
Relationship between Behavioral Infant Speech Perception and Hearing Age for Children with Hearing Loss


Abstract
:1. Introduction
- What proportion of CHH and CNH can demonstrate discrimination of each a vowel and consonant contrast as measured by CHT, at 50, 60, and/or 70 dBA SPL in a single test session while accounting for hearing age?
- Is there a difference in the ability of CHH (who met 1–3–6 benchmarks) and CNH in their demonstration of vowel and consonant discrimination assessed through a CHT task?
- Is there a relationship between aided SII measured at 50 dB SPL and performance on a CHT speech perception task for each contrast?
2. Materials and Methods
2.1. Participants
2.2. Participant Hearing Aids
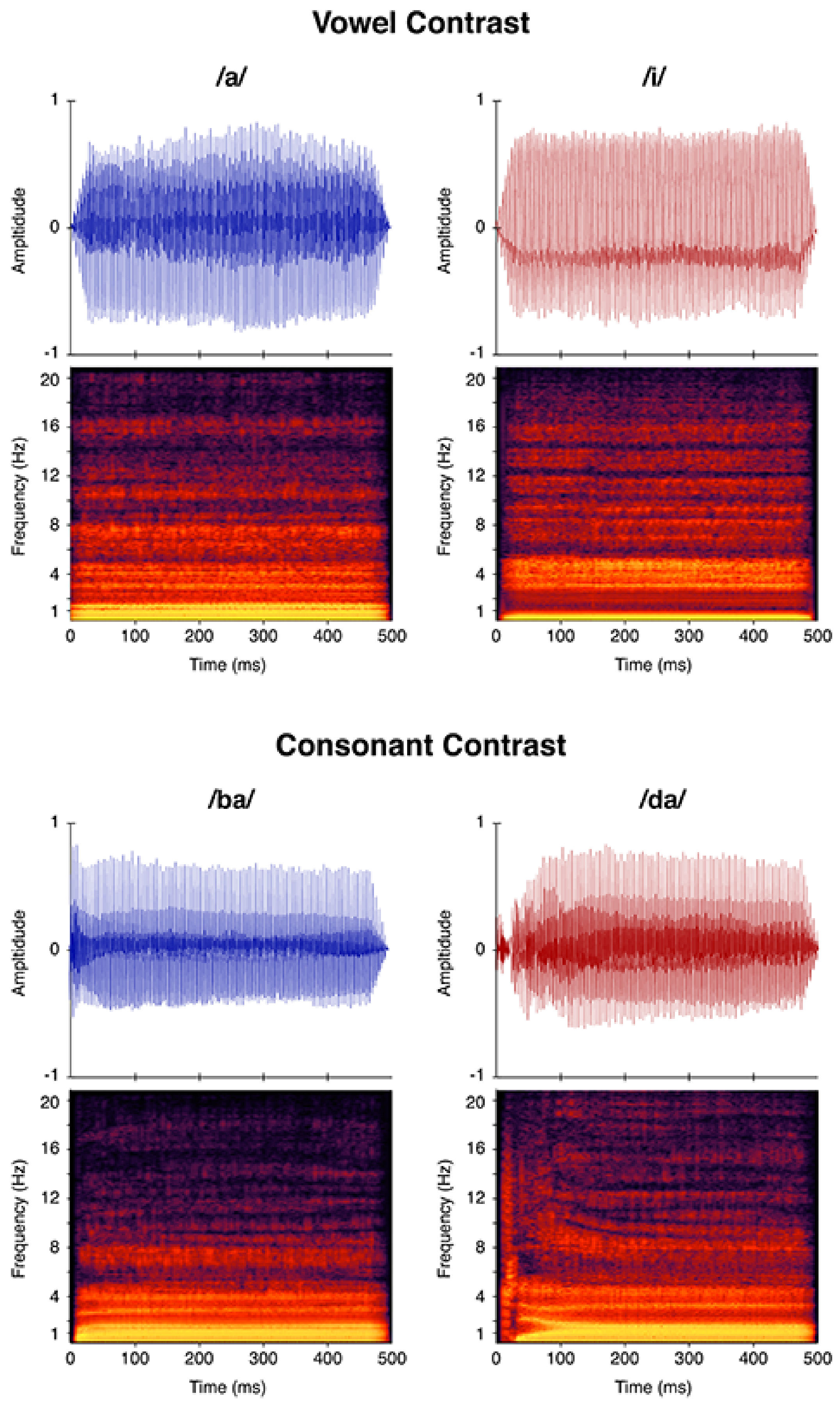
2.3. Stimuli
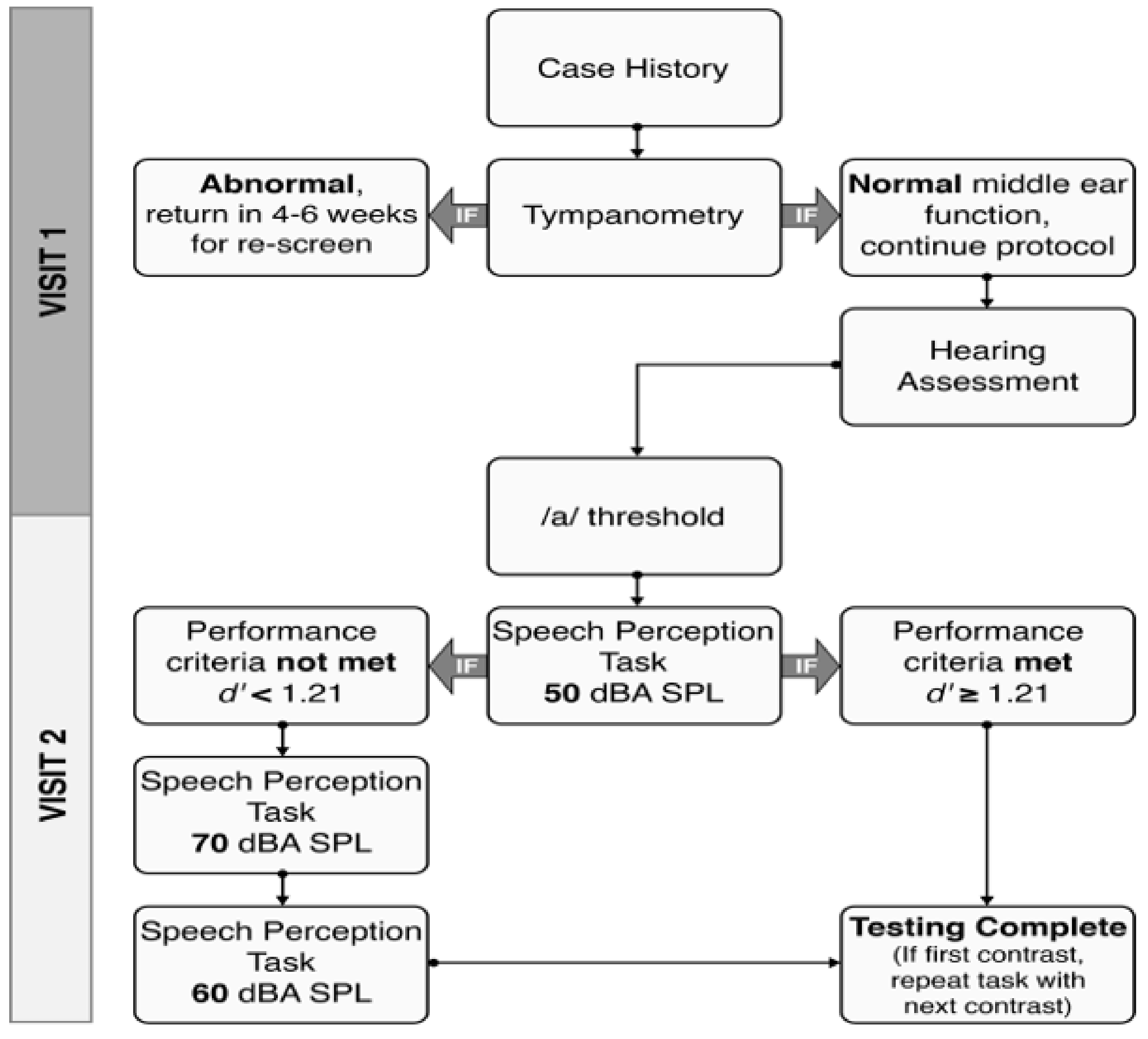
2.4. Testing Protocol
2.5. Statistical Analysis
3. Results
3.1. Effect of Hearing Status on Speech Perception
3.2. Differences in Speech Perception Abilities among CHH and CNH
3.3. Hearing Status
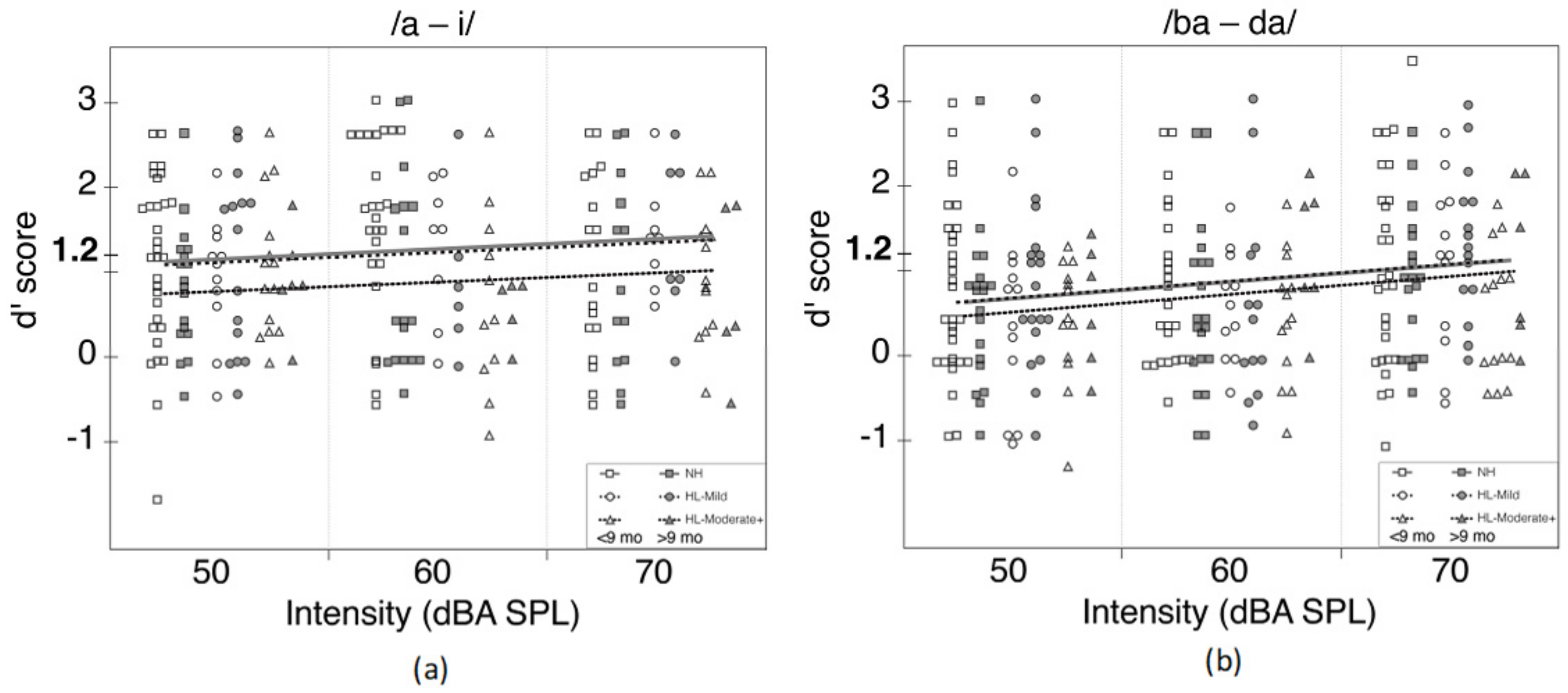
3.4. Presentation Level
3.5. Aided SII
4. Discussion
4.1. Hearing Status
4.2. Presentation Level
4.3. Aided SII
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Joint Committee on Infant Hearing (JCIH). Year 2007 position statement: Principles and guidelines for early hearing detection and intervention programs. Pediatrics 2007, 120, 898–921. [Google Scholar] [CrossRef] [Green Version]
- Mayne, A.M.; Yoshinaga-Itano, C.; Sedey, A.L.; Carey, A. Expressive vocabulary development of infants and toddlers who are deaf or hard of hearing. Volta Rev. 1998, 100, 1–28. [Google Scholar]
- Vohr, B.; Jodoin-Krauzyk, J.; Tucker, R.; Topol, D.; Johnson, M.J.; Ahlgren, M.; Pierre, L.S. Expressive vocabulary of children with hearing loss in the first 2 years of life: Impact of early intervention. J. Perinatol. 2011, 31, 274–280. [Google Scholar] [CrossRef] [Green Version]
- Walker, E.A.; Tomblin, J.B.; Moeller, M.P.; Oleson, J.J.; Harrison, M.; Ambrose, S.E. Language Outcomes in Young Children with Mild to Severe Hearing Loss. Ear Hear. 2015, 36, 76S–91S. [Google Scholar]
- Yoshinaga-Itano, C.; Sedey, A.L.; Coulter, D.K.; Mehl, A.L. Language of early and later-identified children with hearing loss. Pediatrics 1998, 102, 1161–1171. [Google Scholar] [CrossRef] [Green Version]
- Sininger, Y.S.; Grimes, A.; Christensen, E. Auditory development in early amplified children: Factors influencing auditory-based communication outcomes in children with hearing loss. Ear Hear. 2010, 31, 166–185. [Google Scholar] [CrossRef] [Green Version]
- Spivak, L.; Sokol, H.; Auerbach, C.; Gershkovich, S. Newborn hearing screening follow-up: Factors affecting hearing aid fitting by 6 months of age. Am. J. Audiol. 2009, 18, 24–33. [Google Scholar] [CrossRef]
