
Early Microvascular and Oscillatory Potentials Changes in Human Diabetic Retina: Amacrine Cells and the Intraretinal Neurovascular Crosstalk


 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Imaging
2.2. Oscillatory Potentials
2.3. Statistical Analysis
3. Results
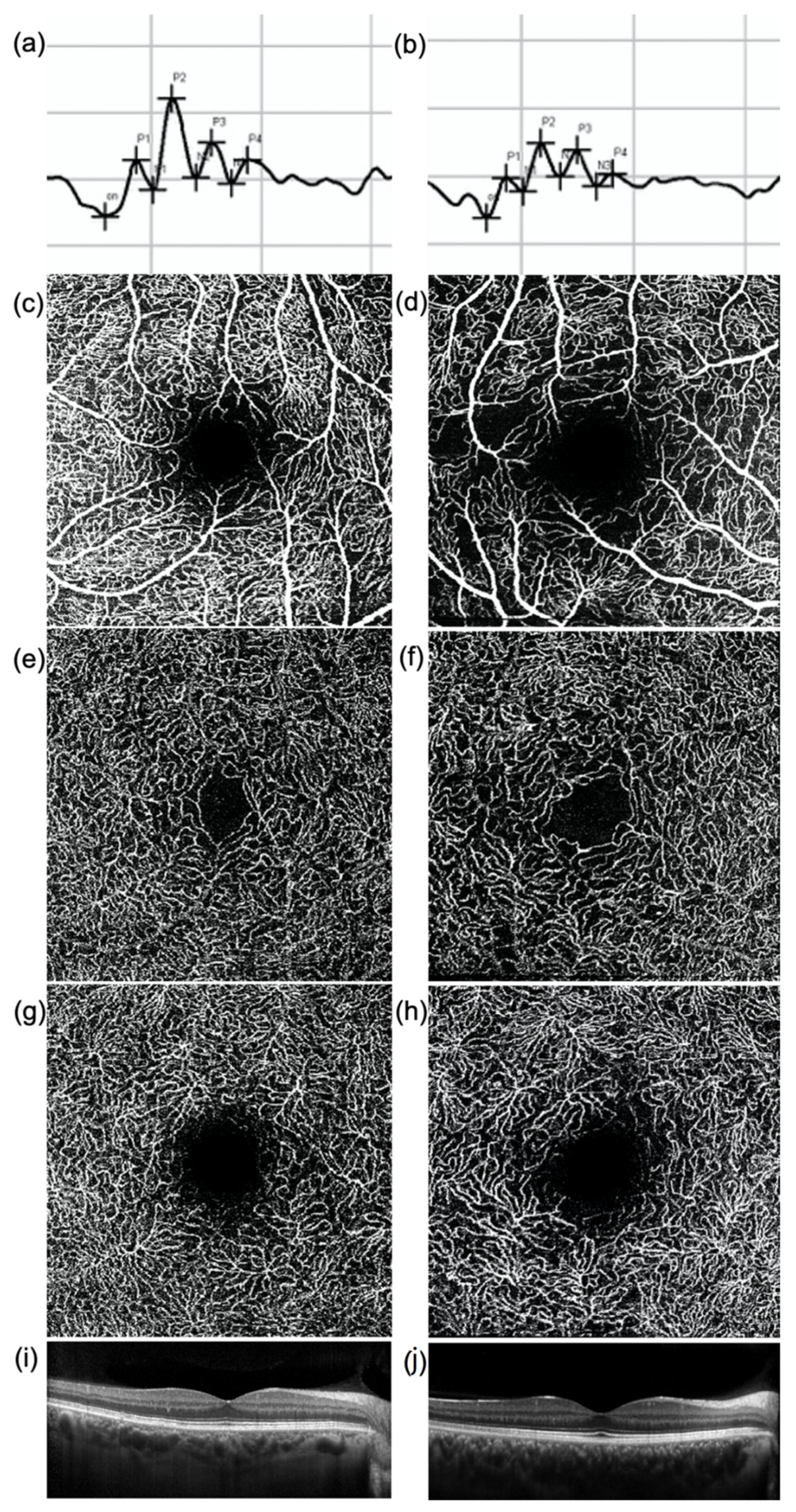
3.1. OCT and OCTA Parameters
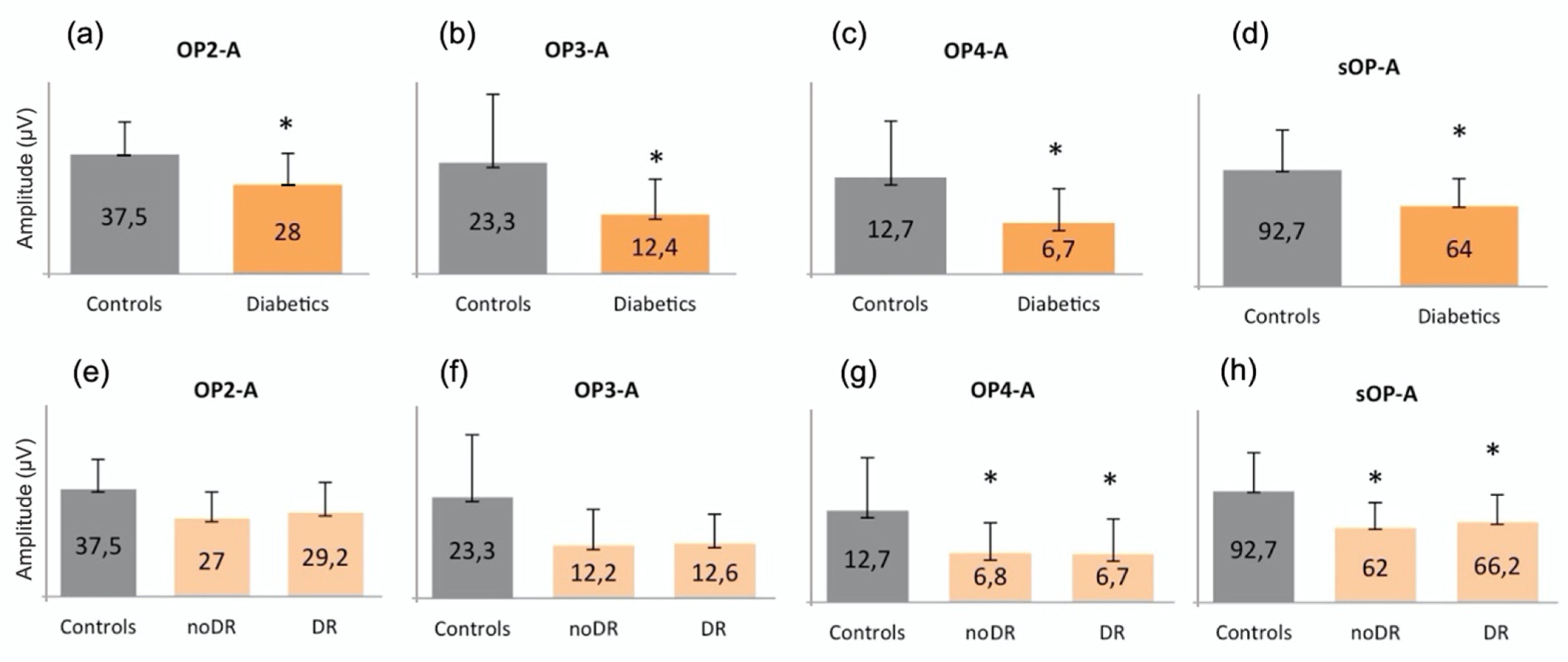
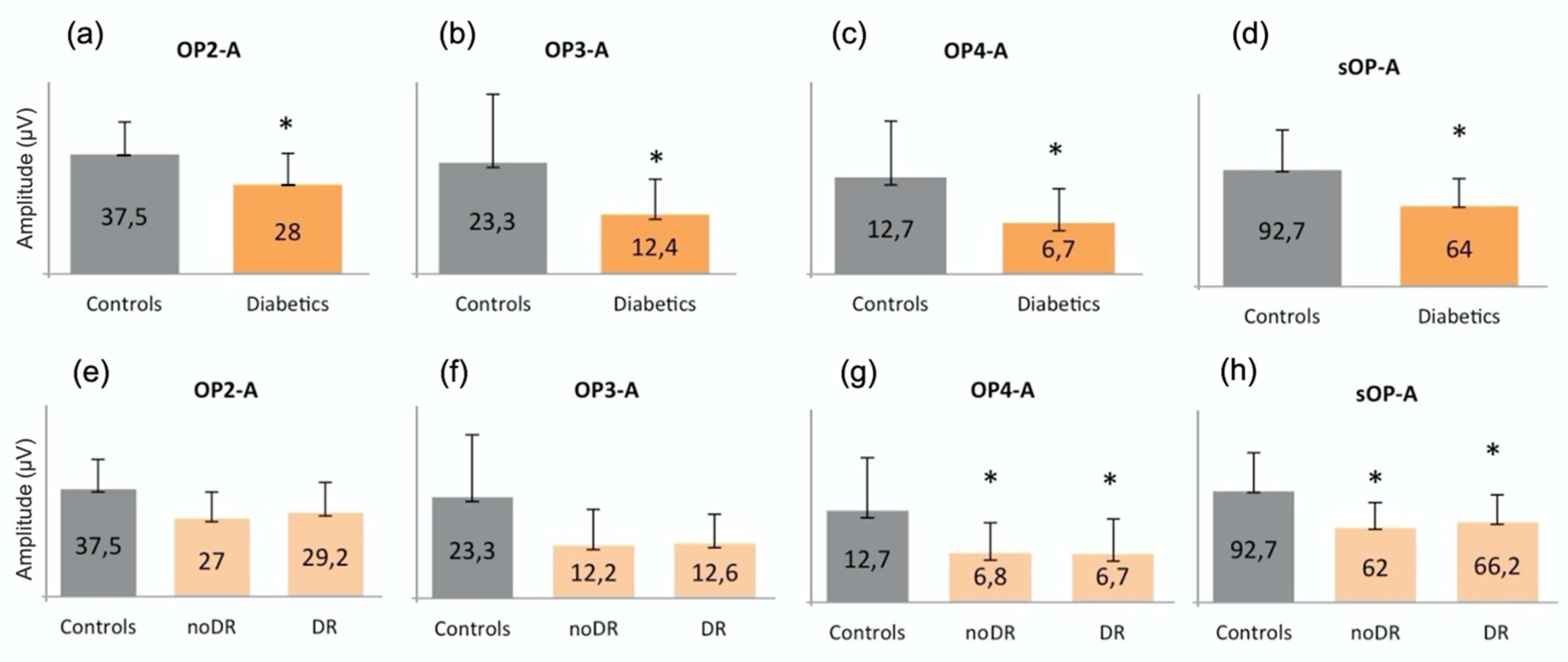
3.2. Oscillatory Potentials
3.3. Correlations between Vascular Parameters and Oscillatory Potentials in Diabetics
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Teo, Z.L.; Tham, Y.C.; Yu, M.; Chee, M.L.; Rim, T.H.; Cheung, N.; Bikbov, M.M.; Wang, Y.X.; Tang, Y.; Lu, Y.; et al. Global Prevalence of Diabetic Retinopathy and Projection of Burden through 2045: Systematic Review and Meta-analysis. Ophthalmology 2021. [Google Scholar] [CrossRef] [PubMed]
- Antonetti, D.A.; Barber, A.J.; Khin, S.; Lieth, E.; Tarbell, J.M.; Gardner, T.W. Vascular permeability in experimental diabetes is associated with reduced endothelial occludin content: Vascular endothelial growth factor decreases occludin in retinal endothelial cells. Penn State Retina Research Group. Diabetes 1998, 47, 1953–1959. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Park, J.W.; Park, S.J.; Kim, K.Y.; Chung, J.W.; Chun, M.H.; Oh, S.J. Apoptotic death of photoreceptors in the streptozotocin-induced diabetic rat retina. Diabetologia 2003, 46, 1260–1268. [Google Scholar] [CrossRef] [PubMed]
- Midena, E.; Pilotto, E. Emerging Insights into Pathogenesis. Dev. Ophthalmol. 2017, 60, 16–27. [Google Scholar] [PubMed]
- Usui, Y.; Westenskow, P.D.; Kurihara, T.; Aguilar, E.; Sakimoto, S.; Paris, L.P.; Wittgrove, C.; Feitelberg, D.; Friedlander, M.S.; Moreno, S.K.; et al. Neurovascular crosstalk between interneurons and capillaries is required for vision. J. Clin. Investig. 2015, 125, 2335–2346. [Google Scholar] [CrossRef] [Green Version]
