
Predictors of Hypoxemia and Related Adverse Outcomes in Patients Hospitalized with COVID-19: A Double-Center Retrospective Study


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Clinical and Laboratory Data and Outcome Assessment
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
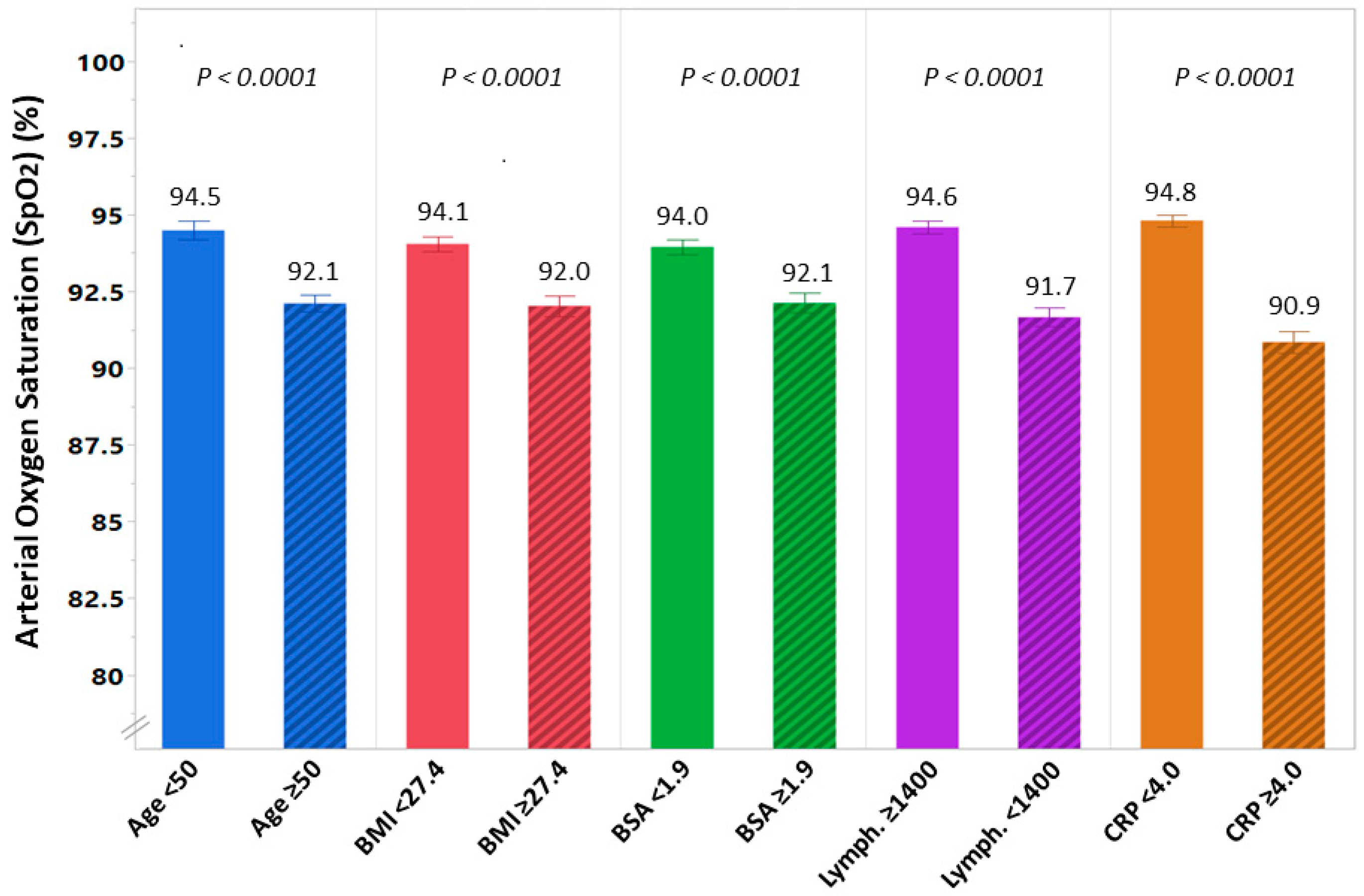
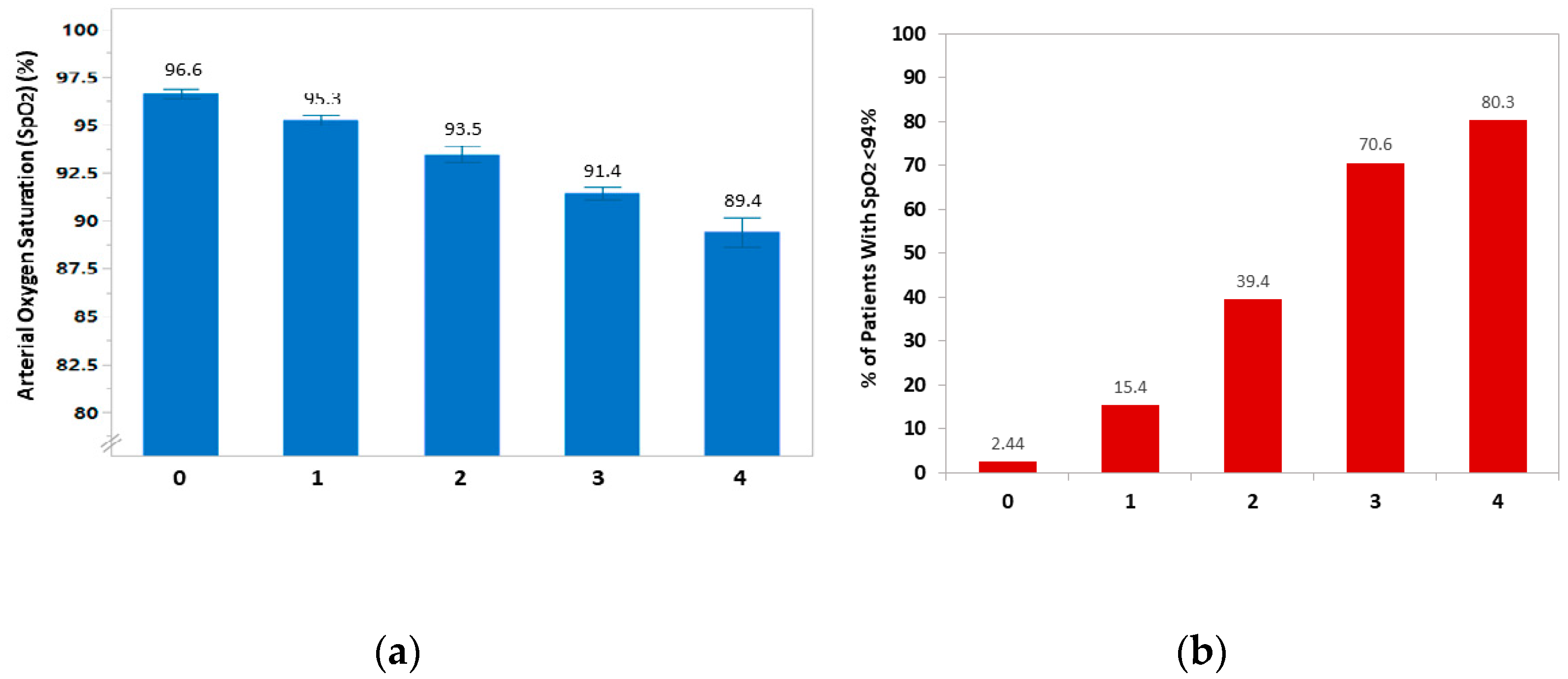
3.2. Predictors of Low Oxygen Saturation
3.3. Receiver Operating Characteristic (ROC) Curves for the Diagnosis of low SpO2
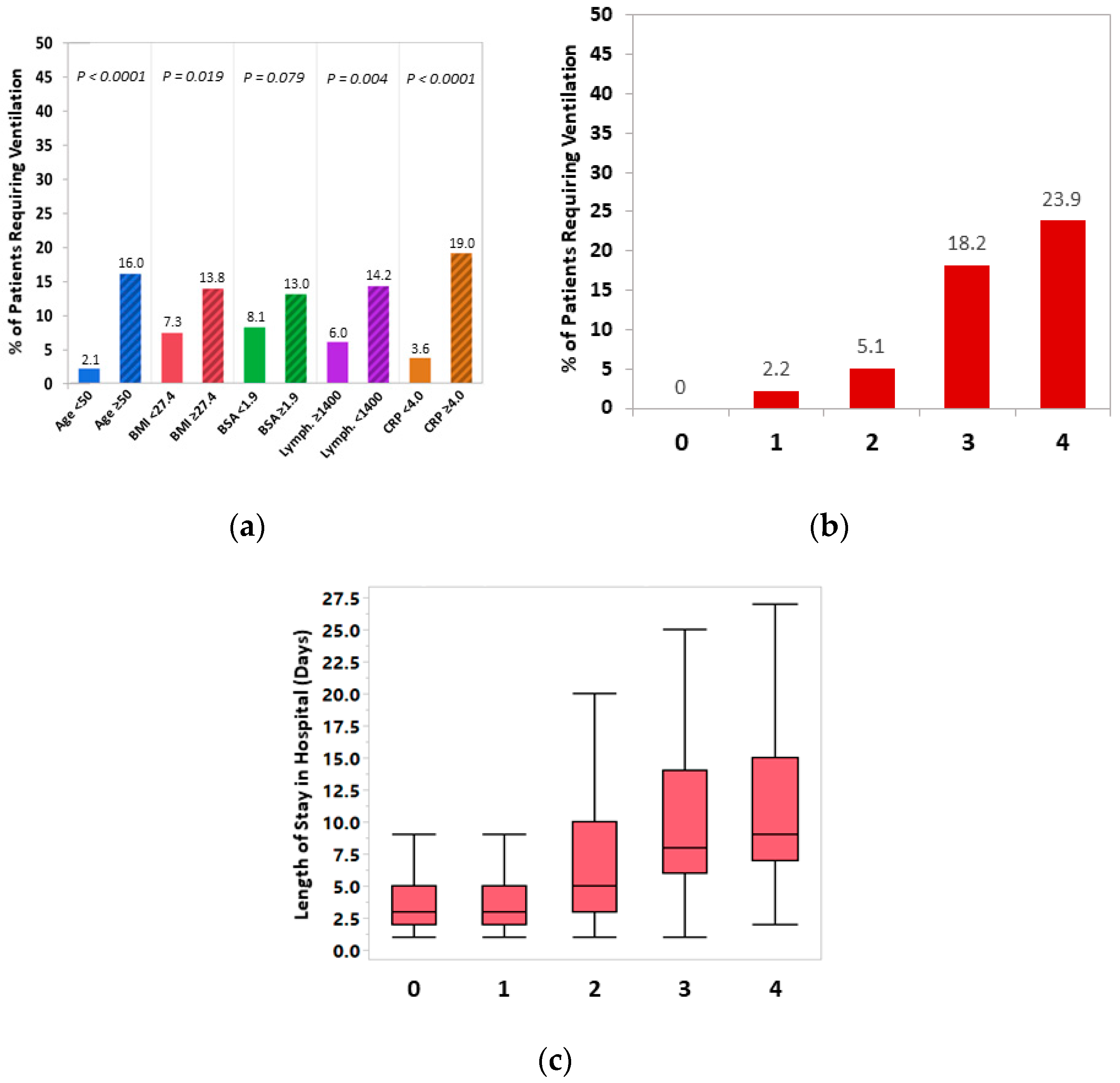
3.4. Respiratory-Related Adverse Outcomes
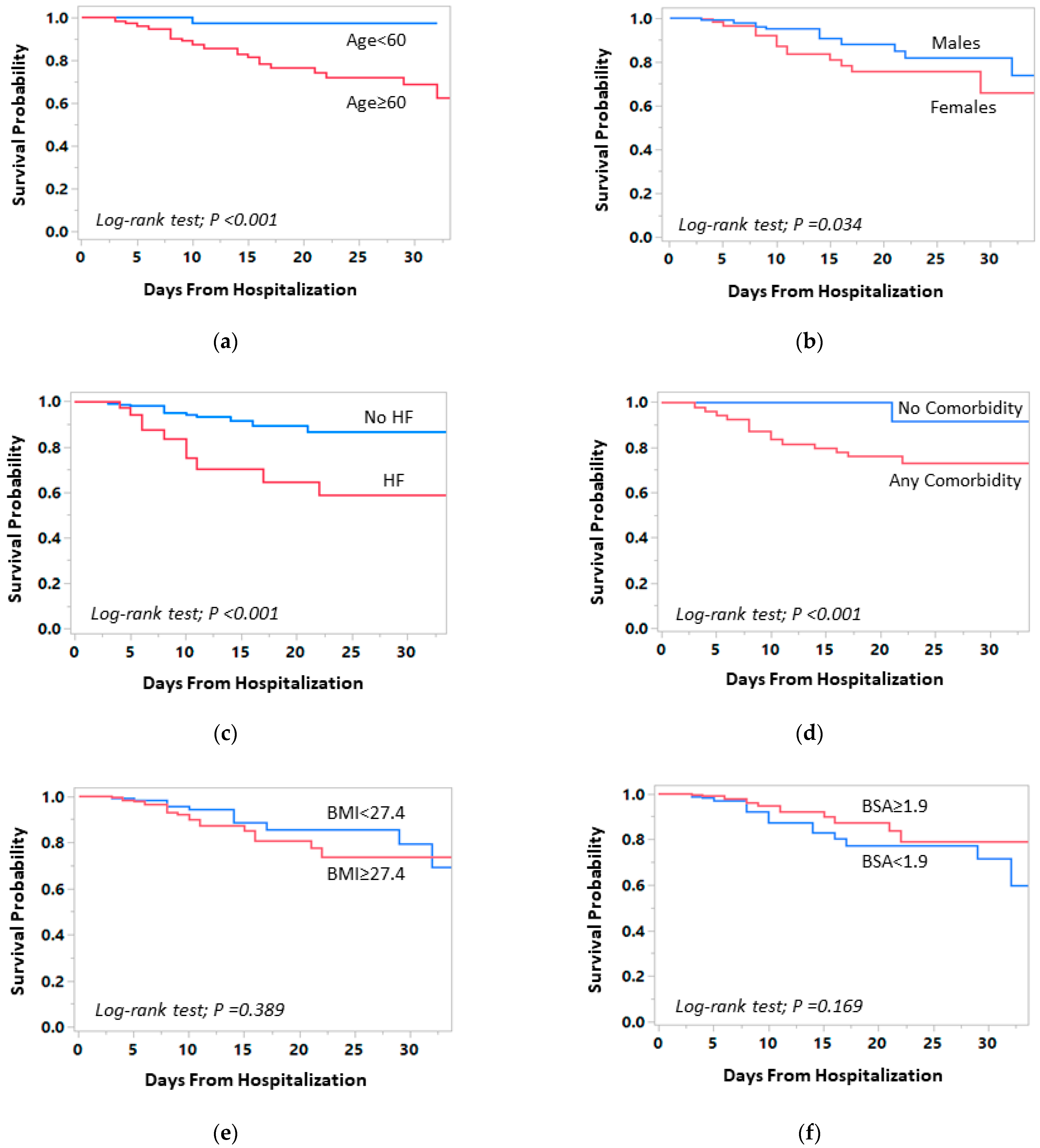
3.5. Associations of Clinical Characteristics and Comorbidities with In-Hospital Mortality
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Yu, C.; Lei, Q.; Li, W.; Wang, X.; Liu, W.; Fan, X.; Li, W. Clinical Characteristics, Associated Factors, and Predicting COVID-19 Mortality Risk: A Retrospective Study in Wuhan, China. Am. J. Prev. Med. 2020, 59, 168–175. [Google Scholar] [CrossRef]
- Dhont, S.; Derom, E.; Van Braeckel, E.; Depuydt, P.; Lambrecht, B.N. The pathophysiology of ‘happy’ hypoxemia in COVID-19. Respir. Res. 2020, 21, 198. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of COVID-19 Interim Guidance; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China. JAMA 2020, 323, 1239. [Google Scholar] [CrossRef]
- Aylward, B.; Liang, W. (PRC) Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19); World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Kashani, K.B. Hypoxia in COVID-19: Sign of Severity or Cause for Poor Outcomes. Mayo Clin. Proc. 2020, 95, 1094–1096. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Chiumello, D.; Caironi, P.; Busana, M.; Romitti, F.; Brazzi, L.; Camporota, L. COVID-19 pneumonia: Different respiratory treatments for different phenotypes? Intensive Care Med. 2020, 46, 1099–1102. