
Importance of In-Hospital Prospective Registry and Infectious Endocarditis Heart Team to Monitor and Improve Quality of Care in Patients with Infectious Endocarditis

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Data Collection and Statistical Methodology
3. Results
3.1. Patient Characteristics and Comparison with Previous Registries
3.2. Treatment and Clinical Outcomes
3.3. Impact of an Infective Endocarditis Heart Team and Prospective Data Collection
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Registry | CVCA | EURO-ENDO | ICE-PCS | RIEI | Fernández-Hidalgo et al. Hospital Universitari Vall d’Hebron, Spain |
|---|---|---|---|---|---|
| N hospitals | 1 | 156 | 58 | 17 | 1 |
| N countries | 1 | 40 | 25 | 1 | 1 |
| Data collection period | 2014–2019 | January 2016–March 2018 | 2000–2005 | 2007–2010 | 2000–2011 |
| Cases included | Definite IE | Possible with treatment & Definite IE | Definite IE | Definite IE | Left-sided possible and definite IE |
| Demography: | |||||
| N | 160 | 3116 | 2781 | 677 | 438 |
| Median age in years (IQR) | 72.50 (62.75 ± 80.00) | 63.0 (46.0–73.0) *** | 57.9 (43.2–71.8) *** | 65.34 (49.60–74.39) *** | 66.4 (51.8–74.9) *** |
| Age ≥ 65 years | 112/160 (70%) | 1443/3116 (46.3%) *** | |||
| Age ≥ 80 years | 44/160 (27.5%) | 375/3116 (12.0%) *** | 60/677 (8.7%) *** | ||
| Females | 40/160 (25%) | 969/3116 (31.1%) | 888/2777 (32.0%) | 185/677 (27.3%) | 153/438 (34.9%) * |
| History of cardiovascular diseases: | |||||
| Heart failure | 33/160 (20.6%) | 662/2840 (23.3%) | |||
| Congenital disease | 13/160 (8.1%) | 365/3114 (11.7%) | 311/2656 (12.0%) | 39/677 (5.8%) | |
| Ischaemic heart disease | 49/160 (30.6%) | 622/2897 (21.5%) ** | 95/677 (14.0%) *** | ||
| Peripheral arterial disease | 28/160 (17.5%) | ||||
| Previous endocarditis | 15/160 (9.4%) | 274/3116 (8.8%) | 222/2780 (8.0%) | ||
| Intra-cardiac device | 44/160 (27.6%) | 537/3116 (17.2%) ** | 122/677 (18.0%) ** | ||
| Presence of prosthetic valve | 75/160 (46.9%) | 618/2686 (23%) *** | 178/677 (26.3%) *** | ||
| Risk factors and comorbidities: | |||||
| Diabetes | 53/160 (33.1%) | 447/2764 (16.0%) *** | 116/677 (17.1%) *** | 99/438 (22.6%) * | |
| Previous stroke/TIA | 14/160 (8.8%) | 340/2860 (11.9%) | 35/677a (5.2%) | ||
| COPD/asthma | 28/160 (17.5%) | 318/3111 (10.2%) ** | 65/677 (9.6%) ** | ||
| Chronic renal failure | 44/160 (27.5%) | 553/3113 (17.8%) ** | 85/677 (12.6%) *** | ||
| Dialysis | 19/160 (11.9%) | 163/3113 (5.2%) *** | 220/2777 (8.0%) | 22/438 (5.0%) ** | |
| HIV | 2/160 (1.2%) | 31/3038 (1.0%) | 58/2748 (2.0%) | 40/677 (5.9%) * | 15/438 (3.4%) |
| Chronic liver disease | 13/160 (8.2%) | 64/677 (9.5%) | |||
| Cancer | 27/160 (16.9%) | 361/3088 (11.7%) | 230/2772 (8.0%) *** | 66/677 (9.8%) * | 56/438 (13.5%) |
| Intravenous drug dependency | 3/160 (1.9%) | 212/3067 (6.9%) * | 268/2746 (10.0%) ** | 61/677 (9.0%) ** | 12/438 (2.7%) |