- Moeller, M.P. Early intervention and language development in children who are deaf and hard of hearing. Pediatrics 2000, 106, E43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halpin, K.S.; Smith, K.Y.; Widen, J.E.; Chertoff, M.E. Effects of universal newborn hearing screening on an early intervention program for children with hearing loss, birth to 3 yr of age. J. Am. Acad. Audiol. 2010, 21, 165–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, C.R.; McCann, D.C.; Campbell, M.J.; Law, C.M.; Mullee, M.; Petrou, S.; Watkin, P.; Worsfold, S.; Yuen, H.M.; Stevenson, J. Language Ability after Early Detection of Permanent Childhood Hearing Impairment. N. Engl. J. Med. 2006, 354, 2131–2141. [Google Scholar] [CrossRef] [Green Version]
- Yoshinaga-Itano, C.; Sedey, A.L.; Wiggin, M.; Chung, W. Early Hearing Detection and Vocabulary of Children With Hearing Loss. Pediatrics 2017, 140, e20162964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pittman, L.; Stewart, E.; Willman, A.; Odgear, I.S. Word Recognition and Learning: Effects of Hearing Loss and Amplification Feature. Trends Hear. 2017, 21, 2331216517709597. [Google Scholar] [CrossRef] [PubMed]
- Qi, S.; Mitchell, R.E. Large-scale academic achievement testing of deaf and hard-of-hearing students: Past, present, and future. J. Deaf Stud. Deaf Educ. 2012, 17, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Tomblin, J.B.; Harrison, M.; Ambrose, S.E.; Walker, E.A.; Oleson, J.J.; Moeller, M.P. Outcomes of Children Who Are Hard of Hearing. Ear Hear. 2015, 36, 14S–23S. [Google Scholar] [CrossRef] [Green Version]
- Walker, E.A.; Sapp, C.; Dallapiazza, M.; Spratford, M.; McCreery, R.W.; Oleson, J.J. Language and reading outcomes in fourth-grade children with mild hearing loss compared to age-matched hearing peers. Lang. Speech Hear. Serv. Sch. 2020, 51, 17–28. [Google Scholar] [CrossRef]
- Uhler, K.M.; Hunter, S.K.; Gilley, P.M. Mismatched Response (MMR) predicts behavioral speech discrimination outcomes in infants with hearing loss and normal hearing. Infancy 2021, 26, 327–348. [Google Scholar] [CrossRef] [PubMed]
- Uhler, K.; Warner-Czyz, A.; Gifford, R. Pediatric minimum speech test battery. J. Am. Acad. Audiol. 2017, 28, 232–247. [Google Scholar] [CrossRef]
- Ching, T.Y.C.; Dillon, H.; Leigh, G.; Cupples, L. Learning from the Longitudinal Outcomes of Children with Hearing Impairment (LOCHI) study: Summary of 5-year findings and implications. Int. J. Audiol. 2017, 57, S105–S111. [Google Scholar] [CrossRef] [PubMed]
- Kuhl, P.K.; Conboy, B.T.; Padden, D.; Nelson, T.; Pruitt, J. Early Speech Perception and Later Language Development: Implications for the “Critical Period”. Lang. Learn. Dev. 2005, 1, 237–264. [Google Scholar] [CrossRef]