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.; Calderón-Villarreal, A.; Bojorquez, I.; Vera Hernández, C.; Schriger, D.L.; Tovar Hirashima, E. Excess Out-of-Hospital Mortality and Declining Oxygen Saturation: The Sentinel Role of Emergency Medical Services Data in the COVID-19 Crisis in Tijuana, Mexico. Ann. Emerg. Med. 2020, 76, 413–426. [Google Scholar] [CrossRef] [PubMed]
- Mosteller, R.D. Simplified calculation of body-surface area. N. Engl. J. Med. 1987, 317, 1098. [Google Scholar] [PubMed]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Moore, J.B.; June, C.H. Cytokine release syndrome in severe COVID-19. Science 2020, 368, 473–474. [Google Scholar] [CrossRef] [Green Version]
- Somers, V.K.; Kara, T.; Xie, J. Progressive Hypoxia: A pivotal pathophysiologic mechanism of COVID-19 pneumonia. Mayo Clin. Proc. 2020, 95, 2339–2342. [Google Scholar]
- Eltzschig, H.K.; Carmeliet, P. Hypoxia and Inflammation. N. Engl. J. Med. 2011, 364, 656–665. [Google Scholar] [CrossRef] [Green Version]
- López-Rodríguez, D.M.; Kirillov, V.; Krug, L.T.; Mesri, E.A.; Andreansky, S. A role of hypoxia-inducible factor 1 alpha in Murine Gammaherpesvirus 68 (MHV68) lytic replication and reactivation from latency. PLoS Pathog. 2019, 15, e1008192. [Google Scholar] [CrossRef]
- Vassilaki, N.; Kalliampakou, K.I.; Kotta-Loizou, I.; Befani, C.; Liakos, P.; Simos, G.; Mentis, A.F.; Kalliaropoulos, A.; Doumba, P.P.; Smirlis, D.; et al. Low Oxygen Tension Enhances Hepatitis C Virus Replication. J. Virol. 2013, 87, 2935–2948. [Google Scholar] [CrossRef] [Green Version]
- Sommer, N.; Dietrich, A.; Schermuly, R.T.; Ghofrani, H.A.; Gudermann, T.; Schulz, R.; Seeger, W.; Grimminger, F.; Weissmann, N. Regulation of hypoxic pulmonary vasoconstriction: Basic mechanisms. Eur. Respir. J. 2008, 32, 1639–1651. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with Covid-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef]
