Abstract
Heritable Disorders of Connective Tissue (HDCTs) are syndromes that disrupt connective tissue integrity. They include Osteogenesis Imperfecta (OI), Ehlers Danlos Syndrome (EDS), Marfan Syndrome (MFS), Loeys-Dietz Syndrome (LDS), Epidermolysis Bullosa (EB), Stickler Syndrome (STL), Wagner Syndrome, and Pseudoxanthoma Elasticum (PXE). Because many patients with HDCTs have ocular symptoms, commonly myopia, they will often present to the clinic seeking refractive surgery. Currently, corrective measures are limited, as the FDA contraindicates laser-assisted in-situ keratomileusis (LASIK) in EDS and discourages the procedure in OI and MFS due to a theoretically increased risk of post-LASIK ectasia, poor wound healing, poor refractive predictability, underlying keratoconus, and globe rupture. While these disorders present with a wide range of ocular manifestations that are associated with an increased risk of post-LASIK complications (e.g., thinned corneas, ocular fragility, keratoconus, glaucoma, ectopia lentis, retinal detachment, angioid streaks, and ocular surface disease), their occurrence and severity are highly variable among patients. Therefore, an HDCT diagnosis should not warrant an immediate disqualification for refractive surgery. Patients with minimal ocular manifestations can consider LASIK. In contrast, those with preoperative signs of corneal thinning and ocular fragility may find the combination of collagen cross-linking (CXL) with either photorefractive keratotomy (PRK), small incision lenticule extraction (SMILE) or a phakic intraocular lens (pIOL) implant to be more suitable options. However, evidence of refractive surgery performed on patients with HDCTs is limited, and surgeons must fully inform patients of the unknown risks and complications before proceeding. This paper serves as a guideline for future studies to evaluate refractive surgery outcomes in patients with HDCTs.
1. Introduction
Heritable Disorders of Connective Tissue (HDCTs) are a group of syndromes that disrupt connective tissue integrity and often cause systemic manifestations. HDCTs involving ocular manifestations include Osteogenesis Imperfecta (OI), Ehlers-Danlos Syndrome (EDS), Marfan Syndrome (MFS), Loeys-Dietz Syndrome (LDS), and Epidermolysis Bullosa (EB), Stickler Syndrome (STL), Wagner Syndrome, and Pseudoxanthoma Elasticum (PXE). Myopia is a common issue in patients with HDCTs and inevitably leads to patients seeking refractive surgery consultations.
Currently, corrective measures are limited, as the FDA states laser-assisted in-situ keratomileusis (LASIK) is an absolute contraindication in EDS. It is not recommended in disorders with abnormal collagen (e.g., MFS and OI) due to a theoretical increased risk of post-LASIK ectasia, poor wound healing, poor refractive predictability, and globe rupture. The concern for post-LASIK ectasia is based on the Ectasia risk score system, which lists abnormal preoperative corneal topography, low residual stromal bed thickness, young age, and thin preoperative corneal thickness as common risk factors in order of significance [1]. Another risk factor is the biomechanical weakening of the cornea from lower corneal hysteresis (CH), which is associated with a thinner central corneal thickness (CCT) and increased intraocular pressure (IOP) [2]. Due to these risk factors, there is potential for corneal or scleral rupture or staphyloma even without refractive surgeries being performed. Many of these risk factors (e.g., low CCT, keratoconus, increased rate of global ruptures) are commonly associated with the various HDCTs.
However, the above risk factors may not be problematic for every person with an HDCT diagnosis. For example, reduced CCT is associated with specific gene sequence variants [3], and clinical presentation for each HDCT is variable and wide-ranging in symptom severity [4,5,6,7,8,9,10,11,12,13,14,15,16,17,18]. The exact rate of post-LASIK complications has been difficult to assess due to limited refractive surgery cases performed on those diagnosed with HDCTs. A literature search revealed only one study surveying patients with EDS about their ophthalmic surgical experiences, showing 43% of patients had undergone radial keratotomy, PRK, LASIK, or LASEK. Of those, 23.3% reported complications, including under correction/regression (18.6%), postoperative pain (9.3%), impaired night vision (7%), dry eye (4.7%), induced astigmatism (7%) and corneal ectasia (4.7%) [19]. The survey demonstrates that refractive surgery on an EDS patient does not make any complication a foregone conclusion. A current perspective on ocular management of patients with MFS suggests corneal refractive surgery can be performed in those without lens dislocation and with mild cases of myopia [8].
Furthermore, the risk of post-LASIK ectasia continues to decrease due to advances in LASIK surgery and preoperative risk analysis [20]. Screening for refractive surgery eligibility is better due to advancements in measuring corneal tomography and hysteresis. These technological changes allow proper evaluation for the risk of ectasia in those diagnosed with HDCTs. Thus, those affected less symptomatically may undergo refractive surgery with safe outcomes.
Overall, the clinical variability and improvements in preoperative screening raise the question of whether a blanket contraindication to refractive surgery in patients with HDCTs is appropriate. This paper details the various clinical presentations of OI, EDS, MFS, LDS, EB, STL, Wagner Syndrome, and PXE and their subtypes to evaluate the spectrum of possibilities for refractive surgery. It also expands on the ocular manifestations that require consideration and evaluation preceding refractive surgery. Finally, it provides a framework to approach the therapeutic possibilities for refractive error correction in each HDCT.
2. Osteogenesis Imperfecta
Osteogenesis Imperfecta (OI) is a disorder disrupting type I collagen, affecting around 1 in 15,000 births and an estimated 25–50,000 people in the United States [21,22]. Approximately 90% of cases are autosomal dominant (AD) inherited mutations in COL1A1 or COL1A2 [4]. Because type I collagen contributes to tensile strength in tissue, common manifestations of OI are long bone fractures, low bone mineral density, bone pain, hearing loss, blue sclera, joint laxity, scoliosis, dental abnormalities, subcutaneous hemorrhages, and heart and lung problems [4,21]. However, symptoms vary between the five classifications of OI: type 1 typically presents with blue sclera and a mild, non-deforming phenotype due to a quantitative defect; type 2 is severe and lethal perinatally; type 3 presents with blue sclera and a moderate to severe, progressively deforming phenotype resulting in multiple fractures; type 4 is moderate with normal sclera and limited fractures; type 5 involves calcification of interosseous membranes (Table 1) [4,5,23].

Table 1.
Osteogenesis Imperfecta subtypes.
While type I collagen is found throughout the eye, it is primarily seen in the cornea and sclera. Type 1 collagen makes up around 70% of the cornea [26] and 90% of the sclera [5]. The absence of corneal K-structures, a sub-Bowman’s fibrous structure, in OI can lead to an absent or atrophic Bowman’s layer maybe be another reason for corneal stromal thinning [27]. The scleral integrity can be severely disrupted and translucent to the underlying uvea, resulting in blue sclera. OI can also present as thin cornea, megalocornea, keratoconus, ocular fragility, zonular cataracts, dislocated lens, congenital glaucoma, optic atrophy, papilledema, partial color blindness, detachment of Descemet’s membrane, or retinal and subhyaloid hemorrhage [21,28,29]. Eye rubbing or finger trauma can lead to corneal or global rupture due to increased ocular fragility, creating concern for scleral perforation during routine procedures [5].
Studies have routinely found patients with OI have a thinner CCT that ranges from 362–571 µm, with 52.9% below 500 µm [21]. A study revealed patients with blue sclera or type 1 OI have a significantly lower CCT [24,30,31]. The average CCT for types 3 and 4 is higher, at 510 µm and 500 µm, respectively [30]. Additionally, reduced CH has been observed in children with OI [24], though keratoconus has not been frequently seen [32].
3. Ehlers Danlos Syndrome
Ehlers Danlos Syndrome (EDS) is a heterogeneous group of HCTDs sharing characteristic features of joint hypermobility, skin hyperextensibility, and tissue fragility due to abnormal type 5 collagen [7]. The prevalence is ~ 1 in 5000 [33], with no specific inheritance pattern. It can be either AD or autosomal recessive (AR), depending on the subtype. Currently, the 13 subtypes of EDS are classified based on their varying clinical presentations: classical, classical-like, cardiac-valvular, vascular, hypermobile, arthrochalasia, dermatosparaxis, kyphoscoliotic, spondylodysplastic, musculocontractural, myopathic, periodontal, and Brittle Cornea Syndrome (BCS) [7].
The ocular manifestations within EDS are wide-ranging, and their prevalence and severity differ among subtypes (Table 2). Patients with EDS can present with blue sclera, epicanthic folds, floppy eyelids, widely spaced eyes, strabismus, high myopia with retinal detachment, keratoglobus/keratoconus, dry eyes, corneal fragility, and angioid streaks [17,34]. Classical, Kyphoscoliotic, and BCS subtypes are associated with significant ophthalmologic findings (i.e., globe rupture) [35,36]. The other subtypes present with minor ophthalmologic findings, except myopathic and periodontal EDS, with no reported eye findings [6].