- Ching, T.Y.C.; Dillon, H.; Button, L.; Seeto, M.; van Buynder, P.; Marnane, V.; Cupples, L.; Leigh, G. Age at Intervention for Permanent Hearing Loss and 5-Year Language Outcomes. Pediatrics 2017, 140, e20164274. [Google Scholar] [CrossRef] [Green Version]
- Tomblin, J.B.; Oleson, J.J.; Ambrose, S.E.; Walker, E.; Moeller, M.P. The Influence of Hearing Aids on the Speech and Language Development of Children With Hearing Loss. JAMA Otolaryngol. Head Neck Surg. 2014, 104, 403–409. [Google Scholar] [CrossRef]
- Uhler, K.; Gifford, R.H. Current trends in pediatric cochlear implant candidate selection and postoperative follow-up. Am. Speech Hear. Assoc. Monogr. 2014, 23, 309–325. [Google Scholar] [CrossRef] [PubMed]
- Horn, D.L.; Houston, D.M.; Miyamoto, R.T. Speech discrimination skills in deaf infants before and after cochlear implantation. Audiol. Med. 2007, 5, 232–241. [Google Scholar] [CrossRef]
- Miyamoto, R.T.; Houston, D.M.; Kirk, K.I.; Perdew, A.E.; Svirsky, M.A. Language development in deaf infants following cochlear implantation. Acta Otolaryngol. 2003, 123, 241–244. [Google Scholar] [CrossRef]
- Phan, J.; Houson, D.; Ruffin, D.; Ting, J.; Holt, R.F. Factors Affecting Speech Discrimination in Children with Cochlear Implants: Evidence from Early Implanted Infants. J. Am. Acad. Audiol. 2016, 27, 480–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uhler, K.; Yoshinaga-Itano, C.; Gabbard, S.A.; Rothpletz, A.M.; Jenkins, H. Longitudinal infant speech perception in young cochlear implant users. J. Am. Acad. Audiol. 2011, 22, 129–142. [Google Scholar] [CrossRef]
- Aslin, R.N.; Smith, L.B. Perceptual Development. Annu. Rev. Psychol. 1998, 39, 435–473. [Google Scholar] [CrossRef]
- Holt, R.F.; Kirk, K.I.; Hay-McCutcheon, M. Assessing multimodal spoken word-in-sentence recognition in children with normal hearing and children with cochlear implants. J. Speech Lang. Hear. Res. 2011, 54, 632–657. [Google Scholar] [CrossRef]
- Newman, R.; Ratner, N.B.; Jusczyk, A.M.; Jusczyk, P.W.; Dow, K.A. Infants’ early ability to segment the conversational speech signal predicts later language development: A retrospective analysis. Dev. Psychol. 2006, 42, 643–655. [Google Scholar] [CrossRef] [Green Version]
- Tsao, F.M.; Liu, H.M.; Kuhl, P.K. Speech perception in infancy predicts language development in the second year of life: A longitudinal study. Child Dev. 2004, 75, 1067–1084. [Google Scholar] [CrossRef]