- Pilli, V.S.; Datta, A.; Afreen, S.; Catalano, D.; Szabo, G.; Majumder, R. Hypoxia downregulates protein S expression. Blood 2018, 132, 452–455. [Google Scholar] [CrossRef] [Green Version]
- Okauchi, Y.; Matsuno, K.; Nishida, T.; Sawada, K.; Kawasaki, A.; Ito, N.; Morimura, O.; Otani, Y.; Yokoe, M.; Abe, K.; et al. Obesity, glucose intolerance, advanced age, and lymphocytopenia are independent risk factors for oxygen requirement in Japanese patients with Coronavirus disease 2019 (COVID-19). Endocr. J. 2021, 68, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Pacheco, M.; Silva, P.L.; Cruz, F.F.; Battaglini, D.; Robba, C.; Pelosi, P.; Morales, M.M.; Caruso Neves, C.; Rocco, P.R.M. Pathogenesis of Multiple Organ Injury in COVID-19 and Potential Therapeutic Strategies. Front. Physiol. 2021, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Wu, Z.; Li, J.-W.; Zhao, H.; Wang, G.-Q. Cytokine release syndrome in severe COVID-19: Interleukin-6 receptor antagonist tocilizumab may be the key to reduce mortality. Int. J. Antimicrob. Agents 2020, 55, 105954. [Google Scholar] [CrossRef] [PubMed]
- The RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Cai, Q.; Chen, F.; Wang, T.; Luo, F.; Liu, X.; Wu, Q.; He, Q.; Wang, Z.; Liu, Y.; Liu, L.; et al. Obesity and COVID-19 Severity in a Designated Hospital in Shenzhen, China. Diabetes Care 2020, 43, 1392–1398. [Google Scholar] [CrossRef]
- Yang, J.; Hu, J.; Zhu, C. Obesity aggravates COVID-19: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 257–261. [Google Scholar] [CrossRef]
- Hendren, N.S.; de Lemos, J.A.; Ayers, C.; Das, S.R.; Rao, A.; Carter, S.; Rosenblatt, A.; Walchok, J.; Omar, W.; Khera, R.; et al. Association of Body Mass Index and Age With Morbidity and Mortality in Patients Hospitalized With COVID-19. Circulation 2021, 143, 135–144. [Google Scholar] [CrossRef]
- Tartof, S.Y.; Qian, L.; Hong, V.; Wei, R.; Nadjafi, R.F.; Fischer, H.; Li, Z.; Shaw, S.F.; Caparosa, S.L.; Nau, C.L.; et al. Obesity and Mortality Among Patients Diagnosed With COVID-19: Results from an Integrated Health Care Organization. Ann. Intern. Med. 2020, 173, 773–781. [Google Scholar] [CrossRef]
