
Coronary Microvascular Dysfunction in Takotsubo Syndrome Assessed by Angiography-Derived Index of Microcirculatory Resistance: A Pressure-Wire-Free Tool

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
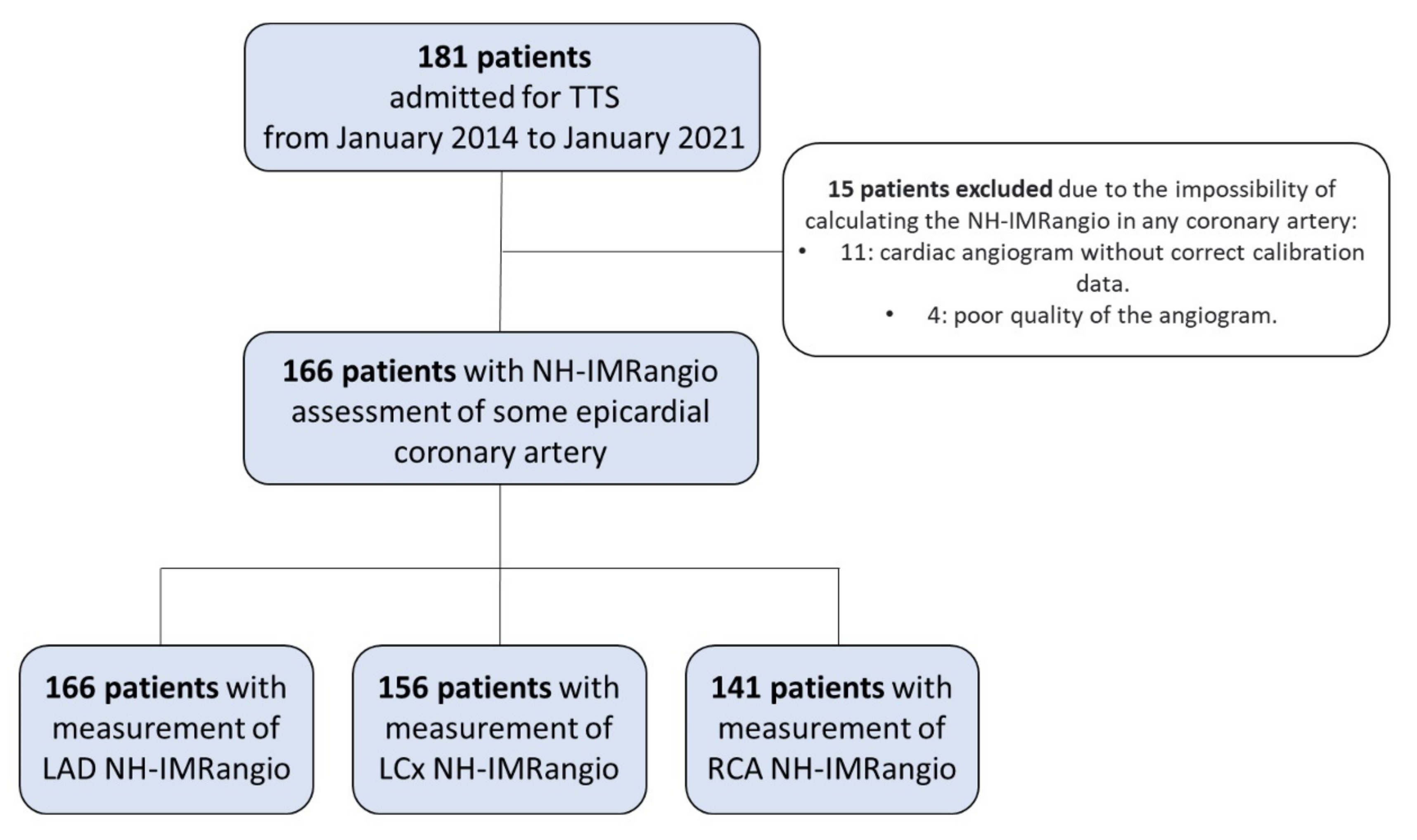
2.1. Study Population
2.2. Study Variables
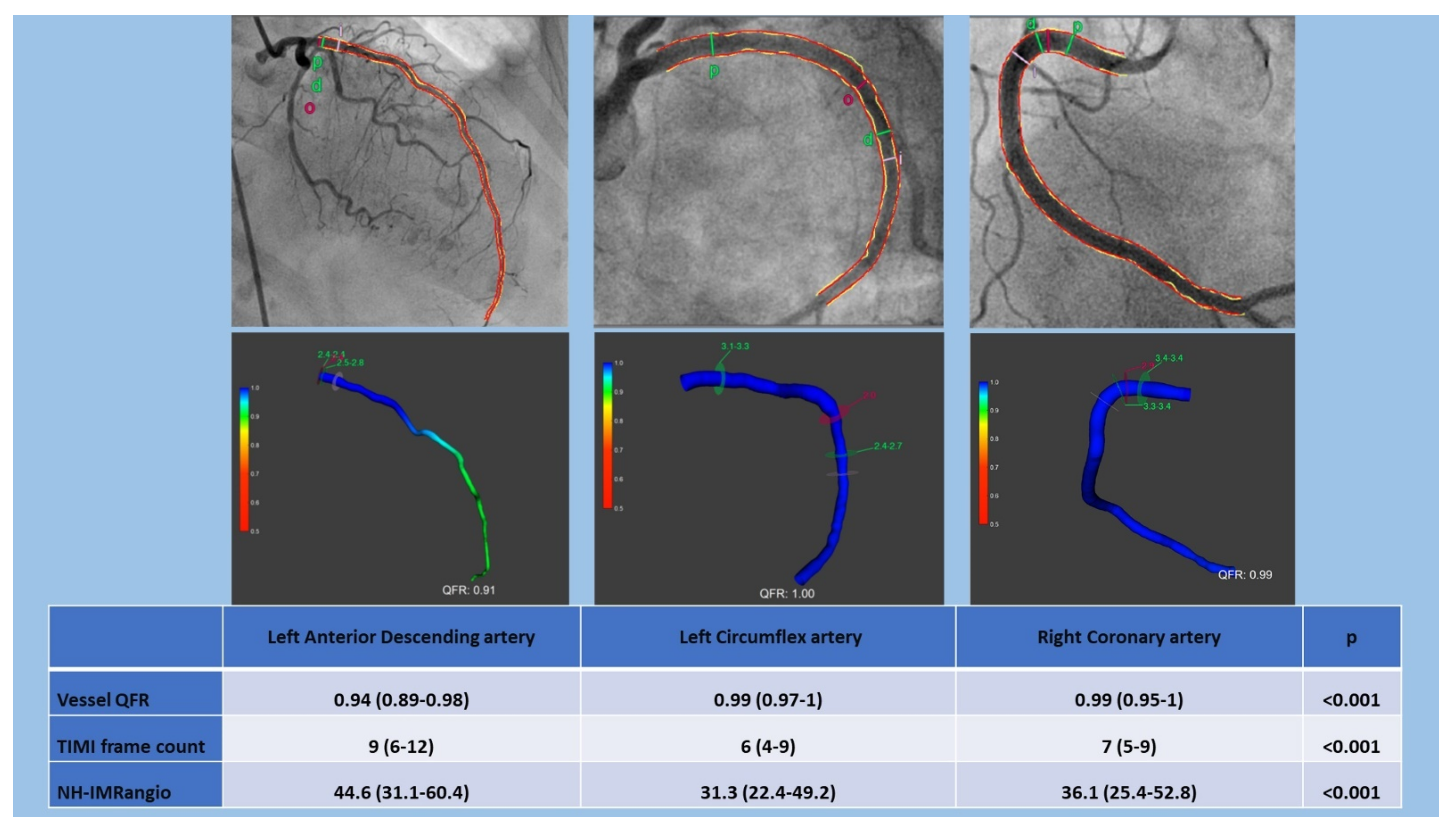
2.3. 3D-QCA, QFR and NH-IMRangio Assessment
2.4. Statistical Analysis
3. Results
3.1. Evaluation of Microcirculatory Status in Epicardial Coronary Arteries
3.2. Evaluation of CMD in the Different Patterns of Wall Motion Abnormalities
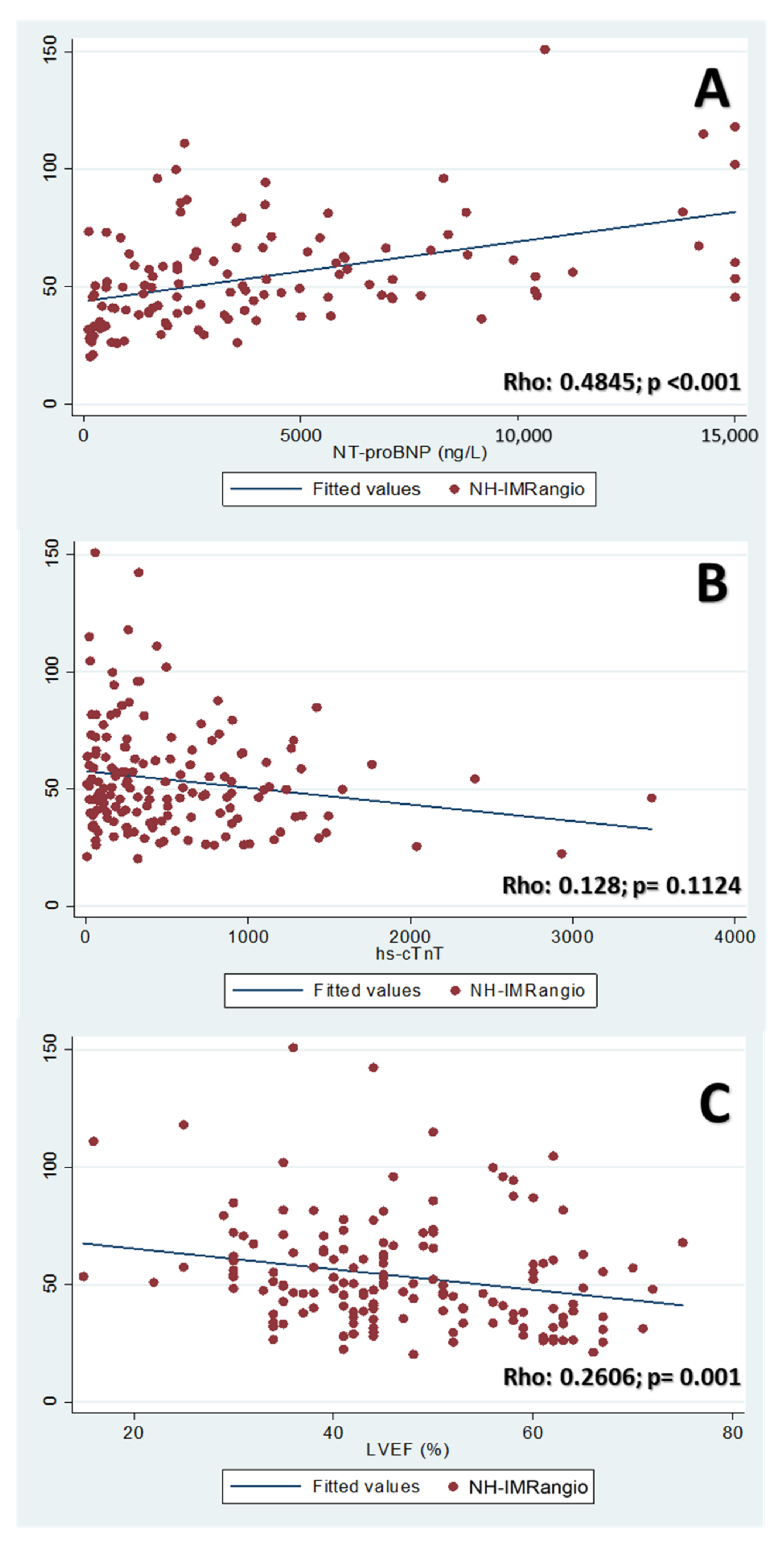
3.3. Correlation of NH-IMRangio with Biomarkers & LVEF
3.4. Differences between Patients by NH-IMRangio Value
3.5. Differences Based on Extension of Microvascular Dysfunction
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ghadri, J.R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; Cammann, V.L.; Crea, F.; Galiuto, L.; Desmet, W.; et al. International Expert Consensus Document on Takotsubo Syndrome (Part II): Diagnostic Workup, Outcome, and Management. Eur. Heart J. 2018, 39, 2047–2062. [Google Scholar] [CrossRef] [PubMed]
- Lyon, A.R.; Bossone, E.; Schneider, B.; Sechtem, U.; Citro, R.; Underwood, S.R.; Sheppard, M.N.; Figtree, G.A.; Parodi, G.; Akashi, Y.J.; et al. Current state of knowledge on Takotsubo syndrome: A Position Statement from the Taskforce on Takotsubo Syndrome of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2016, 18, 8–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boland, T.A.; Lee, V.H.; Bleck, T.P. Stress-induced cardiomyopathy. Crit. Care Med. 2015, 43, 686–693. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, S.W.; Windenburg, D.C.; Lesser, J.R.; Maron, M.S.; Hauser, R.G.; Lesser, J.N.; Haas, T.S.; Hodges, J.S.; Maron, B.J. Natural History and Expansive Clinical Profile of Stress (Tako-Tsubo) Cardiomyopathy. J. Am. Coll. Cardiol. 2010, 55, 333–341. [Google Scholar] [CrossRef] [Green Version]
- Templin, C.; Ghadri, J.R.; Diekmann, J.; Napp, L.C.; Bataiosu, D.R.; Jaguszewski, M.; Cammann, V.L.; Sarcon, A.; Geyer, V.; Neumann, C.A.; et al. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. N. Engl. J. Med. 2015, 373, 929–938. [Google Scholar] [CrossRef] [Green Version]
- Akashi, Y.J.; Nakazawa, K.; Sakakibara, M.; Miyake, F.; Musha, H.; Sasaka, K. 123I-MIBG myocardial scintigraphy in patients with “takotsubo” cardiomyopathy. J. Nucl. Med. 2004, 45, 1121–1127. [Google Scholar]