Table 2.
Subtypes of Ehlers Danlos syndrome.
Classical EDS’s more severe ocular manifestations include blue sclera, thin CCT (410–450 µm), and steep corneas but without a known predisposition to keratoconus [26,41,42]. A case study of 62 patients with classical EDS found blue sclera in 84% of patients [43]. Conjunctivochalasis has also been reported [37]. The kyphoscoliotic subtype has frequent occurrences of corneal rupture with minimal trauma frequently occurs, and corneal pathology has shown an absent Bowman’s layer, marked stromal thinning, and Descemet’s membrane abnormalities [39]. Blue sclera, microcornea, corneal thinning (CCT as low as 400 µm), keratoconus, and keratoglobus may also be present [39,44]. BCS also has a high risk of corneal rupture but is less frequent than kyphoscoliotic EDS [45]. However, their CCT can be thinner than kyphoscoliotic EDS, reaching as low as 200 µm. BCS is also associated with stromal thinning, myopia, blue sclera, keratoconus, keratoglobus, and megalocornea [40,46].
For the less severe ocular findings, hypermobile EDS may present with dry eyes, pathologic myopia, vitreous abnormalities, and asymptomatic lens opacities [38]. In a study of 44 eyes with hypermobile EDS, no cases of keratoconus or significant differences in CCT (average CCT 540s µm) were found compared to controls [38,41]. However, corneal epithelial density was significantly lower, and stromal keratocyte density was higher [38]. In vascular EDS, a common feature is subtle globe protrusion, but retinal disorders, increased risk of globe rupture, and keratoconus are not common [41,46]. Cardiac-valvular, arthrochalasia, dermatosparaxis, and musculocontractural can present with myopia, astigmatism, and blue sclera [6]. Hypermetropia, microcornea, and corneal clouding have been reported in spondylodysplastic EDS [6]. Additionally, classical-like EDS has been reported with recurrent subconjunctival hemorrhages [47].
4. Marfan Syndrome
Marfan syndrome (MFS) is an AD inherited mutation in the FBN1 gene on chromosome 15 that encodes for fibrillin-147, leading to excessive signaling and activation of TBF-beta [9]. The prevalence is 1 in 5000 to 10,000 people [48]. The main clinical manifestations are long bone overgrowth, aortic root aneurysm, and ectopia lentis. Other common features include hypermobility, low bone mineral density, scoliosis, pectus excavatum and carinatum, dural ectasia, foot deformities, and generalized ligamentous laxity (Table 3) [9].
Table 3.
Heritable Diseases of Connective Tissue.
The most common ocular abnormality is ectopia lentis, occurring in 60–80% of cases due to the presence of fibrillin-1 in ciliary zonules [8]. Their corneas are also more deformed due to decreased bending resistance and capacity to dissipate energy [58,59]. Other associated findings include myopia, flat cornea, astigmatism, thinner CCT (thinned CCT as low as 502 µm), premature cataracts, retinal detachment (5–25.6%), glaucoma (33%), and anisocoria [8,49,60,61]. The prevalence of myopia is between 33–63%, with over 50% of those affected having ≥ –3D of myopia [8,62,63]. On the other hand, Konradsen found 61% of patients had < –3D of refractive error and flatter corneas, which compensated for increased myopia [64]. Children with MFS are more myopic and have decreased corneal curvature, CCT, and best-corrected visual acuity (BCVA) than controls [65].
5. Loeys-Dietz Syndrome
Loeys-Dietz Syndrome is an AD inherited disorder with mutations in TGF beta receptor 1 (TGFBR1), TGF beta receptor 2 (TGFBR2), TGF beta 2 (TGFB2), TGF beta 3 (TGFB3), or SMAD3 [10,50,66], with an estimated prevalence of ≤1 in 100,000 [51]. Systemic manifestations of LDS are similar to MFS, including vascular aneurysms (cerebral, thoracic, or abdominal), skeletal abnormalities (pectus excavatum or carinatum), scoliosis, joint laxity, and craniofacial abnormalities (cleft palate, craniosynostosis, or bifid uvula) [10]. Allergies, skin abnormalities, neurological findings, pulmonary manifestations, and pregnancy-related changes have also been reported [67,68]. The distinguishing characteristic separating LDS from MFS is the lack of lens dislocation [69].
Ocular manifestations include myopia, blue or dusky sclera, cataract, retinal detachment, retinal tortuosity, strabismus, and amblyopia [50,68,69,70]. An initial study involving 14 patients with LDS noted 13 with hypertelorism, seven with exotropia, and eight with blue sclera [50]. However, another retrospective review found no patients with hypertelorism or blue/dusky sclera [10], making it challenging to confirm these findings as diagnostic criteria for LDS. Patients with LDS have decreased CCT and increased myopia rates compared to controls, though myopia was less common and severe compared to patients with MFS [10]. The study found CCT was 521 +/− 48 µm in LDS compared to 542 +/− 37 µm in controls [10]. Further, presentations vary between genotypes, with more pronounced myopia, decreased CCT, and increased interpupillary distance (in men) in TGFBR2 compared to TGFBR1 [10].
6. Epidermolysis Bullosa
Epidermolysis Bullosa (EB) is characterized by epithelial tissue fragility, resulting in blisters and erosions from minimal trauma [71]. There are four main types of inherited EB: EB simplex (EBS), junctional EB (JEB), dystrophic EB (DEB), and Kindler Syndrome [17]. The prevalence of EB in the US is 0.4–4.6 per million and, specifically, 0.36 per million people for DEB [12]. EB can be inherited in an AD or AR form with mutations in keratin, laminin, collagen, or kindlin [71]. Dominantly inherited DEB (DDEB) presents at birth with skin blistering, dermal scarring, milia, and dystrophic nails, with normal teeth and oral mucosa. Recessively inherited DEB (RDEB) presents at birth with a wider range of symptoms, such as dermal blisters on the knees and elbows leading to joint deformity, polysyndactyly from scarring around the fingers, and oral mucosa involvement with tooth decay [11].
Eye involvement is common in EB, particularly the surface. Short-lived manifestations may include tearing, blistering of the eyelids, corneal erosions, conjunctival injection, and bullous keratopathy (Table 3) [17]. The presence of corneal erosions and blisters are high in RDEB (74.1%) and JEB (47.5%) and less prevalent in DDEB (2.12%) and EBS (6.19%) [12]. These issues can be treated with artificial tears, topical antibiotics, Vitamin A, topical fibronectin, and soft contact lenses [72]. A reduced tear break-up time (<8 s) occurs in 95.1% and an abnormal Schirmer test (<15 mm) in 92.4% [73], signifying dry eye disease (DED). Prolonged DED can lead to low corneal sensitivity, decreased cellular cohesion, poor tear quality, squamous metaplasia of the conjunctiva, and goblet cell loss [72], and requires treatment with lubricants/artificial tears [74].
Chronic sequelae such as pannus formation, corneal scarring, symblepharon, ankyloblepharon, and ectropion can occur and lead to significant vision loss or blindness [17]. Corneal scarring occurred in 50% of RDEB and 26.83% of JEB patients, but only in 0.95% of DDEB and 3.16% of EBS patients [12]. In RDEB, symblepharon and blepharitis were common findings, with 10.07% and 17.52% of patients affected, respectively [12]. Rare presentations include amblyopia, cataracts, strabismus, pseudopterygia, and microphthalmos [74].
7. Stickler Syndrome
Stickler Syndrome (STL) presents with conductive and sensorineural hearing loss, midfacial underdevelopment, cleft palate, and spondyloepiphyseal dysplasia [52,75]. It has an estimated prevalence of 1–3 in 10,000 [53]. This disorder can be caused by either AD inherited mutations of collagen type 2, collagen type 11, and lysyl oxidase or by AR inherited mutations in collagen type 9 and lysyl oxidase [13]. The most commonly seen mutations are in COL2A1 (STL type 1) and COL11A1 (STL type 2) [13].
Ocular findings include myopia, cataracts, vitreous alterations, glaucoma, and retinal detachments (Table 3) [52,75]. Huang found that 76% had high myopia (>−6D), and 69% had retinal detachment, many of which had a COL2A1 mutation [13]. One study found in COL2A1 mutations that 89% had myopia, 42% had vitreous abnormalities, and 55% had at least one retinal detachment [52]. Mutations in COL2A1 and COL11A1 are associated with early-onset high myopia [76]; however, myopia of ≥−10D was more common in COL2A1 than in COL11A1 (40% vs. 19%) [14]. Additionally, cataracts are more common in COL11A1 than in COL2A1 (59% vs. 36%) [14]. Studies show high rates of retinal detachment (45–69%) [13,14], causing poor visual acuity. Approximately 60–70% of individuals with STL type 1% and 40% with STL type 2 experience a retinal detachment, usually between 10–30 years of age [77]. Conversely, COL9A1 and COL9A3 rarely presented with retinal detachment [13].
