Value of Perioperative Chest X-ray for the Prediction of Sternal Wound Complications after Cardiac Surgery in High-Risk Patients: A “Work in Progress” Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Institutional Protocol
2.3. Study Design
2.4. Inclusion and Exclusion Criteria
2.5. Statistical Analysis
3. Results
4. Discussion
Study Limitation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Phoon, P.H.Y.; Hwang, N.C. Deep sternal wound infection: Diagnosis, treatment and prevention. J. Cardiothorac. Vasc. Anesth. 2020, 34, 1602–1613. [Google Scholar] [CrossRef] [PubMed]
- Baillot, R.; Cloutier, D.; Montalin, L.; Côté, L.; Lellouche, F.; Houde, C.; Gaudreau, G.; Voisine, P. Impact of deep sternal wound infection management with vacuum-assisted closure therapy followed by sternal osteosynthesis: A 15-year review of 23,499 sternotomies. Eur. J. Cardiothorac. Surg. 2010, 37, 880–8807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sears, E.D.; Wu, L.; Waljee, J.F.; Momoh, A.O.; Zhong, L.; Chung, K.C. The Impact of Deep Sternal Wound Infection on Mortality and Resource Utilization: A Population-based Study. World J. Surg. 2016, 40, 2673–2680. [Google Scholar] [CrossRef] [PubMed]
- Filsoufi, F.; Castillo, J.G.; Rahmanian, P.B.; Broumand, S.R.; Silvay, G.; Carpentier, A.; Adams, D.H. Epidemiology of deep sternal wound infection in cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2009, 23, 488–494. [Google Scholar] [CrossRef] [Green Version]
- Graf, K.; Ott, E.; Vonberg, R.P.; Kuehn, C.; Haverich, A.; Chaberny, I.F. Economic aspects of deep sternal wound infections. Eur. J. Cardiothorac. Surg. 2010, 37, 893–896. [Google Scholar] [CrossRef]