- Wittstein, I.; Thieman, D.; Lima, J.; Baughman, K.; Schulman, S.; Gerstenblith, G.; Wu, K.C.; Rade, J.J.; Bivalacqua, T.J.; Champion, H.C. Neurohumoral Features of Myocardial Stunning Due to Sudden Emotional Stress. N. Engl. J. Med. 2005, 352, 2481–2488. [Google Scholar] [CrossRef]
- Bybee, K.A.; Prasad, A.; Barsness, G.W.; Lerman, A.; Jaffe, A.S.; Murphy, J.G.; Wright, R.S.; Rihal, C.S. Clinical characteristics and Thrombolysis in Myocardial Infarction frame counts in women with transient left ventricular apical ballooning syndrome. Am. J. Cardiol. 2004, 94, 343–346. [Google Scholar] [CrossRef]
- Abdelmoneim, S.S.; Mankad, S.V.; Bernier, M.; Dhoble, A.; Hagen, M.E.; Ness, S.A.C.; Chandrasekaran, K.; Pellikka, P.A.; Oh, J.K.; Mulvagh, S.L. Microvascular Function in Takotsubo Cardiomyopathy With Contrast Echocardiography: Prospective Evaluation and Review of Literature. J. Am. Soc. Echocardiogr. 2009, 22, 1249–1255. [Google Scholar] [CrossRef]
- Elesber, A.; Lerman, A.; Bybee, K.A.; Murphy, J.G.; Barsness, G.; Singh, M.; Rihal, C.S.; Prasad, A. Myocardial perfusion in apical ballooning syndrome correlate of myocardial injury. Am. Heart J. 2006, 152, e9–e469. [Google Scholar] [CrossRef]
- Khalid, N.; Ikram, S. Coronary flow assessment in Takotsubo cardiomyopathy with TIMI frame count. Int. J. Cardiol. [Internet] 2015, 197, 208. [Google Scholar] [CrossRef] [PubMed]
- Rigo, F.; Sicari, R.; Citro, R.; Ossena, G.; Buja, P.; Picano, E. Diffuse, marked, reversible impairment in coronary microcirculation in stress cardiomyopathy: A Doppler transthoracic echo study. Ann. Med. 2009, 41, 462–470. [Google Scholar] [CrossRef]
- Martínez, G.J.; Yong, A.S.C.; Fearon, W.F.; Ng, M.K.C. The index of microcirculatory resistance in the physiologic assessment of the coronary microcirculation. Coron. Artery Dis. 2015, 26, e15–e26. [Google Scholar] [CrossRef] [PubMed]
- Möller, C.; Stiermaier, T.; Meusel, M.; Jung, C.; Graf, T.; Eitel, I. Microcirculation in Patients with Takotsubo Syndrome—The Prospective CIRCUS-TTS Study. J. Clin. Med. 2021, 10, 2127. [Google Scholar] [CrossRef]