| Intravenous catheter | 12/160 (7.5%) | 250/3104 (8.1%) | 244/2763 (9.0%) | 71/677 (10.5%) | |
| Invasive procedure within 60 days | 43/160 (26.9%) | 690/2581 (27.0%) | 171/677 (25.3%) |
| Registry | CVCA | EURO-ENDO | ICE-PCS | RIEI | Fernández-Hidalgo et al. Hospital Universitari Vall d’Hebron, Spain |
|---|---|---|---|---|---|
| Clinical onset and assessment: | |||||
| First sign to admission < 1 month | 141/160 (88.1%) | 2088/2711 (77.0%) | 340/677 (50.2%) *** | ||
| Transferred from other centres | 45/160 (28.1%) | 305/677 (45.0%) *** | 170/438 (38.8%) * | ||
| Fever | 95/160 (59.4%) | 2383/3068 (77.7%) *** | 2322/2428 (96.0%) *** | 568/677 (83.9%) *** | |
| Increased C-reactive protein | 159/160 (99.4%) | 1632/2650 (62.0%) *** | 566/877 (83.6%) *** | ||
| New murmur or worsening old murmur | 40/160 (25%) | 2008/3112 (64.5%) *** | 1970/2781 (70.8%) *** | 358/677 (52.9%) *** | |
| Haematuria | 69/160 (43.1%) | 666/2587 (26.0%) *** | 97/677 (14.3%) *** | ||
| Creatinine > 2 | 45/160 (28.1%) | 75/677 (11.1%) *** | |||
| Osler nodes | 1/160 (0.6%) | 60/3116 (1.9%) | 77/2648 (3.0%) | 26/677 (3.8%) | |
| Splint haemorrhage | 1/160 (0.6%) | 213/2655 (8.0%) ** | 9/677 (1.3%) | ||
| Janeway lesion | 2/160 (1.2%) | 109/3116 (3.5%) | 123/2650 (5.0%) | 6/677 (0.9%) | |
| Conjunctival haemorrhage | 2/160 (1.2%) | 122/2655 (5.0%) | 6/677 (0.9%) | ||
| Roth spots | 2/160 (1.2%) | 44/3052 (1.4%) | 50/2649 (1.89%) |
| Registry | CVCA | EURO-ENDO | ICE-PCS | RIEI | Fernández-Hidalgo et al. Hospital Universitari Vall d’Hebron, Spain |
|---|---|---|---|---|---|
| Type IE: | |||||
| Native valve | 63/160 (39.4%) | 1764/3116 (56.6%) *** | 1901/2636 (72.0%) *** | 445/677 (65.7%) *** | 337/485 (76.9%) *** |
| Prosthetic valve | 70/160 (43.8%) | 939/3116 (30.1%) *** | 563/2636 (21.0%) *** | 128/677 (18.9%) *** | 101/485 (23.1%) *** |
| Intra-cardiac device related | 27/160 (16.9%) | 308/3116 (9.9%) ** | 172/2636 (7.0%) *** | 94/677 (13.9%) | |
| Aetiology: | |||||
| Positive blood culture | 154/160 (96.3%) | 2461/3116 (79.0%) *** | 492/677 (72.7%) *** | ||
| Streptococci | 39/160 (24.4%) | 163/438 (37.2%) ** | |||
| Viridans streptococci | 17/160 (10.6%) | 304/2461 (12.4%) | 483/2781 (17.0%) * | 73/677 (14.8%) | 103/438 (23.5%) *** |
| Streptococcus bovis complex | 12/160 (7.5%) | 165/2781 (6.0%) | 57/677 (11.6%) | 33/438 (7.5%) | |
| Streptococcus agalactiae | 3/160 (1.9%) | ||||
| Pneumococcus | 5/160 (3.1%) | ||||
| Other streptococci | 1/160 (0.6%) | 162/2781 (6.0%) ** | |||
| Staphylococci | 60/160 (37.5%) | 1085/2461 (44.1%) | 143/438 (32.6%) | ||
| Staphylococcus aureus | 47/160 (29.4%) | 772/2461 (31.3%) | 869/2781 (31.0%) | 133/677 (27.0%) ** | 99/438 (22.6%) |
| Methicillin-resistant S. aureus | 0/160 (0%) | 177/2461 (7.2%) *** | 37/677 (5.4%) ** | 23/438(5.3%) ** | |
| Coagulase-negative staphylococci | 13/160 (8.1%) | 313/2461 (12.7%) | 304/2781 (11.0%) | 106/677 (21.6%) * | 44/438 (10.0%) |
