
Robot-Assisted Intracorporeal Orthotopic Ileal Neobladder: Description of the “Shell” Technique

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Definition of Population and Variables for Analyses
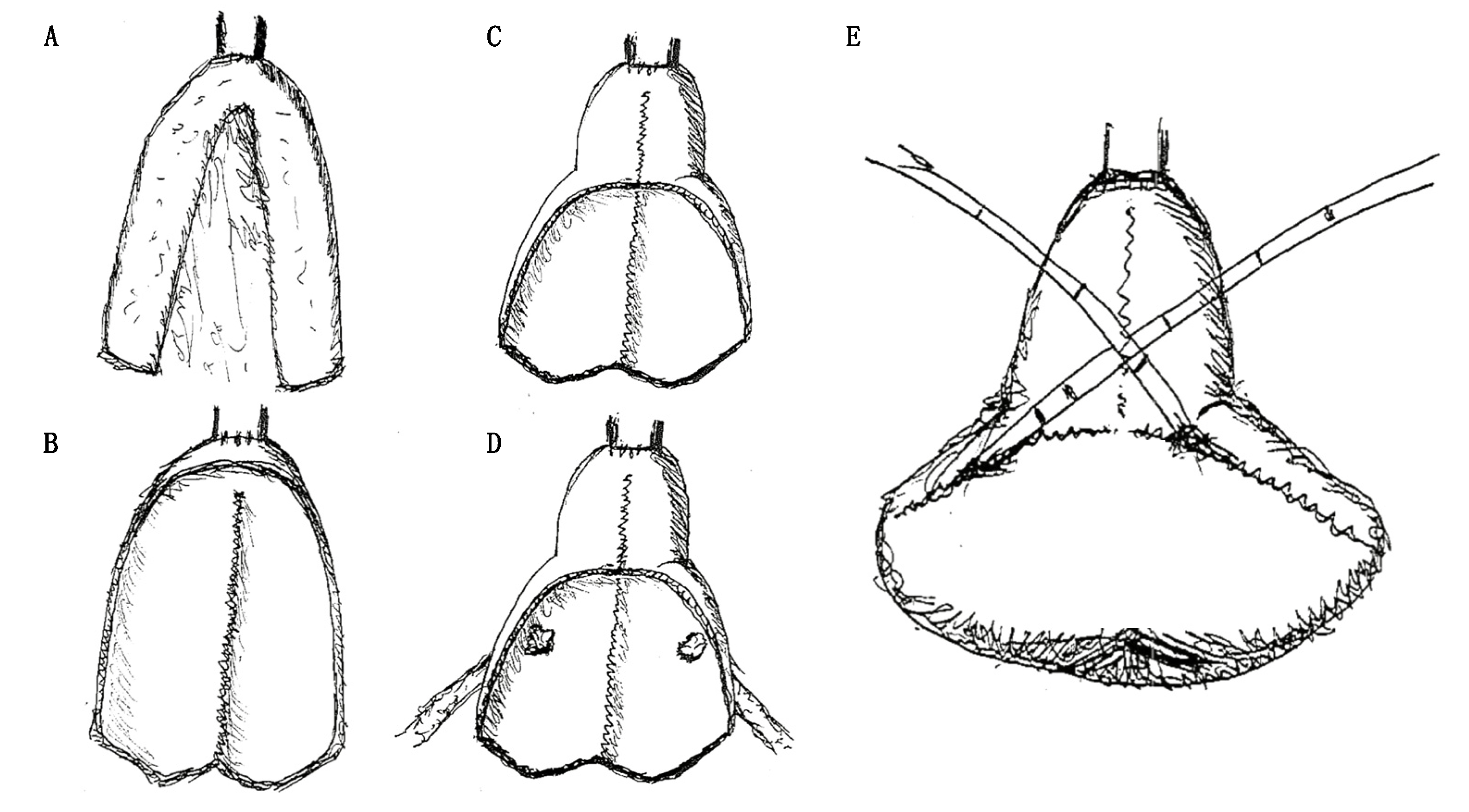
2.2. Description of the Surgical Technique
3. Results
3.1. Preoperative and Intraoperative Characteristics of the Study Population
3.2. Postoperative Outcomes and Complication Rate
3.3. Pathologic, Oncological and Functional Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
Ethical Approval
References
- Alfred Witjes, J.; Lebret, T.; Compérat, E.M.; Cowan, N.C.; De Santis, M.; Bruins, H.M.; Hernández, V.; Espinós, E.L.; Dunn, J.; Rouanne, M.; et al. Updated 2016 EAU Guidelines on Muscle-invasive and Metastatic Bladder Cancer. Eur. Urol. 2017, 71, 462–475. [Google Scholar] [CrossRef]
- Gill, I.S.; Cacciamani, G.E. The changing face of urologic oncologic surgery from 2000–2018 (63.141 patients)—Impact of robotics. Eur. Urol. Suppl. 2019, 18, e656–e657. [Google Scholar] [CrossRef]
- Hussein, A.A.; Ahmed, Y.E.; Kozlowski, J.D.; May, P.R.; Nyquist, J.; Sexton, S.; Curtin, L.; Peabody, J.O.; Abol-Enein, H.; Guru, K.A. Robot-assisted approach to ‘W’-configuration urinary diversion: A step-by-step technique. BJU. Int. 2017, 120, 152–157. [Google Scholar] [CrossRef]
- Hussein, A.A.; May, P.R.; Jing, Z.; Ahmed, Y.E.; Wijburg, C.J.; Canda, A.E.; Dasgupta, P.; Shamim Khan, M.; Menon, M.; Peabody, J.O.; et al. Outcomes of Intracorporeal Urinary Diversion after Robot-Assisted Radical Cystectomy: Results from the International Robotic Cystectomy Consortium. J. Urol. 2018, 199, 1302–1311. [Google Scholar] [CrossRef]
- Cacciamani, G.E.; Rajarubendra, N.; Artibani, W.; Gill, I.S. Robotic intracorporeal urinary diversion: State of the art. Curr. Opin. Urol. 2019, 29, 293–300. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Almeida, G.L.; Musi, G.; Mazzoleni, F.; Matei, D.V.; Brescia, A.; Detti, S.; de Cobelli, O. Intraoperative frozen pathology during robot-assisted laparoscopic radical prostatectomy: Can ALEXIS™ trocar make it easy and fast? J. Endourol. 2013, 27, 1213–1217. [Google Scholar] [CrossRef] [PubMed]
- Murphy, D.G.; Anderson, P. Robotic Radical Cystectomy with Intracorporeal Neobladder: Ready for Prime Time? Eur. Urol. 2013, 64, 742–743. [Google Scholar] [CrossRef] [PubMed]
- Wiklund, N.P.; Collins, J.W.; Ahonen, R.; Nyberg, T.; Hosseini, A.; Sooriakumaran, P.; Sanchez-Salas, R. Robot-assisted radical cystectomy with intracorporeal neobladder diversion: The karolinska experience. Indian J. Urol. 2014, 30, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Desai, M.M.; Abreu, A.L.D.C.; Chopra, S.; Azhar, R.A.; Berger, A.K.; Miranda, G.; Cai, J.; Gill, I.S.; Aron, M. Robotic radical cystectomy and intracorporeal urinary diversion: The USC technique. Indian J. Urol. 2014, 30, 300–306. [Google Scholar] [CrossRef]