- Balachandran, S.; Lee, A.; Denehy, L.; Lin, K.Y.; Royse, A.; Royse, C.; El-Ansary, D. Risk Factors for Sternal Complications After Cardiac Operations: A Systematic Review. Ann. Thorac. Surg. 2016, 102, 2109–2117. [Google Scholar] [CrossRef] [Green Version]
- Losanoff, J.E.; Jones, J.W.; Richman, B.W. Primary closure of median sternotomy: Techniques and principles. Cardiovasc. Surg. 2002, 10, 102–110. [Google Scholar] [CrossRef]
- Smith, J.D.; Stowell, J.T.; Martínez-Jiménez, S.; Desouches, S.L.; Rosado-de-Christenson, M.L.; Jain, K.K.; Magalski, A. Evaluation after Orthotopic Heart Transplant: What the Radiologist Should Know. Radiogr. 2019, 39, 321–343. [Google Scholar] [CrossRef]
- Hayward, R.H.; Knight, W.L.; Reiter, C.G. Sternal dehiscence. Early detection by radiography. J. Thorac. Cardiovasc. Surg. 1994, 108, 616–619. [Google Scholar] [CrossRef]
- Zeitani, J.; Penta de Peppo, A.; Moscarelli, M.; Guerrieri Wolf, L.; Scafuri, A.; Nardi, P.; Nanni, F.; Di Marzio, E.; De Vico, P.; Chiariello, L. Influence of sternal size and inadvertent paramedian sternotomy on stability of the closure site: A clinical and mechanical study. J. Thorac. Cardiovasc. Surg. 2006, 132, 38–42. [Google Scholar] [CrossRef] [Green Version]
- Zeitani, J.; Penta de Peppo, A.; Bianco, A.; Nanni, F.; Scafuri, A.; Bertoldo, F.; Salvati, A.; Nardella, S.; Chiariello, L. Performance of a novel sternal synthesis device after median and faulty sternotomy: Mechanical test and early clinical experience. Ann. Thorac. Surg. 2008, 85, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Listewnik, M.J.; Jędrzejczak, T.; Majer, K.; Szylińska, A.; Mikołajczyk, A.; Mokrzycki, K.; Górka, E.; Brykczyński, M. Complications in cardiac surgery: An analysis of factors contributing to sternal dehiscence in patients who underwent surgery between 2010 and 2014 and a comparison with the 1990–2009 cohort. Adv. Clin. Exp. Med. 2019, 28, 913–922. [Google Scholar] [CrossRef] [Green Version]