- Kalligeros, M.; Shehadeh, F.; Mylona, E.K.; Benitez, G.; Beckwith, C.G.; Chan, P.A.; Mylonakis, E. Association of Obesity with Disease Severity Among Patients with Coronavirus Disease 2019. Obesity 2020, 28, 1200–1204. [Google Scholar] [CrossRef]
- Hendren, N.S.; Drazner, M.H.; Bozkurt, B.; Cooper, L.T. Description and Proposed Management of the Acute COVID-19 Cardiovascular Syndrome. Circulation 2020, 141, 1903–1914. [Google Scholar] [CrossRef]
- Gong, M.N.; Bajwa, E.K.; Thompson, B.T.; Christiani, D.C. Body mass index is associated with the development of acute respiratory distress syndrome. Thorax 2010, 65, 44–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, J.; Covassin, N.; Fan, Z.; Singh, P.; Gao, W.; Li, G.; Kara, T.; Somers, V.K. Association Between Hypoxemia and Mortality in Patients With COVID-19. Mayo Clin. Proc. 2020, 95, 1138–1147. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.W.; Chau, T.N.; Tsang, O.; Tso, E.; Chiu, M.C.; Tong, W.L.; Lee, P.O.; Ng, T.K.; Ng, W.F.; Lee, K.C.; et al. Outcomes and prognostic factors in 267 patients with severe acute respiratory syndrome in Hong Kong. Ann. Intern. Med. 2003, 139, 715–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, K.-H.; Choi, J.-P.; Hong, S.-H.; Lee, J.; Kwon, J.-S.; Kim, S.-M.; Park, S.Y.; Rhee, J.-Y.; Kim, B.-N.; Choi, H.J.; et al. Predictors of mortality in Middle East respiratory syndrome (MERS). Thorax 2018, 73, 286–289. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Patients | SpO2 ≥ 94% | SpO2 < 94% | p-Value |
|---|---|---|---|---|
| n = 492 | n = 271 | n = 221 | ||
| Demographics | ||||
| Age, years, mean ± SD | 55.9 ± 20.6 | 50.7 ± 21.2 | 62.3 ± 17.8 | <0.001 |
| Gender (male), n (%) | 259 (52.6%) | 124 (45.8%) | 135 (61.1%) | <0.001 |
| Height (m), mean ± SD | 1.68 ± 0.09 | 1.68 ± 0.10 | 1.68 ± 0.08 | 0.919 |
