Abstract
Background: The association between markers of inflammation (interleukin (IL)-6 and IL-10), monocyte activation (sCD163 and sCD14), and microbial translocation (lipopolysaccharide (LPS) and LPS binding protein) and liver fibrosis in patients with alcohol use disorder (AUD) and no overt liver disease is not well established. Methods: We studied patients admitted for treatment of AUD at two hospitals in Barcelona. Advanced liver fibrosis (ALF) was defined as FIB-4 > 3.25. Results: A total of 353 participants (76.3% male) were included and 94 (26.5%) had ALF. In adjusted correlation analyses, sCD163, sCD14, IL-6, IL-10, and LPS binding protein levels directly correlated with FIB-4 values (adjusted correlation coefficients 0.214, 0.452, 0.317, 0.204, and 0.171, respectively). However, LPS levels were inversely associated with FIB-4 (−0.283). All plasma marker levels in the highest quartile, except LPS, were associated with ALF (sCD163, sCD14, IL-6, IL-10, and LPS binding protein: adjusted odds ratio (aOR) 11.49 (95% confidence interval 6.42–20.56), 1.87 (1.11–3.16), 2.99 (1.79–5.01), 1.84 (1.11–3.16), and 2.13 (1.30–3.50), respectively). Conversely, LPS levels in the lowest quartile were associated with ALF (aOR 2.58 (1.48–4.58), p < 0.01). Conclusion: In AUD patients, plasma levels of the markers of inflammation, monocyte activation, and microbial translocation are associated with ALF.
1. Introduction
Alcohol-related liver disease is the most frequent alcohol-related chronic medical problem and alcohol use is a major culprit of the global increase in liver-related deaths [1]. Alcohol use promotes microbial translocation due to changes in the microbiome and increased intestinal permeability, leading to systemic inflammation, monocyte activation, and progression of liver disease [2]. However, only a few of those who drink heavily eventually develop end-stage liver disease [3]. The early diagnosis of subjacent liver disease in otherwise healthy patients with AUD is intriguing [4] and there is an interest in obtaining markers to better stratify the risk of progressive liver injury among patients with unhealthy alcohol use [5].
All of the aforementioned pathological features (intestinal permeability, microbial translocation, systemic inflammation, and monocyte activation) have been thoroughly studied in patients with overt end-stage liver disease or severe alcoholic hepatitis [6,7,8,9], but they have been far less frequently assessed in patients with AUD without end-stage liver disease admitted for hospital treatment of the disorder [10,11].
Systemic inflammation can be measured via the plasma levels of interleukin (IL)-6 and IL-10. In addition, sCD14 and sCD163 are markers of monocyte activation [2], with sCD14 levels representing monocyte activation dependent on lipopolysaccharide (LPS). The binding of LPS to LPS binding protein (LBP) is a facilitator of the union of that complex to sCD14 and further activation of toll-like receptor 4 [2]. Increased levels of sCD163 are consistent with monocyte activation derived not only from the presence of LPS in peripheral blood but also from the presence of other damage-associated molecular patterns (DAMPs) that are produced by alcohol metabolism and increased iron deposition [11]. DAMPs trigger sterile inflammation and the activation of monocyte toll-like receptors, which subsequently activate quiescent stellate cells, leading to progressive liver fibrosis [12]. LPS and LBP levels are markers of microbial translocation that have been thoroughly studied in patients with cirrhosis of the liver [13] and in those with HIV infection with or without HCV co-infection [14,15]. However, they have been less frequently measured in patients admitted for the treatment of AUD [9,16].
Liver fibrosis is the main predictor of the progression to cirrhosis of the liver in patients with unhealthy alcohol use [17]. Despite liver biopsy being considered the gold standard for the evaluation of liver fibrosis, it is an invasive and costly procedure [18] and its performance is unlikely in patients with active alcohol or other drug use [19]. FIB-4 is a non-invasive index for estimating liver fibrosis that includes laboratory parameters that are usually monitored in everyday clinical practice [20]. It is a useful index for estimating liver fibrosis in patients with an alcohol or substance use disorder who rarely undergo a liver biopsy [19]. In addition to estimating the presence of liver fibrosis, FIB-4 also accurately predicts mortality and other poor health outcomes in other subsets of patients, such as incident heart failure [21].