- Lecleire-Collet, A.; Audo, I.; Aout, M.; Girmens, J.F.; Sofroni, R.; Erginay, A.; Le Gargasson, J.F.; Mohand-Saïd, S.; Meas, T.; Guillausseau, P.J.; et al. Evaluation of retinal function and flicker light-induced retinal vascular response in normotensive patients with diabetes without retinopathy. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2861–2867. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.P.; Zhang, M.; Hwang, T.S.; Bailey, S.T.; Wilson, D.J.; Jia, Y.; Huang, D. Detailed Vascular Anatomy of the Human Retina by Projection-Resolved Optical Coherence Tomography Angiography. Sci. Rep. 2017, 7, 42201. [Google Scholar] [CrossRef] [Green Version]
- Chan, G.; Balaratnasingam, C.; Xu, J.; Mammo, Z.; Han, S.; Mackenzie, P.; Merkur, A.; Kirker, A.; Albiani, D.; Sarunic, M.V.; et al. In vivo optical imaging of human retinal capillary networks using speckle variance optical coherence tomography with quantitative clinico-histological correlation. Microvasc. Res. 2015, 100, 32–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Carlo, T.E.; Chin, A.T.; Bonini Filho, M.A.; Adhi, M.; Branchini, L.; Salz, D.A.; Baumal, C.R.; Crawford, C.; Reichel, E.; Witkin, A.J.; et al. Detection Of Microvascular Changes In Eyes Of Patients With Diabetes But Not Clinical Diabetic Retinopathy Using Optical Coherence Tomography Angiography. Retina 2015, 35, 2364–2370. [Google Scholar] [CrossRef]
- Vadalà, M.; Anastasi, M.; Lodato, G.; Cillino, S. Electroretinographic oscillatory potentials in insulin-dependent diabetes patients: A long-term follow-up. Acta Ophthalmol. Scand. 2002, 80, 305–309. [Google Scholar] [CrossRef]
- Wachtmeister, L. Oscillatory potentials in the retina: What do they reveal. Prog. Retin. Eye Res. 1998, 17, 485–521. [Google Scholar] [CrossRef]
- Van der Torren, K.; Mulder, P. Comparison of the second and third oscillatory potentials with oscillatory potential power in early diabetic retinopathy. Doc. Ophthalmol. 1993, 83, 111–118. [Google Scholar] [CrossRef]
- Lovasik, J.V.; Kergoat, H. Electroretinographic results and ocular vascular perfusion in type 1 diabetes. Investig. Ophthalmol. Vis. Sci. 1993, 34, 1731–1743. [Google Scholar]