| Weight (kg), mean ± SD | 79.2 ± 18.5 | 76.0 ± 18.6 | 83.1 ± 17.7 | <0.001 |
| BMI (kg/m2), mean ± SD | 28.20 ± 6.10 | 27.13 ± 6.10 | 29.61 ± 5.92 | <0.001 |
| BSA (m2), mean ± SD | 1.91 ± 0.24 | 1.87 ± 0.25 | 1.96 ± 0.23 | <0.001 |
| Current smoking, n (%) | 33 (9.5%) | 17 (9.2%) | 16 (9.9%) | 0.840 |
| Ethnicity: Jews Arabs | 431 (87.6%) 61 (12.4%) | 237 (87.5%) 34 (12.6%) | 194 (87.8%) 27 (12.2%) | 0.912 |
| Comorbidities | ||||
| Hypertension, n (%) | 165 (42%) | 68 (33.0%) | 97 (51.1%) | <0.001 |
| Diabetes mellitus, n (%) | 113 (29%) | 44 (22.2%) | 69 (36.3%) | 0.002 |
| Hyperlipidemia, n (%) | 105 (28%) | 48 (24.0%) | 57 (32.0%) | 0.082 |
| Cognitive decline, n (%) | 68 (18.8%) | 29 (15.2%) | 39 (18.8%) | 0.064 |
| Atherosclerotic CVD, n (%) | 64 (17.8%) | 33 (17.0%) | 31 (18.7%) | 0.681 |
| Lung dysfunction *, n (%) | 43 (12.1%) | 25 (12.4%) | 18 (11.0%) | 0.543 |
| Heart failure, n (%) | 44 (12.3%) | 19 (10.2%) | 25 (14.9%) | 0.178 |
| Atrial fibrillation/flutter, n (%) | 34 (9.7%) | 16 (8.7%) | 18 (10.8%) | 0.498 |
| Malignancy, n (%) | 17 (4.9%) | 9 (5.0%) | 8 (4.9%) | 0.998 |
| VTE, n (%) | 14 (4.1%) | 5 (2.7%) | 9 (5.6%) | 0.181 |
| Immunosuppression, n (%) | 14 (4.1%) | 10 (5.5%) | 4 (2.5%) | 0.166 |
| Autoimmune disease, n (%) | 11 (3.2%) | 7 (3.8%) | 4 (2.5%) | 0.493 |
| Pulmonary hypertension, n (%) | 8 (2.3%) | 5 (2.7%) | 3 (1.9%) | 0.598 |
| Renal replacement therapy, n (%) | 5 (1.0%) | 4 (1.5%) | 1 (0.45%) | 0.256 |
| Medications | ||||
| Statins, n (%) | 93 (25.6%) | 37 (19.7%) | 56 (32.0%) | 0.007 |
| ACE/ARB, n (%) | 82 (22.8%) | 34 (18.1%) | 48 (27.9%) | 0.027 |
| Aspirin, n (%) | 73 (20.1%) | 29 (15.1%) | 44 (25.7%) | 0.012 |
| Antiplatelet therapy (any), n (%) | 95 (19.5%) | 41 (15.4%) | 54 (24.6%) | 0.011 |
| Beta blockers, n (%) | 70 (19.1%) | 32 (16.5%) | 38 (22.1) | 0.174 |
| Insulin, n (%) | 27 (7.7%) | 4 (2.2%) | 23 (13.7%) | <0.001 |
