
Comparative Impact of PD-1 and PD-L1 Inhibitors on Advanced Esophageal or Gastric/Gastroesophageal Junction Cancer Treatment: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analyses (Data Synthesis and Analysis)
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Efficacy Outcomes
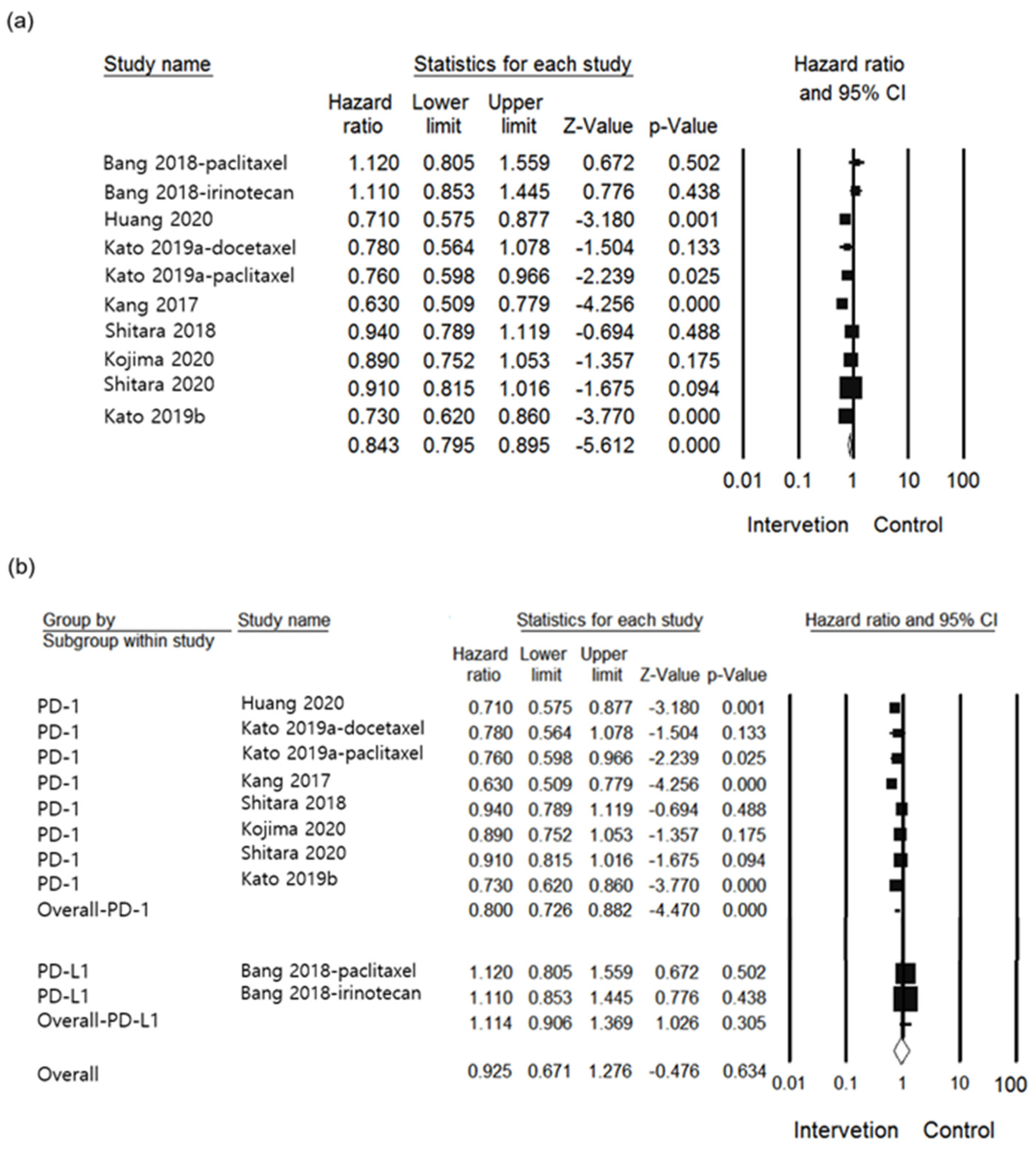
3.3.1. OS
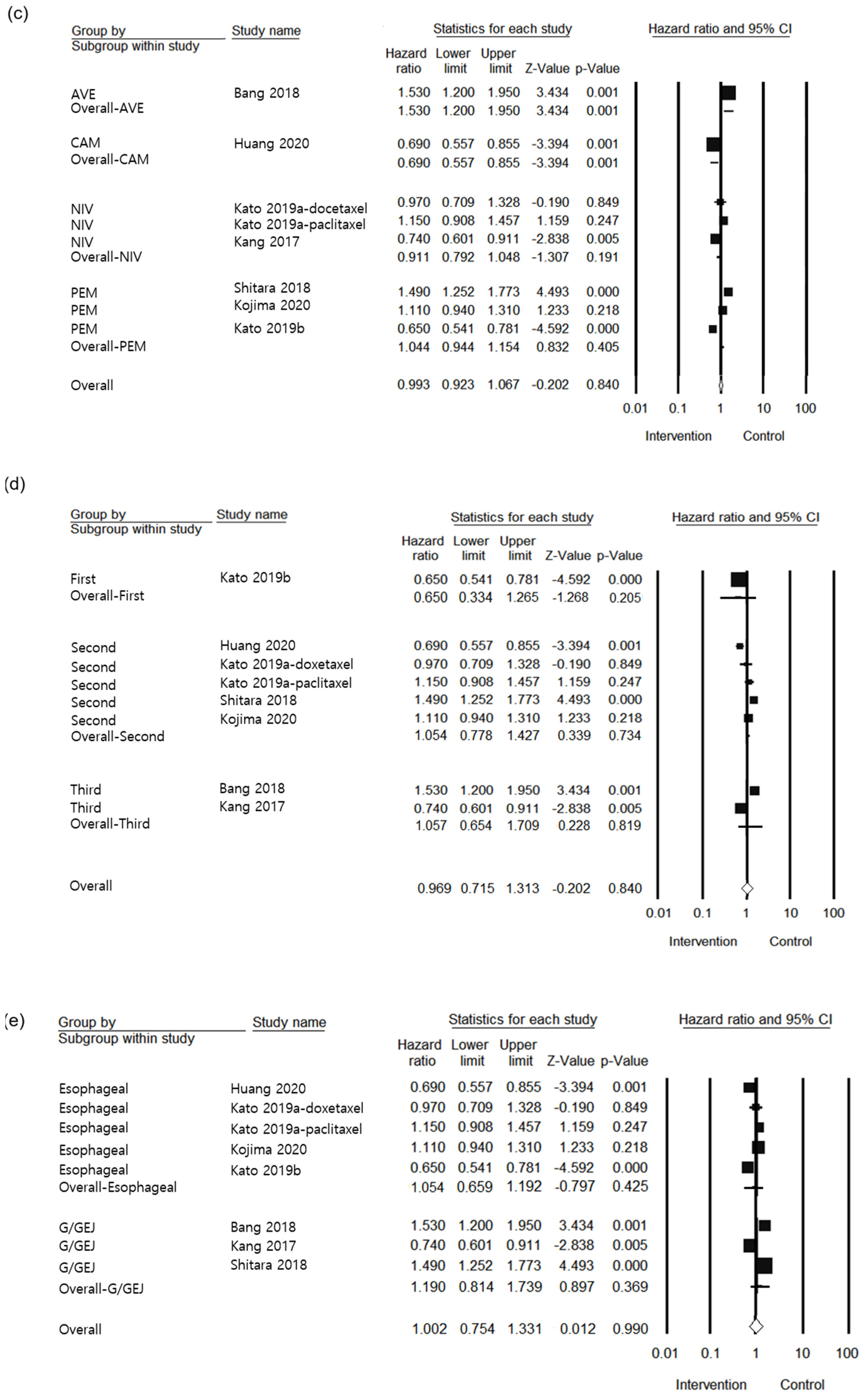
3.3.2. PFS
3.3.3. SAE
3.4. Risk of Bias and Strength of Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rawla, P.; Barsouk, A. Epidemiology of gastric cancer: Global trends, risk factors and prevention. Prz. Gastroenterol. 2019, 14, 26–38. [Google Scholar] [CrossRef]
- Raufi, A.G.; Almhanna, K. Immune checkpoint inhibitors for esophageal cancer: Are we moving in the right direction? Ann. Transl. Med. 2019, 7, S102. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network. Integrated genomic characterization of oesophageal carcinoma. Nature 2017, 541, 169–175. [Google Scholar] [CrossRef]
- Kelly, R.J.; Ajani, J.A. Adjuvant Nivolumab in Resected Esophageal or Gastroesophageal Junction Cancer. N. Engl. J. Med. 2021, 384, 1191–1203. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Chen, K.; Wang, X. The Anti-PD-1/PD-L1 Immunotherapy for Gastric Esophageal Cancer: A Systematic Review and Meta-Analysis and Literature Review. Cancer Control 2021, 28, 1073274821997430. [Google Scholar] [CrossRef]
- Short, M.W.; Burgers, K.G. Esophageal Cancer. Am. Fam. Phys. 2017, 95, 22–28. [Google Scholar]
- Wang, B.C.; Zhang, Z.J. Efficacy and safety of anti-PD-1/PD-L1 agents vs chemotherapy in patients with gastric or gastroesophageal junction cancer: A systematic review and meta-analysis. Medicine 2019, 98, e18054. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Guan, L.; Xu, M.; Wang, F. The efficacy and safety of antibodies targeting PD-1 for treatment in advanced esophageal cancer: A systematic review and meta-analysis. Transl. Oncol. 2021, 14, 101083. [Google Scholar] [CrossRef] [PubMed]
- Ni, X.; Xing, Y. The safety and efficacy of anti-PD-1/anti-PD-L1 antibody therapy in the treatment of previously treated, advanced gastric or gastro-oesophageal junction cancer: A meta-analysis of prospective clinical trials. Clin. Res. Hepatol. Gastroenterol. 2020, 44, 211–222. [Google Scholar] [CrossRef]
- Huedo-Medina, T.B.; Sanchez-Meca, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Barraclough, H.; Simms, L. Biostatistics primer: What a clinician ought to know: Hazard ratios. J. Thorac. Oncol. 2011, 6, 978–982. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, L.L.; Aguiar, P.N., Jr. Comparative Efficacy and Safety of Programmed Death-1 Pathway Inhibitors in Advanced Gastroesophageal Cancers: A Systematic Review and Network Meta-Analysis of Phase III Clinical Trials. Cancers 2021, 13, 2614. [Google Scholar] [CrossRef] [PubMed]