- Simone, G.; Papalia, R.; Misuraca, L.; Tuderti, G.; Minisola, F.; Ferriero, M.; Vallati, G.E.; Guaglianone, S.; Gallucci, M. Robotic Intracorporeal Padua Ileal Bladder: Surgical Technique, Perioperative, Oncologic and Functional Outcomes. Eur. Urol. 2018, 73, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.S.; Sridhar, A.; Goldstraw, M.; Zacharakis, E.; Nathan, S.; Hines, J.; Cathcart, P.; Briggs, T.; Kelly, J.D. Robot-assisted intracorporeal pyramid neobladder. BJU Int. 2015, 116, 771–779. [Google Scholar] [CrossRef]
- Asimakopoulos, A.D.; Campagna, A.; Gakis, G.; Corona Montes, V.E.; Piechaud, T.; Hoepffner, J.L.; Mugnier, C.; Gaston, R. Nerve Sparing, Robot-Assisted Radical Cystectomy with Intracorporeal Bladder Substitution in the Male. J. Urol. 2016, 196, 1549–1557. [Google Scholar]
- Koie, T.; Ohyama, C.; Yoneyama, T.; Nagasaka, H.; Yamamoto, H.; Imai, A.; Hatakeyama, S.; Hashimoto, Y. Robotic cross-folded U-configuration intracorpo-real ileal neobladder for muscle-invasive bladder cancer: Initial experience and functional outcomes. Int. J. Med. Robot. 2018, 14, e1955. [Google Scholar] [CrossRef] [Green Version]
- Minervini, A.; Vanacore, D.; Vittori, G.; Milanesi, M.; Tuccio, A.; Siena, G.; Campi, R.; Mari, A.; Gavazzi, A.; Carini, M. Florence robotic intracorporeal neobladder (FloR-IN): A new reconfiguration strategy developed following the IDEAL guidelines. BJU Int. 2018, 121, 313–317. [Google Scholar] [CrossRef] [Green Version]
- Nouhaud, F.X.; Williams, M.; Yaxley, W.; Cho, J.; Perera, M.; Thangasamy, I.; Esler, R.; Coughlin, G. Robot-assisted orthotopic “W” ileal neobladder in male patients: Step-by-step video-illustrated technique and preliminary outcomes. J. Robot. Surg. 2020, 14, 739–744. [Google Scholar] [CrossRef]
- Thress, T.M.; Cookson, M.S.; Patel, S. Robotic Cystectomy with Intracorporeal Urinary Diversion: Review of Current Techniques and Outcomes. Urol. Clin. N. Am. 2018, 45, 67–77. [Google Scholar] [CrossRef]
- Mistretta, F.A.; Musi, G.; Collà Ruvolo, C.; Conti, A.; Luzzago, S.; Catellani, M.; Di Trapani, E.; Cozzi, G.; Bianchi, R.; Ferro, M.; et al. Robot-Assisted Radical Cystectomy for Non-metastatic Urothelial Carcinoma of Urinary Bladder: A Comparison Between Intracorporeal Versus Extracorporeal Ortho-topic Ileal Neobladder. J. Endourol. 2021, 35, 151–158. [Google Scholar] [CrossRef]
- Gaboardi, F.; Simonato, A.; Galli, S.; Lissiani, A.; Gregori, A.; Bozzola, A. Minimally invasive laparoscopic neobladder. J. Urol. 2002, 168, 1080–1083. [Google Scholar] [CrossRef]
- Hassan, A.A.; Elgamal, S.A.; Sabaa, M.A.; Salem, K.A.; Elmateet, M.S. Evaluation of direct versus non-refluxing technique and functional results in orthotopic Y-ileal neobladder after 12 years of follow up. Int. J. Urol. 2007, 14, 300–304. [Google Scholar] [CrossRef]