The association between markers of inflammation and non-invasive measures of liver fibrosis has been previously studied [22], and markers of inflammation (e.g., IL-6) can predict the presence of advanced liver fibrosis (ALF) in HIV-infected patients [23]. However, whether markers of monocyte activation, intestinal permeability, and microbial translocation are associated with FIB-4 values consistent with ALF in patients with an AUD and no apparent end-stage liver disease remains to be elucidated.
We hypothesized that plasma levels of markers of monocyte activation (sCD163 and sCD14), inflammation (IL-6 and Il-10, and microbial translocation (lipopolysaccharide (LPS) and LPS binding protein (LBP)) are associated with FIB-4 levels in patients with AUD without overt end-stage liver disease admitted to hospital for the treatment of the disorder.
2. Materials and Methods
2.1. Participants
We included patients admitted for hospital alcohol detoxification at two tertiary teaching hospitals in Barcelona, Spain (Hospital Universitari Germans Trias i Pujol and Hospital Universitari de Bellvitge) between 2013 and 2019.
Patients were referred for hospital detoxification if they were deemed ineligible for ambulatory detoxification by addiction physicians. The main reasons for referring patients included a high risk of severe alcohol withdrawal, the presence of severe medical co-morbidities, and poor adherence to outpatient treatment and/or unsuccessful outpatient detoxification. Patients were excluded from the present study if they harbored autoimmune diseases, acute and decompensated medical co-morbidities, or severe mental health problems.
This study was approved by the Ethics Committee of both participant hospitals. Written consent was provided by all patients before study entry and participation. This study was conducted with compliance with ethical standards as well as the principles of good clinical practice defined by the World Medical Association’s Declaration of Helsinki [24].
2.2. Measurements
On the day of admission, all participants underwent a thorough physical examination and an interview regarding their history of alcohol consumption as well as their use of tobacco and other drugs. On the following day, blood was drawn to assess hematological and biochemical parameters and HCV infection. Additional information regarding the admission protocol and the methods for the detection of HCV infection as well as the measure of sCD163, sCD14, and IL-6 has been previously published [11,19,25].
Of note, the upper limit of detection for sCD163 was 1000 ng/mL and, for all assays above that threshold, a value of 1000 ng/m was set for the statistical analysis. IL-10 was determined by the same method as IL-6 [11] and the lower limit of detection was 0.02 pg/mL. For assays with an IL-10 concentration below the detection threshold, a value of 0.02 pg/mL was set for the analysis.
Plasma concentrations of LPS and LBP were determined by enzyme-linked immunosorbent assays. Each sample was diluted 10×. Plasma concentrations of LPS and LBP were measured in duplicate using the LPS ELISA kit (abx517692, Cambridge, UK) and the LBP ELISA kit (abx575210, Abbexa, Cambridge, UK), respectively. All assays were performed according to the manufacturer’s instructions. The inter-assay and intra-assay coefficients of variation were <10% for all analyses.
Liver fibrosis was assessed by the FIB-4 index [20]: age × AST (U/L)/platelet count (109/L) × ALT (U/L)1/2. ALF was defined as FIB-4 > 3.25.
2.3. Statistical Analysis
Descriptive statistics were expressed as the median and interquartile range (IQR) for quantitative variables, or as absolute frequencies and percentages for qualitative variables. We performed the chi-squared test to explore significant differences in qualitative variables and the t-test for the mean differences in quantitative variables between participants that had ALF measured with FIB-4 and those who did not.