- Aarnoudse, W.; Van Den Berg, P.; Van De Vosse, F.; Geven, M.; Rutten, M.; Van Turnhout, M.; Fearon, W.; De Bruyne, B.; Pijls, N. Myocardial Resistance Assessed by Guidewire-Based Pressure-Temperature Measurement: In Vitro Validation. Catheter. Cardiovasc. Interv. 2004, 62, 56–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, M.K.C.; Yong, A.S.C.; Ho, M.; Shah, M.G.; Chawantanpipat, C.; O’Connell, R.; Keech, A.; Kritharides, L.; Fearon, W.F. The index of microcirculatory resistance predicts myocardial infarction related to percutaneous coronary intervention. Circ. Cardiovasc. Interv. 2012, 5, 515–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fearon, W.F.; Kobayashi, Y. Invasive Assessment of the Coronary Microvasculature: The Index of Microcirculatory Resistance. Circ. Cardiovasc. Interv. 2017, 10, 1–11. [Google Scholar] [CrossRef]
- De Maria, G.L.; Alkhalil, M.; Wolfrum, M.; Fahrni, G.; Borlotti, A.; Gaughran, L.; Dawkins, S.; Langrish, J.P.; Lucking, A.J.; Choudhury, R.P.; et al. Index of Microcirculatory Resistance as a Tool to Characterize Microvascular Obstruction and to Predict Infarct Size Regression in Patients With STEMI Undergoing Primary PCI. JACC Cardiovasc. Imaging 2019, 12, 837–848. [Google Scholar] [CrossRef]
- Daniels, D.V.; Fearon, W.F. The index of microcirculatory resistance (IMR) in takotsubo cardiomyopathy. Catheter Cardiovasc Interv. 2011, 77, 128–131. [Google Scholar] [CrossRef]
- Kim, H.S.; Tremmel, J.A.; Nam, C.W.; Zhou, J.; Haddad, F.; Vagelos, R.H.; Lee, D.P.; Yeung, A.C.; Fearon, W.F. Quantitative comparison of microcirculatory dysfunction in patients with stress cardiomyopathy and ST-segment elevation myocardial infarction. J. Am. Coll. Cardiol. 2011, 58, 2430–2431. [Google Scholar] [CrossRef] [Green Version]
- Layland, J.; Whitbourn, R.; MacIsaac, A.; Somaratne, J.; Wilson, A. Takotsubo cardiomyopathy: Reversible elevation in microcirculatory resistance. Cardiovasc. Revascularization Med. 2012, 13, 66–68. [Google Scholar] [CrossRef] [PubMed]
- Warisawa, T.; Naganuma, T.; Nakamura, S. Reversible microvascular dysfunction in takotsubo syndrome shown using index of microcirculatory resistance. Circ. J. 2016, 80, 750–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivero, F.; Cuesta, J.; García-Guimaraes, M.; Bastante, T.; Alvarado, T.; Antuña, P.; Alfonso, F. Time-related microcirculatory dysfunction in patients with Takotsubo cardiomyopathy. JAMA Cardiol. 2017, 2, 699–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez-Barrios, A.; Rivero, F.; Noval-Morillas, I.; Gheorghe, L.; Calle-Pérez, G.; Alfonso, F. Feasibility of absolute coronary blood flow and microvascular resistance quantification in tako-tsubo cardiomyopathy. Rev. Esp. de Cardiol. 2020, 73, 94–95. [Google Scholar] [CrossRef]
