
Multimodal Therapeutic Approach in Women with High Risk of Metabolic Syndrome—A Single Group One Center Pre-Post Study


Abstract
:1. Introduction
2. Materials and Methods
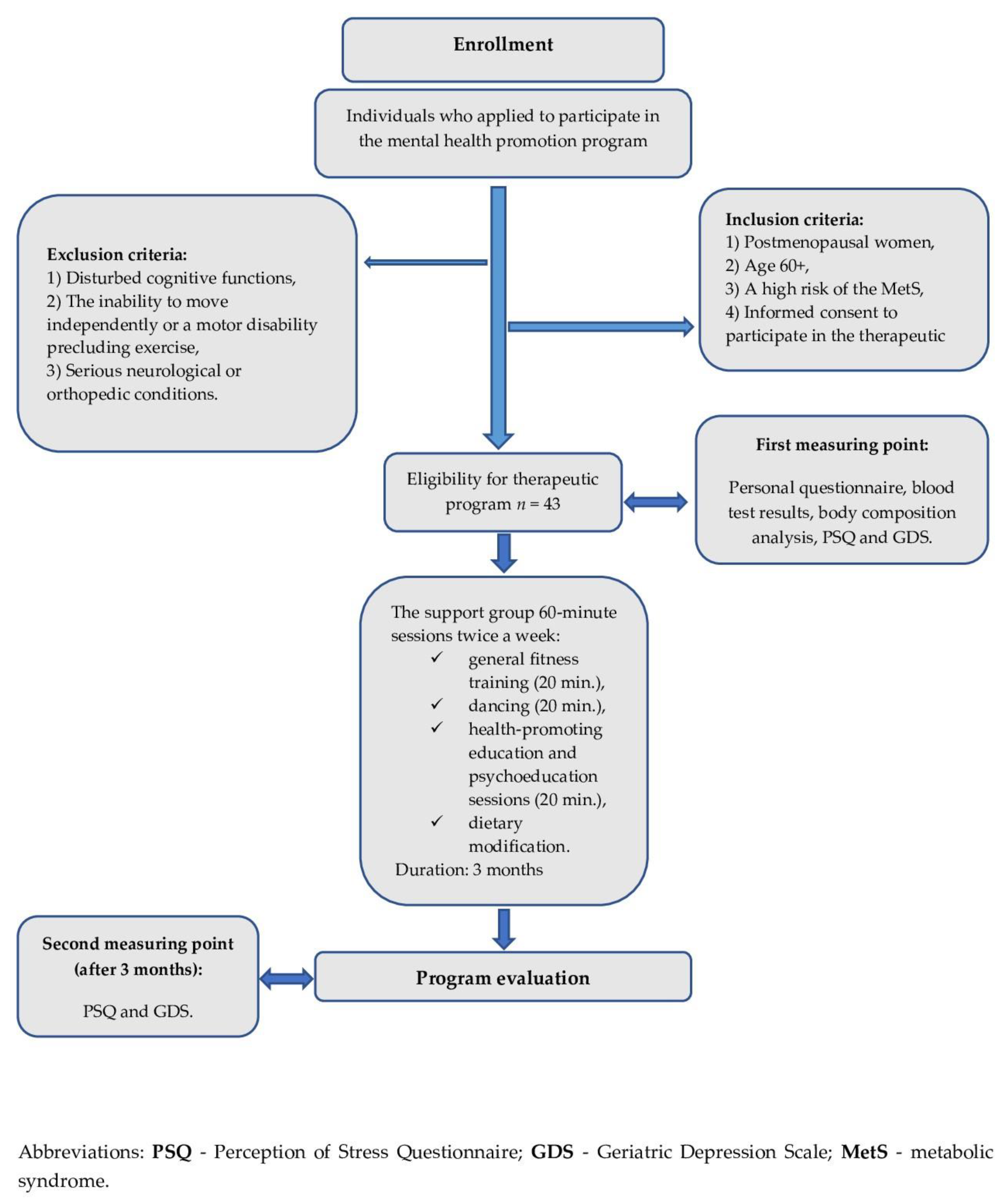
2.1. Design of the Study
2.2. Inclusion Criteria for the Research Project
2.3. Measurements
2.4. Intervention
2.5. Statistical Methods
3. Results
3.1. First Measurement Point
3.2. Correlation Analysis
3.3. Second Measurement Point: Pre-Post Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Ageing and Health. Available online: https://www.who.int/en/news-room/fact-sheets/detail/ageing-and-health (accessed on 22 March 2020).