We performed an unadjusted correlation analysis between plasma marker levels and FIB-4 values as a continuous variable. In addition, we performed an adjusted correlation analysis where all correlations were adjusted for sex, alcohol intake, and the presence of HCV infection. We also performed logistic regression analyses to detect the association between plasma marker levels in the highest quartile and the presence of ALF measured with FIB-4. Finally, we performed a logistic regression analysis to detect the association between LPS levels in the lowest quartile and the presence of ALF. All logistic regression analyses were adjusted for sex, alcohol intake, and the presence HCV infection. The test results were considered significant if the resulting one-tailed p-value was < 0.05. Statistical analyses were performed using SPSS software version 15.0.1 (SPSS, Chicago, IL, USA).
3. Results
A total of 353 participants were included in the present study. Table 1 includes the baseline clinical characteristics and the median values for several laboratory parameters as well as for markers of monocyte activation (sCD163, sCD14), inflammation (IL-6 and IL-10), and microbial translocation (LPS and LBP).

Table 1.
Characteristics of the patients with alcohol use disorder admitted for hospital treatment.
Participants with ALF had a higher alcohol intake at admission (186 vs. 161 g/day, p < 0.05), a higher duration of AUD (22.8 vs. 17.5 years, p < 0.01), and a higher prevalence of HCV infection (23.6 vs. 9.3%, p < 0.01). As seen in Table 2, patients with ALF had higher mean sCD163 (944 vs. 638 ng/mL, p < 0.01), sCD14 (1.9 × 106 vs. 1.7 × 106 pg/mL, p < 0.01), LBP (55 vs. 35.4 pg/mL, p = 0.04), IL-6 (16.9 vs. 5.9 pg/mL, p = 0.04), and IL-10 (2.5 vs. 1.4 pg/mL, p < 0.01) levels and lower mean LPS values (1272 vs. 1975 pg/mL, p = 0.02).
Table 2.
Mean plasma marker values stratified by the presence of advanced liver fibrosis.
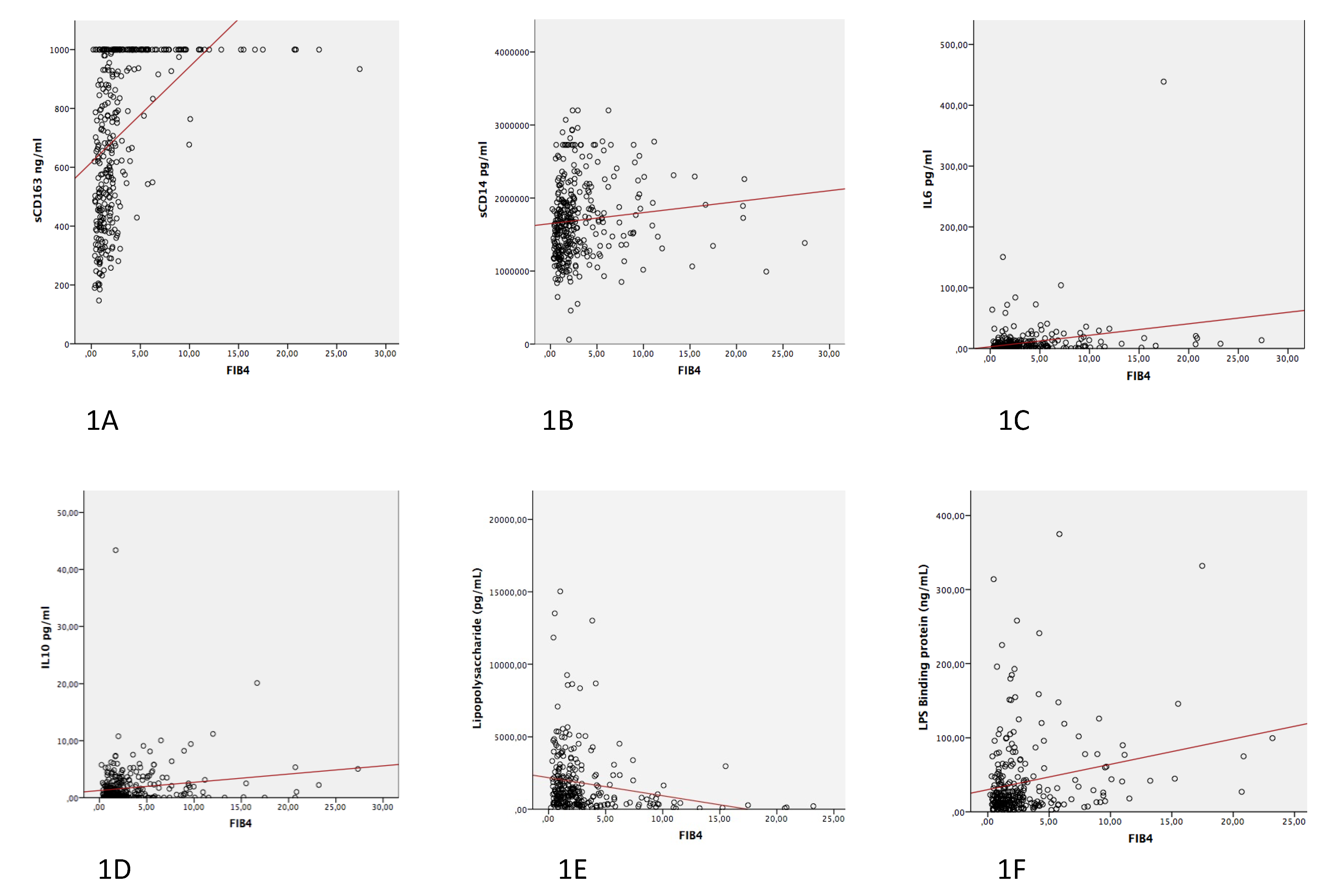