| Enterococci | 37/160 (23.1%) | 390/2461 (15.8%) * | 283/2781 (10.0%) *** | 75/677 (15.1%) *** | 59/438 (13.5%) ** |
| Gram-negative rods (GNR) | 3/160 (1.9%) | 86/2461 (3.5%) | 19/438 (4.3%) | ||
| HACEK group | 1/160 (0.6%) | 44/2781 (2.0%) | 6/677 (1.2%) | 9/438 (2.1%) | |
| Fungi/yeast | 1/160 (0.6%) | 45/2781 (2.0%) | |||
| Polymicrobial | 4/160 (2.5%) | 28/2781 (1.0%) | |||
| Culture negative | 6/160 (3.8%) | 310/2781 (11.1%) ** |
| Prosthetic IE n = 70 | Native IE n = 63 | Cardiac Device Related IE n = 27 | Significance Level of p-Value | Overall n = 160 | |
|---|---|---|---|---|---|
| Median EuroSCORE (IQR) | 19.0 (11.1–27.5) | 8.6 (3.2–18.8) | 9.0 (5.2–16.3) | *** | 13.3 (6.2–24.0) |
| Median STS score (only calculated for aortic or mitral valve surgeries) | 8.6 (5.7–17.8) | 6.6 (3.8–13.5) | 6.8 (4.8–24.6) | 7.5 (4.2–15.9) | |
| Global risk score >= 2 | 49 (70.0%) | 44 (69.8%) | 21 (77.8%) | 114 (71.3%) | |
| Median Charlson comorbidity index-not age related (IQR) | 96.0 (90.2–98.3) | 90.2 (77.5–98.3) | 90.2 (53.4–95.9) | * | 90.2 (77.4–98.3) |
| Median Katz score (IQR) | 4.0 (2.0–5.0) | 3.0 (1.0–5.0) | 4.0 (2.0–5.8) | 3.0 (2.0–5.0) | |
| Median frailty score (IQR) | 4.5 (3.0–6.0) | 6.0 (4.0–7.0) | 5.0 (4.0–6.0) | 5.0 (3.0–7.0) |
| Registry | CVCA | EURO-ENDO | ICE-PCS | RIEI | Fernández-Hidalgo et al. Hospital Universitari Vall d’Hebron, Spain |
|---|---|---|---|---|---|
| Entrance site: | |||||
| Oral/dental | 16/160 (10%) | (9.8%) | |||
| Digestive | 39/160 (24.4%) | (6.3%) *** | |||
| Genitourinary | 7/160 (4.4%) | (4.5%) | |||
| Skin | 33/160 (20.6%) | ||||
| Acquisition: | |||||
| Community-acquired | 92/160 (57.5%) | 2046/3116 (65.7%) * | 1975/2781 (71.0%) *** | 425/677 (62.8%) | |
| Healthcare related | 64/160 (40%) | 1027/3116 (33.0%) | 640/2781 (23%) *** | 160/677 (23.6%) *** | 135/438 (30.8%) * |
| Nosocomial | 15/160 (9.4%) | 624/3116 (19.5%) ** | 390/2781 (14.0%) | 76/677 (11.2%) | |
| No-nosocomial healthcare related | 49/160 (30.6%) | 403/3116 (12.9%) *** | 250/2781 (9.0%) *** | 84/677 (12.4%) *** | |
| Unknown | 4/160 (2.5%) | 43/3116 (1.4%) | 167/2781 (6.0%) | 92/677 (13.6%) *** |
| Registry | CVCA | EURO-ENDO | ICE-PCS | RIEI | Fernández-Hidalgo et al. Hospital Universitari Vall d’Hebron, Spain |
|---|---|---|---|---|---|
| Clinical imaging | |||||
| Cardiac echo performed | 151/160 (94.4%) | 3111/3116 (99.8%) *** | |||
| TTE performed | 85/160 (53%) | 2793/3111 (89.8%) *** | 640/677 (94.5%) *** | ||
| TEE performed | 148/160 (92.5%) | 1808/3111 (58.1%) *** | 478/677 (70.6%) *** | ||
| TTE positive | 42/85 (49.4%) | 395/640 (62.0%) | |||
| TEE positive | 130/148 (87.8%) | 447/478 (93.5%) *** | |||
| PET CT performed | 46/160 (28.8%) | 518/3116 (16.6%) *** | |||
| Leucocyte scintigraphy | 1/160 (0.6%) | 38/3116 (1.2%) | |||
| MDCT | 5/160 (3.1%) | 1656/3116 (53.1%) *** |
| Aortic Valve | Mitral Valve | Tricuspid Valve | Pulmonal Valve | |