- Frizziero, L.; Midena, G.; Longhin, E.; Berton, M.; Torresin, T.; Parrozzani, R.; Pilotto, E. Early Retinal Changes by OCT Angiography and Multifocal Electroretinography in Diabetes. J. Clin. Med. 2020, 9, 3514. [Google Scholar] [CrossRef] [PubMed]
- Luu, C.D.; Szental, J.A.; Lee, S.Y.; Lavanya, R.; Wong, T.Y. Correlation between retinal oscillatory potentials and retinal vascular caliber in type 2 diabetes. Investig. Ophthalmol. Vis. Sci. 2010, 51, 482–486. [Google Scholar] [CrossRef] [Green Version]
- Coupland, S.G. A comparison of oscillatory potential and pattern electroretinogram measures in diabetic retinopathy. Doc. Ophthalmol. 1987, 66, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Early Treatment Diabetic Retinopathy Study Research Group. Grading diabetic retinopathy from stereoscopic color fundus photographs—An extension of the modified Airlie House classification. ETDRS report number 10. Ophthalmology 1991, 98, 786–806. [Google Scholar] [CrossRef]
- Hood, D.C.; Bach, M.; Brigell, M.; Keating, D.; Kondo, M.; Lyons, J.S.; Marmor, M.F.; McCulloch, D.L.; Palmowski-Wolfe, A.M.; International Society For Clinical Electrophysiology of Vision. ISCEV standard for clinical multifocal electroretinography (mfERG) (2011 edition). Doc. Ophthalmol. 2012, 124, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Vujosevic, S.; Midena, E. Retinal layers changes in human preclinical and early clinical diabetic retinopathy support early retinal neuronal and Müller cells alterations. J. Diabetes Res. 2013, 2013, 905058. [Google Scholar] [CrossRef] [PubMed]
- Shinoda, K.; Rejdak, R.; Schuettauf, F.; Blatsios, G.; Völker, M.; Tanimoto, N.; Olcay, T.; Gekeler, F.; Lehaci, C.; Naskar, R.; et al. Early electroretinographic features of streptozotocin-induced diabetic retinopathy. Clin. Exp. Ophthalmol. 2007, 35, 847–854. [Google Scholar] [CrossRef]
- Li, X.; Sun, X.; Hu, Y.; Huang, J.; Zhang, H. Electroretinographic oscillatory potentials in diabetic retinopathy. An analysis in the domains of time and frequency. Doc. Ophthalmol. 1992, 81, 173–179. [Google Scholar] [CrossRef]