8. Wagner Syndrome
Wagner Syndrome is caused by an AD inherited mutation in the VCAN gene on chromosome 5q [54], encoding for versican, an extracellular matrix proteoglycan contributing to the structural integrity of the vitreous [15]. The prevalence is unknown, with an estimated total of 300 individuals affected [55]. The hallmark of Wagner Syndrome is an optically empty vitreous with avascular strands, membranes, or veils [16,54,78]. Other ocular features are myopia, night blindness from chorioretinal atrophy, presenile cataract, retinal detachment, and occasional uveitis beginning in adolescence (Table 3) [78]. In contrast to STL, no systemic abnormalities have been described.
Mild to high myopia and astigmatism are prevalent, with some patients reaching > −10D [15,54,79]. Congenital glaucoma occurs, likely due to altered versican expression during trabecular meshwork development, and often requires surgical intervention [15,16]. Graeminger found peripheral tractional detachments in 55% of the eyes in patients over the age of 45 [16]. Additionally, all patients older than 45 exhibited chorioretinal atrophy and cataracts [16]. Not to mention, chorioretinal abnormalities and retinal detachments can still occur at a young age (5–15 years old) [54]. For this reason, annual visits with a retinal specialist are recommended.
9. Pseudoxanthoma Elasticum
Pseudoxanthoma elasticum (PXE) is an AR inherited mutation in the ABCC6 gene on chromosome 6 with a prevalence estimated between 1 in 25,000 to 100,000 people [17,56]. The mutation causes a defective cell membrane transporter with a subsequent buildup of dystrophic calcification in the elastic tissues of the skin, vasculature, and Bruch’s membrane (Table 3) [56,57]. It classically presents with characteristic small yellow papules on the neck and flexural areas that progress into reticulated plaques and cause loose and wrinkly skin. Cardiovascular manifestations include angina pectoris, arterial hypertension, atherosclerosis, valvular disease, myocardial infarction, cerebrovascular accident, and sudden cardiac death [17,56].
The presentation of PXE can be variable. AD type 1 typically has thin and delicate skin, accelerated atherosclerosis with mitral valve disease, and angioid streaks with choroidal neovascularization. AD type 2 has yellow, flat skin papules, skin hyperelasticity, and angioid streaks with blue sclera. AR-type 1, the most common form of PXE, has similar skin lesions and angioid streaks to AD type 1 with added gastrointestinal bleeding. Finally, AR-type 2, the rarest form of PXE, has severe skin manifestations and angioid streaks without other systemic manifestations [80]. PXE should not be confused with juvenile xanthogranuloma, a non-Langerhans cell histiocytosis with yellow or erythematous skin nodules found commonly on the head and neck and tumors in the iris or conjunctiva that may lead to glaucoma, hyphema, or vision loss [81].
The ocular manifestations of PXE primarily involve the posterior segment of the eye, with the most common being angioid streaks (85%) [17]. PXE can also have a peau d’orange appearance on fundoscopy, optic disc drusen (6–20%), chorioretinal atrophy with comet tail lesions, and macular degeneration with hemorrhage [18,82]. The earliest finding is usually the peau d’orange appearance, presenting as spotted hypo- and hyper-fluorescence on microscopy [18,56,82]. Before the age of 15, the peau d’orange appearance is frequently seen without signs of angioid streaks [83]. However, angioid streaks and choroidal neovascularization are typically present by their 40s [84], resulting in visual acuity of 20/200 or worse by their 4th or 5th decade of life [18,80,82].
10. Refractive Surgery Considerations and Consultation
An HDCT diagnosis is currently viewed as a contraindication to refractive surgery, with surgery attempts to be avoided in these patients. While some patients may remain poor refractive surgery candidates due to the combination of corneal biomechanics and ocular manifestations seen, we believe there is an opportunity to approach refractive surgery in those who have stable refractions and are less severely affected. We suggest a general framework to guide clinicians regarding refractive surgery in patients with HDCTs (Figure 1).
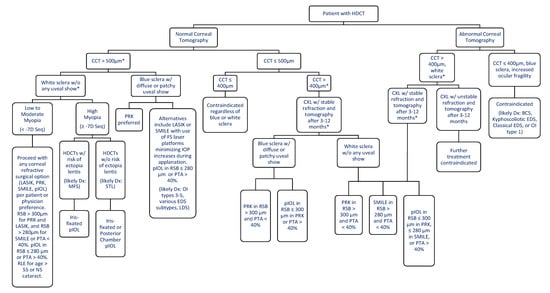
Figure 1.
Framework for refractive surgery in HDCT Patients. * Denotes every patient should have the typical biomechanical evaluation when considering refractive surgery measuring corneal hysteresis (CH) and a corneal resistance factor (CRF) using an ocular response analyzer (ORA; Reichert Ophthalmic Instruments, NY, USA) or dynamic schiempflug tonometer (DST; CorVis ST, OCULUS, Wetzlar, Germany). Normal corneal tomography refers to patients without signs of keratoconus, pellucid marginal degeneration or forme fruste keratoconus, asymmetric astigmatism, asymmetric corneal steepening. HDCT = Heritable Disorder of Connective Tissue, CCT—Central Corneal Thickness, CXL = Collagen Cross-linking, LASIK = Laser-Assisted in-situ keratomileusis, PRK = Photorefractive Keratectomy, SMILE = Small Incision Lenticule Extraction, Seq = Spherical equivalent, BCS = Brittle Cornea Syndrome, EDS = Ehlers Danlos Syndrome, OI = Osteogenesis Imperfecta, IOP = Intraocular Pressure, FS = Femtosecond, RSB = Residual Stromal Bed, pIOL = Phakic Intraocular Lens, PTA = Percent Tissue Alteration, RLE = Refractive Lens Exchange, NS= Nuclear Sclerotic.
In general, patients with a normal corneal tomography (no signs of keratoconus, asymmetric astigmatism, and pellucid marginal degeneration, a CCT > 500 µm, and white sclera without uveal showing can proceed with any corneal refractive surgery option per patient or physician preference. This assumes a residual stromal bed thickness (RSB) > 300 µm for PRK and LASIK or RSB > 280 µm for SMILE, and a percentage tissue altered (PTA) <40%, as well as a biomechanical evaluation measuring CH and a corneal resistance factor (CRF). An RSB > 280 µm for SMILE can be recommended due to the residual intact anterior corneal cap’s contribution to biomechanical stability, allowing for a reduced RSB in SMILE.
Corneal cross-linking (CXL) immediately after LASIK and the use of femtosecond lasers producing the lowest suction increase in IOP, such as VisuMax (Carl Zeiss Meditec AG, Jena, Germany) [85,86,87], can be utilized as added measures to prevent the development of ectasia or other intraoperative and postoperative complications [88,89]. If VisuMax is unavailable, other options to be considered are the Wavelight FS200 (Alcon Laboratories Inc., Fort Worth, TX, USA), LenSx (Alcon LenSx Inc., Aliso Viejo, CA, USA), or Victus (Bausch & Lomb Incorporated, Rochester, NY, USA). With any refractive surgery, larger optical zones require more tissue removal to achieve the same refractive power, leading to a smaller residual stromal bed [90]. This may increase the risk of ectasia [91] and forward displacement of the posterior cornea [92] and increase ocular fragility. For a 0.5 mm difference in optic zone size, an additional 3−4 microns of tissue is ablated for every diopter of myopic correction [90]. Therefore, using smaller optical zones is recommended. A refractive lens exchange is an option for patients over 55 years old or with early presence of nuclear sclerotic cataract. However, there is loss of accommodation and cumulative risk of retinal detachment over time.
Patients with blue sclera should proceed with caution regarding refractive surgery involving suction, such as LASIK or SMILE, due to the risk of intraoperative scleral rupture. In conjunction, femtosecond platforms with the lowest suction IOP increase (e.g., VisuMax) should be used. Patients who meet the above criteria but have high myopia > −7D may consider proceeding with pIOLs. Those who do not meet an RSB > 300 µm for PRK and LASIK or RSB > 280 µm for SMILE, or a percentage tissue altered (PTA) < 40% may also consider pIOLs. The pIOL can be placed in the posterior chamber, such as the Visian Implantable Collamer Lens (STAAR Surgical Co, Monrovia, CA, USA), or fixated to the iris, such as the Verisyse phakic lens (Artisan; Advanced Medical Optics, Santa Ana, CA, USA). Both options are safe, effective, and predictable in patients with high myopia and astigmatism [93,94,95,96,97,98]. Specifically, those with an increased risk of ectopia lentis, like MFS, should preferably use an iris-fixated pIOL. Those without risk of ectopia lentis, like STL, can proceed with either an iris-fixated or posterior chamber pIOL.