In addition, we performed correlation analyses between the different marker levels and FIB-4 levels as a continuous variable. The unadjusted correlation plots are seen in Figure 1.
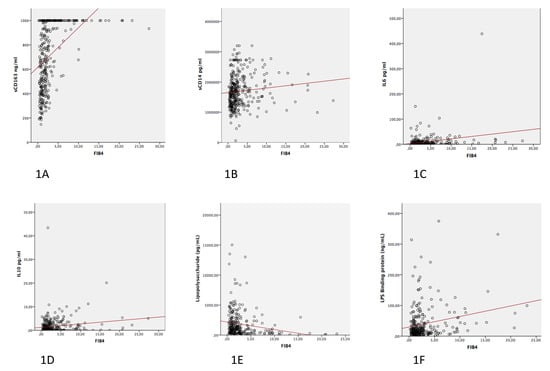
Figure 1.
Unadjusted correlation plots between the different markers and FIB-4 levels: (1A) sCD163; (1B) sCD14; (1C) IL-6; (1D) IL-10; (1E) LPS; and (1F) LBP.
Table 3 includes the results of the correlation analyses adjusted by sex, alcohol intake before admission, and the presence of HCV infection. As seen in Table 3, the levels of sCD163, sCD14, IL-6, IL-10, and LBP directly correlated with FIB-4 values (adjusted correlation coefficients 0.214, 0.452, 0.317, 0.204, and 0.171, respectively) whereas LPS levels were inversely associated with FIB-4 values (adjusted correlation coefficient −0.283).
Table 3.
Adjusted correlations between plasma marker levels and FIB-4 values.
Finally, we performed adjusted logistic regression analyses to assess the association between plasma marker levels in the highest quartile and the presence of ALF. All analyses were adjusted by sex, alcohol consumption, and the presence of HCV infection. As seen in Table 4, plasma levels of all markers, except LPS, in the highest quartile were significantly associated with the presence of ALF with an adjusted odds ratio ranging from 1.84 for IL-10 to 11.49 for sCD163. Conversely, LPS levels in the lowest quartile were significantly associated with the presence of ALF (adjusted odds ratio 2.58 (95% confidence interval: 1.48–4.58), p < 0.01).
Table 4.
Logistic regression for the association between marker levels in the highest quartile and advanced liver fibrosis.
4. Discussion
In this series of AUD patients with no decompensated liver disease admitted for hospital treatment of the disorder, plasma marker levels consistent with increased monocyte activation and increased systemic inflammation were associated with the presence of ALF, as were higher LBP levels.