- Van Dijk, H.W.; Verbraak, F.D.; Kok, P.H.; Stehouwer, M.; Garvin, M.K.; Sonka, M.; DeVries, J.H.; Schlingemann, R.O.; Abràmoff, M.D. Early neurodegeneration in the retina of type 2 diabetic patients. Investig. Ophthalmol. Vis. Sci. 2012, 53, 2715–2719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolb, H. Roles of Amacrine Cells. 1 May 2005 [Updated 30 April 2007]. In Webvision: The Organization of the Retina and Visual System; Kolb, H., Fernandez, E., Nelson, R., Eds.; University of Utah Health Sciences Center: Salt Lake City, UT, USA, 1995. Available online: https://www.ncbi.nlm.nih.gov/books/NBK11539/ (accessed on 24 June 2021).
- Leung, C.K.; Weinreb, R.N.; Li, Z.W.; Liu, S.; Lindsey, J.D.; Choi, N.; Liu, L.; Cheung, C.Y.; Ye, C.; Qiu, K.; et al. Long-term in vivo imaging and measurement of dendritic shrinkage of retinal ganglion cells. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1539–1547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beltrán-Matas, P.; Hartveit, E.; Veruki, M.L. Different glutamate sources and endogenous co-agonists activate extrasynaptic NMDA receptors on amacrine cells of the rod pathway microcircuit. Eur. J. Neurosci. 2021, 54, 4456–4474. [Google Scholar] [CrossRef] [PubMed]
- Castilho, Á.; Ambrósio, A.F.; Hartveit, E.; Veruki, M.L. Disruption of a neural microcircuit in the rod pathway of the mammalian retina by diabetes mellitus. J. Neurosci. 2015, 35, 5422–5433. [Google Scholar] [CrossRef] [PubMed]
- Castilho, Á.; Madsen, E.; Ambrósio, A.F.; Veruki, M.L.; Hartveit, E. Diabetic hyperglycemia reduces Ca2+ permeability of extrasynaptic AMPA receptors in AII amacrine cells. J. Neurophysiol. 2015, 114, 1545–1553. [Google Scholar] [CrossRef]
- Gastinger, M.J.; Singh, R.S.; Barber, A.J. Loss of cholinergic and dopaminergic amacrine cells in streptozotocin-diabetic rat and Ins2Akita-diabetic mouse retinas. Investig. Ophthalmol. Vis. Sci. 2006, 47, 3143–3150. [Google Scholar] [CrossRef] [Green Version]