The following treatment considerations are for patients with a normal corneal tomography and biomechanical evaluation but a CCT ≤ 500 µm. For those with a CCT ≤ 400 µm, refractive surgery should be contraindicated regardless of white or blue sclera. For those with CCT > 400 µm, initial CXL can be performed. Patients may proceed with additional refractive surgery if stable refraction and normal tomography are seen 3–12 months after CXL. In patients with white sclera, PRK can be done with an RSB > 300 µm and SMILE with RSB > 280 µm, as long as PTA < 40%. Combining SMILE and CXL has been shown to safely protect against the development of ectasia [99,100]. However, for those with RSB ≤ 280 µm, patients may proceed with a pIOL. On the other hand, in those with blue sclera, PRK is preferred due to no risk of scleral rupture and can be done if the RSB is >300 µm. Those with a lower RSB can proceed with a pIOL.
Lastly, the following options are for patients with an abnormal corneal tomography (Figure 1). Surgery would be contraindicated if patients additionally have a CCT ≤ 400 µm, blue sclera, or ocular fragility (reflected by abnormal indices such as CH and CRF). These cases will likely include patients with BCS, kyphoscoliotic EDS, or OI type 1. Patients with a CCT > 400 µm, biomechanical evaluation, and white sclera can proceed with CXL. The increased corneal stiffness (reflected by improved CH and CRF) in CXL provides additional stability for patients with keratoconus [101,102,103]. However, further research addressing safety is needed as corneal melting has occurred in patients with keratoconus receiving CXL [104]. Patients with stable refraction and normal tomography may proceed with PRK if RSB > 300 µm or SMILE if RSB > 280 µm, as long as PTA < 40%. If the RSB is too low for PRK or SMILE, they can proceed with pIOL, which is effective and safe without keratoconus progression [105,106]. Those with low myopia and early signs of stable keratoconus who received PRK and CXL have been shown to stop disease progression and improve vision [107]. Patients who do not have stable refraction or normal tomography after CXL would be ineligible for refractive surgery.
11. Specific Recommendations
In OI patients presenting with blue sclera and very thin CCT (i.e., OI type 1), refractive surgery is likely contraindicated. However, OI type 1 with a CCT > 400 µm may potentially undergo initial CXL. With the presence of thicker corneas (CCT > 500 µm), OI types 3, 4, and 5 are likely eligible for any refractive surgery type, though some may need initial CXL. Given the prevalence of ocular fragility and reduced CH and CRF in patients with OI, femtosecond platforms with the lowest IOP suction increase (e.g., VisuMax) minimize the risk of complications in LASIK or SMILE. Further research is needed to determine the full scope of ocular manifestations and the natural progression of changes in visual acuity.
For kyphoscoliotic EDS and BCS, refractive surgery should not be pursued due to the extreme corneal thinning, presence of keratoconus and keratoglobus, and ocular fragility seen in these patients. Even CXL carries extreme risk as corneal perforation has occurred post-CXL in patients with BCS [36]. Those with normal corneal tomography and a CCT > 500 µm (typically classical-like, cardiac-valvular, arthrochalasia, spondylodysplastic, musculocontractural, myopathic, and periodontal) may receive refractive surgery of their choice. In dermatosparaxis EDS, the presence of congenital or early progressive myopia may make pIOL a more suitable option. Classical EDS often presents with a decreased CCT and steep cornea, making initial CXL the preferred pathway. Vascular EDS should also proceed down this same pathway, as post-LASIK development of myopic regression, Salzmann nodular degeneration, and dry eye syndrome has occurred [108].
Individuals with MFS typically present with normal corneal tomography and CCT > 500 µm. Additionally, a 10-year follow-up of patients with MFS showed stable myopia and no change in the frequency of those with refraction > -3D increased corneal thinning or keratoconus [109]. Given their ocular stability, many patients would be good candidates for any type of refractive surgery. Of note, a subset of these patients can present with high myopia, which would make iris-fixated pIOLs a suitable option in those without significant crystalline lenses or signs of iridodonesis. Patients that present with iridodonesis may benefit from sutureless methods such as the glued technique or Yamane technique. Placement of a posterior segment pIOL in one MFS patient with high myopic astigmatism and lens coloboma showed promising results, with a postoperative bilateral UCVA of 20/20 [110]. However, due to zonular weakness and erosion in these patients, an iris-fixated pIOL is preferred.
The two most common forms of LDS (TGFBR1 and TGFBR2) have average CCTs > 500 µm, and therefore, most are conducive to refractive surgery. With the presence of blue or dusky sclera, PRK would be preferable. An alternative would be LASIK or SMILE using femtosecond platforms with the lowest IOP suction increase (e.g., VisuMax). Keratoconus has been observed in a patient with LDS [10], although more research is needed to determine if initial CXL would benefit these patients.
Regardless of the EB subtype, the ocular surface needs to be optimized before any refractive surgery. It is also necessary for clinicians to evaluate limbal stem cell and corneal epithelium health with impression cytology or high-resolution anterior ocular coherence tomography. The presence of irregular ocular surface and DED in patients with EB makes LASIK a poor choice since dry eyes are the most common post-LASIK complication [111]. Therefore, PRK and SMILE would be more preferable options. The lack of flap in SMILE provides increased corneal stability and decreased incidence of postoperative dry eye compared to LASIK [112]. Patients who cannot optimize their ocular surface or are concerned about the recurrent corneal disease during the healing period of refractive surgery may want to consider pIOL.
Patients with STL present with myopia in childhood, but most studies show it is stable rather than progressive [14], making them promising candidates for surgical correction. However, before any refractive surgery, consultation with a retinal specialist is necessary due to the high prevalence of retinal detachment. No studies have reported their average CCT, but for those with >500 µm, any type of refractive surgery can be performed. Many of these patients will need a pIOL due to the increased prevalence of high myopia. The use of pIOLs needs to be approached with precaution as retinal detachments have occurred in 4.8% and 2.07% of the anterior chamber and posterior chamber pIOL surgeries, respectively [113,114]. Patients presenting with STL type 2 are likely better candidates for refractive surgery than STL type 1 due to decreased retinal detachments and the lower degree of myopia.
Due to the characteristic empty vitreous appearance and other posterior segment abnormalities in Wagner Syndrome, consultation with a vitreoretinal specialist is recommended before refractive surgery. If the vitreoretinal specialist approves, the patient can proceed with any refractive surgical option as their anterior segment is largely unaffected. For patients with high myopia, pIOL is an option but needs to be used cautiously due to the chance of retinal detachments [113,114].
Finally, patients with PXE should consult with a retinal specialist before refractive surgery due to their retinal abnormalities. Because no corneal abnormalities are noted in these patients, all refractive surgical options can be available. However, femtosecond platforms with the lowest IOP suction increase (e.g., VisuMax) may be beneficial in reducing the possibility of subretinal hemorrhage through breaks in Bruch’s membrane. The patient and surgeon should also discuss the long-term outcome of refractive surgery, as it will not solve the underlying retinal issues (i.e., angioid streaks and choroidal neovascularization) responsible for much of the vision loss in patients with PXE. Patients should be aware of the risk of blindness from the natural course of the disease.
12. Conclusions
This paper examined several HDCTs to determine whether a blanket contraindication for refractive surgery is appropriate. As myopia is more prevalent among patients with HDCTs, they will inevitably present for a refractive surgery consultation. Based on the ocular manifestations of each HDCT, an all-inclusive absolute contraindication may not be in the best interest of the patient seeking a refractive procedure. Certain HDCTs and their subtypes are more amenable to refractive surgery than others. Because of phenotypic variation, every patient should be evaluated on an individual basis and provided appropriate options. However, surgery should not be performed if these patients do not meet the minimum recommendations for each procedure listed in our framework. Furthermore, any patient presenting with symptoms of HDCTs may be advised for genetic testing with a geneticist who specializes in hypermobility and connective tissue disorders with the genes outlined in Table 1, Table 2 and Table 3.
A limitation of this study is the lack of published scientific literature on refractive surgery outcomes in patients with HDCTs. The creation of these guidelines and recommendations are based on the principles of refractive surgery and corneal biomechanics, knowledge of excimer and femtosecond lasers, known risk factors for post-refractive complications, and the ocular characteristics of each HDCT. Therefore, the guidelines do not serve as definitive cutoffs for eligibility, and surgeons must use their best judgment and intuition to determine the appropriate course of action for each patient. Given the lack of large-scale, long-term studies on refractive surgery outcomes in patients with HDCTs, surgeons need to ensure that patients are fully informed and consented to the high degree of unknown risks and complications before moving forward with these elective surgeries. Nevertheless, the hope is that this paper will change the paradigm that refractive surgery is contraindicated in all patients with HDCTs and prompt future studies, including the role of biomechanical evaluation in determining the safety and efficacy of surgical options in these patients.