- Zając, K.; Serweta, A.; Salamon-Krakowska, K.; Szczepańska-Gieracha, J. The level of stress experienced in women over the age of 60 who take regular physical activity and pro-health activities. Contemporary Gerontology. 2017, 5, 120–124. [Google Scholar]
- Statistics Poland. The situation of older people in Poland in 2018; Statistics Poland: Warsaw, Poland, 2018. [Google Scholar]
- Szczepańska-Gieracha, J.; Mazurek, J.; Serweta, A.; Boroń-Krupińska, K.; Kowalska, J.; Skrzek, A. Effectiveness Assessment of a Therapeutic Programme for Women with Overweight and Obesity: A Biopsychosocial Perspective. Fam. Med. Prim. Care Rev. 2019, 21, 381–386. [Google Scholar] [CrossRef]
- Kusnanto, H.; Agustian, D.; Hilmanto, D. Biopsychosocial Model of Illnesses in Primary Care: A Hermeneutic Literature Review. J. Fam. Med. Prim. Care 2018, 7, 497. [Google Scholar] [CrossRef] [PubMed]
- Raczkiewicz, D.; Bojar, I.; Wdowiak, A.; Rzeźnicki, A.; Krakowiak, J. Stress at Intellectual Work and Cardiovascular Diseases in Women at Non-Mobility Working Age. Ann. Agric Environ. Med. 2019, 26, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Morga, P.; Cieślik, B.; Sekułowicz, M.; Bujnowska-Fedak, M.; Drower, I.; Szczepańska-Gieracha, J. Low-Intensity Exercise as a Modifier of Depressive Symptoms and Self-Perceived Stress Level in Women with Metabolic Syndrome. J. Sports Sci. Med. 2021, 20, 222–228. [Google Scholar] [CrossRef]
- Murrock, C.J.; Graor, C.H. Effects of Dance on Depression, Physical Function, and Disability in Underserved Adults. J. Aging Phys. Act. 2014, 22, 380–385. [Google Scholar] [CrossRef]
- McNeely, M.E.; Duncan, R.P.; Earhart, G.M. Impacts of Dance on Non-Motor Symptoms, Participation, and Quality of Life in Parkinson Disease and Healthy Older Adults. Maturitas 2015, 82, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Hwang, P.W.-N.; Braun, K.L. The Effectiveness of Dance Interventions to Improve Older Adults’ Health: A Systematic Literature Review. Altern. Ther. Health Med. 2015, 21, 64–70. [Google Scholar]
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. Metabolic Syndrome-a New World-Wide Definition. A Consensus Statement from the International Diabetes Federation. Diabet Med. 2006, 23, 469–480. [Google Scholar] [CrossRef]
- International Diabetes Federation. The IDF Consensus Worldwide Definition of the Metabolic Syndrome; International Diabetes Federation: Brussels, Belgium, 2006. [Google Scholar]
- Tykarski, A.; Mastalerz-Migas, A.; Wieczorowska-Tobis, K.; Kokoszka-Paszkot, J.; Kusz-Rynkun, A.; Rymaszewska, J.; Bujnowska-Fedak, M.; Neumann-Podczaska, A.; Bień, B.; Siebert, J.; et al. REcomMEndations for DIAgnostics and maNagemenT of arterial hypertension in adults aged 65 years and older for General Practitioners—REMEDIA NT 65+ GP. Lek. POZ/Gen. Pract. 2018, 22, 263–288. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Plopa, M.; Makarowski, R. The Perception of Stress Questionnaire; Vizja Press & IT: Warszawa, Poland, 2010; ISBN 978-83-61086-79-6. [Google Scholar]
- Yesavage, J.A. Geriatric Depression Scale. Psychopharmacol. Bull. 1988, 24, 709–711. [Google Scholar]
- Albiński, R.; Kleszczewska-Albińska, A.; Bedyńska, S. Geriatric Depression Scale (GDS). Validity and reliability of different versions of the scale—Review. Psychiatr. Pol. 2011, 45, 555–562. [Google Scholar]
- Yesavage, J.A.; Sheikh, J.I. 9/Geriatric Depression Scale (GDS): Recent Evidence and Development of a Shorter Version. Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics Publishers: Champaign, IL, USA, 1998; ISBN 0-88011-623-4. [Google Scholar]