- Thorlund, K.; Mills, E.J. Sample size and power considerations in network meta-analysis. Syst. Rev. 2012, 1, 41. [Google Scholar] [CrossRef]
- Chen, Y.; Pei, Y. Looking for the Optimal PD-1/PD-L1 Inhibitor in Cancer Treatment: A Comparison in Basic Structure, Function, and Clinical Practice. Front. Immunol. 2020, 11, 1088. [Google Scholar] [CrossRef]
- Li, Z.; Li, X.; Lam, W.; Cao, Y.; Han, H.; Zhang, X.; Fang, J.; Xiao, K.; Zhou, F. Safety and Activity of Programmed Cell Death 1 Versus Programmed Cell Death Ligand 1 Inhibitors for Platinum-Resistant Urothelial Cancer: A Meta-Analysis of Published Clinical Trials. Front. Oncol. 2021, 11, 965. [Google Scholar]
- Page, M.J.; McKenzie, J.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372. [Google Scholar] [CrossRef]
- National Comprehensive Cancer. Gastric or Esophageal and Esophagogastric Junction Cancer Guideline. Available online: https://www.nccn.org/guidelines/category_1 (accessed on 1 August 2021).
- Higgins, J.P.; Altman, D.G. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Tierney, J.F.; Stewart, L.A. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Fleiss, J.L. Analysis of data from multiclinic trials. Control. Clin. Trials 1986, 7, 267–275. [Google Scholar] [CrossRef]
- Lin, L.; Chu, H. Quantifying publication bias in meta-analysis. Biometrics 2018, 74, 785–794. [Google Scholar] [CrossRef]
- Kang, Y.-K.; Boku, N. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 390, 2461–2471. [Google Scholar] [CrossRef]
- Shitara, K.; Özgüroğlu, M. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer (KEYNOTE-061): A randomised, open-label, controlled, phase 3 trial. Lancet 2018, 392, 123–133. [Google Scholar] [CrossRef]
- Bang, Y.J.; Ruiz, E.Y. Phase III, randomised trial of avelumab versus physician's choice of chemotherapy as third-line treatment of patients with advanced gastric or gastro-oesophageal junction cancer: Primary analysis of JAVELIN Gastric 300. Ann. Oncol. 2018, 29, 2052–2060. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Cho, B.C. Nivolumab versus chemotherapy in patients with advanced oesophageal squamous cell carcinoma refractory or intolerant to previous chemotherapy (ATTRACTION-3): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 1506–1517. [Google Scholar] [CrossRef]