- Singh, L.; Reznick, J.; Xuehua, L. Infant Word Segmentation and Childhood Vocabulary Development: A Longitudinal Analysis. Dev. Sci. 2012, 15, 482–495. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.M.; Thompson, G.; Thompson, M. Auditory localization of infants as a function of reinforcement conditions. J. Speech Lang. Hear. Disord. 1975, 40, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Eilers, R.E.; Morse, P.A.; Gavin, W.J.; Oller, D.K. Discrimination of voice onset time in infancy. J. Acoust. Soc. Am. 1981, 70, 955–965. [Google Scholar] [CrossRef] [PubMed]
- Nozza, R.J. Infant speech-sound discrimination testing: Effects of stimulus intensity and procedural model on measures of performance. J. Acoust. Soc. Am. 1987, 81, 1928–1939. [Google Scholar] [CrossRef] [PubMed]
- Nozza, R.J.; Miller, S.L.; Rossman, R.N.; Bond, L.C. Reliability and validity of infant speech-sound discrimination-in-noise thresholds. J. Speech Hear. Res. 1991, 34, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Nozza, R.J. Thresholds are not enough: Understanding how infants’ Process. Speech has a role in how we manage hearing loss. In A Sound Foundation through Early Amplification; Phonak AG: Stäfa, Switzerland, 2000; pp. 47–54. Available online: https://www.phonakpro.com/content/dam/phonakpro/gc_hq/en/events/2016/international_pediatric_audiology_conference_atlanta/chapter_14_moodie_draft.pdf (accessed on 25 September 2021).
- Uhler, K.M.; Gifford, R.H.; Forster, J.E.; Anderson, M.; Tierney, E.; Claycomb, S.D.; Werner, L.A. Refining Stimulus Parameters in Assessing Infant Speech Perception Using Visual Reinforcement Infant Speech Discrimination in Infants with and without Hearing Loss: Presentation Level. J. Am. Acad. Audiol. 2017, 29, 847–854. [Google Scholar] [CrossRef]
- Uhler, K.M.; Baca, R.; Dudas, E.; Fredrickson, T. Refining Stimulus Parameters in Assessing Infant Speech Perception Using Visual Reinforcement Infant Speech Discrimination: Sensation Level. J. Am. Acad. Audiol. 2015, 26, 807–814. [Google Scholar] [CrossRef] [Green Version]
- Werker, J.F.; Shi, R.; Desjardins, R.; Pegg, J.E.; Polka, L.; Patterson, M. Three methods for testing infant speech perception. In Perceptual Development: Visual, Auditory, and Speech Perception in Infancy; Slater, A., Ed.; Psychology Press: New York, NY, USA, 1998; pp. 389–420. [Google Scholar]
- Eilers, R.E.; Wilson, W.R.; Moore, J.M. Developmental changes in speech discrimination in infants. J. Speech Hear. Res. 1977, 20, 766–780. [Google Scholar] [CrossRef]
- Moog, J.; Geers, A. Early Speech Perception Test; Central Institute for the Deaf: St. Louis, MO, USA, 1990. [Google Scholar]
- Ertmer, D.J.; Miller, C.M.; Quesenberry, J.K. The Open and Closed Set Test; Purdue University: West Lafayette, IN, USA, 2004. [Google Scholar]
- Werker, J.F.; Tees, R.C. Cross-language speech perception: Evidence for perceptual reorganization during the first year of life. Infant Behav. Dev. 1984, 7, 49–63. [Google Scholar] [CrossRef]