- Cohen, A.; Katz, M.; Katz, R.; Hauptman, E.; Schachner, A. Chronic obstructive pulmonary disease in patients undergoing coronary artery bypass grafting. J. Thorac. Cardiovasc. Surg. 1995, 109, 574–581. [Google Scholar] [CrossRef] [Green Version]
- Bryan, A.J.; Lamarra, M.; Angelini, G.D.; West, R.R.; Breckenridge, I.M. Median sternotomy wound dehiscence: A retrospective case control study of risk factors and outcome. J. R. Coll. Surg. Edinb. 1992, 37, 305–308. [Google Scholar]
- Park, J.; Lee, C.H.; Lee, Y.J.; Park, J.S.; Cho, Y.J.; Lee, J.H.; Lee, C.T.; Yoon, H.I. Longitudinal changes in lung hyperinflation in COPD. Int. J. Chron. Obstr. Pulm. Dis. 2017, 12, 501–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Washko, G.R. Diagnostic imaging in COPD. Semin. Respir. Crit. Care Med. 2010, 31, 276–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangram, A.J.; Horan, T.C.; Pearson, M.L.; Silver, L.C.; Jarvis, W.R. Guideline for Prevention of Surgical Site Infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. Am. J. Infect. Control 1999, 27, 97–132. [Google Scholar] [CrossRef]
- Robicsek, F.; Daugherty, H.K.; Cook, J.W. The prevention and treatment of sternum separation following open-heart surgery. J. Thorac. Cardiovasc. Surg. 1977, 73, 267–268. [Google Scholar] [CrossRef]
- Gatti, G.; Perrotti, A.; Reichart, D.; Maschietto, L.; Onorati, F.; Chocron, S.; Dalén, M.; Svenarud, P.; Faggian, G.; Santarpino, G.; et al. Glycated Hemoglobin and Risk of Sternal Wound Infection After Isolated Coronary Surgery. Circ. J. 2016, 81, 36–43. [Google Scholar] [CrossRef] [Green Version]