- Tebaldi, M.; Biscaglia, S.; Di Girolamo, D.; Erriquez, A.; Penzo, C.; Tumscitz, C.; Campo, G. Angio-based index of microcirculatory resistance for the assessment of the coronary resistance: A proof of concept study. J. Interv. Cardiol. 2020, 2020, 8887369. [Google Scholar] [CrossRef]
- De Maria, G.L.; Scarsini, R.; Shanmuganathan, M.; Kotronias, R.A.; Terentes-Printzios, D.; Borlotti, A.; Langrish, J.P.; Lucking, A.J.; Choudhury, R.P.; Kharbanda, R.; et al. Angiography-derived index of microcirculatory resistance as a novel, pressure-wire-free tool to assess coronary microcirculation in ST elevation myocardial infarction. Int. J. Cardiovasc. Imaging 2020, 36, 1395–1406. [Google Scholar] [CrossRef]
- Scarsini, R.; Shanmuganathan, M.; Kotronias, R.A.; Terentes-Printzios, D.; Borlotti, A.; Langrish, J.P.; Lucking, A.J.; OxAMI Study Investigators; Ribichini, F.; Ferreira, V.M.; et al. Angiography-derived index of microcirculatory resistance (IMRangio) as a novel pressure-wire-free tool to assess coronary microvascular dysfunction in acute coronary syndromes and stable coronary artery disease. Int. J. Cardiovasc. Imaging 2021, 37, 1801–1813. [Google Scholar] [CrossRef]
- Kotronias, R.; Terentes-Printzios, D.; Shanmuganathan, M.; Marin, F.; Scarsini, R.; Bradley-Watson, J.; Langrish, J.P.; Lucking, A.J.; Choudhury, R.; Kharbanda, R.K.; et al. Long-Term Clinical Outcomes in Patients With an Acute ST-Segment-Elevation Myocardial Infarction Stratified by Angiography-Derived Index of Microcirculatory Resistance. Front. Cardiovasc. Med. 2021, 1, 717114. [Google Scholar] [CrossRef]
- Prasad, A.; Lerman, A.; Rihal, C.S. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): A mimic of acute myocardial infarction. Am. Heart J. 2008, 155, 408–417. [Google Scholar] [CrossRef] [PubMed]
- Stevens, L.A.; Manzi, J.; Levey, A.S.; Chen, J.; Deysher, A.E.; Greene, T.; Poggio, E.D.; Schmid, C.; Steffes, M.W.; Zhang, Y.; et al. Impact of Creatinine Calibration on Performance of GFR Estimating Equations in a Pooled Individual Patient Database. Am. J. Kidney Dis. 2007, 50, 21–35. [Google Scholar] [CrossRef]