In particular, levels of IL-6, IL-10, sCD14, sCD163, and LBP in the highest quartile and levels of LPS in the lowest quartile were associated with ALF measured with FIB-4. The same associations were found when marker levels were correlated with FIB-4 as a continuous variable; IL-10, sCD14, sCD163, and LBP levels directly correlated with FIB-4 values whereas the LPS levels negatively correlated with FIB-4. All analyses that detected these associations were adjusted by sex, amount of alcohol consumption before admission, and the presence of HCV infection. Notably, in this study population, patients with ALF had a greater alcohol consumption before admission and a higher prevalence of HCV infection.
As mentioned previously, LPS levels negatively correlated with FIB-4 values and LPS levels in the lowest quartile were associated with higher odds of ALF. These findings suggest that higher levels of LPS may be indicative of microbial translocation occurring in an earlier phase of the pathogenesis of alcohol-related liver disease when patients have not yet developed significant liver fibrosis. Monocyte activation, inflammation, and higher levels of LBP would be more prominent pathological features in later stages of the disease, which is why all those markers were associated with higher FIB-4 values and with higher odds of FIB-4 values suggestive of the presence of ALF.
The association between IL-6 levels and ALF has been previously described in a cohort of HIV-infected patients with unhealthy alcohol use [23] and in other cohorts of HIV-infected patients [26]. However, prior studies failed to detect an association between IL-10 levels and non-invasive markers of liver fibrosis [23]. The association between inflammatory markers and liver fibrosis is of interest as both higher IL-6 levels and FIB-4 values consistent with ALF have been associated with higher mortality and other health outcomes in different settings [27,28,29].
Other authors have shown that markers of monocyte activation, especially sCD14, have also been associated with mortality and other health complications [30,31]. In a study performed on HIV-infected patients, Sandler and colleagues showed that sCD14 levels correlated with AST and ferritin levels, which the authors found to be suggestive of liver inflammation [32]. In that same study, sCD4 levels correlated with gamma-glutamyl transpeptidase, alkaline phosphatase, and alpha-fetoprotein, which the authors found to be suggestive of liver fibrosis [32]. In a prior study by our group, sCD14 levels in the higher quartile were associated with AST levels whereas sCD163 values in the highest quartile were associated with AST and bilirubin levels and the presence of HCV infection, which suggests the presence of underlying a liver injury [11]. We are not aware of another study that has studied the association of plasma markers of monocyte activation and intestinal permeability and ALF in patients with AUD.
LPS levels have been studied in patients with AUD and seem to decrease with alcohol abstinence [9,33]. LBP levels are associated with mortality in patients with decompensated cirrhosis [34] and appear to decrease with the use of beta-blockers in patients with portal hypertension [13] but the levels in patients with AUD without overt liver disease have not received much attention in the literature. Our findings support the use of LBP as a surrogate marker of microbial translocation in patients with AUD. In addition, no other studies have evaluated the association between LPS and LBP levels and ALF.
Importantly, our findings underscore that monocyte activation, systemic inflammation, and microbial translocation are present in patients with AUD but without end-stage liver disease and admitted for hospital treatment, and that these levels are associated with FIB-4 values and the presence of ALF assessed with non-invasive measures. Patients with FIB-4 values suggestive of ALF should be prioritized to receive more intensive forms of follow-up treatment to secure alcohol abstinence. Abstinence from alcohol is associated with increased survival even in patients who already present with advanced forms of alcohol-related liver disease [3].
