
Microvascular and Structural Alterations of the Macula in Early to Moderate Glaucoma: An Optical Coherence Tomography-Angiography Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
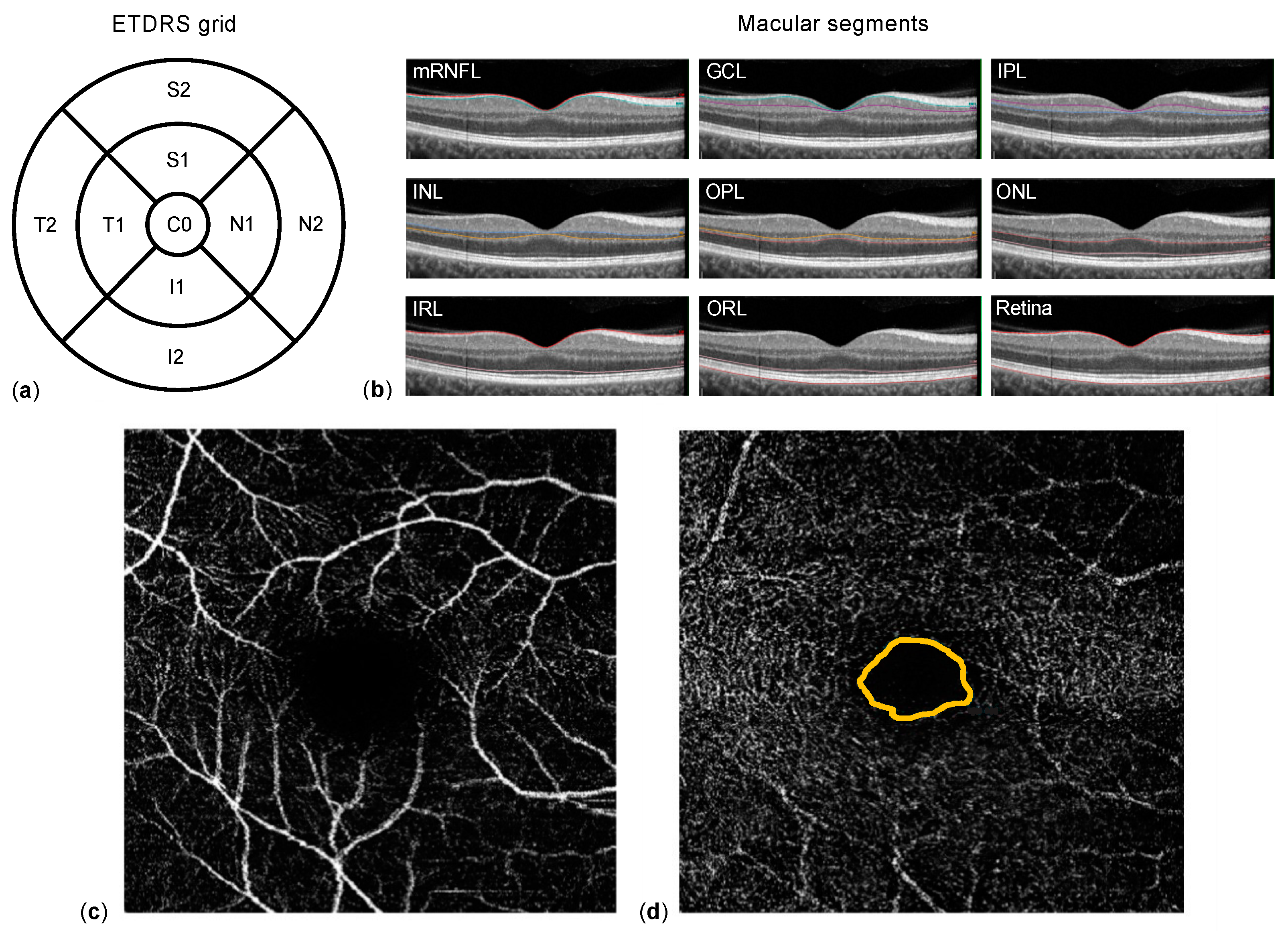
2.2. Data Acquisition
2.3. Statistical Methods
3. Results
3.1. Patients’ Characteristics
3.2. Differences in Macular Segment Thickness between Glaucoma and Healthy
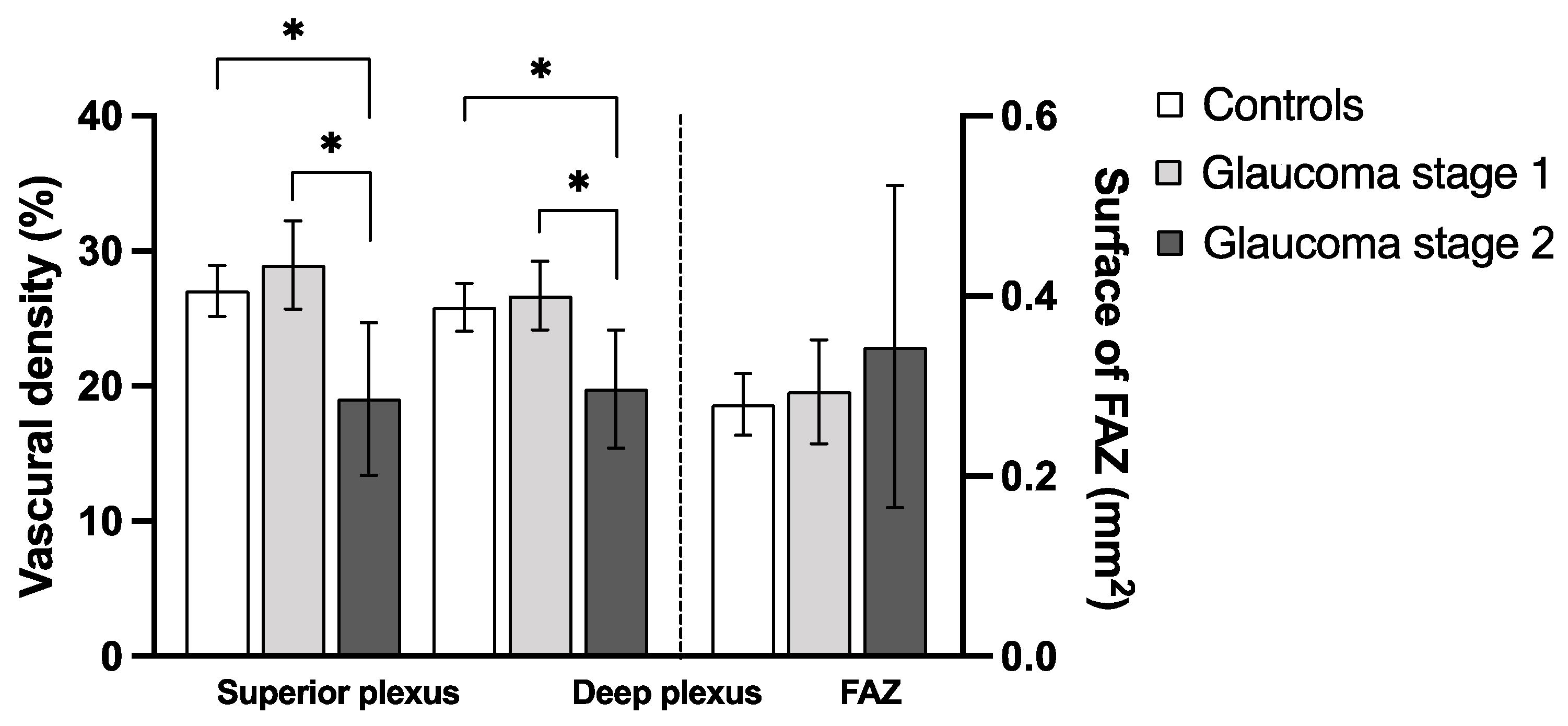
3.3. Macular Vasculature Differences between Glaucoma Patients and Healthy Controls
3.4. Correlation of Vascular Density and Macular Segment Thickness
4. Discussion
- The vascular density of the deep and superficial plexus is reduced in glaucoma and correlates with the presence of glaucoma.
- Differences in macular vascular density are mainly detectable in GS2 but less so in GS1 eyes.
- The foveal avascular zone is not affected by glaucoma.