|---|---|---|---|---|
| Prosthetic | 56 | 22 | 3 | 0 |
| Vegetation | 66/160 (41.3%) | 55/160 (34.4%) | 14/160 (8.8%) | 1/160 (0.6%) |
| Vegetation median size in mm (IQR) | 10.0 (7.0–13.0) | 12.5 (9.0–20.0) | 16.0 (10.0–20.0) | 18 (18.0–18.0) |
| Vegetation range in mm | 2–35 | 3–50 | 6–25 | – |
| Valve regurgitation >= 3/4 | 33 | 27 | 16 | 1 |
| Leaflet perforation | 9 | 17 | 3 | 0 |
| Periannular abscess | 28 | 5 | 0 | 0 |
| Periannular pseudoaneurysm | 3 | 2 | 0 | 0 |
| Prosthetic valve dehiscence | 12 | 4 | 1 | 0 |
| Prosthetic valve obstruction | 2 | 0 | 0 | 0 |
| Registry | CVCA | EURO-ENDO | ICE-PCS | RIEI | Fernández-Hidalgo et al. Hospital Universitari Vall d’Hebron, Spain |
|---|---|---|---|---|---|
| Complications (at admission or while under treatment): | |||||
| Congestive heart failure | 69/160 (43.1%) | 1288/3116 (41.3%) | 876/2713 (32.0%) ** | 301/677 (44.5%) | 205/438 (46.8%) |
| Intracardiac abscess | 31/160 (19.4%) | 556/3116 (17.8%) | 389/2707 (14.0%) | 77/677 (11.4%) ** | |
| New conduction abnormality | 42/160 (26.2%) | 459 (16.0%) ** | 217/2695 (8.0%) *** | 84/438 (19.1%) | |
| Persistent positive blood cultures | 21/160 (13.1%) | 413/3088 (13.4%) | 251/2699 (9.0%) | ||
| Pulmonary embolism | 10/160 (5.6%) | 366/3116 (11.7%) * | |||
| Intracranial haemorrhage | 5/160 (3.1%) | 138/3116 (4.4%) | 14/677 (2.1%) | ||
| Vascular embolic event | 54/160 (33.8%) | 1429/3116 (45.8%) ** | 1067/2781 (38.6%) | 57/677 (8.4%) *** | |
| Cerebral embolism | 38/160 (23.8%) | 633/3116 (20.3%) | |||
| Stroke/TIA | 30/160 (18.8%) | 403/3116 (12.9%) * | 462/2727 (17.0%) | 89/438 (20.3%) | |
| Splenic/Renal embolism/ Spondylodiscitis | 14/160 (8.1%) | 762/3116 (24.5%) *** | |||
| Septic shock | 33/160 (20.6%) | 494/3116 (15.9%) | |||
| Valvular assessment: | |||||
| Vegetation present: | 134/160 (83.8%) | 2406/2764 (87.0%) | 605/677 (92.0%) | ||
| AV | 66/160 (41.3%) | 1031/2741 (38.0%) | |||
| MV | 55/160 (34.4%) | 1125/2740 (41.0%) | |||
| TV | 14/160 (8.8%) | 323/2741 (12.0%) | |||
| PV | 1/160 (0.6%) | 29/2739 (1.0%) | |||
| Paravalvular abscess | 31/160 (19.4%) | (15.0%) | 77/677 (11.4%) ** | ||
| Prosthetic valve complication | 57/160 (35.6%) | 518/2781 (18.2%) *** | |||
| Aortic valve affected | 77/160 (48.1%) | (49.5%) | 258/438 (58.9%) * | ||
| Mitral valve affected | 65/160 (41%) | (42.0%) | |||
| Tricuspid valve affected | 21/160 (13.1%) | (11.4%) | |||
| Pulmonal valve affected | 1/160 (0.6%) | (2.4%) | |||
| Multiple valves affected | 31/160 (19.3%) | (18.2%) | |||
| Valvular assessment: |


References