- Kuhl, P.K.; Williams, K.A.; Lacerda, F.; Stevens, B.; Lindblom, K.N. Linguistic Experience Alters Phonetic Perception in Infants by 6 months of Age. Science 1992, 255, 606–608. [Google Scholar] [CrossRef]
- Kuhl, P.K.; Conboy, B.T.; Coffey-Corina, S.; Padden, D.; Rivera-Gaxiola, M.; Nelson, T. Phonetic learning as a pathway to language: New data and native language magnet theory expanded (NLM-e). Philos. Trans. R. Soc. B Biol. Sci. 2008, 363, 979–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strange, W.; Jenkins, J.J. Role of linguistic experience in the perception of speech. In Perception and Experience; Pick, J.H.D., Pic, H.J., Eds.; Plenum: New York, NY, USA, 1978. [Google Scholar]
- Nozza, R.J.; Wilson, W.R. Masked and unmasked pure-tone thresholds of infants and adults: Development of auditory frequency selectivity and sensitivity. J. Speech Hear. Res. 1984, 27, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Martinez, A.; Eisenberg, L.; Boothroyd, A.; Visser-Dumont, L. Assessing speech pattern contrast perception in infants: Early results on VRASPAC. Otol. Neurotol. 2008, 29, 183–188. [Google Scholar] [CrossRef] [Green Version]
- Fredrickson, T. Visual Reinforcement Infant Speech Discrimination: Developing a Method of Performance Analysis. Ph.D. Thesis, University of Colorado Boulder, Boulder, CO, USA, 2010. [Google Scholar]
- Boothroyd, A. Speech perception tests and hearing impaired children. In Profound Deafness and Speech Communication; Plant, G., Spens, K.E., Eds.; Whurr: London, UK, 1995; pp. 345–371. [Google Scholar]
- Stika, C.J.; Eisenberg, L.S.; Johnson, K.C.; Henning, S.C.; Colson, B.G.; Ganguly, D.H.; DesJardin, J.L. Developmental outcomes of early identified children who are hard of hearing at 12 to 18months of age. Early Hum. Dev. 2015, 91, 47–55. [Google Scholar] [CrossRef] [Green Version]
- Schauwers, K.; Gillis, S.; Daemers, K.; de Beukelaer, C.; Govaerts, P.J. Cochlear Implantation Between 5 and 20 months of Age: The Onset of Babbling and the Audiologic Outcome. Otol. Neurotol. 2004, 25, 263–270. [Google Scholar] [CrossRef] [Green Version]
- Govaerts, P.J.; Daemers, K.; Yperman, M.; de Beukelaer, C.; de Saegher, G.; de Ceulaer, G. Auditory speech sounds evaluation (A§E®): A new test to assess detection, discrimination, and identification in hearing impairment. Cochlear Implants Int. 2006, 7, 97–106. [Google Scholar] [CrossRef]
- Houston, D.M.; Pisoni, D.B.; Kirk, K.I.; Ying, E.A.; Miyamoto, R.T. Speech perception skills of deaf infants following cochlear implantation: A first report. Int. J. Pediatr. Otorhinolaryngol. 2003, 67, 479–495. [Google Scholar] [CrossRef] [Green Version]