- Kato, K.; Shah, M.A. KEYNOTE-590: Phase III study of first-line chemotherapy with or without pembrolizumab for advanced esophageal cancer. Future Oncol. 2019, 15, 1057–1066. [Google Scholar] [CrossRef] [PubMed]
- Kojima, T.; Shah, M.A. Randomized Phase III KEYNOTE-181 Study of Pembrolizumab Versus Chemotherapy in Advanced Esophageal Cancer. J. Clin. Oncol. 2020, 38, 4138–4148. [Google Scholar] [CrossRef]
- Huang, J.; Xu, J. Camrelizumab versus investigator’s choice of chemotherapy as second-line therapy for advanced or metastatic oesophageal squamous cell carcinoma (ESCORT): A multicentre, randomised, open-label, phase 3 study. Lancet Oncol. 2020, 21, 832–842. [Google Scholar] [CrossRef]
- Shitara, K.; Van Cutsem, E. Efficacy and Safety of Pembrolizumab or Pembrolizumab Plus Chemotherapy vs Chemotherapy Alone for Patients With First-line, Advanced Gastric Cancer: The KEYNOTE-062 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1571–1580. [Google Scholar] [CrossRef]
- Chuk, M.K.; Chang, J.T. FDA Approval Summary: Accelerated Approval of Pembrolizumab for Second-Line Treatment of Metastatic Melanoma. Clin. Cancer Res. 2017, 23, 5666–5670. [Google Scholar] [CrossRef]
- Cho, H.; Mariotto, A.B. When do changes in cancer survival mean progress? The insight from population incidence and mortality. J. Natl. Cancer Inst. Monogr. 2014, 2014, 187–197. [Google Scholar] [CrossRef]
- Blumenthal, G.M.; Karuri, S.W. Overall response rate, progression-free survival, and overall survival with targeted and standard therapies in advanced non-small-cell lung cancer: US Food and Drug Administration trial-level and patient-level analyses. J. Clin. Oncol. 2015, 33, 1008–1014. [Google Scholar] [CrossRef]
- Mushti, S.L.; Mulkey, F. Evaluation of Overall Response Rate and Progression-Free Survival as Potential Surrogate Endpoints for Overall Survival in Immunotherapy Trials. Clin. Cancer Res. 2018, 24, 2268–2275. [Google Scholar] [CrossRef]
- Yang, L.; Dong, X.Z. Efficacy and safety of anti-PD-1/anti-PD-L1 antibody therapy in treatment of advanced gastric cancer or gastroesophageal junction cancer: A meta-analysis. World J. Gastrointest. Oncol. 2020, 12, 1346–1363. [Google Scholar] [CrossRef]
- Han, Y.; Liu, D. PD-1/PD-L1 pathway: Current researches in cancer. Am. J. Cancer Res. 2020, 10, 727–742. [Google Scholar]
- Chen, S.; Zhang, Z. Response Efficacy of PD-1 and PD-L1 Inhibitors in Clinical Trials: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 562315. [Google Scholar] [CrossRef]
- Koneru, M.; Patnaik, A. A meta-analysis to indirectly compare the safety and efficacy of PD-1 and PD-L1 antibodies across solid tumors using a Bayesian hierarchical model. J. Clin. Oncol. 2018, 36, 3065. [Google Scholar] [CrossRef]