- Pérez-Idárraga, A.; Valencia Gómez, K.; Gallo Villegas, J.; Arenas Sosa, M.; Quintero Velásquez, M.A. Intervention with rumba and nutrition education to modify cardiovascular risk factors in adults with metabolic syndrome. Rev. Panam. Salud Publ. 2015, 37, 29–37. [Google Scholar]
- Hofgaard, J.; Ermidis, G.; Mohr, M. Effects of a 6-Week Faroese Chain Dance Programme on Postural Balance, Physical Function, and Health Profile in Elderly Subjects: A Pilot Study. BioMed. Res. Int. 2019, 2019, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Guzmán-García, A.; Hughes, J.C.; James, I.A.; Rochester, L. Dancing as a Psychosocial Intervention in Care Homes: A Systematic Review of the Literature: Dance Research in Dementia. Int. J. Geriatr. Psychiatry 2013, 28, 914–924. [Google Scholar] [CrossRef]
- Hearing, C.M.; Chang, W.C.; Szuhany, K.L.; Deckersbach, T.; Nierenberg, A.A.; Sylvia, L.G. Physical Exercise for Treatment of Mood Disorders: A Critical Review. Curr. Behav. Neurosci. Rep. 2016, 3, 350–359. [Google Scholar] [CrossRef] [Green Version]
- Brooks, S.; Brnayan, K.W.; DeVallance, E.; Skinner, R.; Lemaster, K.; Sheets, J.W.; Pitzer, C.R.; Asano, S.; Bryner, R.W.; Olfert, I.M.; et al. Psychological Stress-Induced Cerebrovascular Dysfunction: The Role of Metabolic Syndrome and Exercise. Exp. Physiol. 2018, 103, 761–776. [Google Scholar] [CrossRef]
- Favieri, F.; Forte, G.; Casagrande, M. The Executive Functions in Overweight and Obesity: A Systematic Review of Neuropsychological Cross-Sectional and Longitudinal Studies. Front. Psychol. 2019, 10, 2126. [Google Scholar] [CrossRef]
- Castro-Barquero, S.; Ruiz-León, A.M.; Sierra-Pérez, M.; Estruch, R.; Casas, R. Dietary Strategies for Metabolic Syndrome: A Comprehensive Review. Nutrients 2020, 12, 2983. [Google Scholar] [CrossRef] [PubMed]
- Chedraui, P.; Pérez-López, F.R.; Hidalgo, L.; Villacreses, D.; Domínguez, A.; Escobar, G.S.; Genazzani, A.R.; Simoncini, T.; Research Group for the Omega Women’s Health Project. Evaluation of the Presence and Severity of Menopausal Symptoms among Postmenopausal Women Screened for the Metabolic Syndrome. Gynecol. Endocrinol. 2014, 30, 918–924. [Google Scholar] [CrossRef] [PubMed]
- Tziallas, D.; Kastanioti, C.; Kostapanos, M.S.; Skapinakis, P.; Elisaf, M.S.; Mavreas, V. The Impact of the Metabolic Syndrome on Health-Related Quality of Life: A Cross-Sectional Study in Greece. Eur. J. Cardiovasc. Nurs. 2012, 11, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Okosun, I.S.; Annor, F.; Esuneh, F.; Okoegwale, E.E. Metabolic Syndrome and Impaired Health-Related Quality of Life and in Non-Hispanic White, Non-Hispanic Blacks and Mexican-American Adults. Diabetes Metab. Syndr. Clin. Res. Rev. 2013, 7, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Raikkonen, K.; Matthews, K.A.; Kuller, L.H. Depressive Symptoms and Stressful Life Events Predict Metabolic Syndrome Among Middle-Aged Women: A Comparison of World Health Organization, Adult Treatment Panel III, and International Diabetes Foundation Definitions. Diabetes Care 2007, 30, 872–877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eschweiler, G.W. Diagnostik und multimodale Therapie der Altersdepression: Neue Entwicklungen. Z Gerontol Geriat. 2017, 50, 99–105. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Total n = 43 (mean ± SD) | ||
|---|---|---|
| Age (years) | 68.6 ± 6.5 | |
| Mass (kg) | 73.2 ± 17.9 | |
| Height (m) | 159.6 ± 6.0 | |
| BMI (kg/cm2) | 28.9 ± 6.2 | |
| Waist Circumference (cm) | 97 ± 14.3 | |
| Hips Circumference (cm) | 113 ± 16.4 | |
| WHR | 0.86 ± 0.08 | |
| Education (%) | Basic/vocational | 15 |
| Secondary | 51 | |
| Higher education | 34 | |
| Marital status (%) | Married | 37 |
| Single | 24 | |
| Divorced | 7 | |
| Widowed | 32 | |