- Ferriero, M.; Simone, G.; Rocchegiani, A.; Buscarini, M.; Papalia, R.; Alcini, A.; Flammia, G.P.; Gallucci, M. Early and Late Urodynamic Assessment of Padua Ileal Bladder. Urology 2009, 73, 1357–1362. [Google Scholar] [CrossRef] [PubMed]
- Studer, U.E.; Danuser, H.; Thalmann, G.N.; Springer, J.P.; Turner, W.H. Antireflux nipples or afferent tubular segments in 70 patients with ileal low pressure bladder substitutes: Long-term results of a prospective randomized trial. J. Urol. 1996, 156, 1913–1917. [Google Scholar] [CrossRef]
- De Nunzio, C.; Cindolo, L.; Leonardo, C.; Antonelli, A.; Ceruti, C.; Franco, G.; Falsaperla, M.; Gallucci, M.; Alvarez-Maestro, M.; Minervini, A.; et al. Analysis of radical cystectomy and urinary diversion complications with the Clavien classification system in an Italian real life cohort. Eur. J. Surg. Oncol. 2013, 39, 792–798. [Google Scholar] [CrossRef]
- Novara, G.; Catto, J.; Wilson, T.; Annerstedt, M.; Chan, K.; Murphy, D.G.; Motttrie, A.; Peabody, J.O.; Skinner, E.C.; Wiklund, P.N.; et al. Systematic Review and Cumulative Analysis of Perioperative Outcomes and Complications After Robot-assisted Radical Cystectomy. Eur. Urol. 2015, 67, 376–401. [Google Scholar] [CrossRef] [PubMed]
- Wilson, T.G.; Guru, K.; Rosen, R.C.; Wiklund, P.; Annerstedt, M.; Bochner, B.H.; Chan, K.G.; Montorsi, F.; Mottrie, A.; Murphy, D.; et al. Best practices in robot-assisted radical cystectomy and urinary reconstruction: Recommendations of the Pasadena Consensus Panel. Eur. Urol. 2015, 67, 363–375. [Google Scholar] [CrossRef]
- Schwentner, C.; Sim, A.; Balbay, M.D.; Todenhöfer, T.; Aufderklamm, S.; Halalsheh, O.; Mischinger, J.; Böttge, J.; Rausch, S.; Bier, S.; et al. Robot-assisted radical cystectomy and intracorporeal neobladder formation: On the way to a standardized procedure. World J. Surg. Oncol. 2015, 13, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyritzis, S.I.; Hosseini, A.; Collins, J.; Nyberg, T.; Jonsson, M.N.; Laurin, O.; Khazaeli, D.; Adding, C.; Schumacher, M.; Wiklund, N.P. Oncologic, Functional, and Complications Outcomes of Robot-assisted Radical Cystectomy with Totally Intracorporeal Neobladder Diversion. Eur. Urol. 2013, 64, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Tae, J.H.; Pyun, J.H.; Shim, J.S.; Cho, S.; Kang, S.G.; Ko, Y.H.; Cheon, J.; Lee, J.G.; Kang, S.H. Oncological and functional outcomes of robot-assisted radical cys-tectomy in bladder cancer patients in a single tertiary center: Can these be preserved throughout the learning curve? Investig. Clin. Urol. 2019, 60, 463–471. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall (n = 30) | ||
|---|---|---|
| Age (years) | Median | 61 |
| IQR | 55–66 | |
| Body mass index (kg/m2) | Median | 26.9 |
| IQR | 24.5–29.4 | |
| T-stage | Ta-Tis-T1 | 10 (33.3%) |