- Cristia, A.; Seidl, A.; Singh, L.; Houston, D. Test–Retest Reliability in Infant Speech Perception Tasks. Infancy 2016, 21, 648–667. [Google Scholar] [CrossRef]
- American Academy of Audiology (AAA) Task Force on Pediatric Amplification. American Academy of Audiology Clinical Practice Guidelines Pediatric Amplification American Academy of Audiology Clinical Practice Guidelines; American Academy of Audiology: Reston, VA, USA, 2011. [Google Scholar]
- Eisenberg, L.S.; Martinez, A.S.; Boothroyd, A. Assessing auditory capabilities in young children. Int. J. Pediatr. Otorhinolaryngol. 2007, 71, 1339–1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macmillan, N.; Creelman, C. Detection Theory: A User’s Guide; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2005. [Google Scholar]
- McArdle, R.; Hnath-Chisolm, T. Speech Audiometry. In Handbook of Clinical Audiology, 6th ed.; Katz, J., Medwetsky, L., Burkard, R., Hood, L., Eds.; Lippincott Williams and Wilkins: Baltimore, MD, USA, 2009. [Google Scholar]
- McCreery, R.W.; Walker, E.A.; Spratford, M.; Bentler, R.; Holte, L.; Roush, P.; Oleson, J.; van Buren, J.; Moeller, M.P. Longitidinal predictors of aided speech audibility in infants and children. Ear Hear. 2015, 36, 24S–37S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boothroyd, A. Auditory Perception of Speech Contrasts by Subjects with Sensorineural Hearing Loss. J. Speech Hear. Res. 1984, 27, 134–144. [Google Scholar] [CrossRef]
- van Wieringen, A.; Wouters, J. Natural vowel and consonant recognition by Laura Cochlear implantees. Ear Hear. 1999, 20, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Toro, J.M.; Nespor, M.; Mehler, J.; Bonatti, L.L. Finding words and rules in a speech stream: Functional differences between vowels and consonants: Research article. Psychol. Sci. 2008, 19, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Scollie, S.; Glista, D.; Seto, J.; Dunn, A.; Schuett, B.; Hawkins, M.; Pourmand, N.; Parsa, V. Fitting Frequency-Lowering Signal Processing Applying the American Academy of Audiology Pediatric Amplification Guideline: Updates and Protocols. J. Am. Acad. Audiol. 2016, 27, 219–236. [Google Scholar] [CrossRef] [PubMed]
- Scollie, S. Children’s speech Frecognition scores: The speech intelligibility index and proficiency factors for age and hearing level. Ear Hear. 2008, 29, 543–556. [Google Scholar] [CrossRef] [PubMed]
- McCreery, R.W.; Stelmachowicz, P.G. Audibility-based predictions of speech recognition for children and adults with normal hearing. J. Acoust. Soc. Am. 2011, 130, 4070–4081. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Demographic | CHH | CNH | Statistical Test | p-Value |
|---|---|---|---|---|
| (N = 57) | (N = 70) | |||