- Duan, J.; Cui, L. Use of Immunotherapy With Programmed Cell Death 1 vs Programmed Cell Death Ligand 1 Inhibitors in Patients With Cancer: A Systematic Review and Meta-analysis. JAMA Oncol. 2020, 6, 375–384. [Google Scholar] [CrossRef]
- De Mello, R.A.; Lordick, F. Current and Future Aspects of Immunotherapy for Esophageal and Gastric Malignancies. Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 237–247. [Google Scholar] [CrossRef]
- Salmaninejad, A.; Valilou, S.F. PD-1/PD-L1 pathway: Basic biology and role in cancer immunotherapy. J. Cell Physiol. 2019, 234, 16824–16837. [Google Scholar] [CrossRef]
- Wagner, A.D.; Syn, N.L. Chemotherapy for advanced gastric cancer. Cochrane Database Syst. Rev. 2017, 8, Cd004064. [Google Scholar] [CrossRef] [PubMed]
- Ventola, C.L. Cancer Immunotherapy, Part 2: Efficacy, Safety, and Other Clinical Considerations. Pharm. Ther. 2017, 42, 452–463. [Google Scholar]
- Nishimura, R.; Osonoi, T. A Randomized Pilot Study of the Effect of Trelagliptin and Alogliptin on Glycemic Variability in Patients with Type 2 Diabetes. Adv. Ther. 2019, 36, 3096–3109. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Shitara, K. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): A randomised, open-label, phase 3 trial. Lancet 2021, 398, 27–40. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Publication Year, Ref | Trial | Tumor | ClinicalTrials.gov Number | PD-1/PD-L1 Inhibitor | Control | Study Design | Phase | Patient Number (n) | Treatment Line | Primary Endpoint of Included Study | Intervention Methods | Used Outcomes | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention | Control | ||||||||||||
| Kang 2017 [24] | ATTRACTION-2 | G/GEJ | NCT02267343 | Nivolumab | Placebo | RCT | III | 330 | 163 | Third line | OS | Nivolumab 3 mg/kg Q2W a | OS, PFS, SAE |
| Shitara 2018 [25] | KEYNOTE-061 | G/GEJ | NCT02370498 | Pembrolizumab | Paclitaxel | RCT | III | 296 | 296 | Second line | OS | Pembrolizumab 200 mg Q3W b | OS, PFS |
| Bang 2018 [26] | JAVELIN Gastric 300 | G/GEJ | NCT02625623 | Avelumab | Paclitaxel or Irinotecan | RCT | III | 185 | 186 | Third line | OS | Avelumab 10 mg/kg Q2W a | OS, PFS |
| Kato 2019a [27] | ATTRACTION-3 | Esophageal | NCT02569242 | Nivolumab | Paclitaxel + Docetaxel | RCT | III | 210 | 209 | Second line | OS | Nivolumab 240 mg Q2W a | OS, PFS, SAE |
| Kato 2019b [28] | KEYNOTE-590 | Esophageal | NCT03189719 | Pembrolizumab | Placebo | RCT | III | 373 | 376 | First line | OS | Pembrolizumab 200 mg Q3W b | OS, PFS, SAE |