- Ma, M.; Xu, Y.; Xiong, S.; Zhang, J.; Gu, Q.; Ke, B.; Xu, X. Involvement of ciliary neurotrophic factor in early diabetic retinal neuropathy in streptozotocin-induced diabetic rats. Eye 2018, 32, 1463–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hombrebueno, J.R.; Chen, M.; Penalva, R.G.; Xu, H. Loss of synaptic connectivity, particularly in second order neurons is a key feature of diabetic retinal neuropathy in the Ins2Akita mouse. PLoS ONE 2014, 9, e97970. [Google Scholar] [CrossRef] [PubMed]
- Ebihara, S.; Machida, S.; Hara, Y.; Tada, A.; Ishizuka, M.; Gonmori, M.; Nishimura, T. Relationships between the vascular structure and neural function of the macula in patients with diabetes mellitus. Jpn. J. Ophthalmol. 2021, 65, 77–88. [Google Scholar] [CrossRef]
- Rogers, S.L.; Tikellis, G.; Cheung, N.; Tapp, R.; Shaw, J.; Zimmet, P.Z.; Mitchell, P.; Wang, J.J.; Wong, T.Y. Retinal arteriolar caliber predicts incident retinopathy: The Australian Diabetes, Obesity and Lifestyle (AusDiab) study. Diabetes Care 2008, 31, 761–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bresnick, G.H.; Palta, M. Predicting progression to severe proliferative diabetic retinopathy. Arch. Ophthalmol. 1987, 105, 810–814. [Google Scholar] [CrossRef] [PubMed]
- Simonsen, S.E. Prognostic value of ERG (oscillatory potential) in juvenile diabetics. Acta Ophthalmol. Suppl. 1974, 123, 223–224. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
| Control Group (9 Subjects) | Diabetic Group (22 Subjects) | |
|---|---|---|
| Number of eyes | 18 | 44 |
| Mean age ± SD (years) | 50.8 ± 12.9 | 50.5 ± 14.1 |
| Sex (M:F) | 4:5 | 12:10 |
| Mean duration of DM ± SD (years) | - | 15.2 ± 8.5 |
| Type of DM (DM1:DM2) | - | 7:15 |
| Mean Intraocular tension ± SD (mmHg) | 15.8 ± 1.3 | 16.8 ± 2 |
| Mean refractive error ± SD (diopters) | −0.15 ± 1.31 | −0.13 ± 1.02 |
| Mean Visual acuity ± SD (ETDRS score) | 85 ± 0 | 85 ± 0 |
| SVP | ICP | DCP | |
|---|---|---|---|
| IT-OP1 | |||
| VAD | b = 0.004; p = 0.650 | b = 0.004; p = 0.539 | b = −0.016; p = 0.077 |
| VLF | b = 0.001; p = 0.954 | b = 0.001; p = 0.894 | b = −0.004; p = 0.042 |