| Male | 28 (49.1%) | 38 (54.3%) | Chi-squared | 0.69 |
| Age 9 months or Greater | 30 (52.6%) | 28 (40.0%) | Chi-squared | 0.21 |
| Hearing Age 9 months or Greater | 14 (24.6%) | 28 (40.0%) | Chi-squared | 0.1 |
| Age Category: | Fisher’s exact | 0.006 | ||
| 6 to 7 months | 7 (12.3%) | 19 (27.1%) | ||
| 8 to 10 months | 32 (56.1%) | 42 (60.0%) | ||
| 11 to 13 months | 13 (22.8%) | 3 (4.3%) | ||
| 14 to 17 months | 5 (8.8%) | 5 (7.1%) | ||
| Age < 5 months | 0 (0.0%) | 1 (1.4%) | ||
| PTA Category: | ||||
| Normal (0–15 dB HL) | 0 (0.0%) | 70 (100.0%) | ||
| Mild (16–40 dB HL) | 39 (68.4%) | 0 (0.0%) | ||
| Moderate+ (≥1 dB HL) | 18 (31.5%) | 0 (0.0%) | ||
| Hearing Age Category: | Fisher’s exact | <0.001 | ||
| 0 to 5 months | 19 (33.3%) | 1 (1.4%) | ||
| 6 to 7 months | 22 (38.6%) | 19 (27.1%) | ||
| 8 to 10 months | 11 (19.3%) | 42 (60.0%) | ||
| 11 to 13 months | 5 (8.8%) | 3 (4.3%) | ||
| 14 to 17 months | 0 (0.0%) | 5 (7.1%) | ||
| PTA: | 41.3 (14.6) | 15.0 (0.0) | ||
| Missing | 2 (3.51%) | 0 (0.0%) | ||
| Age at CHT in months (M, SD): | 10.2 (2.34) | 9.16 (2.26) | t-test | 0.02 |
| Hearing Age in months (M, SD): | 7.05 (2.49) | 9.16 (2.26) | t-test | <0.001 |
| Missing | 0 (0.0%) | 70 (100.0%) |
| Mean (SD/%) | Median (Min, Max) | |
|---|---|---|
| Age at Hearing Aid Fit | 2.92 months (1.24) | 2.69 months (1.12, 8.03) |
| Datalogging | 6.52 h (4.12) | 6.55 h (0.00, 16.00) |
| Missing | 9 (15.8%) | |
| Aided SII: | ||
| 50 dBA | 0.73 (0.18) | 0.74 (0.21, 0.98) |
| Missing | 1 (1.75%) | |
| CHH | CNH | ||||||
|---|---|---|---|---|---|---|---|
| Contrast | Level dBA SPL | Number of Participants | % of Participants | Mean Performance in d’ (S.D.) | Number of Participants | % of Participants | Mean Performance in d’ (S.D.) |
| /a-i/ | 50 | 20 | 37 | 1.94 (0.41) | 21 | 31 | 1.87 (0.46) |
| 60 | 9 | 17 | 1.94 (0.46) | 25 | 37 | 2.02 (0.54) | |
| 70 | 11 | 20 | 1.66 (0.34) | 6 | 9 | 1.80 (0.32) | |
| Did not qualify | 10 | 19 | 11 | 16 | |||
| Did not qualify, some missing | 4 | 7 | 4 | 6 | |||
| Completed Testing | 54 | 67 | |||||
| Did not test | 3 | 3 | |||||
| /ba-da/ | 50 | 9 | 16 | 1.88 (0.61) | 13 | 21 | 1.90 (0.62) |
| 60 | 10 | 18 | 1.77 (0.60) | 8 | 13 | 1.98 (0.58) | |
| 70 | 12 | 22 | 1.65 (0.31) | 13 | 21 | 1.97 (0.63) | |
| Did not qualify | 20 | 36 | 25 | 41 | |||
| Did not qualify, incomplete testing | 4 | 7 | 2 | 3 | |||
| Completed Testing | 55 | 61 | |||||
| Did not test | 2 | 9 | |||||
| Covariate | Estimate | 95% CI | Wald Statistic (W) | p Value |
|---|---|---|---|---|
| Model 1-Outcome: d’ /ba-da/ for Overall Sample | ||||
| Intercept | 0.28 | (−0.32, 0.88) | 0.90 | 0.37 |
| Hearing Age at Test | 0.04 | (−0.02, 0.1) | 1.33 | 0.18 |
