and the rational design of influenza vaccination strategies. J. Infect. Dis. 2014, 209, S114–S119. [Google Scholar] [CrossRef]
- Gabriel, G.; Arck, P.C. Sex, immunity and influenza. J. Infect. Dis. 2014, 209, S93–S99. [Google Scholar] [CrossRef] [PubMed]
- Weng, C.F.; Chen, L.J.; Lin, C.W.; Chen, H.M.; Lee, H.H.; Ling, T.Y.; Hsiao, F.Y. Association between the risk of lung cancer and influenza: A population-based nested case-control study. Int. J. Infect. Dis. 2019, 88, 8–13. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Whole Cohort (n = 22,252) | Unvaccinated (n = 14,392) | Vaccinated (n = 7860) | p | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Age, years (Mean ± SD) | 66.48 (8.70) | 64.64 (8.74) | 69.85 (7.54) | <0.001 | |||
| 55–64 | 11,464 | 51.52 | 9111 | 63.31 | 2353 | 29.94 | <0.001 |
| 65–74 | 6749 | 30.33 | 3202 | 22.25 | 3547 | 45.13 | |
| ≥75 | 4039 | 18.15 | 2079 | 14.45 | 1960 | 24.94 | |
| Gender | |||||||
| Female | 11,248 | 50.55 | 7032 | 48.86 | 4216 | 53.64 | <0.001 |
| Male | 11,004 | 49.45 | 7360 | 51.14 | 3644 | 46.36 | |
| CCI Index | |||||||
| 0 | 6821 | 30.65 | 4743 | 32.96 | 2078 | 26.44 | <0.001 |
| 1 | 5959 | 26.78 | 3881 | 26.97 | 2078 | 26.44 | |
| 2 | 4322 | 19.42 | 2689 | 18.68 | 1633 | 20.78 | |
| ≥3 | 5150 | 23.14 | 3079 | 21.39 | 2071 | 26.35 | |
| Hypertension | |||||||
| No | 7775 | 34.94 | 5389 | 37.44 | 2386 | 30.36 | <0.001 |
| Yes | 14,477 | 65.06 | 9003 | 62.56 | 5474 | 69.64 | |
| Dyslipidemia | |||||||
| No | 14,300 | 64.26 | 9263 | 64.36 | 5037 | 64.08 | 0.679 |
| Yes | 7952 | 35.74 | 5129 | 35.64 | 2823 | 35.92 | |
| Hypoglycemic medications | |||||||
| Insulin and analogues | 3788 | 17.02 | 2242 | 15.58 | 1546 | 19.67 | <0.001 |
| Biguanides | 16,711 | 75.10 | 10,813 | 75.13 | 5898 | 75.04 | 0.877 |
| Sulfonamides, urea derivatives | 14,330 | 64.40 | 8980 | 62.40 | 5350 | 68.07 | <0.001 |
| Alpha glucosidase inhibitors | 3889 | 17.48 | 2325 | 16.15 | 1564 | 19.90 | <0.001 |
| Thiazolidinediones | 2949 | 13.25 | 1770 | 12.30 | 1179 | 15.00 | <0.001 |
| Dipeptidyl peptidase 4 (DPP-4) | 3089 | 13.88 | 1975 | 13.72 | 1114 | 14.17 | 0.353 |
| Oral blood glucose lowering | 2808 | 12.62 | 1843 | 12.81 | 965 | 12.28 | 0.257 |
| Other blood glucose lowering drugs | 2917 | 13.11 | 1700 | 11.81 | 1217 | 15.48 | <0.001 |
| Number of hypoglycemic medications | |||||||
| 0–1 | 6652 | 29.89 | 4522 | 31.42 | 2130 | 27.10 | <0.001 |
| 2-3 | 9987 | 44.88 | 6587 | 45.77 | 3400 | 43.26 | |
| >3 | 5613 | 25.22 | 3283 | 22.81 | 2330 | 29.64 | |
| Combined medications | |||||||
| Statins | |||||||
| <28 days | 11,051 | 49.66 | 7428 | 51.61 | 3623 | 46.09 | <0.001 |
| 28–365 days | 5150 | 23.14 | 3418 | 23.75 | 1732 | 22.04 | |
| >365 days | 6051 | 27.19 | 3546 | 24.64 | 2505 | 31.87 | |
| Aspirin | |||||||
| <28 days | 12,296 | 55.26 | 8908 | 61.90 | 3388 | 43.10 | <0.001 |
| 28–365 days | 4192 | 18.84 | 2535 | 17.61 | 1657 | 21.08 | |
| >365 days | 5764 | 25.90 | 2949 | 20.49 | 2815 | 35.81 | |
| ACEI and ARB | |||||||
| <28 days | 8138 | 36.57 | 6026 | 41.87 | 2112 | 26.87 | <0.001 |
| 28–365 days | 4765 | 21.41 | 3174 | 22.05 | 1591 | 20.24 | |
| >365 days | 9349 | 42.01 | 5192 | 36.08 | 4157 | 52.89 | |
| Level of Urbanization | |||||||