This study has a few limitations to be noted. First, plasma markers were assessed on the second day of hospital admission and their levels may be modified by alcohol abstinence. A sequential measurement of these markers during hospital alcohol detoxification is a potential future line of inquiry. Second, we included patients with the most severe forms of AUD (i.e., a 20-year history of the disorder and a median daily alcohol intake upon admission of 140 g/day) and our findings may not be extrapolated to patients with milder forms of unhealthy alcohol use as seen in primary care or hepatology clinics. Third, we estimated liver fibrosis with FIB-4, which has not been validated against the gold standard of liver biopsy for alcohol-related liver disease [35]. Despite that few authors have expressed concerns about the accuracy of FIB-4 [36], the European Association for the Study of the Liver has recently published an updated version of their guideline for the non-invasive diagnosis of a liver injury and recommends the use of FIB-4 as a first-line method for detecting patients with high probability of presenting significant liver disease [37]. The present study adds to the literature that categorizes FIB-4 as a reliable tool for estimating liver fibrosis in patients in whom the performance of a liver biopsy is unlikely [38]. In addition, FIB-4 includes variables that are routinely assessed in the everyday care of subjects with liver disease and is an ideal method of estimating liver fibrosis in resource-limited settings where the use of transient elastography is prohibitive. In addition to being a reliable predictor of mortality [29], FIB-4 values are associated with important disease correlates in this case series of patients with an AUD admitted for hospital treatment for the disorder.
In summary, the present study shows that higher levels of markers of inflammation, monocyte activation, and LBP and lower levels of LPS are associated with FIB-4 values as well as with ALF in patients admitted for the treatment of AUD.
Author Contributions
Conceptualization, D.F., X.G.-C. and R.M.; methodology, D.F., X.G.-C., O.F. and A.L.; formal analysis, D.F., X.G.-C. and O.F.; investigation, D.F., X.G.-C., P.Z., F.B., A.H.-R., I.R. and R.M.; data curation, D.F., X.G.-C. and O.F.; writing—original draft preparation, D.F.; writing—review and editing, D.F., X.G.-C., O.F. and R.M.; funding acquisition, D.F. and R.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was partially funded by the Ministry of Economy and Competitiveness, Institute of Health Carlos III (RETICS RD16/0017/0003, Programa Juan Rodes JR20/00016, Programa Sara Borrell CD19/00019, grant nos. PI17/00174 and PI20/00883, and Physician Intensification Program INT19/00026), European Fund for Regional Development (FEDER), Ministry of Health, Social Services and Equality, National Plan on Drugs, Spain (grant nos. 2018/020 and 2020/024), and Consolidated Research Group (2017-SGR-316), Autonomous Government of Catalonia, Spain.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Hospital Universitari Germans Trias i Pujol and Hospital Universitari de Bellvitge (protocol code PNSD2015-027, 15 March 2013).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data presented in this study are available to any scientist wishing to use them for non-commercial purposes on request from the corresponding author without breaching participant confidentiality. The data are not publicly available due to privacy.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rehm, J.; Samokhvalov, A.V.; Shield, K. Global burden of alcoholic liver diseases. J. Hepatol. 2013, 59, 160–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louvet, A.; Mathurin, P. Alcoholic liver disease: Mechanisms of injury and targeted treatment. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 231–242. [Google Scholar] [CrossRef]