- Habib, G.; Erba, P.A.; Iung, B.; Donal, E.; Cosyns, B.; Laroche, C.; Popescu, B.A.; Prendergast, B.; Tornos, P.; Sadeghpour, A.; et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO(European infective endocarditis) registry: A prospective cohort study. Eur. Heart J. 2019, 40, 3222–3233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erbaa, P.A.; Iung, B.; et al. ESC Guidelines for the management of infective endocarditis. Eur. Heart J. 2015, 36, 3075–3123. [Google Scholar] [CrossRef]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., III; Guyton, R.A.; O’Gara, P.T.; Ruiz, C.E.; Skubas, N.J.; Sorajja, P.; et al. AHA/ACC guideline for the management of patients with valvular heart disease: Executive summary a report of the american college of cardiology/american heart association task force on practice guidelines. Circulation 2014, 129, 2440–2492. [Google Scholar] [CrossRef]
- Mostaghim, A.S.; Lo, H.Y.A.; Khardori, N. A retrospective epidemiologic study to define risk factors, microbiology, and clinical outcomes of infective endocarditis in a large tertiary-cary teaching hospital. SAGE Open Med. 2017, 5, 1–9. [Google Scholar] [CrossRef]
- Murdoch, D.R.; Corey, R.; Hoen, B.; Miro, J.M.; Fowler, V.G.; Bayer, A.S.; Karchmer, A.W.; Olaison, L.; Pappas, P.A.; Moreillon, P.; et al. Clinical presentation, etiology and outcome of infective endocarditis in the 21st century: The International Collaboration on Endocarditis-Prospective Cohort Study. Arch. Intern. Med. 2009, 169, 463–473. [Google Scholar] [CrossRef] [Green Version]
- Cahill, T.J.; Baddour, L.M.; Habib, G.; Hoen, B.; Salaun, E.; Pettersson, G.B.; Schäfers, H.J.; Prendergast, B.D. Challenges in Infective Endocarditis. J. Am. Coll. Cardiol. 2017, 69, 325–344. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Erba, P.A.; Sadeghpour, A.; Meshaal, M.; Sambola, A.; Furnaz, S.; Citro, R.; Ternacle, J.; Donal, E.; et al. The ESC-EORP EURO-ENDO (European Infective Endocarditis) registry. Eur. Heart J. 2019, 5, 202–207. [Google Scholar] [CrossRef]
- Cecchi, E.; Chirillo, F.; Castiglione, A.; Faggiano, P.; Cecconi, M.; Moreo, A.; Cialfi, A.; Rinaldi, M.; Del Ponte, S.; Squeri, A.; et al. Clinical epidemiology in Italian Registry of Infective Endocarditis (RIEI): Focus on age, intravascular devicesd and enterocci. Int. J. Cardiol. 2015, 190, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Hidalgo, N.; Almirante, B.; Tornos, P.; Gonzalez-Alujas, M.T.; Planes, A.M.; Galinanes, M.; Pahissa, A. Immediate and long-term outcome of left-sided infective endocarditis. A 12-year prospective study from contemporary cohort in a referral hospital. Clin. Microbiol. Infect. 2012, 18, E522–E530. [Google Scholar] [CrossRef] [Green Version]
- Kastner, C.; Armitage, J.; Kimble, A.; Rawal, J.; Carter, P.G.; Venn, S. The Charlson comorbidity score: A superior comorbidity assessment tool for the prostate cancer multidisciplinary meeting. Prostate Cancer Prostatic Dis. 2006, 9, 270–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, S.; Down, T.D.; Cash, H.R.; Grotz, R.C. Progress in the development of the index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. Cmaj 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slipczuk, L.; Codolosa, J.N.; Davila, C.D.; Romero-Corral, A.; Yun, J.; Pressman, G.S.; Figueredo, V.M. Infective endocarditis epidemiology over five decades: A systematic review. PLoS ONE 2013, 8, e82665. [Google Scholar] [CrossRef] [PubMed]