Author Contributions
Conceptualization, M.M., M.R.B.; writing—original draft preparation, M.R.B., R.H., A.J.W.; writing—review and editing, M.M., M.R.B., R.H., A.J.W., B.P., Y.C.R.; visualization, M.R.B., R.H.; supervision, M.M., Y.C.R.; project administration, M.M.; funding acquisition, P.C.H.; resources, P.C.H. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work, and have given final approval to the version to be published. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by an unrestricted grant from Research to Prevent Blindness (RPB), 360 Lexington Avenue, 22nd Floor New York, NY 10017. No support was received for the publication of this article.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
We confirm that this publication is original.
Conflicts of Interest
The authors declare no conflict of interest or financial interest.
References
- Randleman, J.B.; Woodward, M.; Lynn, M.J.; Stulting, R.D. Risk Assessment for Ectasia after Corneal Refractive Surgery. Ophthalmology 2008, 115, 37–50.e4. [Google Scholar] [CrossRef]
- Kamiya, K.; Hagishima, M.; Fujimura, F.; Shimizu, K. Factors affecting corneal hysteresis in normal eyes. Graefe’s Arch. Clin. Exp. Ophthalmol. 2008, 246, 1491–1494. [Google Scholar] [CrossRef]
- Świerkowska, J.; Gajecka, M. Genetic factors influencing the reduction of central corneal thickness in disorders affecting the eye. Ophthalmic Genet. 2017, 38, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Thomas, I.H.; DiMeglio, L.A. Advances in the Classification and Treatment of Osteogenesis Imperfecta. Curr. Osteoporos. Rep. 2016, 14, 1–9. [Google Scholar] [CrossRef]
- Treurniet, S.; Burger, P.; Ghyczy, E.A.; Verbraak, F.D.; Tafili, K.R.C.; Micha, D.; Bravenboer, N.; Ralston, S.H.; de Vries, R.; Moll, A.C.; et al. Ocular characteristics and complications in patients with osteogenesis imperfecta: A systematic review. Acta Ophthalmol. 2021. [Google Scholar] [CrossRef]
- Brady, A.F.; Demirdas, S.; Fournel-Gigleux, S.; Ghali, N.; Giunta, C.; Kapferer-Seebacher, I.; Kosho, T.; Mendoza-Londono, R.; Pope, M.F.; Rohrbach, M.; et al. The Ehlers-Danlos syndromes, rare types. Am. J. Med. Genet. C Semin. Med. Genet. 2017, 175, 70–115. [Google Scholar] [CrossRef]
- De Paepe, A.; Malfait, F. The Ehlers-Danlos syndrome, a disorder with many faces. Clin. Genet. 2012, 82, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ansari, S.; Esfandiari, H.; Mohammad-Rabei, H.; Mets, M.B. Management strategies of ocular abnormalities in patients with marfan syndrome: Current perspective. J. Ophthalmic Vis. Res. 2019, 14, 71–77. [Google Scholar] [CrossRef]
- Bitterman, A.D.; Sponseller, P.D. Marfan Syndrome. J. Am. Acad. Orthop. Surg. 2017, 25, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Busch, C.; Voitl, R.; Goergen, B.; Zemojtel, T.; Gehle, P.; Salchow, D.J. Ocular findings in Loeys-Dietz syndrome. Br. J. Ophthalmol. 2018, 102, 1036–1040. [Google Scholar] [CrossRef]
- Mahdavi, M.; Javadi, M.-A. External Ocular Manifestations in Autosomal Dominant Dystrophic Epidermolysis Bullosa; a Case Report. J. Ophthalmic Vis. Res. 2008, 3, 70–73. [Google Scholar] [PubMed]
- Fine, J.-D.; Johnson, L.B.; Weiner, M.; Stein, A.; Cash, S.; Deleoz, J.; Devries, D.T.; Suchindran, C. Eye involvement in inherited epidermolysis bullosa: Experience of the National Epidermolysis Bullosa Registry. Am. J. Ophthalmol. 2004, 138, 254–262. [Google Scholar] [CrossRef]
- Huang, L.; Chen, C.; Wang, Z.; Sun, L.; Li, S.; Zhang, T.; Luo, X.; Ding, X. Mutation Spectrum and De Novo Mutation Analysis in Stickler Syndrome Patients with High Myopia or Retinal Detachment. Genes 2020, 11, 882. [Google Scholar] [CrossRef] [PubMed]
- Boysen, K.B.; La Cour, M.; Kessel, L. Ocular complications and prophylactic strategies in Stickler syndrome: A systematic literature review. Ophthalmic Genet. 2020, 41, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Jewsbury, H.; Fry, A.E.; Watts, P.; Nas, V.; Morgan, J. Congenital glaucoma in Wagner syndrome. J. AAPOS 2014, 18, 291–293. [Google Scholar] [CrossRef]
- Graemiger, R.A.; Niemeyer, G.; Schneeberger, S.A.; Messmer, E.P. Wagner Vitreoretinal Degeneration Follow-up of the Original Pedigree. Ophthalmology 1995, 102, 1830–1839. [Google Scholar] [CrossRef]
- Jen, M.; Nallasamy, S. Ocular manifestations of genetic skin disorders. Clin. Dermatol. 2016, 34, 242–275. [Google Scholar] [CrossRef]
- Egliem, M.; Zaeytijd, J.E.; Finger, R.P.; Holz, F.G.; Leroy, B.P.; Issa, P.E. An update on the ocular phenotype in patients with pseudoxanthoma elasticum. Front. Genet. 2013, 4, 14. [Google Scholar] [CrossRef]
- Louie, A.; Meyerle, C.; Francomano, C.; Srikumaran, D.; Merali, F.; Doyle, J.J.; Bower, K.; Bloom, L.; Boland, M.V.; Mahoney, N.; et al. Survey of Ehlers‒Danlos Patients’ ophthalmic surgery experiences. Mol. Genet. Genom. Med. 2020, 8, e1155. [Google Scholar] [CrossRef]
- Tatar, M.G.; Kantarci, F.A.; Yildirim, A.; Uslu, H.; Colak, H.N.; Goker, H.; Gürler, B. Risk Factors in Post-LASIK Corneal Ectasia. J. Ophthalmol. 2014, 2014, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Keleş, A.; Doğuizi, S.; Şahin, N.M.; Koç, M.; Aycan, Z. Anterior Segment Findings in Patients with Osteogenesis Imperfecta: A Case-Control Study. Cornea 2020, 39, 935–939. [Google Scholar] [CrossRef]
- MedlinePlus. Osteogenesis Imperfecta. Available online: https://medlineplus.gov/genetics/condition/osteogenesis-imperfecta/#frequency (accessed on 22 July 2021).
- Subramanian, S.; Viswanathan, V.K. Osteogenesis Imperfecta Continuing Education Activity. Available online: https://www.ncbi.nlm.nih.gov/books/NBK536957/?report=printable (accessed on 19 July 2021).
- Lagrou, L.M.; Gilbert, J.; Hannibal, M.; Caird, M.S.; Thomas, I.; Moroi, S.E.; Bohnsack, B.L. Altered corneal biomechanical properties in children with osteogenesis imperfecta. J. AAPOS 2018, 22, 183–187.e1. [Google Scholar] [CrossRef]
- Warman, M.L.; Cormier-Daire, V.; Hall, C.; Krakow, D.; Lachman, R.; LeMerrer, M.; Mortier, G.; Mundlos, S.; Nishimura, G.; Rimoin, D.L.; et al. Nosology and classification of genetic skeletal disorders: 2010 revision. Am. J. Med. Genet. A 2011, 155, 943–968. [Google Scholar] [CrossRef]
- Pesudovs, K. Orbscan mapping in Ehlers-Danlos syndrome. J. Cataract Refract. Surg. 2004, 30, 1795–1798. [Google Scholar] [CrossRef]
- Kobayashi, A.A.; Higashide, T.; Yokogawa, H.; Yamazaki, N.; Masaki, T.; Sugiyama, K. In vivo laser confocal microscopy findings of a cornea with osteogenesis imperfecta. Clin. Ophthalmol. 2014, 8, 429–433. [Google Scholar] [CrossRef][Green Version]
- Gorovoy, M.S.; Gorovoy, I.R.; Ullman, S.; Gorovoy, J.B. Descemet Stripping Automated Endothelial Keratoplasty for Spontaneous Descemet Membrane Detachment in a Patient with Osteogenesis Imperfecta. Cornea 2012, 31, 832–835. [Google Scholar] [CrossRef]
- Polat, N.; Ulucan, P.B. Nontraumatic Descemet Membrane Detachment with Tear in Osteogenesis Imperfecta. Ophthalmol. Ther. 2015, 4, 59–63. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hald, J.; Folkestad, L.; Swan, C.Z.; Wanscher, J.; Schmidt, M.; Gjørup, H.; Haubek, D.; Leonhard, C.-H.; Larsen, D.; Hjortdal, J.; et al. Osteogenesis imperfecta and the teeth, eyes, and ears—A study of non-skeletal phenotypes in adults. Osteoporos. Int. 2018, 29, 2781–2789. [Google Scholar] [CrossRef]
- Evereklioglu, C.; Madenci, E.; Bayazit, Y.A.; Yilmaz, K.; Balat, A.; Bekir, N.A. Central corneal thickness is lower in osteogenesis imperfecta and negatively correlates with the presence of blue sclera. Ophthalmic Physiol. Opt. 2002, 22, 511–515. [Google Scholar] [CrossRef]
- Magalhaes, O.A.; Rohenkohl, H.C.; de Souza, L.T.; Schuler-Faccini, L.; Félix, T.M. Collagen I Defect Corneal Profiles in Osteogenesis Imperfecta. Cornea 2018, 37, 1561–1565. Available online: www.corneajrnl.com (accessed on 19 July 2021). [CrossRef]
- MedlinePlus. Ehlers-Danlos Syndrome. Available online: https://medlineplus.gov/ehlersdanlossyndrome.html (accessed on 22 July 2021).