- Melikian, N.; Vercauteren, S.; Fearon, W.F.; Cuisset, T.; MacCarthy, P.A.; Davidavicius, G.; Aarnoudse, W.; Bartunek, J.; Vanderheyden, M.; Wyffels, E.; et al. Quantitative assessment of coronary microvascular function in patients with and without epicardial atherosclerosis. EuroIntervention 2010, 5, 939–945. [Google Scholar] [CrossRef] [PubMed]
- Khalid, N.; Iqbal, I.; Coram, R.; Raza, T.; Fahsah, I.; Ikram, S. Thrombolysis in Myocardial Infarction Frame Count in Takotsubo Cardiomyopathy. Int. J. Cardiol. 2015, 191, 107–108. [Google Scholar] [CrossRef] [PubMed]
- Reddin, G.; Forrestal, B.J.; Garcia-Garcia, H.M.; Medvedofsky, D.; Singh, M.; Asch, F.M.; Ribeiro, H.B.C.C. Left ventricular global longitudinal strain assessment in patients with Takotsubo Cardiomyopathy: A call for an echocardiography-based classification. Minerva Cardioangiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Reddin, G.; Garcia-Garcia, H.M.; Medvedofsky, D.; Asch, F.M.; Kumar, P.; Franken, M.; Campos, C.M. Comparison of Contractility Patterns on Left Ventriculogram Versus Longitudinal Strain by Echocardiography in Patients With Takotsubo Cardiomyopathy. Cardiovasc. Revascularization Med. 2021, 27, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.H.; Neil, C.J.; Sverdlov, A.L.; Mahadavan, G.; Chirkov, Y.Y.; Kucia, A.M.; Stansborough, J.; Beltrame, J.F.; Selvanayagam, J.B.; Zeitz, C.; et al. N-terminal pro-brain natriuretic protein levels in takotsubo cardiomyopathy. Am. J. Cardiol. 2011, 108, 1316–1321. [Google Scholar] [CrossRef]
- Khan, H.; Gamble, D.; Mezincescu, A.; Abbas, H.; Rudd, A.; Dawson, D. A systematic review of biomarkers in Takotsubo syndrome: A focus on better understanding the pathophysiology. IJC Heart Vasc. 2021, 34, 100795. [Google Scholar] [CrossRef]
- Ai, H.; Feng, Y.; Gong, Y.; Zheng, B.; Jin, Q.; Zhang, H.P.; Sun, F.; Li, J.; Chen, Y.; Huo, Y.; et al. Coronary Angiography-Derived Index of Microvascular Resistance. Front. Physiol. 2020, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.H.; Dai, N.; Li, Y.L.; Kim, J.; Shin, D.; Lee, S.H.; Joh, H.S.; Kim, H.K.; Jeon, K.-H.; Ha, S.J.; et al. Functional Coronary Angiography–Derived Index of Microcirculatory Resistance in Patients With ST-Segment Elevation Myocardial Infarction. JACC Cardiovasc. Interv. 2021, 14, 1670–1684. [Google Scholar] [CrossRef]