- Fuster, D.; Samet, J.H. Alcohol Use in Patients with Chronic Liver Disease. N. Engl. J. Med. 2018, 379, 1251–1261. [Google Scholar] [CrossRef]
- Moreno, C.; Mueller, S.; Szabo, G. Non-invasive diagnosis and biomarkers in alcohol-related liver disease. J. Hepatol. 2019, 70, 273–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altamirano, J.; Qi, Q.; Choudhry, S. Non-invasive diagnosis: Non-alcoholic fatty liver disease and alcoholic liver disease. Transl. Gastroenterol. Hepatol. 2020, 5, 31. [Google Scholar] [CrossRef] [PubMed]
- Michelena, J.; Altamirano, J.; Abraldes, J.G. Systemic inflammatory response and serum lipopolysaccharide levels predict multiple organ failure and death in alcoholic hepatitis. Hepatology 2015, 62, 762–772. [Google Scholar] [CrossRef]
- Szabo, G. Gut–Liver Axis in Alcoholic Liver Disease. Gastroenterology 2015, 148, 30–36. [Google Scholar] [CrossRef] [Green Version]
- Saha, B.; Tornai, D.; Kodys, K. Biomarkers of Macrophage Activation and Immune Danger Signals Predict Clinical Outcomes in Alcoholic Hepatitis. Hepatology 2019, 70, 1134–1149. [Google Scholar] [CrossRef]
- Donnadieu-Rigole, H.; Pansu, N.; Mura, T. Beneficial Effect of Alcohol Withdrawal on Gut Permeability and Microbial Translocation in Patients with Alcohol Use Disorder. Alcohol. Clin. Exp. Res. 2018, 42, 32–40. [Google Scholar] [CrossRef]
- Donnadieu-Rigole, H.; Mura, T.; Portales, F. Effects of alcohol withdrawal on monocyte subset defects in chronic alcohol users. J. Leukoc. Biol. 2016, 100, 1191–1199. [Google Scholar] [CrossRef] [Green Version]
- García-Calvo, X.; Bolao, F.; Sanvisens, A. Significance of Markers of Monocyte Activation (CD163 and sCD14) and Inflammation (IL-6) in Patients Admitted for Alcohol Use Disorder Treatment. Alcohol. Clin. Exp. Res. 2019, 44, 152–158. [Google Scholar] [CrossRef]
- Lackner, C.; Tiniakos, D. Fibrosis and alcohol-related liver disease. J. Hepatol. 2019, 70, 294–304. [Google Scholar] [CrossRef] [PubMed]
- Reiberger, T.; Ferlitsch, A.; Payer, B.A. Non-selective betablocker therapy decreases intestinal permeability and serum levels of LBP and IL-6 in patients with cirrhosis. J. Hepatol. 2013, 58, 911–921. [Google Scholar] [CrossRef] [PubMed]
- Monnig, M.A.; Cohen, R.; Ramratnam, B.; McAdams, M.; Tashima, K.; Monti, P.M. HIVInfection, HCVCoinfection, and Alcohol Use: Associations with Microbial Translocation and Immune Activation. Alcohol. Clin. Exp. Res. 2019, 43, 1126–1134. [Google Scholar] [CrossRef]
- French, A.L.; Evans, C.T.; Agniel, D.M. Microbial Translocation and Liver Disease Progression in Women Coinfected With HIV and Hepatitis C Virus. J. Infect. Dis. 2013, 208, 679–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leclercq, S.; Matamoros, S.; Cani, P.D. Intestinal permeability, gut-bacterial dysbiosis, and behavioral markers of alcohol-dependence severity. Proc. Natl. Acad. Sci. USA 2014, 111, E4485–E4493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bataller, R.; Brenner, D. Liver fibrosis. J. Clin. Investig. 2005, 115, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Gebo, K.A.; Herlong, H.F.; Torbenson, M.S. Role of liver biopsy in management of chronic hepatitis C: A systematic review. Hepatology 2002, 36, s161–s172. [Google Scholar] [CrossRef] [Green Version]
- Sanvisens, A.; Muñoz, A.; Bolao, F. Do serum markers of liver fibrosis vary by HCV infection in patients with alcohol use disorder? Drug Alcohol Depend. 2018, 188, 180–186. [Google Scholar] [CrossRef]
- Sterling, R.K.; Lissen, E.; Clumeck, N. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- So-Armah, K.A.; Lim, J.K.; Re, V.L. FIB-4 stage of liver fibrosis predicts incident heart failure among HIV-infected and uninfected patients. Hepatology 2017, 66, 1286–1295. [Google Scholar] [CrossRef] [Green Version]
- Armah, K.A.; Quinn, E.K.; Cheng, D.M. Human immunodeficiency virus, hepatitis C, and inflammatory biomarkers in individuals with alcohol problems: A cross-sectional study. BMC Infect. Dis. 2013, 13, 399. [Google Scholar] [CrossRef] [Green Version]
