
Antibody Response after BNT162b2 Vaccination in Healthcare Workers Previously Exposed and Not Exposed to SARS-CoV-2


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 MRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, F.; Buonfrate, D.; Moro, L.; Rodari, P.; Piubelli, C.; Caldrer, S.; Riccetti, S.; Sinigaglia, A.; Barzon, L. Antibody Response to the BNT162b2 MRNA COVID-19 Vaccine in Subjects with Prior SARS-CoV-2 Infection. Viruses 2021, 13, 422. [Google Scholar] [CrossRef] [PubMed]
- Shieh, G.; Jan, S.; Randles, R.H. On Power and Sample Size Determinations for the Wilcoxon–Mann–Whitney Test. J. Nonparametr. Stat. 2006, 18, 33–43. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Mazzoni, A.; Di Lauria, N.; Maggi, L.; Salvati, L.; Vanni, A.; Capone, M.; Lamacchia, G.; Mantengoli, E.; Spinicci, M.; Zammarchi, L.; et al. First-Dose MRNA Vaccination Is Sufficient to Reactivate Immunological Memory to SARS-CoV-2 in Subjects Who Have Recovered from COVID-19. J. Clin. Investig. 2021, 131, e149150. [Google Scholar] [CrossRef] [PubMed]
- Levi, R.; Azzolini, E.; Pozzi, C.; Ubaldi, L.; Lagioia, M.; Mantovani, A.; Rescigno, M. One Dose of SARS-CoV-2 Vaccine Exponentially Increases Antibodies in Individuals Who Have Recovered from Symptomatic COVID-19. J. Clin. Investig. 2021, 131, e149154. [Google Scholar] [CrossRef] [PubMed]