- Mejia-Renteria, H.; Lee, J.M.; Choi, K.H.; Lee, S.H.; Wang, L.; Kakuta, T.; Koo, B.K.; Escaned, J. Coronary microcirculation assessment using functional angiography: Development of a wire-free method applicable to conventional coronary angiograms. Catheter. Cardiovasc. Interv. 2021. [Google Scholar] [CrossRef]
- Fearon, W.F.; Low, A.F.; Yong, A.S.; McGeoch, R.; Berry, C.; Shah, M.G.; Ho, M.Y.; Kim, H.S.; Loh, J.P.; Oldroyd, K.G. Prognostic value of the Index of Microcirculatory Resistance measured after primary percutaneous coronary intervention. Circulation 2013, 127, 2436–3441. [Google Scholar] [CrossRef] [Green Version]
- Solberg, O.G.; Ragnarsson, A.; Kvarsnes, A.; Endresen, K.; Kongsgård, E.; Aakhus, S.; Gullestad, L.; Stavem, K.A.L. Reference interval for the index of coronary microvascular resistance. EuroIntervention 2014, 9, 1069–1075. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 181) | |
|---|---|
| Age (years) | 75.3 (65.3–81.8) |
| Female gender | 83.4 |
| Hypertension | 68.5 |
| Diabetes mellitus | 24.9 |
| Dyslipidemia | 46.9 |
| Current smoker | 17.1 |
| Body mass index (kg/m2) | 24.7 (22.2–27.5) |
| Previous coronary artery disease | 5.0 |
| Previous psychiatric disorder | 34.3 |
| Chronic kidney disease | 10.5 |
| TAKOTSUBO-RELATED DATA | |
| Clinical presentation: | |
| - Chest pain | 69.3 |
| - Vegetative symptoms | 42.2 |
| - Dyspnea | 50.0 |
| - Palpitations | 3.6 |
| - Syncope | 6.6 |
| - Cardiac arrest | 6.0 |
| Previous stressful situation | 57.5 |
| Secondary form of TTS | 31.9 |
| Systolic blood pressure (mmHg) | 128 (114–146) |
| Heart rate (bpm) | 85 (75–100) |
| Killip-Kimball class: | |
| - I | 64.1 |
| - II | 14.9 |
| - III | 11.1 |
| - IV | 9.9 |
| Left ventricular ejection fraction (%) | 45 (35–55) |
| Patterns of wall motion abnormalities: | |
| - Apical limited | 48.1 |
| - Mid-ventricular and Apical | 25.4 |
| - Mid-ventricular | 13.8 |
| - Basal limited | 6.1 |
| - Mid-ventricular and Basal | 2.8 |
| - Other | 3.8 |
| ECG DATA | |
| Sinus rhythm | 87.9 |
| ST-segment elevation | 54.7 |
| ST-segment depression | 46.4 |
| Negative T waves | 34.9 |
| Long QT interval | 45.3 |
| QT interval (msec) | 450 (430–500) |
| BLOOD TEST DATA | |
| pH | 7.36 (7.27–7.43) |
| Lactate (mmol/L) | 2.7 (1.2–5.0) |
| Hemoglobin (g/L) | 129 (116–141) |
| hs-cTnT (ng/L) | 250.5 (80.5–656.0) |