| Kojima 2020 [29] | KEYNOTE-181 | Esophageal | NCT02564263 | Pembrolizumab | Paclitaxel, Docetaxel or Irinotecan | RCT | III | 314 | 314 | Second line | OS | Pembrolizumab 200 mg Q3W b | OS, PFS |
| Huang 2020 [30] | ESCORT | Esophageal | NCT03099382 | Camrelizumab | Docetaxel or Irinotecan | RCT | III | 228 | 220 | Second line | OS | Camrelizumab 200 mg Q2W a | OS, PFS, SAE |
| Shitara 2020 [31] | KEYNOTE-062 | G/GEJ | NCT02494583 | Pembrolizumab | Cisplatin + Fluorouracil or Capecitabine | RCT | III | 256 | 250 | First line | OS | Pembrolizumab 200 mg Q3W b | OS |
| Outcomes | No. of Participants (Studies) | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Effect (95% CI) | Quality of Evidence |
|---|---|---|---|---|---|---|---|---|
| OS | ||||||||
| Overall | 3738 (8) | Not serious | Not serious | Not serious | Not serious | None | HR 0.843 (0.795, 0.895) | ⨁⨁⨁⨁ HIGH |
| Anti-PD-1 | 3835 (7) | Not serious | Not serious | Not serious | Not serious | None | HR 0.822 (0.773, 0.875) | ⨁⨁⨁⨁ HIGH |
| Anti-PD-L1 | 371 (1) | Not serious | Not serious | Not serious | Not serious | None | HR 1.114 (0.906, 1.369) | ⨁⨁⨁⨁ HIGH |
| Avelumab | 371 (1) | Not serious | Not serious | Not serious | Not serious | None | HR 1.114 (0.906, 1.369) | ⨁⨁⨁〇 MODERATE |
| Camrelizumab | 448 (1) | Not serious | Not serious | Not serious | Not serious | None | HR 0.710 (0.575, 0.877) | ⨁⨁⨁⨁ HIGH |
| Nivolumab | 912 (4) | Not serious | Not serious | Not serious | Not serious | None | HR 0.702 (0.608, 0.810) | ⨁⨁⨁⨁ HIGH |
| Pembrolizumab | 1847 (4) | Not serious | Not serious | Not serious | Not serious | None | HR 0.872 (0.811, 0.938) | ⨁⨁⨁⨁ HIGH |
| Treatment line (first) | 1255 (2) | Not serious | serious | Not serious | Not serious | None | HR 0.849 (0.775, 0.931) | ⨁⨁⨁〇 MODERATE |
| Treatment line (second) | 2087 (3) | Not serious | Not serious | Not serious | Not serious | None | HR 0.836 (0.763, 0.917) | ⨁⨁⨁⨁ HIGH |
| Treatment line (third) | 864 (2) | Not serious | serious | Not serious | Not serious | None | HR 0.845 (0.729, 0.980) | ⨁⨁⨁〇 MODERATE |
| Tumor site (esophageal) | 2244 (4) | Not serious | Not serious | Not serious | Not serious | None | HR 0.778 (0.710, 0.851) | ⨁⨁⨁⨁ HIGH |
| Tumor site (G/GEJ) | 1962 (4) | Not serious | serious | Not serious | Not serious | None | HR 0.897 (0.829, 0.971) | ⨁⨁⨁〇 MODERATE |
| PFS | ||||||||
| Overall | 3700 (7) | Not serious | Very serious | Not serious | Not serious | None | HR 0.993 (0.923, 1.067) | ⨁⨁〇〇 LOW |
| Anti-PD-1 | 3329 (6) | Not serious | serious | Not serious | Not serious | None | HR 0.951 (0.881, 1.026) | ⨁⨁⨁〇 MODERATE |