- Krammer, F.; Srivastava, K.; Alshammary, H.; Amoako, A.A.; Awawda, M.H.; Beach, K.F.; Bermúdez-González, M.C.; Bielak, D.A.; Carreño, J.M.; Chernet, R.L.; et al. Antibody Responses in Seropositive Persons after a Single Dose of SARS-CoV-2 MRNA Vaccine. N. Engl. J. Med. 2021, 384, 1372–1374. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.S.; Cox, M.A.; Zajac, A.J. T-Cell Exhaustion: Characteristics, Causes and Conversion: T-Cell Exhaustion. Immunology 2010, 129, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.-X.; Tang, X.-J.; Shi, Q.-L.; Li, Q.; Deng, H.-J.; Yuan, J.; Hu, J.-L.; Xu, W.; Zhang, Y.; Lv, F.-J.; et al. Clinical and Immunological Assessment of Asymptomatic SARS-CoV-2 Infections. Nat. Med. 2020, 26, 1200–1204. [Google Scholar] [CrossRef] [PubMed]
- Mazzoni, A.; Maggi, L.; Capone, M.; Spinicci, M.; Salvati, L.; Colao, M.G.; Vanni, A.; Kiros, S.T.; Mencarini, J.; Zammarchi, L.; et al. Cell-mediated and Humoral Adaptive Immune Responses to SARS-CoV-2 Are Lower in Asymptomatic than Symptomatic COVID-19 Patients. Eur. J. Immunol. 2020, 50, 2013–2024. [Google Scholar] [CrossRef] [PubMed]
- Pormohammad, A.; Zarei, M.; Ghorbani, S.; Mohammadi, M.; Razizadeh, M.H.; Turner, D.L.; Turner, R.J. Efficacy and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Vaccines 2021, 9, 467. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Frenck, R.W.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine Side-Effects and SARS-CoV-2 Infection after Vaccination in Users of the COVID Symptom Study App in the UK: A Prospective Observational Study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- Cabanillas, B.; Novak, N. Allergy to COVID-19 Vaccines: A Current Update. Allergol. Int. 