- Jensen, M.D.; Ryan, D.H. American College of Cardiology/American Heart Association Task Force on Practice Guidelines; Obesity Society. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J. Am. Coll. Cardiol. 2014, 63 Pt B, 2985–3023. [Google Scholar] [CrossRef] [Green Version]
- Semper, O.; Leclerc, Y.; Cartier, R.; Carrier, M. Médiastinite post-sternotomie: Stratégie de traitement [Post-sternotomy mediastinitis: Strategy of treatment]. Ann. Chir. 1991, 45, 770–773. [Google Scholar] [PubMed]
- Newman, L.S.; Szczukowski, L.C.; Bain, R.P.; Perlino, C.A. Suppurative mediastinitis after open heart surgery. A case control study of risk factors. Chest 1988, 94, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Kirbas, A.; Celik, S.; Gurer, O.; Yildiz, Y.; Isik, O. Sternal wrapping for the prevention of sternal morbidity in elderly osteoporotic patients undergoing median sternotomy. Tex. Heart Inst. J. 2011, 38, 132–136. [Google Scholar] [PubMed]
- Nishida, H.; Grooters, R.K.; Soltanzadeh, H.; Thieman, K.C.; Schneider, R.F.; Kim, W.P. Discriminate use of electrocautery on the median sternotomy incision. A 0.16% wound infection rate. J. Thorac. Cardiovasc. Surg. 1993, 101, 488–494. [Google Scholar] [CrossRef]
- Copeland, M.; Senkowski, C.; Ulcickas, M.; Mendelson, M.; Griepp, R.B. Breast size as a risk factor for sternal wound complications following cardiac surgery. Arch. Surg. 1994, 129, 757–759. [Google Scholar] [CrossRef]
- Casha, A.R.; Manché, A.; Gatt, R.; Duca, E.; Gauci, M.; Schembri-Wismayer, P.; Camilleri-Podesta, M.T.; Grima, J.N. Mechanism of sternotomy dehiscence. Interact. Cardiovasc. Thorac. Surg. 2014, 19, 617–621. [Google Scholar] [CrossRef] [Green Version]
- Casha, A.R.; Gauci, M.; Yang, L.; Saleh, M.; Kay, P.H.; Cooper, G.J. Fatigue testing median sternotomy closures. Eur. J. Cardiothorac. Surg. 2001, 19, 249–253. [Google Scholar] [CrossRef] [Green Version]