- Glaucoma severity directly influences the strength of association between macular inner segments’ thickness and vascular density.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Medeiros, F.A.; Zangwill, L.M.; Bowd, C.; Mansouri, K.; Weinreb, R.N. The structure and function relationship in glaucoma: Implications for detection of progression and measurement of rates of change. Investig. Ophthalmol. Vis. Sci. 2012, 53, 6939–6946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lever, M.; Unterlauft, J.D.; Halfwassen, C.; Bechrakis, N.E.; Manthey, A.; Böhm, M.R.R. Individualized Significance of 24-Hour Intraocular Pressure Curves for Therapeutic Decisions in Primary Chronic Open-Angle Glaucoma Patients. Clin. Ophthalmol. 2020, 14, 1483–1494. [Google Scholar] [CrossRef] [PubMed]
- Abe, R.Y.; Gracitelli, C.P.B.; Medeiros, F.A. The Use of Spectral-Domain Optical Coherence Tomography to Detect Glaucoma Progression. Open Ophthalmol. J. 2015, 9, 78–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshikawa, M.; Akagi, T.; Hangai, M.; Ohashi-Ikeda, H.; Takayama, K.; Morooka, S.; Kimura, Y.; Nakano, N.; Yoshimura, N. Alterations in the neural and connective tissue components of glaucomatous cupping after glaucoma surgery using swept-source optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2014, 55, 477–484. [Google Scholar] [CrossRef] [Green Version]
- Enders, P.; Longo, V.; Adler, W.; Horstmann, J.; Schaub, F.; Dietlein, T.; Cursiefen, C.; Heindl, L.M. Analysis of peripapillary vessel density and Bruch’s membrane opening-based neuroretinal rim parameters in glaucoma using OCT and OCT-angiography. Eye 2020, 34, 1086–1093. [Google Scholar] [CrossRef]
- Unterlauft, J.D.; Rehak, M.; Böhm, M.R.R.; Rauscher, F.G. Analyzing the impact of glaucoma on the macular architecture using spectral-domain optical coherence tomography. PLoS ONE 2018, 13, e0209610. [Google Scholar] [CrossRef] [PubMed]
- Lever, M.; Halfwassen, C.; Unterlauft, J.D.; Bechrakis, N.E.; Manthey, A.; Böhm, M.R.R. The Paediatric Glaucoma Diagnostic Ability of Optical Coherence Tomography: A Comparison of Macular Segmentation and Peripapillary Retinal Nerve Fibre Layer Thickness. Biology 2021, 10, 260. [Google Scholar] [CrossRef]
- Renard, J.P.; Fénolland, J.R.; Giraud, J.M. Glaucoma progression analysis by Spectral-Domain Optical Coherence Tomography (SD-OCT). J. Fr. Ophtalmol. 2019, 42, 499–516. [Google Scholar] [CrossRef] [PubMed]
- Sung, K.R.; Wollstein, G.; Kim, N.R.; Na, J.H.; Nevins, J.E.; Kim, C.Y.; Schuman, J.S. Macular assessment using optical coherence tomography for glaucoma diagnosis. Br. J. Ophthalmol. 2012, 96, 1452–1455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oddone, F.; Lucenteforte, E.; Michelessi, M.; Rizzo, S.; Donati, S.; Parravano, M.; Virgili, G. Macular versus Retinal Nerve Fiber Layer Parameters for Diagnosing Manifest Glaucoma: A Systematic Review of Diagnostic Accuracy Studies. Ophthalmology 2016, 123, 939–949. [Google Scholar] [CrossRef] [PubMed]
- Lommatzsch, A. OCT Angiography. Klin. Monbl. Augenheilkd. 2020, 237, 95–111. [Google Scholar] [CrossRef] [PubMed]
- Jia, Y.; Morrison, J.C.; Tokayer, J.; Tan, O.; Lombardi, L.; Baumann, B.; Lu, C.D.; Choi, W.; Fujimoto, J.G.; Huang, D. [BOE]2012 Quantitative OCT angiography of optic nerve.pdf. Biomed. Opt. Express 2012, 3, 183–189. [Google Scholar]
- Xu, H.; Kong, X.M. Study of retinal microvascular perfusion alteration and structural damage at macular region in primary open-angle glaucoma patients. Zhonghua Yan Ke Za Zhi 2017, 53, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Manalastas, P.I.C.; Zangwill, L.M.; Saunders, L.J.; Mansouri, K.; Belghith, A.; Suh, M.H.; Yarmohammadi, A.; Penteado, R.C.; Akagi, T.; Shoji, T.; et al. Reproducibility of optical coherence tomography angiography macular and optic nerve head vascular density in glaucoma and healthy eyes. J. Glaucoma 2017, 26, 851–859. [Google Scholar] [CrossRef] [PubMed]