| THRT, n (%) | 48 (13.7%) | 19 (10.3%) | 29 (17.5%) | 0.050 |
| CCB, n (%) | 47 (13.2%) | 21 (11.2%) | 26 (15.5%) | 0.239 |
| Diuretics, n (%) | 47 (13.2%) | 15 (8.1%) | 32 (18.8%) | 0.003 |
| Bronchodilator, n (%) | 23 (6.6%) | 15 (8.2%) | 8 (4.9%) | 0.231 |
| Anticoagulation, n (%) | 11 (3.2%) | 6 (3.3%) | 5 (3.1%) | 0.935 |
| MRA, n (%) | 9 (2.6%) | 4 (2.2%) | 5 (3.1%) | 0.588 |
| Laboratory | ||||
| Leukocytes, 103/µL | 6.4 (5.0–8.3) | 6.4 (5.1–8.4) | 6.6 (4.9–8.0) | 0.642 |
| Neutrophils, 103/µL | 4.4 (3.1–6.1) | 4.0 (2.8–6.2) | 4.7 (3.4–6.1) | 0.036 |
| Lymphocytes, 103/µL | 1.3 (0.9–1.8) | 1.5 (1.1–2.2) | 1.1 (0.8–1.4) | <0.001 |
| Platelets, 103/µL | 193 (156–249) | 195 (163–254) | 189 (152–246) | 0.324 |
| Hemoglobin, g/dL, mean ± SD | 13.5 ± 1.8 | 13.4 ± 1.9 | 13.6 ± 1.8 | 0.161 |
| BUN, mg/dL | 13 (10–20) | 13 (9–17) | 15 (10–23) | <0.001 |
| Creatinine. mg/dL, median (IQR) | 0.80 (0.63–0.98) | 0.76 (0.61–0.95) | 0.84 (0.65–1.11) | 0.003 |
| eGFR, mL/min, median (IQR) | 105.9 (75.0–143.8) | 114.2 (79.8–149.7) | 100.6 (68.8–129.3) | 0.012 |
| Uric acid, mg/dL, mean ± SD | 5.4 ± 2.4 | 5.8 ± 2.2 | 5.0 ± 2.7 | 0.090 |
| Sodium, mmol/L, mean ± SD | 137.0 ± 4.1 | 138.1 ± 3.1 | 135.4 ± 4.4 | <0.001 |
| Potassium, mmol/L, mean ± SD | 4.0 ± 0.5 | 4.0 ± 0.5 | 4.0 ± 0.5 | 0.638 |
| Phosphate, mg/dL, mean ± SD | 3.1 ± 0.8 | 3.2 ± 0.9 | 3.0 ± 0.8 | 0.066 |
| CRP, mg/dL, median (IQR) | 4.2 (0.9–9.9) | 1.5 (0.4–5.2) | 7.3 (4.0–13.5) | <0.001 |
| D-dimer, ng/mL, median (IQR) | 719 (408–1188) | 564 (306–1011) | 896 (540–1416) | <0.001 |
| Fibrinogen, mg/dL, mean ± SD | 604.3 ± 173.5 | 534.8 ± 151.6 | 669.6 ± 167.5 | <0.001 |
| AST, IU/L, median (IQR) | 32.0 (24.0–49.0) | 27.0 (22.0–36.0) | 39.5 (30.0–55.0) | <0.001 |
| ALT, IU/L, median (IQR) | 21.0 (14.0–34.0) | 20.0 (14.0–34.0) | 24.0 (15.0–36.5) | 0.118 |
| GGT, IU/L, median (IQR) | 30.0 (18.0–56.0) | 26.0 (16.0–44.0) | 36.0 (21.5–71.0) | <0.001 |