- Cohen, D.J.; Griffin, L.V. A biomechanical comparison of three sternotomy closure techniques. Ann. Thorac. Surg. 2002, 73, 563–568. [Google Scholar] [CrossRef] [Green Version]
- Matros, E.; Aranki, S.F.; Bayer, L.R.; McGurk, S.; Neuwalder, J.; Orgill, D.P. Reduction in incidence of deep sternal wound infections: Random or real? J. Thorac. Cardiovasc. Surg. 2010, 139, 680–685. [Google Scholar] [CrossRef] [Green Version]
- Casha, A.R.; Manché, A.; Gauci, M.; Camilleri-Podesta, M.T.; Schembri-Wismayer, P.; Sant, Z.; Gatt, R.; Grima, J.N. Placement of trans-sternal wires according to an ellipsoid pressure vessel model of sternal forces. Interact. Cardiovasc. Thorac. Surg. 2012, 14, 283–287. [Google Scholar] [CrossRef]
- Nenna, A.; Nappi, F.; Dougal, J.; Satriano, U.; Chello, C.; Mastroianni, C.; Lusini, M.; Chello, M.; Spadaccio, C. Sternal wound closure in the current era: The need of a tailored approach. Gen. Thorac. Cardiovasc. Surg. 2019, 67, 907–916. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.A.; Goodson, W.H.; Hopf, H.W.; Hunt, T.K. Cigarette smoking decreases tissue oxygen. Arch. Surg. 1991, 126, 1131–1134. [Google Scholar] [CrossRef] [PubMed]
- McGregor, W.E.; Trumble, D.R.; Magovern, J.A. Mechanical analysis of midline sternotomy wound closure. J. Thorac. Cardiovasc. Surg. 1999, 117, 1144–1150. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Age | 67.0 ± 11.5 |
| Sex (Female) | 142 (16.7%) |
| EuroSCORE-II | 3.5 ± 2.2 |
| LVEF (%) | 47.3 ± 13.0 |
| Diabetes Mellitus | 185 (21.8%) |
| Hb1Ac > 53 mmol/mol | 105 (12.4%) |
| COPD | 25 (2.9%) |
| Obesity | 213 (25.1%) |
| BMI (Kg/m2) | 27.3 ± 4.3 |
| Chronic Kidney Disease | 261 (30.7%) |