- Beighton, P. Serious ophthalmological complications in the Ehlers-Danlos syndrome. Br. J. Ophthalmol. 1970, 54, 263–268. [Google Scholar] [CrossRef]
- Ticho, U.; Ivry, M.; Merin, S. Brittle cornea, blue sclera, and red hair syndrome (the brittle cornea syndrome). Br. J. Ophthalmol. 1980, 64, 175–177. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Ben Margines, J.; Jacobs, D.; Rabinowitz, Y.S.; Hanser, E.M.; Chauhan, T.; Chung, D.; Bykhovskaya, Y.; Gaster, R.N.; Aldave, A.J. Corneal Perforation After Corneal Cross-Linking in Keratoconus Associated with Potentially Pathogenic ZNF469 Mutations. Cornea 2019, 38, 1033–1039. [Google Scholar] [CrossRef]
- Whitaker, J.K.; Alexander, P.; Chau, D.Y.; Tint, N.L. Severe conjunctivochalasis in association with classic type Ehlers-Danlos syndrome. BMC Ophthalmol. 2012, 12, 47. [Google Scholar] [CrossRef]
- Gharbiya, M.; Moramarco, A.; Castori, M.; Parisi, F.; Celletti, C.; Marenco, M.; Mariani, I.; Grammatico, P.; Camerota, F. Ocular Features in Joint Hypermobility Syndrome/Ehlers-Danlos Syndrome Hypermobility Type: A Clinical and In Vivo Confocal Microscopy Study. Am. J. Ophthalmol. 2012, 154, 593–600.e1. [Google Scholar] [CrossRef] [PubMed]
- Cameron, J.A. Corneal Abnormalities in Ehlers-Danlos Syndrome Type VI. Cornea 1993, 12, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Wright, E.M.B.; Spencer, H.L.; Daly, S.B.; Manson, F.; Zeef, L.A.; Urquhart, J.; Zoppi, N.; Bonshek, R.; Tosounidis, I.; Mohan, M.; et al. Mutations in PRDM5 in Brittle Cornea Syndrome Identify a Pathway Regulating Extracellular Matrix Development and Maintenance. Am. J. Hum. Genet. 2011, 88, 767–777. [Google Scholar] [CrossRef]
- McDermott, M.L.; Holladay, J.T.; Liu, D.; Puklin, J.E.; Shin, D.H.; Cowden, J.W. Corneal topography in Ehlers-Danlos syndrome. J. Cataract Refract. Surg. 1998, 24, 1212–1215. [Google Scholar] [CrossRef]
- Segev, F.; Héon, E.; Cole, W.G.; Wenstrup, R.J.; Young, F.; Slomovic, A.R.; Rootman, D.S.; Whitaker-Menezes, D.; Chervoneva, I.; Birk, D.E. Structural Abnormalities of the Cornea and Lid Resulting from Collagen V Mutations. Investig. Opthalmology Vis. Sci. 2006, 47, 565–573. [Google Scholar] [CrossRef]
- Colombi, M.; Dordoni, C.; Venturini, M.; Ciaccio, C.; Morlino, S.; Chiarelli, N.; Zanca, A.; Calzavara-Pinton, P.; Zoppi, N.; Castori, M.; et al. Spectrum of mucocutaneous, ocular and facial features and delineation of novel presentations in 62 classical Ehlers-Danlos syndrome patients. Clin. Genet. 2017, 92, 624–631. [Google Scholar] [CrossRef]
- Ihme, A.; Risteli, L.; Krieg, T.; Risteli, J.; Feldmann, U.; Kruse, K.; Müller, P.K.; Ristell, J. Biochemical characterization of variants of the Ehlers-Danlos syndrome type VI. Eur. J. Clin. Investig. 1983, 13, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Ramappa, M.; Wilson, M.E.; Rogers, R.C.; Trivedi, R. Brittle cornea syndrome: A case report and comparison with Ehlers Danlos syndrome. J. AAPOS 2014, 18, 509–511. [Google Scholar] [CrossRef]
- Byers, P.H.; Belmont, J.; Black, J.; De Backer, J.; Frank, M.; Jeunemaitre, X.; Johnson, D.; Pepin, M.; Robert, L.; Sanders, L.; et al. Diagnosis, natural history, and management in vascular Ehlers-Danlos syndrome. Am. J. Med. Genet. C Semin. Med. Genet. 2017, 175, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Demirdas, S.; Dulfer, E.; Robert, L.; Kempers, M.; Van Beek, D.; Micha, D.; Van Engelen, B.; Hamel, B.; Schalkwijk, J.; Loeys, B.; et al. Recognizing the tenascin-X deficient type of Ehlers–Danlos syndrome: A cross-sectional study in 17 patients. Clin. Genet. 2017, 91, 411–425. [Google Scholar] [CrossRef]
- Dietz, H.; McKusick, V.A. Marfan Syndrome. Available online: https://rarediseases.org/rare-diseases/marfan-syndrome/ (accessed on 22 July 2021).
- Gehle, P.; Goergen, B.; Pilger, D.; Ruokonen, P.; Robinson, P.N.; Salchow, D.J. Biometric and structural ocular manifestations of Marfan syndrome. PLoS ONE 2017, 12, e0183370. [Google Scholar] [CrossRef] [PubMed]
- Loeys, B.; Chen, J.; Neptune, E.R.; Judge, D.; Podowski, M.; Holm, T.; Meyers, J.; Leitch, C.C.; Katsanis, N.; Sharifi, N.; et al. A syndrome of altered cardiovascular, craniofacial, neurocognitive and skeletal development caused by mutations in TGFBR1 or TGFBR2. Nat. Genet. 2005, 37, 275–281. [Google Scholar] [CrossRef]
- Loughborough, W.W.; Minhas, K.S.; Rodrigues, J.; Lyen, S.M.; Burt, H.E.; Manghat, N.; Brooks, M.J.; Stuart, G.; Hamilton, M.C.K. Cardiovascular Manifestations and Complications of Loeys-Dietz Syndrome: CT and MR Imaging Findings. Radiographics 2018, 38, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Hoornaert, K.P.; Vereecke, I.; Dewinter, C.; Rosenberg, T.; A Beemer, F.; Leroy, J.G.; Bendix, L.; Björck, E.; Bonduelle, M.; Boute, O.; et al. Stickler syndrome caused by COL2A1 mutations: Genotype–phenotype correlation in a series of 100 patients. Eur. J. Hum. Genet. 2010, 18, 872–880. [Google Scholar] [CrossRef]
- Goldenberg, P.C. Stickler Syndrome. Available online: https://rarediseases.org/rare-diseases/stickler-syndrome/ (accessed on 21 July 2021).
- Araújo, J.R.; Tavares-Ferreira, J.; Silva, S.E.; Rocha, P.; Brandão, E.; Faria, P.A.; Falcão-Reis, F.; Rocha-Sousa, A. WAGNER syndrome: Anatomic, functional and genetic characterization of a Portuguese family. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 256, 163–171. [Google Scholar] [CrossRef]
- MedlinePlus. Wagner Syndrome. Available online: https://medlineplus.gov/genetics/condition/wagner-syndrome/#:~:text=Wagner%20syndrome%20is%20a%20rare,individuals%20are%20from%20the%20Netherlands (accessed on 21 July 2021).