| Characteristic | Univariable Model | Multivariable Model | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p-Value | Odds Ratio | 95% CI | p-Value | |
| Age (per year) | 1.03 | 1.01 to 1.04 | <0.001 | 1.02 | 1.01 to 1.03 | <0.001 |
| Gender (male) | 1.86 | 1.30 to 2.67 | <0.001 | 1.50 | 0.96 to 2.32 | 0.074 |
| BMI (per 1 kg/m2) | 1.08 | 1.04 to 1.011 | <0.001 | 1.05 | 1.01 to 1.09 | 0.011 |
| BSA (per 0.1 m2) | 1.17 | 1.08 to 1.26 | <0.001 | 1.16 | 1.05 to 1.27 | 0.003 |
| Diabetes Mellitus | 2.00 | 1.30 to 2.67 | 0.002 | |||
| Hypertension | 2.11 | 1.41 to 3.18 | <0.001 | |||
| Hyperlipidemia | 1.49 | 0.95 to 2.34 | 0.083 | |||
| Cognitive decline | 1.65 | 0.97 to 2.81 | 0.065 | |||
| Baseline creatinine (per 1 mg/dL) | 1.37 | 0.98 to 1.93 | 0.068 | |||
| BUN (per 1 mg/dL) | 1.03 | 1.01 to 1.05 | 0.001 | |||
| Lymphocyte count (per 103/µL) | 0.39 | 0.29 to 0.53 | <0.001 | 0.58 | 0.41 to 0.81 | 0.002 |
| CRP (per mg/dL) | 1.15 | 1.11 to 1.20 | <0.001 | 1.11 | 1.07 to 1.16 | <0.001 |
| D-dimer (per 0.1 ug/mL) | 1.04 | 1.01 to 1.06 | 0.003 | |||
| Fibrinogen (per 10 ng/mL) | 1.05 | 1.04 to 1.07 | <0.001 | |||
| AST (per 10 IU/L) | 1.12 | 1.04 to 1.21 | 0.004 | |||
| GGT (per 10 IU/L) | 1.04 | 1.01 to 1.07 | 0.017 | |||
| ACE-I/ARB therapy | 1.75 | 1.06 to 2.89 | 0.027 | |||
| THRT | 1.85 | 0.99 to 3.44 | 0.052 | |||
| Diuretic therapy | 2.63 | 1.37 to 5.05 | 0.004 | |||
| Risk Factor | Univariate Analysis | Multivariate Analysis * | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age ≥60 years | 15.7 (2.1 to 115.8) | 0.007 | ||
| Sex (females vs. males) | 2.1 (1.1 to 4.3) | 0.039 | ||
| Hypertension | 2.0 (0.9 to 4.6) | 0.090 | 1.0 (0.5 to 2.4) | 0.950 |
| Diabetes mellitus | 1.3 (0.6 to 2.8) | 0.493 | 1.0 (0.5 to 2.2) | 0.916 |
| Established CVD | 2.3 (1.1 to 5.1) | 0.036 | 1.7 (0.8 to 3.8) | 0.187 |
| Chronic heart failure | 4.1 (1.8 to 9.1) | <0.001 | 2.7 (1.2 to 6.0) | 0.016 |
| Chronic renal failure # | 4.3 (2.0 to 9.3) | <0.001 | 2.8 (1.3 to 6.0) | 0.012 |