| Preoperative dialysis | 41 (4.8%) |
| eGFR (ml/min/m2) | 79.5 ± 18.8 |
| Peripheral arteriopathy | 122 (14.4%) |
| Redo | 3 (0.5%) |
| NYHA class | 2.4 ± 0.6 |
| BIMA | 3 (0.5%) |
| SIMA | 250 (29.5%) |
| CABG | 253 (29.8%) |
| Valve surgery | 548 (64.5%) |
| Other type of cardiac surgery * | 48 (5.7%) |
| ACC time (mins) | 81.5 ± 40.2 |
| CPB time (mins) | 110.0 ± 52.6 |
| Transfusion > 4 Units RPC | 178 (21.0%) |
| Re-exploration for bleeding | 33 (3.9%) |
| Prolonged ventilation (>96 h) | 72 (8.5%) |
| Postoperative tracheostomy | 12 (1.4%) |
| Postoperative CPR | 7 (0.8%) |
| Variable | SD (75 Patients) | No SD (774 Patients) | p | MG1-SSI (58 Patients) | No MG1-SSI (791 Patients) | p |
|---|---|---|---|---|---|---|
| NPWT | 72 (96%) | 0 (-) | <0.001 | 47 (81%) | 25 (3.1%) | <0.001 |
| Surgical debridement | 11 (14%) | 0 (-) | <0.001 | 11 (19%) | 0 (-) | <0.001 |
| LOS | 12.2 ± 17.5 | 6.1 ± 3.4 | <0.001 | 13.2 ± 18.1 | 8.3 ± 11.4 | 0.0027 |
| Death | 2 (2.6%) | 17 (2.2%) | 0.6822 | 2 (3.4%) | 17 (2.2%) | 0.3771 |
| Variable | SD (75 Patients) | No SD (774 Patients) | p | MG1-SSI (58 Patients) | No MG1-SSI (791 Patients) | p |
|---|---|---|---|---|---|---|
| Age | 68.0 ± 11.9 | 66.9 ± 11.5 | 0.391 | 69.2 ± 9.9 | 66.8 ± 11.6 | 0.137 |
| Sex (Female) | 47 (62.7%) | 660 (85.3%) | <0.001 | 22 (37.9%) | 120 (15.2%) | <0.001 |
| EuroSCORE-II | 4.7 ± 3.6 | 3.4 ± 2.0 | <0.001 | 4.0 ± 3.5 | 3.5 ± 2.1 | 0.088 |
| LVEF (%) | 47.1 ± 14.9 | 47.3 ± 12.8 | 0.907 | 46.7 ± 16.6 | 47.4 ± 12.7 | 0.707 |
| Diabetes Mellitus | 29 (38.7%) | 156 (20.2%) | <0.001 | 23 (39.7%) | 162 (20.5%) | 0.001 |
| Hb1Ac > 53 mmol/mol | 11 (14.7%) | 94 (12.1%) | 0.526 | 11 (19.0%) | 94 (11.9%) | 0.114 |
| COPD | 13 (17.3%) | 12 (1.6%) | <0.001 | 11 (19.0%) | 14 (1.8%) | <0.001 |