- DeSimone, D.C.; Tleyjeh, I.M.; Correa de Sa, D.D.; Anavekar, N.S.; Lahr, B.D.; Sohail, M.R.; Steckelberg, J.M.; Wilson, W.R.; Baddour, L.M. Temporal trends in infective endocarditis epidemiology from 2007 to 2013 in Olmsted County, MN. Am. Heart J. 2015, 170, 830–836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrosioni, J.; Hernandez-Meneses, M.; Téllez, A.; Pericàs, J.; Falces, C.; Tolosana, J.M.B.; Vidal, B.; Almela, M.; Quintana, E.; Llopis, J.; et al. The changing epidemiology of infective endocarditis in the twenty-first century. Curr. Infect. Dis. Rep. 2017, 19, 21. [Google Scholar] [CrossRef] [PubMed]
- Chambers, H.F.; Bayer, A.S. Native-Valve Infective Endocarditis. N. Engl. J. Med. 2020, 383, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.; Glaudemans, A.W.J.M.; Touw, D.J.; van Melle, J.P.; Willems, T.P.; Maass, A.H.; Natour, E.; Prakken, N.H.J.; Borra, R.J.H.; van Geel, P.P.; et al. Diagnostic value of imaging in infective endocarditis: A systematic review. Lancet Infect. Dis. 2017, 17, e1–e14. [Google Scholar] [CrossRef]
- Que, Y.A.; More, P. Infective endocarditis. Nat. Rev. Cardiol. 2011, 8, 322–336. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, E.F.; Huang, G.; Aldea, G.; Koomalsingh, K.; Klein, J.W.; Dhanireddy, S.; Harrington, R. A Multidisciplinary Pathway for the Diagnosis and Treatment of Infectious Endocarditis. Crit. Pathw. Cardiol. 2020, 19, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Chambers, J.; Sandoe, J.; Ray, S.; Prendergast, B.; Taggart, D.; Westaby, S.; Arden, C.; Grothier, L.; Wilson, J.; Campbell, B.; et al. The infective endocarditis team: Recommendations from an international working group. Heart 2014, 100, 524–527. [Google Scholar] [CrossRef] [PubMed]


| Registry | CVCA |
|---|---|
| n hospitals | 1 |
| n countries | 1 |
| Data collection period | 2014–2019 |
| Cases included | Definite IE |
| Demography: | |
| N | 160 |
| Median age in years (IQR) | 72.50 (62.75 ± 80.00) |
| Age ≥ 65 years | 112/160 (70%) |
| Age ≥ 80 years | 44/160 (27.5%) |
| Females | 40/160 (25%) |
| History of cardiovascular diseases: | |
| Heart failure | 33/160 (20.6%) |
| Congenital disease | 13/160 (8.1%) |
| Ischaemic heart disease | 49/160 (30.6%) |
| Peripheral arterial disease | 28/160 (17.5%) |
| Previous endocarditis | 15/160 (9.4%) |
| Intra-cardiac device | 44/160 (27.6%) |
| Presence of prosthetic valve | 75/160 (46.9%) |
| Risk factors and comorbidities: | |
| Diabetes | 53/160 (33.1%) |
| Previous stroke/TIA | 14/160 (8.8%) |
| COPD/asthma | 28/160 (17.5%) |
| Chronic renal failure | 44/160 (27.5%) |
| Dialysis | 19/160 (11.9%) |
| HIV | 2/160 (1.2%) |
| Chronic liver disease | 13/160 (8.2%) |
| Cancer | 27/160 (16.9%) |