| Urban | 15,587 | 70.05 | 10,619 | 73.78 | 4968 | 63.21 | <0.001 |
| Suburban | 4432 | 19.92 | 2626 | 18.25 | 1806 | 22.98 | |
| Rural | 2233 | 10.04 | 1147 | 7.97 | 1086 | 13.82 | |
| Monthly income (NT$) | |||||||
| 0 | 2016 | 9.06 | 1129 | 7.84 | 887 | 11.28 | <0.001 |
| 1–19,200 | 6212 | 27.92 | 3687 | 25.62 | 2525 | 32.12 | |
| 19,200–25,000 | 6746 | 30.32 | 3896 | 27.07 | 2850 | 36.26 | |
| ≥25,001 | 7278 | 32.71 | 5680 | 39.47 | 1598 | 20.33 | |
| All Group (n = 22,252) | Unvaccinated (Total Follow-Up 59,866.2 Person-Years) | Vaccinated (Total Follow-Up 51,033.7 Person-Years) | Adjusted HR † (95% C.I.) | ||
|---|---|---|---|---|---|
| No. of Patients With Cancer | Incidence Rate (per 105 Person-Years) (95% C.I.) | No. of Patients With Cancer | Incidence Rate (per 105 Person-Years) (95% C.I.) | ||
| Whole cohort | 244 | 407.6 (356.4, 458.7) | 165 | 323.3 (274.0, 372.6) | 0.77 (0.62, 0.95) * |
| Age (years) | |||||
| 55–64 a | 112 | 268.9 (219.1, 318.7) | 28 | 151.9 (95.6, 208.2) | 0.61 (0.40, 0.94) * |
| 65–74 b | 74 | 600.0 (463.3, 736.8) | 87 | 386.1 (305.0, 467.3) | 0.74 (0.54, 1.03) |
| ≥75 c | 58 | 986.4 (732.5, 1240.2) | 50 | 496.5 (358.9, 634.1) | 0.63 (0.42, 0.92) * |
| Sex | |||||
| Female d | 77 | 254.3 (197.5, 311.1) | 64 | 226.4 (170.9, 281.8) | 0.85 (0.60, 1.22) |
| Male e | 167 | 564.4 (478.8, 650.0) | 101 | 443.7 (357.2, 530.2) | 0.72 (0.55, 0.94) * |
| Unvaccinated | Vaccinated | p for Trend | |||
|---|---|---|---|---|---|
| 1 | 2–3 | ≥4 | |||
| Adjusted HR (95% C.I.) | Adjusted HR (95% C.I.) | Adjusted HR (95% C.I.) | Adjusted HR (95% C.I.) | ||
| Main model † | 1.00 | 0.95(0.72, 1.26) | 0.88(0.67, 1.16) | 0.42(0.29, 0.61) *** | <0.001 |
| Subgroup effects | |||||
| Age, years | |||||
| 55–64 | 1.00 | 0.60(0.32, 1.11) | 0.66(0.35, 1.24) | 0.56(0.24, 1.28) | 0.041 |
| 65–74 | 1.00 | 1.08(0.71, 1.64) | 0.90(0.60, 1.36) | 0.37(0.23, 0.62) *** | <0.001 |
| ≥75 | 1.00 | 0.82(0.49, 1.37) | 0.68(0.41, 1.12) | 0.31(0.15, 0.66) ** | 0.002 |
| Sex | |||||
| Female | 1.00 | 1.01(0.63, 1.63) | 0.97(0.61, 1.53) | 0.53(0.30, 0.95) * | 0.076 |
| Male | 1.00 | 0.93(0.65, 1.32) | 0.84(0.59, 1.20) | 0.35(0.21, 0.57) *** | <0.001 |
| CCI Index | |||||
| 0 | 1.00 | 0.97(0.58, 1.62) | 0.72(0.41, 1.26) | 0.35(0.17, 0.75) ** | 0.006 |
| 1 | 1.00 | 0.71(0.37, 1.34) | 1.08(0.63, 1.86) | 0.50(0.25, 0.99) * | 0.130 |
| 2 | 1.00 | 1.20(0.66, 2.17) | 1.03(0.57, 1.86) | 0.40(0.16, 0.97) * | 0.124 |
| ≥3 | 1.00 | 0.89(0.52, 1.52) | 0.70(0.40, 1.21) | 0.38(0.18, 0.80) * | 0.009 |
| Hypertension | |||||
| No | 1.00 | 1.11(0.70, 1.76) | 1.14(0.72, 1.81) | 0.56(0.31, 1.01) | 0.196 |
| Yes | 1.00 | 0.86(0.60, 1.24) | 0.77(0.54, 1.09) | 0.35(0.22, 0.57) *** | <0.001 |
| Dyslipidemia | |||||
| No | 1.00 | 0.90(0.63, 1.27) | 0.98(0.70, 1.36) | 0.39(0.24, 0.62) *** | 0.001 |
| Yes | 1.00 | 1.06(0.65, 1.72) | 0.69(0.41, 1.16) | 0.46(0.24, 0.85) * | 0.010 |
| Insulins and analogues | |||||
| No (<28 days) | 1.00 | 0.93(0.69, 1.26) | 0.84(0.62, 1.13) | 0.36(0.23, 0.54) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 1.07(0.49, 2.33) | 1.12(0.54, 2.34) | 0.75(0.32, 1.75) | 0.666 |
| Biguanides | |||||