- Finger, R.P.; Charbel Issa, P.; Ladewig, M.S.; Götting, C.; Szliska, C.; Scholl, H.P.; Holz, F.G. Pseudoxanthoma Elasticum: Genetics, Clinical Manifestations and Therapeutic Approaches. Surv. Ophthalmol. 2009, 54, 272–285. [Google Scholar] [CrossRef]
- Germain, D.P. Pseudoxanthoma elasticum. Orphanet J. Rare Dis. 2017, 12, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Beene, L.C.; Traboulsi, E.I.; Seven, I.; Ford, M.R.; Roy, A.S.; Butler, R.S.; Dupps, W.J. Corneal Deformation Response and Ocular Geometry: A Noninvasive Diagnostic Strategy in Marfan Syndrome. Am. J. Ophthalmol. 2016, 161, 56–64.e1. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Scheibenberger, D.; Frings, A.; Steinberg, J.; Schüler, H.; Druchkiv, V.; Katz, T.; Von Kodolitsch, Y.; Linke, S. Ocular manifestation in Marfan syndrome: Corneal biomechanical properties relate to increased systemic score points. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 256, 1159–1163. [Google Scholar] [CrossRef] [PubMed]
- Sultan, G.; Baudouin, C.; Auzerie, O.; Jean, M.D.S.; Goldschild, M.; Pisella, P.-J. Cornea in Marfan disease: Orbscan and in vivo confocal microscopy analysis. Investig. Ophthalmol. Vis. Sci. 2002, 43, 1757–1764. [Google Scholar]
- Nahum, Y.; Spierer, A. Ocular features of Marfan syndrome: Diagnosis and management. Isr. Med. Assoc. J. 2008, 10, 179–181. [Google Scholar] [PubMed]
- Maumenee, I.H. The eye in the Marfan syndrome. Birth Defects Orig. Artic. Ser. 1982, 18, 515–524. [Google Scholar] [PubMed]
- Kinori, M.; Wehrli, S.; Kassem, I.S.; Azar, N.F.; Maumenee, I.H.; Mets, M.B. Biometry Characteristics in Adults and Children with Marfan Syndrome: From the Marfan Eye Consortium of Chicago. Am. J. Ophthalmol. 2017, 177, 144–149. [Google Scholar] [CrossRef]
- Konradsen, T.R.; Zetterström, C. A descriptive study of ocular characteristics in Marfan syndrome. Acta Ophthalmol. 2013, 91, 751–755. [Google Scholar] [CrossRef] [PubMed]
- Salchow, D.J.; Gehle, P. Ocular manifestations of Marfan syndrome in children and adolescents. Eur. J. Ophthalmol. 2019, 29, 38–43. [Google Scholar] [CrossRef]
- MedlinePlus. Loeys-Dietz Syndrome. Available online: https://medlineplus.gov/genetics/condition/loeys-dietz-syndrome/ (accessed on 21 July 2021).
- Loeys, B.L.; Dietz, H.C. Loeys-Dietz Syndrome. In GeneReviews®; Adam, M.P., Ardinger, H.H., Pagon, R.A., Eds.; University of Washington: Seattle, WA, USA, 2008. [Google Scholar]
- Van Hemelrijk, C.; Renard, M.; Loeys, B. The Loeys–Dietz syndrome: An update for the clinician. Curr. Opin. Cardiol. 2010, 25, 546–551. [Google Scholar] [CrossRef]
- Van De Laar, I.M.B.H.; Van Der Linde, D.; Oei, E.H.G.; Bos, P.K.; Bessems, J.H.; Bierma-Zeinstra, S.M.; Van Meer, B.L.; Pals, G.; Oldenburg, R.A.; Bekkers, J.A.; et al. Phenotypic spectrum of the SMAD3-related aneurysms–osteoarthritis syndrome. J. Med. Genet. 2012, 49, 47–57. [Google Scholar] [CrossRef] [PubMed]
- MacCarrick, G.; Black, J.H.; Bowdin, S.; El-Hamamsy, I.; Frischmeyer-Guerrerio, P.A.; Guerrerio, A.L.; Sponseller, P.D.; Loeys, B.; Dietz, H.C. Loeys–Dietz syndrome: A primer for diagnosis and management. Genet. Med. 2014, 16, 576–587. [Google Scholar] [CrossRef] [PubMed]
- Laimer, M.; Prodinger, C.; Bauer, J.W. Hereditäre Epidermolysen. JDDG J. Ger. Soc. Dermatol. 2015, 13, 1125–1134. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Dogru, M.; Tsubota, K. Ocular Surface Findings in Hallopeau-Siemens Subtype of Dystrophic Epidermolysis Bullosa Report of a Case and Literature Review. Cornea 2005, 24, 474–479. [Google Scholar] [CrossRef]
- Hung Chow Lee, B.W.; Tan, J.; Radjenovic, M.; Tat, L.; Murrell, D.F.; Coroneo, M.T. Prospective study of the ocular manifestations in epidermolysis bullosa and autoimmune blistering diseases identifies dry eye disease. Investig. Ophthalmol. Vis. Sci. 2019, 60, 4707. Available online: https://iovs.arvojournals.org/article.aspx?articleid=2744191 (accessed on 5 July 2021).
- Tong, L.; Hodgkins, P.R.; Denyer, J.; Brosnahan, D.; Harper, J.; Russell-Eggitt, I.; I Taylor, D.S.; Atherton, D. The eye in epidermolysis bullosa. Br. J. Ophthalmol. 1999, 83, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Robin, N.H.; Moran, R.T.; Ala-Kokko, L. Stickler Syndrome. In GeneReviews®; Adam, M.P., Ardinger, H.H., Pagon, R.A., Eds.; University of Washington: Seattle, WA, USA, 1993–2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK1302/ (accessed on 22 July 2021).
- Zhou, L.; Xiao, X.; Li, S.; Jia, X.; Wang, P.; Sun, W.; Zhang, F.; Li, J.; Li, T.; Zhang, Q. Phenotypic characterization of patients with early-onset high myopia due to mutations in COL2A1 or COL11A1: Why not Stickler syndrome? Mol. Vis. 2018, 24, 560–573. [Google Scholar]
- Boothe, M.; Morris, R.; Robin, N. Stickler Syndrome: A Review of Clinical Manifestations and the Genetics Evaluation. J. Pers. Med. 2020, 10, 105. [Google Scholar] [CrossRef]
- Kloeckener-Gruissem, B.; Amstutz, C. VCAN-Related Vitreoretinopathy. Available online: https://www.ncbi.nlm.nih.gov/books/ (accessed on 19 July 2021).