| Intravenous drug dependency | 3/160 (1.9%) |
| Intravenous catheter | 12/160 (7.5%) |
| Invasive procedure within 60 days | 43/160 (26.9%) |
| Registry | CVCA | EURO-ENDO | ICE-PCS | RIEI | Fernández-Hidalgo et al. Hospital Universitari Vall d’Hebron, Spain |
|---|---|---|---|---|---|
| Treatment type: | |||||
| Indication for surgery | 110/160 (68.8%) | 2160/3115 (69.3%) | 318/438 (72.6%) | ||
| Surgery performed | 82/160 (51.3%) | 1596/3116 (51.2%) | 1335/2769 (48.0%) | 422/677 (62.3%) * | 174/438 (39.7%) * |
| Type of surgery performed: | |||||
| Mechanical prosthesis | 5/81 (3.1%) | 560/1596 (35.1%) *** | 135/438 (30.8%) *** | ||
| Bioprosthesis | 61/81 (75.3%) | 817/1596 (51.2%) *** | 36/438 (8.2%) *** | ||
| Repair | 9/81 (11.1%) | 311/1596 (19.5%) | 3/438 (0.6%) *** | ||
| Surgery indicated but not performed | 28/160 (17.5%) | 564/3115 (18.1%) | 144/438 (32.8%) *** | ||
| Medical treatment (surgery not indicated) | 50/160 (31.3%) | 955/3115 (30.6%) | 161/438 (36.8%) |
| Registry | OLV Hospital | EURO-ENDO | ICE-PCS | RIEI | Fernández-Hidalgo et al. Hospital Universitari Vall d’Hebron, Spain |
|---|---|---|---|---|---|
| Risk assessments: | |||||
| Median EuroSCORE | 13.3 (6.2–24.0) | 5.0 (2.0–13.3) *** | |||
| Median EuroSCORE when surgery performed (IQR) | 12.5 (6.2–22.3) | 9 (9–12) *** | |||
| Median EuroSCORE when surgery indicated but not performed (IQR) | 17.8 (9.5–26.7) | 11 (8–13) ** | |||
| Subjects with definite Modified Duke criteria | 160 | 2610/3116 (83.8%) *** | 386/438 (88.1%) *** | ||
| Median EuroSCORE prosthetic IE (IQR) | 19.0 (11.1–27.5) | 10.9 (5.2–24.9) *** | |||
| Median EuroSCORE native IE (IQR) | 8.6 (3.2–18.8) | 3.0 (1.5–8.0) *** | |||
| Median EuroSCORE device-related IE (IQR) | 9.0 (5.2–16.3) | 6.0 (2.2–15.0) ** | |||
| Mortality: | |||||
| In-hospital mortality | 46/160 (28.7%) | 532/3116 (17.1%) *** | 490/2774 (18.0%) *** | 93/677 (13.7%) *** | 125/677 (28.5%) |
| In-hospital mortality prosthetic IE | 18/70 (25.7%) | 187/939 (19.9%) | |||
| In-hospital mortality native IE | 19/63 (30.2%) | 286/1764 (16.2%) ** | |||
| In-hospital mortality device-related IE | 9/27 (30%) | 47/308 (15.3%) * | |||
| Cumulative 1-month mortality | 31/160 (19.4%) | ||||
| Cumulative 3-month mortality | 49/160 (30.6%) | (13.8%) *** | |||
| Cumulative 6-months mortality | 55/160 (34.4%) | (15.5%) *** | |||
| Cumulative 1-year mortality | 60/160 (37.5%) | (16.7%) *** | 150/397 (37.8%) |
| IEHT Approach | Standard Care | p Value | |
|---|---|---|---|
| Baseline characteristics | |||
| Age | 6/69.5 (sd: 13.3) | 71.0 (sd: 11.8) | 0.4710 |
| Gender (male) | 66/92 (71.7%) | 54/68 (79.4%) | 0.3558 |
| Diabetes | 33/92 (35.9%) | 20/68 (29.4%) | 0.4914 |
| COPD | 16/92 (17.6%) | 12/68 (17.4%) | 0.9999 |
| GFR | 52.1 (sd: 28.7) | 54.1 (sd: 25.7) | 0.6393 |
| Previous cardiac surgery | 44/92 (47.8%) | 36/68 (52.9%) | 0.6314 |