2021, 70, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Al-Maqbali, J.S.; Al Rasbi, S.; Kashoub, M.S.; Al Hinaai, A.M.; Farhan, H.; Al Rawahi, B.; Al Alawi, A.M. A 59-Year-Old Woman with Extensive Deep Vein Thrombosis and Pulmonary Thromboembolism 7 Days Following a First Dose of the Pfizer-BioNTech BNT162b2 MRNA COVID-19 Vaccine. Am. J. Case Rep. 2021, 22, e932946. [Google Scholar] [CrossRef] [PubMed]
- Cines, D.B.; Bussel, J.B. SARS-CoV-2 Vaccine–Induced Immune Thrombotic Thrombocytopenia. N. Engl. J. Med. 2021, 384, 2254–2256. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
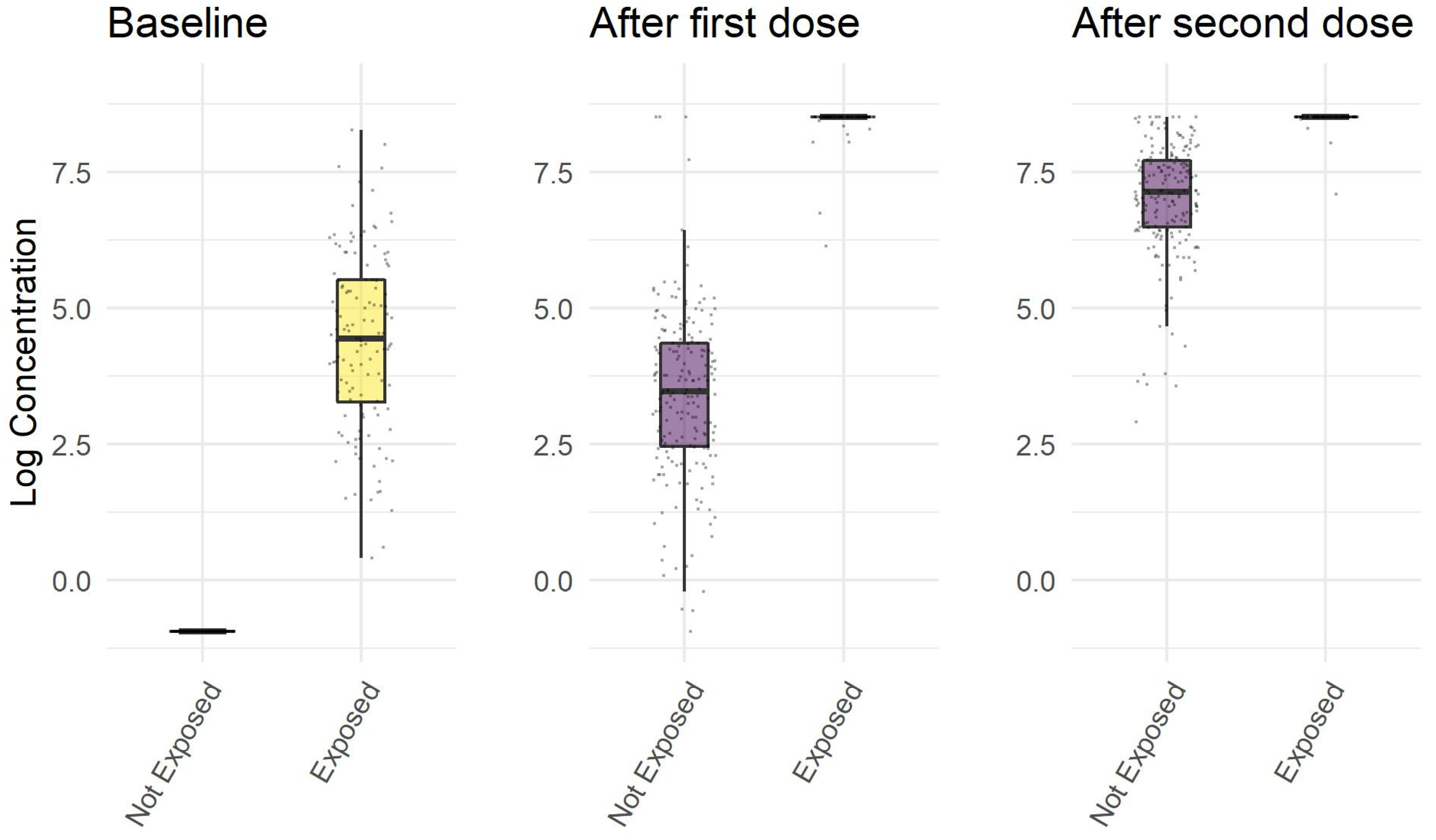
| Non Exposed Subjects | Exposed Subjects | p | |
|---|---|---|---|
| Ab concentration before first dose, U/mL | 0.4 (0.4–0.4) | 85 (26–250) | <0.001 |
| Ab concentration 21 days after first dose, U/mL | 32 (12–78) | 5001 (5001–5001) | <0.001 |
| Ab concentration 12 days after second dose, U/mL | 1258 (657–224) | 5001 (5001–5001) | <0.001 |
| age, years | 50 (42–57) | 46 (39–53) | 0.003 |
| sex, female | 157 (80%) | 102 (85%) | 0.34 |
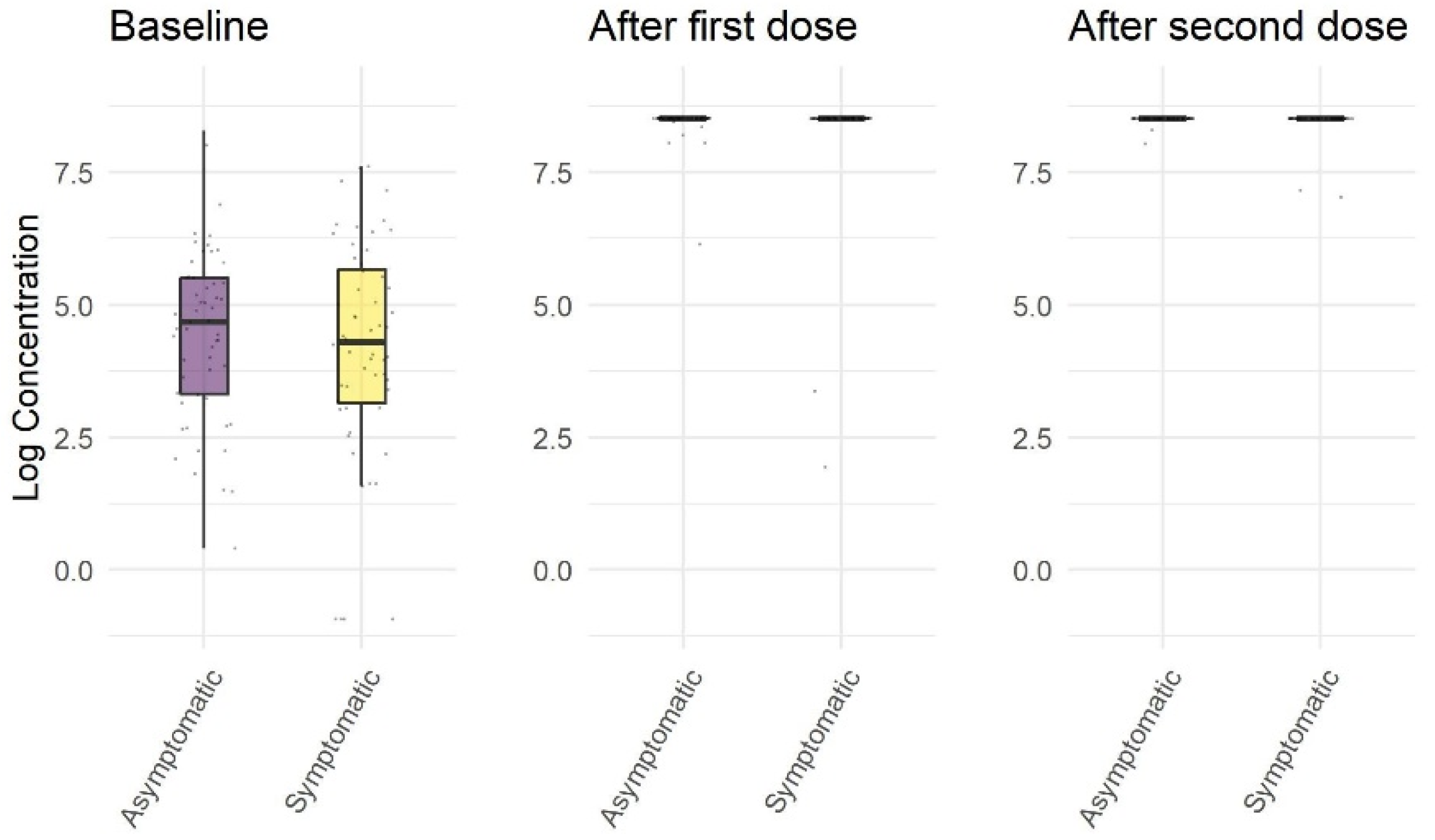
| Asymptomatic Subjects | Symptomatic Subjects | p | |
|---|---|---|---|
| Ab concentration before first dose, U/mL | 108.0 (27.3 to 247.9) | 73.4 (23.1 to 290.7) | 0.59 |
| Ab concentration 21 days after first dose, U/mL | 5001.0 (5001.0 to 5001.0) | 5001.0 (5001.0 to 5001.0) | 0.16 |
| Ab concentration 12 days after second dose, U/mL | 5001.0 (5001.0 to 5001.0) | 5001.0 (5001.0 to 5001.0) | 0.67 |