| Obesity | 27 (36.0%) | 186 (24.0%) | 0.022 | 20 (34.5%) | 193 (24.4%) | 0.087 |
| BMI (Kg/m2) | 28.4 ± 4.3 | 27.2 ± 4.3 | 0.016 | 28.3 ± 4.3 | 27.2 ± 4.3 | 0.055 |
| Chronic Kidney Disease | 23 (30.7%) | 238 (30.7%) | 0.988 | 23 (39.7%) | 238 (30.1%) | 0.127 |
| Preoperative dialysis | 6 (8.0%) | 35 (4.5%) | 0.180 | 6 (10.3%) | 35 (4.4%) | 0.042 |
| eGFR (ml/min/m2) | 67.4 ± 25.7 | 80.7 ± 17.6 | <0.001 | 65.2 ± 25.7 | 80.6 ± 17.8 | <0.001 |
| Peripheral arteriopathy | 18 (24.0%) | 104 (13.4%) | 0.013 | 18 (31.0%) | 104 (13.1%) | <0.001 |
| Redo | 3 (4.0%) | 0 (-) | <0.001 | 3 (5.2%) | 0 (-) | <.001 |
| NYHA class | 2.3 ± 0.7 | 2.5 ± 0.6 | 0.076 | 2.4 ± 0.7 | 2.4 ± 0.6 | 0.691 |
| BIMA | 3 (4.0%) | 0 (-) | <0.001 | 3 (5.2%) | 0 (-) | <0.001 |
| SIMA | 31 (41.3%) | 219 (28.3%) | 0.018 | 31 (53.4%) | 219 (27.7%) | <0.001 |
| CABG | 34 (45.3%) | 219 (28.3%) | 0.002 | 34 (58.6%) | 219 (27.7%) | <0.001 |
| Valve surgery | 38 (50.7%) | 510 (65.9%) | 0.008 | 21 (36.2%) | 527 (66.6%) | <0.001 |
| Other type of cardiac surgery * | 3 (4.0%) | 45 (5.8%) | 0.516 | 3 (5.2%) | 45 (5.7%) | 0.869 |
| ACC time (mins) | 67.1 ± 33.8 | 82.9 ± 40.5 | 0.001 | 67.4 ± 36.1 | 82.6 ± 40.3 | 0.005 |
| CPB time (mins) | 101.9 ± 52.5 | 110.8 ± 52.6 | 0.163 | 104.6 ± 57.6 | 110.4 ± 52.2 | 0.416 |
| Transfusion > 4 Units RPC | 17 (22.7%) | 161 (20.8%) | 0.705 | 13 (22.4%) | 165 (20.9%) | 0.779 |
| Re-exploration for bleeding | 4 (5.3%) | 29 (3.7%) | 0.497 | 4 (6.9%) | 29 (3.7%) | 0.219 |
| Prolonged ventilation (>96 h) | 6 (8.0%) | 66 (8.5%) | 0.876 | 6 (10.3%) | 66 (8.3%) | 0.598 |
| Postoperative tracheostomy | 2 (2.7%) | 10 (1.3%) | 0.336 | 2 (3.4%) | 10 (1.3%) | 0.174 |
| Postoperative CPR | 2 (2.7%) | 5 (0.6%) | 0.065 | 2 (3.4%) | 5 (0.6%) | 0.022 |