- Fuster, D.; Tsui, J.; Cheng, D. Interleukin-6 Is Associated with Noninvasive Markers of Liver Fibrosis in HIV-Infected Patients with Alcohol Problems. AIDS Res. Hum. Retrovir. 2013, 29, 1110–1116. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association General Assembly World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects Revised October 7, 2000. HIV Clin. Trials 2001, 2, 92–95. [CrossRef] [PubMed]
- Rivas, I.; Sanvisens, A.; Bolao, F. Impact of Medical Comorbidity and Risk of Death in 680 Patients with Alcohol Use Disorders. Alcohol. Clin. Exp. Res. 2013, 37, E221–E227. [Google Scholar] [CrossRef]
- Shah, S.; Ma, Y.; Scherzer, R. Association of HIV, hepatitis C virus and liver fibrosis severity with interleukin-6 and C-reactive protein levels. AIDS 2015, 29, 1325–1333. [Google Scholar] [CrossRef] [PubMed]
- Kuller, L.H.; Tracy, R.; Belloso, W. Inflammatory and Coagulation Biomarkers and Mortality in Patients with HIV Infection. PLoS Med. 2008, 5, e203. [Google Scholar] [CrossRef] [PubMed]
- So-Armah, K.A.; Tate, J.P.; Chang, C.-C.H. Do Biomarkers of Inflammation, Monocyte Activation, and Altered Coagulation Explain Excess Mortality Between HIV Infected and Uninfected People? JAIDS J. Acquir. Immune Defic. Syndr. 2016, 72, 206–213. [Google Scholar] [CrossRef] [Green Version]
- Nunes, D.; Fleming, C.; Offner, G. Noninvasive Markers of Liver Fibrosis Are Highly Predictive of Liver-Related Death in a Cohort of HCV-Infected Individuals With and Without HIV Infection. Am. J. Gastroenterol. 2010, 105, 1346–1353. [Google Scholar] [CrossRef]
- Lien, E.; Aukrust, P.; Sundan, A.; Müller, F.; Frøland, S.S.; Espevik, T. Elevated levels of serum-soluble CD14 in human immuno-deficiency virus type 1 (HIV-1) infection: Correlation to disease progression and clinical events. Blood 1998, 92, 2084–2092. [Google Scholar] [CrossRef]
- Sandler, N.G.; Wand, H.; Roque, A. Plasma Levels of Soluble CD14 Independently Predict Mortality in HIV Infection. J. Infect. Dis. 2011, 203, 780–790. [Google Scholar] [CrossRef] [Green Version]
- Sandler, N.G.; Koh, C.; Roque, A. Host Response to Translocated Microbial Products Predicts Outcomes of Patients With HBV or HCV Infection. Gastroenterology 2011, 141, 1220–1230. [Google Scholar] [CrossRef] [Green Version]
- Leclercq, S.; Cani, P.D.; Neyrinck, A. Role of intestinal permeability and inflammation in the biological and behavioral control of alcohol-dependent subjects. Brain Behav. Immun. 2012, 26, 911–918. [Google Scholar] [CrossRef] [PubMed]
- Agiasotelli, D.; Alexopoulou, A.; Vasilieva, L.; Hadziyannis, E.; Goukos, D.; Daikos, G.L.; Dourakis, S.P. High serum lipopolysaccharide binding protein is associated with increased mortality in patients with decompensated cirrhosis. Liver Int. 2016, 37, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Fuster, D.; Tsui, J.I.; Cheng, D.M. Impact of Lifetime Alcohol Use on Liver Fibrosis in a Population of HIV-Infected Patients With and Without Hepatitis C Coinfection. Alcohol. Clin. Exp. Res. 2013, 37, 1527–1535. [Google Scholar] [CrossRef]
- Hashem, A.; Awad, A.; Shousha, H. Validation of a machine learning approach using FIB-4 and APRI scores assessed by the metavir scoring system: A cohort study. Arab. J. Gastroenterol. 2021, 22, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Berzigotti, A.; Tsochatzis, E.; Boursier, J.; Castera, L.; Cazzagon, N.; Friedrich-Rust, M.; Petta, S.; Thiele, M. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis–2021 update. J. Hepatol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Blackard, J.T.; Welge, J.A.; Taylor, L.E. HIV Mono-infection Is Associated With FIB-4-A Noninvasive Index of Liver Fibrosis-in Women. Clin. Infect. Dis. 2011, 52, 674–680. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).