| eGFR (ml/min/1.73 m2) | 76.0 (54.3–89.7) |
| NT-proBNP (pg/mL) | 3300 (1318–6955) |
| MANAGEMENT | |
| Need for non-invasive ventilation | 13.3 |
| Need for invasive ventilation | 13.8 |
| Use of inotropes | 13.3 |
| Intra-aortic counterpulsation balloon | 2.2 |
| Renal replacement therapy | 5.0 |
| Characteristic | NH-IMRangio < 50.6 (n: 83) | NH-IMRangio ≥ 50.6 (n: 83) | p-Value |
|---|---|---|---|
| Age (years) | 75.6 (65.0–82.4) | 74.4 (64.9–80.6) | 0.7578 |
| Female gender | 79.5 | 86.8 | 0.214 |
| Prior physical stressful trigger | 44.6 | 26.5 | 0.015 |
| Prior emotional stressful trigger | 13.3 | 27.7 | 0.021 |
| Patterns of wall motion abnormalities: | 0.04 | ||
| - Apical limite | 60.2 | 39.8 | 0.008 |
| - Mid-ventricular + Apical | 16.9 | 34.9 | 0.008 |
| - Mid-ventricular limited | 12.1 | 12.1 | 1 |
| - Basal limited | 7.2 | 4.8 | 0.514 |
| - Mid-ventricular + Basal | 0 | 2.4 | 0.155 |
| - Other | 3.6 | 6.0 | 0.469 |
| SBP (mmHg) | 134 (120–150) | 124 (110–140) | 0.056 |
| Heart rate (bpm) | 85 (73–100) | 85 (77–96) | 0.719 |
| Killip class at admission: | 0.499 | ||
| - I | 62.7 | 67.5 | 0.515 |
| - II | 16.9 | 14.5 | 0.669 |
| - III | 13.3 | 7.2 | 0.201 |
| - IV | 7.2 | 10.8 | 0.417 |
| Atrial fibrillation | 2.4 | 9.6 | 0.05 |
| LVED-pressure (mmHg) | 17 (13–23) | 19 (12–25) | 0.5957 |
| LVEF (%) | 47 (42–59) | 42.5 (35–50) | 0.0047 |
| pH | 7.36 (7.29–7.42) | 7.37 (7.26–7.44) | 0.6097 |
| Lactate (mmol/L) | 2.6 (1.2–3.1) | 2.6 (0.9–3.4) | 0.7478 |
| Hemoglobin (g/L) | 124 (111–140) | 133.5 (122–143) | 0.007 |
| NT-proBNP (pg/mL) | 2716.5 (935.5–5315.5) | 4198 (2154–8390) | 0.011 |
| hs-cTnT (ng/L) | 250 (79–630) | 247 (77–661) | 0.8185 |
| One Artery Affected (n: 11) | Two Arteries Affected (n: 38) | Three Arteries Affected (n: 82) | p | |
|---|---|---|---|---|
| Age (years) | 72.9 (67.5–81.3) | 70.5 (64.7–77.3) | 75.6 (64.3–83.0) | 0.1467 |
| Female gender | 72.7 | 79.0 | 86.6 | 0.363 |
| Prior physical stressful trigger | 36.3 | 39.5 | 36.6 | 0.952 |
| Prior emotional stressful trigger | 18.2 | 21.1 | 20.7 | 0.978 |
| Patterns of wall motion abnormalities: | 0.296 | |||
| - Apical limited | 72.7 | 55.3 | 42.7 | 0.054 |
| - Mid-ventricular + Apical | 15.8 | 18.2 | 35.4 | 0.064 |
| - Mid-ventricular limited | 0 | 13.2 | 12.2 | 0.455 |
| - Basal limited | 9.1 | 7.9 | 4.9 | 0.741 |