| age, years | 44.0 (38.5 to 51.5) | 47.5 (38.0 to 54.0) | 0.38 |
| sex, female | 47 (85.5) | 52 (92.9) | 0.34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvaggio, M.; Fusina, F.; Albani, F.; Salvaggio, M.; Beschi, R.; Ferrari, E.; Costa, A.; Agnoletti, L.; Facchi, E.; Natalini, G. Antibody Response after BNT162b2 Vaccination in Healthcare Workers Previously Exposed and Not Exposed to SARS-CoV-2. J. Clin. Med. 2021, 10, 4204. https://doi.org/10.3390/jcm10184204
Salvaggio M, Fusina F, Albani F, Salvaggio M, Beschi R, Ferrari E, Costa A, Agnoletti L, Facchi E, Natalini G. Antibody Response after BNT162b2 Vaccination in Healthcare Workers Previously Exposed and Not Exposed to SARS-CoV-2. Journal of Clinical Medicine. 2021; 10(18):4204. https://doi.org/10.3390/jcm10184204
Chicago/Turabian StyleSalvaggio, Marcello, Federica Fusina, Filippo Albani, Maurizio Salvaggio, Rasula Beschi, Emanuela Ferrari, Alberto Costa, Laura Agnoletti, Emanuela Facchi, and Giuseppe Natalini. 2021. "Antibody Response after BNT162b2 Vaccination in Healthcare Workers Previously Exposed and Not Exposed to SARS-CoV-2" Journal of Clinical Medicine 10, no. 18: 4204. https://doi.org/10.3390/jcm10184204
APA StyleSalvaggio, M., Fusina, F., Albani, F., Salvaggio, M., Beschi, R., Ferrari, E., Costa, A., Agnoletti, L., Facchi, E., & Natalini, G. (2021). Antibody Response after BNT162b2 Vaccination in Healthcare Workers Previously Exposed and Not Exposed to SARS-CoV-2. Journal of Clinical Medicine, 10(18), 4204. https://doi.org/10.3390/jcm10184204