| VDI | b = 0.039; p = 0.558 | b = 0.049; p = 0.043 | b = 0.005; p = 0.846 |
| FD | b = −0.003; p = 0.632 | b = 0.001; p = 0.967 | b = −0.0197; p = 0.030 |
| IT-OP2 | |||
| VAD | b = −0.003; p = 0.618 | b = 0.001; p = 0.718 | b = −0.008; p = 0.154 |
| VLF | b = −0.001; p = 0.205 | b = −0.001; p = 0.781 | b = −0.002; p = 0.058 |
| VDI | b = 0.040; p = 0.319 | b = 0.034; p = 0.019 | b = 0.016; p = 0.288 |
| FD | b = −0.007; p = 0.080 | b = −0.002; p = 0.659 | b = −0.011; p = 0.039 |
| IT-OP3 | |||
| VAD | b = −0.003; p = 0.448 | b = 0.001; p = 0.891 | b = −0.004; p = 0.361 |
| VLF | b = −0.001; p = 0.211 | b = −0.001; p = 0.737 | b = −0.001; p = 0.204 |
| VDI | b = 0.017; p = 0.593 | b = 0.019; p = 0.105 | b = 0.011; p = 0.355 |
| FD | b = −0.005; p = 0.103 | b = −0.002; p = 0.636 | b = −0.006; p = 0.166 |
| IT-OP4 | |||
| VAD | b = −0.001; p = 0.657 | b = −0.002; p = 0.172 | b = −0.004; p = 0.023 |
| VLF | b = −0.001; p = 0.572 | b = −0.001; p = 0.106 | b = −0.001; p = 0.009 |
| VDI | b = 0.001; p = 0.943 | b = 0.001; p = 0.858 | b = 0.001; p = 0.961 |
| FD | b = −0.001; p = 0.411 | b = −0.002; p = 0.092 | b = −0.005; p = 0.003 |
| A-OP1 | |||
| VAD | b = 0.002; p = 0.095 | b = −0.001; p = 0.470 | b = 0.001; p = 0.212 |
| VLF | b = 0.001; p = 0.002 | b = −0.001; p = 0.710 | b = 0.001; p = 0.105 |
| VDI | b = −0.011; p = 0.142 | b = −0.004; p = 0.160 | b = −0.002; p = 0.454 |
| FD | b = 0.002; p = 0.001 | b = −0.001; p = 0.771 | b = 0.002; p = 0.082 |
| A-OP2 | |||
| VAD | b = 0.001; p = 0.267 | b = 0.001; p = 0.884 | b = 0.001; p = 0.517 |
| VLF | b = 0.001; p = 0.033 | b = 0.001; p = 0.680 | b = 0.001; p = 0.288 |
| VDI | b = −0.006; p = 0.250 | b = −0.002; p = 0.454 | b = −0.003; p = 0.175 |
| FD | b = 0.001; p = 0.019 | b = 0.001; p = 0.567 | b = 0.001; p = 0.162 |
| A-OP3 | |||
| VAD | b = 0.002; p = 0.086 | b = −0.001; p = 0.364 | b = −0.001; p = 0.643 |
| VLF | b = 0.001; p = 0.002 | b = −0.001; p = 0.793 | b = 0.001; p = 0.910 |
| VDI | b = −0.011; p = 0.130 | b = −0.007; p = 0.013 | b = −0.008; p = 0.005 |