| No (<28 days) | 1.00 | 0.73(0.47, 1.13) | 0.67(0.43, 1.04) | 0.30(0.15, 0.59) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 1.09(0.75, 1.58) | 1.02(0.71, 1.46) | 0.49(0.31, 0.77) ** | 0.013 |
| Sulfonamides, urea derivatives | |||||
| No (<28 days) | 1.00 | 0.81(0.53, 1.25) | 0.59(0.37, 0.94) * | 0.35(0.19, 0.65) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 1.04(0.72, 1.52) | 1.08(0.76, 1.54) | 0.45(0.28, 0.72) *** | 0.011 |
| Alpha glucosidase inhibitors | |||||
| No (<28 days) | 1.00 | 0.86(0.63, 1.17) | 0.85(0.63, 1.15) | 0.41(0.27, 0.62) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 1.63(0.78, 3.40) | 1.04(0.47, 2.32) | 0.45(0.16, 1.24) | 0.197 |
| Thiazolidinediones | |||||
| No (<28 days) | 1.00 | 0.94(0.70, 1.26) | 0.81(0.60, 1.09) | 0.37(0.25, 0.55) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.96(0.35, 2.60) | 1.57(0.69, 3.62) | 0.88(0.31, 2.54) | 0.783 |
| Dipeptidyl peptidase 4 (DPP-4) | |||||
| No (<28 days) | 1.00 | 0.93(0.70, 1.24) | 0.85(0.64, 1.12) | 0.40(0.28, 0.59) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.61(0.07, 5.21) | 1.50(0.35, 6.34) | 0.46(0.05, 4.30) | 0.782 |
| Oral blood glucose lowering | |||||
| No (< 28 days) | 1.00 | 0.98(0.73, 1.31) | 0.88(0.66, 1.18) | 0.43(0.29, 0.63) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.44(0.10, 1.96) | 0.72(0.22, 2.31) | 0.14(0.02, 1.15) | 0.062 |
| Other hypoglycemic medications | |||||
| No (<28 days) | 1.00 | 0.99(0.74, 1.32) | 0.80(0.59, 1.08) | 0.39(0.26, 0.59) *** | <0.001 |
| Yes (≥28 days) | 1.00 | 0.38(0.09, 1.66) | 1.66(0.75, 3.65) | 0.54(0.17, 1.69) | 0.822 |
| Number of hypoglycemic medications | |||||
| 0–1 | 1.00 | 0.70(0.45, 1.10) | 0.55(0.34, 0.87) * | 0.32(0.17, 0.59) *** | <0.001 |
| 2–3 | 1.00 | 1.34(0.89, 2.03) | 1.02(0.66, 1.57) | 0.42(0.23, 0.76) ** | 0.022 |
| >3 | 1.00 | 0.66(0.29, 1.51) | 1.30(0.69, 2.44) | 0.53(0.23, 1.21) | 0.387 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, J.-Q.; Lin, C.-H.; Chen, C.-C.; Lin, Y.-F.; Chiu, C.-C.; Yang, T.Y.; Hsu, M.-H.; Fang, Y.-A.; Hao, W.-R.; Liu, J.-C.; et al. Role of Annual Influenza Vaccination against Lung Cancer in Type 2 Diabetic Patients from a Population-Based Cohort Study. J. Clin. Med. 2021, 10, 3434. https://doi.org/10.3390/jcm10153434
Zheng J-Q, Lin C-H, Chen C-C, Lin Y-F, Chiu C-C, Yang TY, Hsu M-H, Fang Y-A, Hao W-R, Liu J-C, et al. Role of Annual Influenza Vaccination against Lung Cancer in Type 2 Diabetic Patients from a Population-Based Cohort Study. Journal of Clinical Medicine. 2021; 10(15):3434. https://doi.org/10.3390/jcm10153434
Chicago/Turabian StyleZheng, Jing-Quan, Cheng-Hsin Lin, Chun-Chao Chen, Yuan-Feng Lin, Chun-Chih Chiu, Tsung Yeh Yang, Min-Huei Hsu, Yu-Ann Fang, Wen-Rui Hao, Ju-Chi Liu, and et al. 2021. "Role of Annual Influenza Vaccination against Lung Cancer in Type 2 Diabetic Patients from a Population-Based Cohort Study" Journal of Clinical Medicine 10, no. 15: 3434. https://doi.org/10.3390/jcm10153434
APA StyleZheng, J.-Q., Lin, C.-H., Chen, C.-C., Lin, Y.-F., Chiu, C.-C., Yang, T. Y., Hsu, M.-H., Fang, Y.-A., Hao, W.-R., Liu, J.-C., & Lee, K.-Y. (2021). Role of Annual Influenza Vaccination against Lung Cancer in Type 2 Diabetic Patients from a Population-Based Cohort Study. Journal of Clinical Medicine, 10(15), 3434. https://doi.org/10.3390/jcm10153434