| Body weight classification (%) | Normal weight | 25 |
| Overweight | 39 | |
| Class I obesity | 22 | |
| Class II obesity | 14 | |
| Mood and well-being (%) | Lack of depression | 76 |
| Moderate depression | 22 | |
| Severe depression | 2 | |
| Feature | Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|---|
| Blood pressure (mmHg) | systolic | 134.9 | 21.2 | 90 | 184 |
| diastolic | 74.8 | 10.2 | 52 | 98 | |
| Cholesterol (mg/dL) | total | 211.5 | 42.1 | 149 | 342 |
| HDL | 70.6 | 23.8 | 42 | 183 | |
| LDL | 118.7 | 39.9 | 63 | 238 | |
| Triglycerides (mg/dL) | 120.5 | 47.2 | 48 | 253 | |
| Blood sugar level (mg%) | 98.4 | 13.8 | 60 | 125 | |
| Feature | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|
| Fat (%) | 38.9 | 6.9 | 21.1 | 50.2 |
| Water Composition (%) | 44.2 | 4.6 | 36.5 | 55.2 |
| Muscle Mass (kg) | 41.7 | 7.4 | 28.6 | 58.9 |
| Bone Mass (kg) | 2.2 | 0.4 | 1 | 3.1 |
| Basal Metabolic Rate (kcal) | 1332.8 | 238.3 | 983 | 1947 |
| Visceral Fat | 11 | 2.9 | 6.5 | 19 |
| Stress Components | Spearman’s Rank Correlation Coefficient | |||
|---|---|---|---|---|
| Age | GDS | BMI | Visceral Fat | |
| Emotional tension | 0.1, p = 0.52 | 0.57 * p = 0.00 | 0.31 p = 0.06 | 0.3 p = 0.08 |
| External stress | 0.13, p = 0.40 | 0.53 * p = 0.00 | 0.4 * p = 0.02 | 0.32 p = 0.06 |
| Intrapsychic stress | 0.19, p = 0.23 | 0.52 * p = 0.00 | 0.4 * p = 0.02 | 0.36 * p = 0.03 |
| General PSQ score | 0.15, p = 0.35 | 0.61 * p = 0.00 | 0.39 * p = 0.02 | 0.33 * p = 0.05 |
| N = 43 | Mean | SD | Minimum | Maximum | p-Value | Z | T |
|---|---|---|---|---|---|---|---|
| GDS | |||||||
| Before | 6.95 | 5.66 | 0 | 30 | |||
| After | 6.79 | 5.18 | 0 | 20 | |||
| Change | 0.16 | NS | 0.337 | 246.00 | |||
| General PSQ Score | |||||||
| Before | 60.53 | 18.28 | 23 | 104 | |||
| After | 49.81 | 16.41 | 22 | 83 | |||
| Change | 10.72 | <0.001 | 4.095 | 124.00 | |||
| Emotional Tension | |||||||
| Before | 18.21 | 6.97 | 7 | 32 | |||
| After | 18.33 | 7.34 | 7 | 35 | |||
| Change | −0.12 | NS | 0.283 | 351.00 | |||
| External Stress | |||||||
| Before | 16.91 | 5.32 | 8 | 30 | |||
| After | 14.30 | 4.70 | 7 | 25 | |||
| Change | 2.61 | <0.001 | 3.734 | 113.00 | |||
| Intrapsychic Stress | |||||||
| Before | 17.91 | 5.61 | 7 | 30 | |||
| After | 17.19 | 6.35 | 7 | 31 | |||
| Change | 0.72 | NS | 1.584 | 276.50 | |||
| STEN | PRE% | POST% |
|---|---|---|
| 1 | 5 | 23 |
| 2 | 9 | 19 |
| 3 | 16 | 9 |
| 4 | 21 | 16 |
| 5 | 18 | 19 |
| 6 | 14 | 7 |
| 7 | 5 | 5 |
| 8 | 7 | 0 |
| 9 | 0 | 0 |
| 10 | 5 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rusowicz, J.; Serweta, A.; Idzikowski, W.; Szczepańska-Gieracha, J. Multimodal Therapeutic Approach in Women with High Risk of Metabolic Syndrome—A Single Group One Center Pre-Post Study. J. Clin. Med. 2021, 10, 4915. https://doi.org/10.3390/jcm10214915
Rusowicz J, Serweta A, Idzikowski W, Szczepańska-Gieracha J. Multimodal Therapeutic Approach in Women with High Risk of Metabolic Syndrome—A Single Group One Center Pre-Post Study. Journal of Clinical Medicine. 2021; 10(21):4915. https://doi.org/10.3390/jcm10214915
Chicago/Turabian StyleRusowicz, Jagoda, Anna Serweta, Wojciech Idzikowski, and Joanna Szczepańska-Gieracha. 2021. "Multimodal Therapeutic Approach in Women with High Risk of Metabolic Syndrome—A Single Group One Center Pre-Post Study" Journal of Clinical Medicine 10, no. 21: 4915. https://doi.org/10.3390/jcm10214915
APA StyleRusowicz, J., Serweta, A., Idzikowski, W., & Szczepańska-Gieracha, J. (2021). Multimodal Therapeutic Approach in Women with High Risk of Metabolic Syndrome—A Single Group One Center Pre-Post Study. Journal of Clinical Medicine, 10(21), 4915. https://doi.org/10.3390/jcm10214915