| - Mid-ventricular + Basal | 0 | 0 | 2.4 | 0.545 |
| - Other | 0 | 7.9 | 2.4 | 0.275 |
| SBP (mmHg) | 113 (95–133) | 111 (94–143) | 128 (115–143) | 0.5594 |
| Heart rate (bpm) | 88.5 (77–120) | 84.5 (74–95) | 81 (73–93) | 0.4548 |
| Atrial fibrillation | 9.1 | 2.6 | 7.3 | 0.554 |
| LVED-pressure (mmHg) | 16.5 (14–23.5) | 16.5 (12–23) | 18 (12.5–24.5) | 0.9201 |
| LVEF (%) | 48 (41–58) | 44 (35–58) | 44 (38–52) | 0.7174 |
| pH | 7.32 (7.30–7.36) | 7.29 (7.26–7.37) | 7.42 (7.34–7.44) | 0.1820 |
| Lactate (mmol/L) | 2.4 (0.4–2.9) | 2.9 (0.9–3.5) | 2.3 (0.8–3.1) | 0.4237 |
| Hemoglobin (g/L) | 121 (100–130) | 133 (122–143) | 130 (117–140) | 0.0741 |
| NT-proBNP (pg/mL) | 200 (127–3907) | 2799 (1414–5786) | 3650 (1924–7400) | 0.0075 |
| hs-cTnT (ng/L) | 215 (45–487) | 216 (91–628) | 260 (64–643) | 0.8283 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sans-Roselló, J.; Fernández-Peregrina, E.; Duran-Cambra, A.; Carreras-Mora, J.; Sionis, A.; Álvarez-García, J.; Garcia-Garcia, H.M. Coronary Microvascular Dysfunction in Takotsubo Syndrome Assessed by Angiography-Derived Index of Microcirculatory Resistance: A Pressure-Wire-Free Tool. J. Clin. Med. 2021, 10, 4331. https://doi.org/10.3390/jcm10194331
Sans-Roselló J, Fernández-Peregrina E, Duran-Cambra A, Carreras-Mora J, Sionis A, Álvarez-García J, Garcia-Garcia HM. Coronary Microvascular Dysfunction in Takotsubo Syndrome Assessed by Angiography-Derived Index of Microcirculatory Resistance: A Pressure-Wire-Free Tool. Journal of Clinical Medicine. 2021; 10(19):4331. https://doi.org/10.3390/jcm10194331
Chicago/Turabian StyleSans-Roselló, Jordi, Estefanía Fernández-Peregrina, Albert Duran-Cambra, Jose Carreras-Mora, Alessandro Sionis, Jesús Álvarez-García, and Hector M. Garcia-Garcia. 2021. "Coronary Microvascular Dysfunction in Takotsubo Syndrome Assessed by Angiography-Derived Index of Microcirculatory Resistance: A Pressure-Wire-Free Tool" Journal of Clinical Medicine 10, no. 19: 4331. https://doi.org/10.3390/jcm10194331
APA StyleSans-Roselló, J., Fernández-Peregrina, E., Duran-Cambra, A., Carreras-Mora, J., Sionis, A., Álvarez-García, J., & Garcia-Garcia, H. M. (2021). Coronary Microvascular Dysfunction in Takotsubo Syndrome Assessed by Angiography-Derived Index of Microcirculatory Resistance: A Pressure-Wire-Free Tool. Journal of Clinical Medicine, 10(19), 4331. https://doi.org/10.3390/jcm10194331