| Any Comorbidity $ | 17.0 (2.3 to 126.7) | 0.006 | 9.4 (1.2 to 75.4) | 0.035 |
| BMI ≥27.4 kg/m2 | 1.4 (1.7 to 2.8) | 0.392 | 1.4 (0.7 to 2.9) | 0.337 |
| BSA ≥ 1.9 m2 | 0.62 (0.31 to 1.20) | 0.175 | 0.86 (0.42 to 1.80) | 0.682 |
| CRP ≥4 mg/dL | 1.0 (0.5 to 2.2) | 0.954 | 1.1 (0.5 to 2.4) | 0.794 |
| Hypoxemia requiring ventilatory support | 2.2 (1.0 to 4.6) | 0.047 | 2.3 (1.1 to 4.9) | 0.036 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asleh, R.; Asher, E.; Yagel, O.; Samuel, T.; Elbaz-Greener, G.; Wolak, A.; Durst, R.; Ben-Chetrit, E.; Nir-Paz, R.; Helviz, Y.; et al. Predictors of Hypoxemia and Related Adverse Outcomes in Patients Hospitalized with COVID-19: A Double-Center Retrospective Study. J. Clin. Med. 2021, 10, 3581. https://doi.org/10.3390/jcm10163581
Asleh R, Asher E, Yagel O, Samuel T, Elbaz-Greener G, Wolak A, Durst R, Ben-Chetrit E, Nir-Paz R, Helviz Y, et al. Predictors of Hypoxemia and Related Adverse Outcomes in Patients Hospitalized with COVID-19: A Double-Center Retrospective Study. Journal of Clinical Medicine. 2021; 10(16):3581. https://doi.org/10.3390/jcm10163581
Chicago/Turabian StyleAsleh, Rabea, Elad Asher, Oren Yagel, Tal Samuel, Gabby Elbaz-Greener, Arik Wolak, Ronen Durst, Eli Ben-Chetrit, Ran Nir-Paz, Yigal Helviz, and et al. 2021. "Predictors of Hypoxemia and Related Adverse Outcomes in Patients Hospitalized with COVID-19: A Double-Center Retrospective Study" Journal of Clinical Medicine 10, no. 16: 3581. https://doi.org/10.3390/jcm10163581
APA StyleAsleh, R., Asher, E., Yagel, O., Samuel, T., Elbaz-Greener, G., Wolak, A., Durst, R., Ben-Chetrit, E., Nir-Paz, R., Helviz, Y., Rubin, L., Tvito, A., Glikson, M., & Amir, O. (2021). Predictors of Hypoxemia and Related Adverse Outcomes in Patients Hospitalized with COVID-19: A Double-Center Retrospective Study. Journal of Clinical Medicine, 10(16), 3581. https://doi.org/10.3390/jcm10163581