| Previous coronary artery disease | 25/92 (27.2%) | 24/68 (35.3%) | 0.3534 |
| Stroke | 8/92 (8.7%) | 6/68 (8.8%) | 0.9999 |
| Peripheral arterial disease | 13/92 (14.1%) | 15/68 (22.1%) | 0.2738 |
| LVEF < 50% | 23/92 (25.0%) | 10/68 (14.7%) | 0.1835 |
| Degenerative Valve Disease | 54/92 (58.7%) | 35/68 (51.5%) | 0.4542 |
| Previous endocarditis | 9/92 (9.8%) | 6/68 (8.8%) | 0.9999 |
| Cancer | 14/92 (19.1%) | 13/68 (15.2%) | 0.6616 |
| Aetiology | |||
| Streptococcus viridans | 8/92 (8.7%) | 9/68 (13.2%) | 0.5082 |
| Staphylococcus aureus | 27/92 (29.4%) | 20/68 (29.3%) | 0.9999 |
| Enterococcus | 18/92 (19.6%) | 19/68 (27.9%) | 0.2925 |
| Risk Assessment | |||
| Charlson index (not age related) | 82.7 (sd: 21.4) | 81.1 (sd: 27.3) | 0.6745 |
| Frailty score | 5.6 (sd: 1.8) | 3.8 (sd: 2.5) | 0.0001 |
| Euroscore II | 16.7 (sd: 12.6) | 17.4 (sd: 16.7) | 0.7535 |
| KATZ score | 3.2 (sd: 2.1) | 3.4 (sd: 2.3) | 0.6216 |
| Global Risk score | 1.8 (sd: 0.8) | 2.1 (sd: 0.9) | 0.0879 |
| IE Type: | |||
| Prosthetic | 38/92 (41.3%) | 32/68 (47.1%) | 0.1610 |
| Native | 34/92 (37.0%) | 29/68 (42.6%) | |
| Device-related | 20/92 (21.7%) | 7/68 (10.3%) |
| IEHT Approach | Standard Care | p Value | |
|---|---|---|---|
| Unadjusted mortality | |||
| In-hospital mortality | 28.3% | 29.4% | 0.8737 |
| 30 days mortality | 20.7% | 20.7% | 0.8104 |
| 180 days mortality | 32.6% | 36.8% | 0.5843 |
| 1 year mortality | 34.8% | 41.2% | 0.4089 |
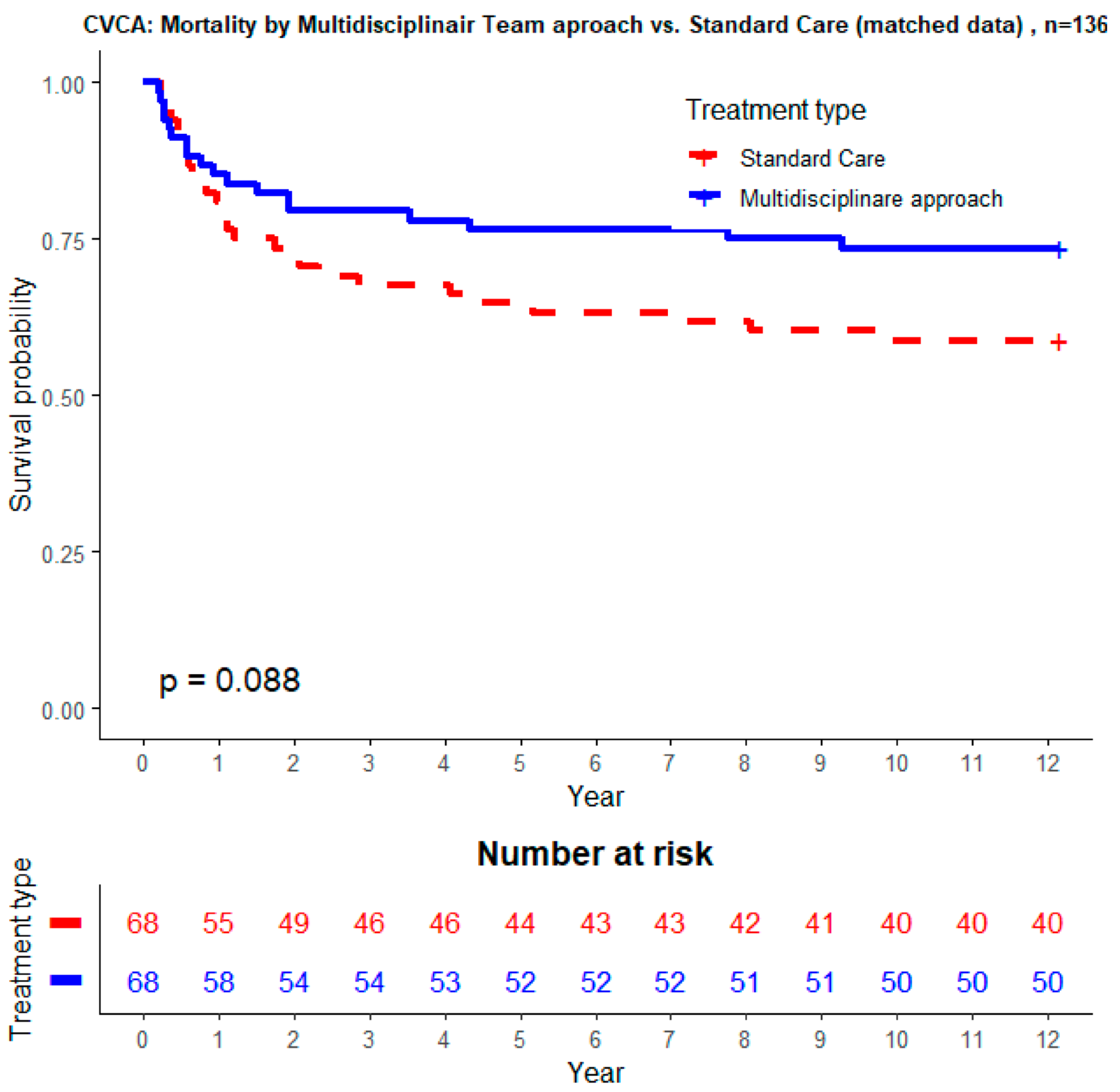
| After propensity score matching | |||
| In-hospital mortality | 17.7% | 29.4% | 0.1058 |
| 30 days mortality | 14.7% | 19.1% | 0.4926 |
| 180 days mortality | 23.5% | 36.8% | 0.0926 |
| 1 year mortality | 26.5% | 41.2% | 0.0699 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Camp, G.; Beles, M.; Penicka, M.; Schelfaut, D.; Wouters, S.; De Raedt, H.; Wyffels, E.; Spapen, J.; Nasser, R.; Balogh, Z.; et al. Importance of In-Hospital Prospective Registry and Infectious Endocarditis Heart Team to Monitor and Improve Quality of Care in Patients with Infectious Endocarditis. J. Clin. Med. 2021, 10, 3832. https://doi.org/10.3390/jcm10173832
Van Camp G, Beles M, Penicka M, Schelfaut D, Wouters S, De Raedt H, Wyffels E, Spapen J, Nasser R, Balogh Z, et al. Importance of In-Hospital Prospective Registry and Infectious Endocarditis Heart Team to Monitor and Improve Quality of Care in Patients with Infectious Endocarditis. Journal of Clinical Medicine. 2021; 10(17):3832. https://doi.org/10.3390/jcm10173832
Chicago/Turabian StyleVan Camp, Guy, Monika Beles, Martin Penicka, Dan Schelfaut, Stijn Wouters, Herbert De Raedt, Eric Wyffels, Jerrold Spapen, Riwa Nasser, Zsuzsanna Balogh, and et al. 2021. "Importance of In-Hospital Prospective Registry and Infectious Endocarditis Heart Team to Monitor and Improve Quality of Care in Patients with Infectious Endocarditis" Journal of Clinical Medicine 10, no. 17: 3832. https://doi.org/10.3390/jcm10173832