- Jansen, L. Degeneratio Hyaloideo-Retinalis Hereditaria. Ophthalmologica 1962, 144, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Georgalas, I.; Tservakis, I.; Papaconstantinou, D.; Kardara, M.; Koutsandrea, C.; Ladas, I. Pseudoxanthoma elasticum, ocular manifestations, complications and treatment. Clin. Exp. Optom. 2011, 94, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Martín, M.H.-S.; Vargas-Mora, P.; Aranibar, L. Xantogranuloma juvenil: Una entidad con amplio espectro clínico. Actas Dermo-Sifiliogr. 2020, 111, 725–733. [Google Scholar] [CrossRef]
- Gliem, M.; Birtel, J.; Müller, P.L.; Hendig, D.; Faust, I.; Herrmann, P.; Holz, F.G.; Adamus, G.; Charbel Issa, P. Acute Retinopathy in Pseudoxanthoma Elasticum. JAMA Ophthalmol. 2019, 137, 1165–1173. [Google Scholar] [CrossRef]
- Naouri, M.; Boisseau, C.; Bonicel, P.; Daudon, P.; Bonneau, D.; Chassaing, N.; Martin, L. Manifestations of pseudoxanthoma elasticum in childhood. Br. J. Dermatol. 2009, 161, 635–639. [Google Scholar] [CrossRef]
- Orssaud, C.; Roche, O.; Dufier, J.-L.; Germain, D.P. Visual Impairment in Pseudoxanthoma Elasticum: A Survey of 40 Patients. Ophthalmic Genet. 2015, 36, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Lauzirika, G.; Garcia-Gonzalez, M.; Bolivar, G.; Hernández-Verdejo, J.L.; Sánchez, V.B.; Gros-Otero, J.; Teus, M.A. Measurement of the Intraocular Pressure Elevation During Laser-Assisted In Situ Keratomileusis Flap Creation Using a Femtosecond Laser Platform. Transl. Vis. Sci. Technol. 2021, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Strohmaier, C.; Runge, C.; Seyeddain, O.; Emesz, M.; Nischler, C.; Dexl, A.; Grabner, G.; Reitsamer, H.A. Profiles of Intraocular Pressure in Human Donor Eyes during Femtosecond Laser Procedures—A Comparative Study. Investig. Opthalmology Vis. Sci. 2013, 54, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Vetter, J.M.; Holzer, M.P.; Teping, C.; Weingärtner, W.E.; Gericke, A.; Stoffelns, B.; Pfeiffer, N.; Sekundo, W. Intraocular Pressure During Corneal Flap Preparation: Comparison Among Four Femtosecond Lasers in Porcine Eyes. J. Refract. Surg. 2011, 27, 427–433. [Google Scholar] [CrossRef]
- Kanellopoulos, J. Long-term safety and efficacy follow-up of prophylactic higher fluence collagen cross-linking in high myopic laser-assisted in situ keratomileusis. Clin. Ophthalmol. 2012, 6, 1125–1130. [Google Scholar] [CrossRef][Green Version]
- Kanellopoulos, A.J. Comparison of Sequential vs Same-Day Simultaneous Collagen Cross-Linking and Topography-Guided PRK for Treatment of Keratoconus. J. Refract. Surg. 2009, 25, S812–S818. [Google Scholar] [CrossRef]
- Gatinel, D.; Hoang-Xuan, T.; Azar, D.T. Volume estimation of excimer laser tissue ablation for correction of spherical myopia and hyperopia. Investig. Ophthalmol. Vis. Sci. 2002, 43, 1445–1449. [Google Scholar]
- Santhiago, M.; Giacomin, N.; Smadja, D.; Bechara, S. Ectasia risk factors in refractive surgery. Clin. Ophthalmol. 2016, 10, 713–720. [Google Scholar] [CrossRef]
- Li, M.; Yang, D.; Zhao, Y.; Yang, W.; Shang, J.; Zhou, X.; Yao, P.; Yang, D.; Lin, X.; Zhou, X. Impact of ablation ratio on 5-year postoperative posterior corneal stability after refractive surgery: SMILE and FS-LASIK. Eye Vis. 2020, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Alfonso, J.F.; Fernández-Vega, L.; Fernandes, P.; Gonzalez-Meijome, J.M.; Montés-Micó, R. Collagen copolymer toric posterior chamber phakic intraocular lens for myopic astigmatism. J. Cataract Refract. Surg. 2010, 36, 568–576. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Lim, D.H.; Nam, S.W.; Yang, C.M.; Chung, E.S.; Chung, T.-Y. Ten-year clinical outcomes after implantation of a posterior chamber phakic intraocular lens for myopia. J. Cataract Refract. Surg. 2019, 45, 1555–1561. [Google Scholar] [CrossRef] [PubMed]
- Alfonso, J.F.; Palacios, A.; Montés-Micó, R. Myopic Phakic STAAR Collamer Posterior Chamber Intraocular Lenses for Keratoconus. J. Refract. Surg. 2008, 24, 867–874. [Google Scholar] [CrossRef] [PubMed]
- Güell, J.L.; Morral, M.; Gris, O.; Gaytan, J.; Sisquella, M.; Manero, F. Five-Year Follow-up of 399 Phakic Artisan–Verisyse Implantation for Myopia, Hyperopia, and/or Astigmatism. Ophthalmology 2008, 115, 1002–1012. [Google Scholar] [CrossRef] [PubMed]
- Tehrani, M.; Dick, B.H. Iris-fixated toric phakic intraocular lens: Three-year follow-up. J. Cataract Refract. Surg. 2006, 32, 1301–1306. [Google Scholar] [CrossRef]
- Ruckhofer, J.; Seyeddain, O.; Dexl, A.K.; Grabner, G.; Stoiber, J. Correction of myopic astigmatism with a foldable iris-claw toric phakic intraocular lens: Short-term follow-up. J. Cataract Refract. Surg. 2012, 38, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Konstantopoulos, A.; Liu, Y.-C.; Teo, E.P.; Nyein, C.L.; Yam, G.H.; Mehta, J.S. Corneal Stability of LASIK and SMILE When Combined with Collagen Cross-Linking. Transl. Vis. Sci. Technol. 2019, 8, 21. [Google Scholar] [CrossRef] [PubMed]
- Brar, S.; Gautam, M.; Sute, S.S.; Ganesh, S. Refractive surgery with simultaneous collagen cross-linking for borderline corneas—A review of different techniques, their protocols and clinical outcomes. Indian J. Ophthalmol. 2020, 68, 2744–2756. [Google Scholar] [CrossRef]
- Sorkin, N.; Varssano, D. Corneal Collagen Crosslinking: A Systematic Review. Ophthalmologica 2014, 232, 10–27. [Google Scholar] [CrossRef]
- Pawiroranu, S.; Herani, D.N.; Setyowati, R.; Mahayana, I.T. Outcomes of corneal collagen cross linking prior to photorefractive keratectomy in prekeratoconus. Ann. Res. Hosp. 2017, 1, 1. [Google Scholar] [CrossRef]
- Kymionis, G.D.; Kontadakis, G.; Kounis, G.A.; Portaliou, D.M.; Karavitaki, A.E.; Magarakis, M.; Yoo, S.; Pallikaris, I.G. Simultaneous Topography-Guided PRK Followed by Corneal Collagen Cross-Linking for Keratoconus. J. Refract. Surg. 2009, 25, 807–811. [Google Scholar] [CrossRef]
- Labiris, G.; Kaloghianni, E.; Koukoula, S.; Zissimopoulos, A.; Kozobolis, V.P. Corneal melting after collagen cross-linking for keratoconus: A case report. J. Med. Case Rep. 2011, 5, 152. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, K.; Shimizu, K.; Kobashi, H.; Igarashi, A.; Komatsu, M.; Nakamura, A.; Kojima, T.; Nakamura, T. Three-year follow-up of posterior chamber toric phakic intraocular lens implantation for the correction of high myopic astigmatism in eyes with keratoconus. Br. J. Ophthalmol. 2015, 99, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Moshirfar, M.; Grégoire, F.J.; Mirzaian, G.; Whitehead, G.F.; Kang, P.C. Use of Verisyse iris-supported phakic intraocular lens for myopia in keratoconic patients. J. Cataract Refract. Surg. 2006, 32, 1227–1232. [Google Scholar] [CrossRef]
- Al-Amri, A.M. 5-year follow-up of combined non-topography guided photorefractive keratectomy and corneal collagen cross linking for keratoconus. Int. J. Ophthalmol. 2018, 11, 48–52. [Google Scholar] [CrossRef]
- Hopping, G.; Somani, A.N.; Vaidyanathan, U.; Liu, H.; Barnes, J.R.; Ronquillo, Y.; Hoopes, P.C.; Moshirfar, M. Myopic regression and recurrent Salzmann nodule degeneration after laser in situ keratomileusis in Ehlers Danlos Syndrome. Am. J. Ophthalmol. Case Rep. 2020, 19, 100729. [Google Scholar] [CrossRef]
- Sandvik, G.F.; Vanem, T.T.; Rand-Hendriksen, S.; Cholidis, S.; Sæthre, M.; Drolsum, L.; Saethre, M. Ten-year reinvestigation of ocular manifestations in Marfan syndrome. Clin. Exp. Ophthalmol. 2019, 47, 212–218. [Google Scholar] [CrossRef]
- Singh, B.; Sharma, S.; Dadia, S.; Bharti, N.; Bharti, S. Bilateral Toric Phakic Intraocular Lens Implantation for Correction of High Myopic Astigmatism in a Patient with Marfan Syndrome with Lens Coloboma: A Case Report. Case Rep. Ophthalmol. 2021, 12, 208–213. [Google Scholar] [CrossRef]
- Bower, K.S.; Woreta, F. Update on contraindications for laser-assisted in situ keratomileusis and photorefractive keratectomy. Curr. Opin. Ophthalmol. 2014, 25, 251–257. [Google Scholar] [CrossRef]
- Yesilirmak, N.; Davis, Z.; Yoo, S.H. Refractive Surgery (SMILE vs. LASIK vs. Phakic IOL). Int. Ophthalmol. Clin. 2016, 61, 1–2. Available online: www.internat-ophthalmology.com (accessed on 19 July 2021).
- Ruiz-Moreno, J.M.; Alió, J.L.; Pérez-Santonja, J.J.; de la Hoz, F. Retinal Detachment in Phakic Eyes with Anterior Chamber Intraocular Lenses to Correct Severe Myopia. Am J Ophthalmol. 1999, 127, 270–275. [Google Scholar] [CrossRef]
- Martinezcastillo, V.; Boixadera, A.; Verdugo, A.; Elies, D.; Coret, A.; Garciaarumi, J. Rhegmatogenous Retinal Detachment in Phakic Eyes After Posterior Chamber Phakic Intraocular Lens Implantation for Severe Myopia. Ophthalmology 2005, 112, 580–585.e1. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).