| T2 | 20 (66.7%) | |
| Neoadjuvant CHT | Administered | 15 (50.0%) |
| Not administered | 15 (50.0%) | |
| Operative time (min) | Median | 493 |
| IQR | 433–530 | |
| Estimated blood loss (mL) | Median | 400 |
| IQR | 350–700 | |
| Overall (n = 30) | ||
|---|---|---|
| Length of stay (days) | Median | 11 |
| IQR | 10–17 | |
| Catheterization days | ≤14 days | 8 (26.7%) |
| >14 days | 22 (73.3%) | |
| Complication | Not occurred | 22 (73.3%) |
| Occurred | 8 (26.7%) | |
| Early complication (<30 days from discharge) | No complication | 16 (53.3%) |
| Clavien-Dindo 2 | 8 (26.7%) | |
| Clavien-Dindo 3a | 3 (10.0%) | |
| Clavien-Dindo 3b | 2 (6.7%) | |
| Clavien-Dindo 4a | 1 (3.3%) | |
| Late complication (>30 days from discharge) | No complication | 16 (53.3%) |
| Clavien-Dindo 1 | 1 (3.3%) | |
| Clavien-Dindo 2 | 4 (13.4%) | |
| Clavien-Dindo 3a | 5 (16.7%) | |
| Clavien-Dindo 3b | 3 (10.0%) | |
| Clavien-Dindo 4a | 1 (3.3%) | |
| Overall (n = 30) | ||
|---|---|---|
| pT-stage | T0 | 6 (20.0%) |
| Ta-Tis-T1 | 10 (33.3%) | |
| T2 | 8 (26.7%) | |
| T3 | 6 (20.0%) | |
| pN-stage | Absence of lymph node invasion | 28 (93.3%) |
| Lymph node invasion | 2 (6.7%) | |
| Number of removed lymph nodes | Median | 26 |
| IQR | 18–34 | |
| Tumour relapse | Yes | 2 (6.7%) |
| No | 28 (93.3%) | |
| Cancer specific mortality | Yes | 1 (3.3%) |
| No | 29 (96.7%) | |
| Other cause mortality | Yes | 1 (3.3%) |
| No | 29 (96.7%) | |
| Daytime continence | 0–1 pad | 22 (73.3%) |
| ≥2 pads | 5 (16.7%) | |
| 3 (10.0%) | ||
| Night-time continence | 0–1 pad | 18 (60.0%) |
| ≥2 pads | 9 (30.0%) | |
| Not assessable | 3 (10.0%) | |
| Potency recovery | Erectile dysfunction | 10 (33.3%) |
| Potency with PDE5i | 8 (26.7%) | |
| Complete potency recovery | 6 (20.0%) | |
| 6 (20.0%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bianchi, R.; Mistretta, F.A.; Musi, G.; Luzzago, S.; Morelli, M.; Lorusso, V.; Catellani, M.; Di Trapani, E.; Cozzi, G.; Ferro, M.; et al. Robot-Assisted Intracorporeal Orthotopic Ileal Neobladder: Description of the “Shell” Technique. J. Clin. Med. 2021, 10, 3601. https://doi.org/10.3390/jcm10163601
Bianchi R, Mistretta FA, Musi G, Luzzago S, Morelli M, Lorusso V, Catellani M, Di Trapani E, Cozzi G, Ferro M, et al. Robot-Assisted Intracorporeal Orthotopic Ileal Neobladder: Description of the “Shell” Technique. Journal of Clinical Medicine. 2021; 10(16):3601. https://doi.org/10.3390/jcm10163601
Chicago/Turabian StyleBianchi, Roberto, Francesco Alessandro Mistretta, Gennaro Musi, Stefano Luzzago, Michele Morelli, Vito Lorusso, Michele Catellani, Ettore Di Trapani, Gabriele Cozzi, Matteo Ferro, and et al. 2021. "Robot-Assisted Intracorporeal Orthotopic Ileal Neobladder: Description of the “Shell” Technique" Journal of Clinical Medicine 10, no. 16: 3601. https://doi.org/10.3390/jcm10163601