| FD | b = 0.002; p = 0.001 | b = −0.001; p = 0.923 | b = 0.001; p = 0.837 |
| A-OP4 | |||
| VAD | b = 0.001; p = 0.610 | b = −0.002; p = 0.050 | b = −0.001; p = 0.362 |
| VLF | b = 0.001; p = 0.203 | b = −0.001; p = 0.155 | b = −0.001; p = 0.681 |
| VDI | b = −0.011; p = 0.313 | b = −0.010; p = 0.009 | b = −0.012; p = 0.008 |
| FD | b = 0.002; p = 0.185 | b = −0.001; p = 0.190 | b = −0.001; p = 0.775 |
| A-OP | |||
| VAD | b = 0.001; p = 0.125 | b = −0.001; p = 0.435 | b = 0.001; p = 0.756 |
| VLF | b = 0.001; p = 0.003 | b = −0.001; p = 0.775 | b = 0.001; p = 0.397 |
| VDI | b = −0.003; p = 0.123 | b = −0.002; p = 0.055 | b = −0.002; p = 0.037 |
| FD | b = 0.001; p = 0.002 | b = −0.001; p = 0.898 | b = 0.001; p = 0.285 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Midena, E.; Torresin, T.; Longhin, E.; Midena, G.; Pilotto, E.; Frizziero, L. Early Microvascular and Oscillatory Potentials Changes in Human Diabetic Retina: Amacrine Cells and the Intraretinal Neurovascular Crosstalk. J. Clin. Med. 2021, 10, 4035. https://doi.org/10.3390/jcm10184035
Midena E, Torresin T, Longhin E, Midena G, Pilotto E, Frizziero L. Early Microvascular and Oscillatory Potentials Changes in Human Diabetic Retina: Amacrine Cells and the Intraretinal Neurovascular Crosstalk. Journal of Clinical Medicine. 2021; 10(18):4035. https://doi.org/10.3390/jcm10184035
Chicago/Turabian StyleMidena, Edoardo, Tommaso Torresin, Evelyn Longhin, Giulia Midena, Elisabetta Pilotto, and Luisa Frizziero. 2021. "Early Microvascular and Oscillatory Potentials Changes in Human Diabetic Retina: Amacrine Cells and the Intraretinal Neurovascular Crosstalk" Journal of Clinical Medicine 10, no. 18: 4035. https://doi.org/10.3390/jcm10184035
APA StyleMidena, E., Torresin, T., Longhin, E., Midena, G., Pilotto, E., & Frizziero, L. (2021). Early Microvascular and Oscillatory Potentials Changes in Human Diabetic Retina: Amacrine Cells and the Intraretinal Neurovascular Crosstalk. Journal of Clinical Medicine, 10(18), 4035. https://doi.org/10.3390/jcm10184035