| Mild HL (vs. Normal) | 0.07 | (−0.24, 0.38) | 0.46 | 0.65 |
| Mod+ HL (vs. Normal) | −0.02 | (−0.42, 0.38) | −0.08 | 0.94 |
| 60 Intensity (vs. 50 Intensity) | 0.08 | (−0.15, 0.30) | 0.66 | 0.51 |
| 70 Intensity (vs. 50 Intensity) | 0.36 | (0.13, 0.58) | 3.09 | 0.002 * |
| Model 2-Outcome: d’ /a-i/ for Overall Sample | ||||
| Intercept | 1.31 | (0.81, 1.80) | 5.21 | <0.001 |
| Hearing Age at Test | −0.022 | (−0.07, 0.02) | −0.97 | 0.33 |
| Mild HL (vs. Normal) | −0.052 | (−0.38, 0.28) | −0.31 | 0.76 |
| Mod + HL (vs. Normal) | −0.45 | (−0.86, −0.04) | −2.14 | 0.03 * |
| 60 Intensity (vs. 50 Intensity) | 0.149 | (−0.09, 0.39) | 1.21 | 0.23 |
| 70 Intensity (vs. 50 Intensity) | 0.184 | (−0.06, 0.43) | 1.47 | 0.14 |
| Covariate | Estimate | 95% CI | Wald Statistic | p Value |
|---|---|---|---|---|
| Model 1HL-Outcome: d’ /ba-da/ for HL Only | ||||
| Intercept | −0.43 | (−1.59, 0.73) | −0.73 | 0.47 |
| Hearing Age at Test | 0.03 | (−0.06, 0.12) | 0.61 | 0.55 |
| Mod+ HL (vs. Mild HL) | 0.15 | (−0.30, 0.61) | 0.66 | 0.51 |
| 60 Intensity (vs. 50 Intensity) | 0.09 | (−0.24, 0.43) | 0.54 | 0.59 |
| 70 Intensity (vs. 50 Intensity) | 0.47 | (0.17, 0.77) | 3.08 | 0.002 * |
| Aided SII at 50 dB | 1.01 | (−0.17, 2.19) | 1.67 | 0.09 |
| Model 2HL-Outcome: d’ /a-i/ for HL Only | ||||
| Intercept | 1.15 | (0.30, 1.99) | 2.65 | 0.01 |
| Hearing Age at Test | −0.05 | (−0.11, 0.01) | −1.61 | 0.11 |
| Mod+ HL (vs. Mild HL) | −0.24 | (−0.66, 0.18) | −1.11 | 0.27 |
| 60 Intensity (vs. 50 Intensity) | −0.21 | (−0.57, 0.16) | −1.10 | 0.27 |
| 70 Intensity (vs. 50 Intensity) | 0.08 | (−0.26, 0.42) | 0.46 | 0.64 |
| Aided SII at 50 dB | 0.41 | (−0.63, 1.45) | 0.77 | 0.44 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uhler, K.M.; Kaizer, A.M.; Walker, K.A.; Gilley, P.M. Relationship between Behavioral Infant Speech Perception and Hearing Age for Children with Hearing Loss. J. Clin. Med. 2021, 10, 4566. https://doi.org/10.3390/jcm10194566
Uhler KM, Kaizer AM, Walker KA, Gilley PM. Relationship between Behavioral Infant Speech Perception and Hearing Age for Children with Hearing Loss. Journal of Clinical Medicine. 2021; 10(19):4566. https://doi.org/10.3390/jcm10194566
Chicago/Turabian StyleUhler, Kristin M., Alexander M. Kaizer, Kerry A. Walker, and Phillip M. Gilley. 2021. "Relationship between Behavioral Infant Speech Perception and Hearing Age for Children with Hearing Loss" Journal of Clinical Medicine 10, no. 19: 4566. https://doi.org/10.3390/jcm10194566
APA StyleUhler, K. M., Kaizer, A. M., Walker, K. A., & Gilley, P. M. (2021). Relationship between Behavioral Infant Speech Perception and Hearing Age for Children with Hearing Loss. Journal of Clinical Medicine, 10(19), 4566. https://doi.org/10.3390/jcm10194566