| Anti-PD-L1 | 371 (1) | Not serious | Not serious | Not serious | Serious | None | HR 1.530 (1.200, 1.950) | ⨁⨁⨁〇 MODERATE |
| Avelumab | 371 (1) | Not serious | Not serious | Not serious | Serious | None | HR 1.530 (1.200, 1.950) | ⨁⨁⨁〇 MODERATE |
| Camrelizumab | 448 (1) | Not serious | Not serious | Not serious | Not serious | None | HR 0.690 (0.557, 0.855) | ⨁⨁⨁⨁ HIGH |
| Nivolumab | 912 (2) | Not serious | Serious | Not serious | Not serious | None | HR 0.911 (0.792, 1.048) | ⨁⨁⨁〇 MODERATE |
| Pembrolizumab | 1969 (3) | Not serious | Not serious | Not serious | Not serious | None | HR 1.044 (0.944, 1.154) | ⨁⨁⨁⨁ HIGH |
| Treatment line (first) | 749 (1) | Not serious | Not serious | Not serious | Serious | None | HR 0.650 (0.541, 0.781) | ⨁⨁⨁〇 MODERATE |
| Treatment line (second) | 2161 (4) | Not serious | Serious | Not serious | Not serious | None | HR 1.097 (1.001, 1.203) | ⨁⨁⨁〇 MODERATE |
| Treatment line (third) | 864 (2) | Not serious | Serious | Not serious | Not serious | None | HR 1.006 (0.859, 1.179) | ⨁⨁⨁〇 MODERATE |
| Tumor site (esophageal) | 2244 (4) | Not serious | Serious | Not serious | Not serious | None | HR 0.880 (0.802, 0.965) | ⨁⨁⨁〇 MODERATE |
| Tumor site (G/GEJ) | 1456 (3) | Not serious | Serious | Not serious | Serious | None | HR 1.202 (1.069, 1.351) | ⨁⨁〇〇 LOW |
| SAE | 2147 (5) | Not serious | Serious | Not serious | Not serious | None | OR 0.983 (0.795, 1.217) | ⨁⨁⨁〇 MODERATE |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, S.; Kim, E.; Lee, H. Comparative Impact of PD-1 and PD-L1 Inhibitors on Advanced Esophageal or Gastric/Gastroesophageal Junction Cancer Treatment: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3612. https://doi.org/10.3390/jcm10163612
Oh S, Kim E, Lee H. Comparative Impact of PD-1 and PD-L1 Inhibitors on Advanced Esophageal or Gastric/Gastroesophageal Junction Cancer Treatment: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(16):3612. https://doi.org/10.3390/jcm10163612
Chicago/Turabian StyleOh, SuA, Eunyoung Kim, and Heeyoung Lee. 2021. "Comparative Impact of PD-1 and PD-L1 Inhibitors on Advanced Esophageal or Gastric/Gastroesophageal Junction Cancer Treatment: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 16: 3612. https://doi.org/10.3390/jcm10163612
APA StyleOh, S., Kim, E., & Lee, H. (2021). Comparative Impact of PD-1 and PD-L1 Inhibitors on Advanced Esophageal or Gastric/Gastroesophageal Junction Cancer Treatment: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 10(16), 3612. https://doi.org/10.3390/jcm10163612