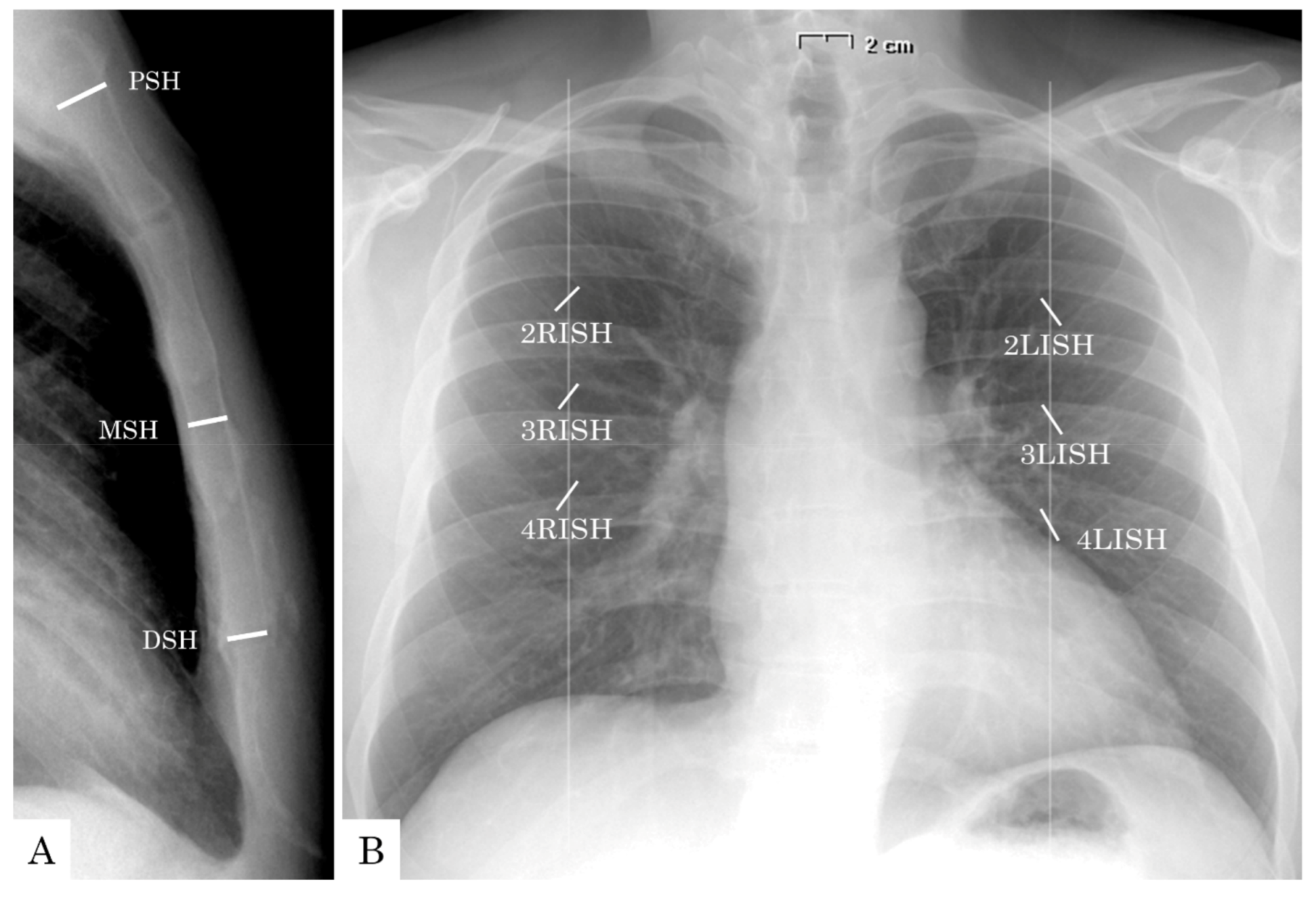
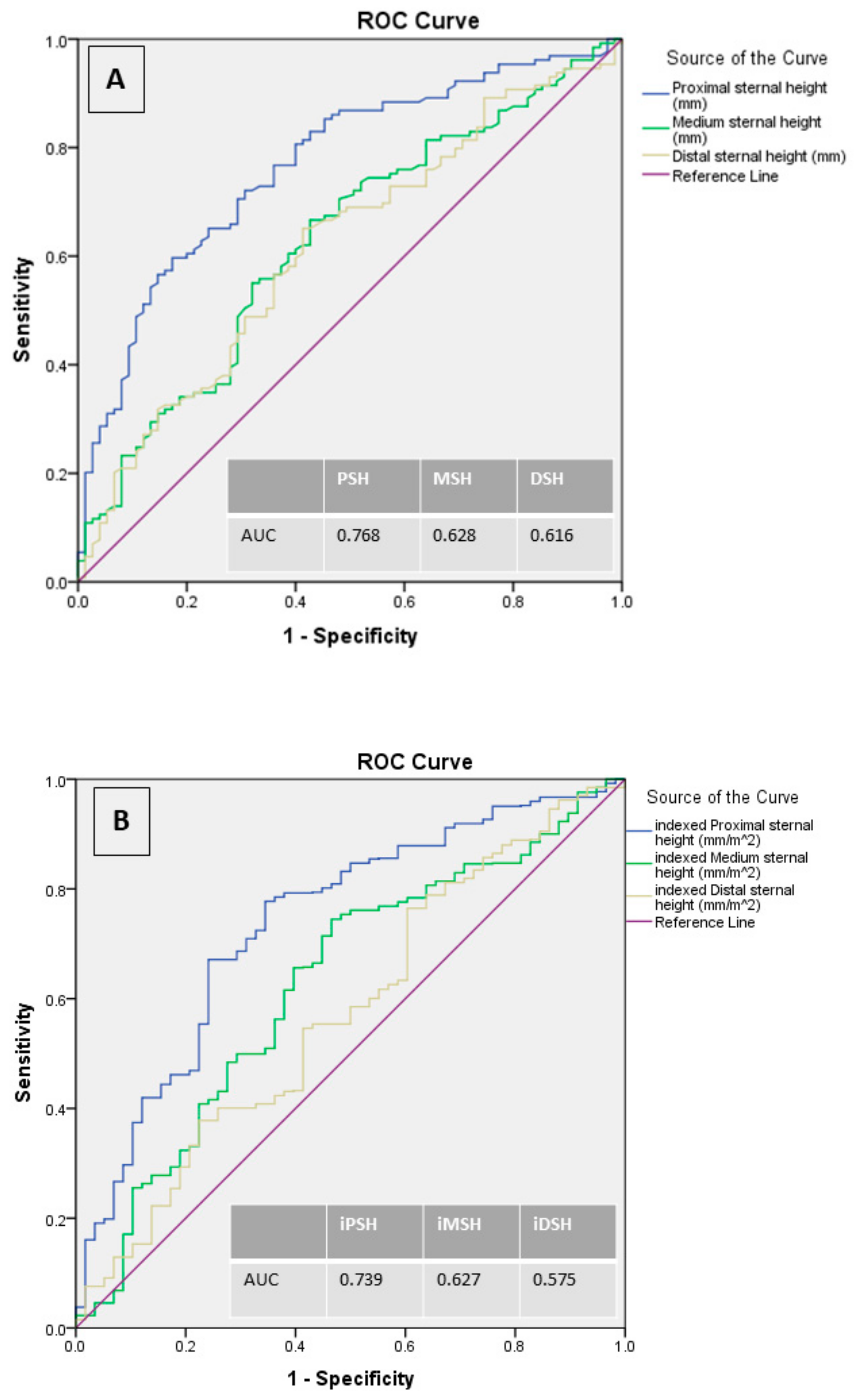
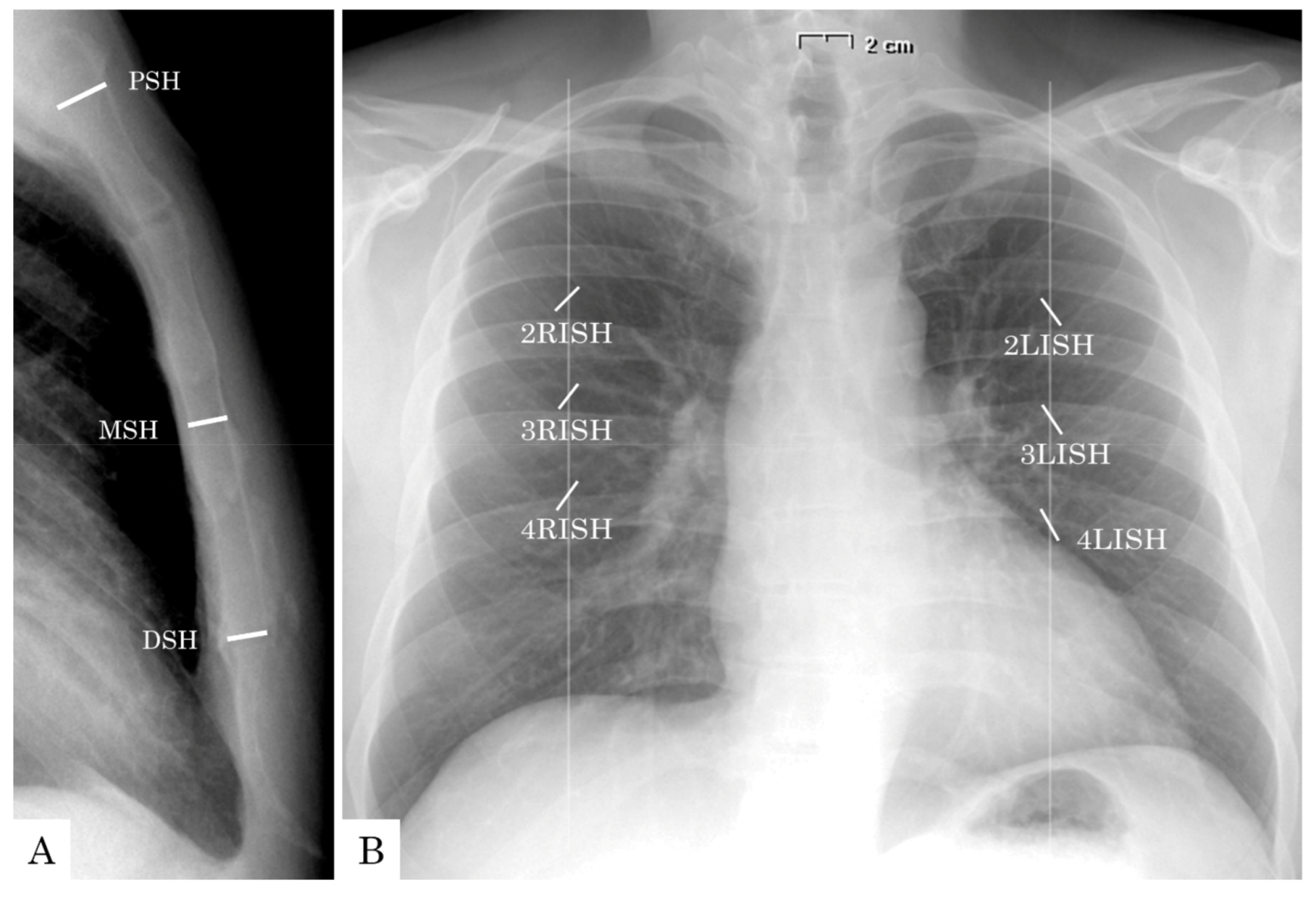
| PSH (mm) | 10.8 ± 1.7 | 12.7 ± 1.9 | <0.001 | 10.8 ± 1.7 | 12.6 ± 1.9 | <0.001 |
| MSH (mm) | 9.5 ± 1.7 | 10.3 ± 1.9 | <0.001 | 9.4 ± 1.8 | 10.3 ± 1.9 | 0.001 |
| DSH (mm) | 9.5 ± 1.8 | 10.3 ± 2.1 | 0.002 | 9.6 ± 1.9 | 10.3 ± 2.2 | 0.016 |
| iPSH (mm/m2) | 5.8 ± 0.9 | 6.7 ± 1.1 | <0.001 | 5.7 ± 1.0 | 6.6 ± 1.1 | <0.001 |
| iMSH (mm/m2) | 5.1 ± 1.0 | 5.4 ± 1.0 | 0.005 | 5.0 ± 1.0 | 5.4 ± 0.9 | 0.003 |
| iDSH (mm/m2) | 5.1 ± 1.1 | 5.4 ± 1.1 | 0.021 | 5.1 ± 1.1 | 5.4 ± 1.1 | 0.059 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ardigò, A.; Francica, A.; Veraldi, G.F.; Tropea, I.; Tonelli, F.; Rossetti, C.; Onorati, F.; Faggian, G. Value of Perioperative Chest X-ray for the Prediction of Sternal Wound Complications after Cardiac Surgery in High-Risk Patients: A “Work in Progress” Analysis. J. Clin. Med. 2021, 10, 207. https://doi.org/10.3390/jcm10020207
Ardigò A, Francica A, Veraldi GF, Tropea I, Tonelli F, Rossetti C, Onorati F, Faggian G. Value of Perioperative Chest X-ray for the Prediction of Sternal Wound Complications after Cardiac Surgery in High-Risk Patients: A “Work in Progress” Analysis. Journal of Clinical Medicine. 2021; 10(2):207. https://doi.org/10.3390/jcm10020207
Chicago/Turabian StyleArdigò, Andrea, Alessandra Francica, Gian Franco Veraldi, Ilaria Tropea, Filippo Tonelli, Cecilia Rossetti, Francesco Onorati, and Giuseppe Faggian. 2021. "Value of Perioperative Chest X-ray for the Prediction of Sternal Wound Complications after Cardiac Surgery in High-Risk Patients: A “Work in Progress” Analysis" Journal of Clinical Medicine 10, no. 2: 207. https://doi.org/10.3390/jcm10020207