- Rao, H.L.; Pradhan, Z.S.; Weinreb, R.N.; Riyazuddin, M.; Dasari, S.; Venugopal, J.P.; Puttaiah, N.K.; Rao, D.A.S.; Devi, S.; Mansouri, K.; et al. A comparison of the diagnostic ability of vessel density and structural measurements of optical coherence tomography in primary open angle glaucoma. PLoS ONE 2017, 12, e0173930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lommatzsch, C.; Rothaus, K.; Koch, J.M.; Heinz, C.; Grisanti, S. OCTA vessel density changes in the macular zone in glaucomatous eyes. Graefes Arch. Clin. Exp. Ophthalmol. 2018, 256, 1499–1508. [Google Scholar] [CrossRef]
- Shoji, T.; Zangwill, L.M.; Akagi, T.; Saunders, L.J.; Yarmohammadi, A.; Manalastas, P.I.C.; Penteado, R.C.; Weinreb, R.N. Progressive Macula Vessel Density Loss in Primary Open-Angle Glaucoma: A Longitudinal Study. Am. J. Ophthalmol. 2017, 182, 107–117. [Google Scholar] [CrossRef]
- Jeon, S.J.; Park, H.Y.L.; Park, C.K. Effect of Macular Vascular Density on Central Visual Function and Macular Structure in Glaucoma Patients. Sci. Rep. 2018, 8, 16009. [Google Scholar] [CrossRef] [Green Version]
- Mills, R.P.; Budenz, D.L.; Lee, P.P.; Noecker, R.J.; Walt, J.G.; Siegartel, L.R.; Evans, S.J.; Doyle, J.J. Categorizing the stage of glaucoma from pre-diagnosis to end-stage disease. Am. J. Ophthalmol. 2006, 141, 24–30. [Google Scholar] [CrossRef]
- Curcio, C.A.; Allen, K.A. Topography of ganglion cells in human retina. J. Comp. Neurol. 1990, 300, 5–25. [Google Scholar] [CrossRef]
- Kim, N.R.; Lee, E.S.; Seong, G.J.; Kim, J.H.; An, H.G.; Kim, C.Y. Structure–Function Relationship and Diagnostic Value of Macular Ganglion Cell Complex Measurement Using Fourier-Domain OCT in Glaucoma. Investig. Opthalmol. Vis. Sci. 2010, 51, 4646. [Google Scholar] [CrossRef]
- Hood, D.C.; Raza, A.S.; de Moraes, C.G.V.; Liebmann, J.M.; Ritch, R. Glaucomatous damage of the macula. Prog. Retin. Eye Res. 2013, 32, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Kuang, T.M.; Zhang, C.; Zangwill, L.M.; Weinreb, R.N.; Medeiros, F.A. Estimating lead time gained by optical coherence tomography in detecting glaucoma before development of visual field defects. Ophthalmology 2015, 122, 2002–2009. [Google Scholar] [CrossRef] [Green Version]
- Kass, M.A.; Heuer, D.K.; Higginbotham, E.J.; Johnson, C.A.; Keltner, J.L.; Miller, J.P.; Parrish, R.K.; Wilson, M.R.; Gordon, M.O. The Ocular Hypertension Treatment Study. Arch. Ophthalmol. 2002, 120, 701. [Google Scholar] [CrossRef]
- Cherecheanu, A.P.; Garhofer, G.; Schmidl, D.; Werkmeister, R.; Schmetterer, L. Ocular perfusion pressure and ocular blood flow in glaucoma. Curr. Opin. Pharmacol. 2013, 13, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Tobe, L.A.; Harris, A.; Hussain, R.M.; Eckert, G.; Huck, A.; Park, J.; Egan, P.; Kim, N.J.; Siesky, B. The role of retrobulbar and retinal circulation on optic nerve head and retinal nerve fibre layer structure in patients with open-angle glaucoma over an 18-month period. Br. J. Ophthalmol. 2015, 99, 609–612. [Google Scholar] [CrossRef] [PubMed]
- Akil, H.; Huang, A.S.; Francis, B.A.; Sadda, S.R.; Chopra, V. Retinal vessel density from optical coherence tomography angiography to differentiate early glaucoma, pre-perimetric glaucoma and normal eyes. PLoS ONE 2017, 12, e0170476. [Google Scholar] [CrossRef] [PubMed]
- Takusagawa, H.L.; Liu, L.; Ma, K.N.; Jia, Y.; Gao, S.S.; Zhang, M.; Edmunds, B.; Parikh, M.; Tehrani, S.; Morrison, J.C.; et al. Projection-Resolved Optical Coherence Tomography Angiography of Macular Retinal Circulation in Glaucoma. Ophthalmology 2017, 124, 1589–1599. [Google Scholar] [CrossRef] [PubMed]
- Ragkousis, A.; Kozobolis, V.; Kabanarou, S.; Bontzos, G.; Mangouritsas, G.; Heliopoulos, I.; Chatziralli, I. Vessel Density around Foveal Avascular Zone as a Potential Imaging Biomarker for Detecting Preclinical Diabetic Retinopathy: An Optical Coherence Tomography Angiography Study. Semin. Ophthalmol. 2020, 35, 316–323. [Google Scholar] [CrossRef]
- Shahlaee, A.; Samara, W.A.; Hsu, J.; Say, E.A.T.; Khan, M.A.; Sridhar, J.; Hong, B.K.; Shields, C.L.; Ho, A.C. In Vivo Assessment of Macular Vascular Density in Healthy Human Eyes Using Optical Coherence Tomography Angiography. Am. J. Ophthalmol. 2016, 165, 39–46. [Google Scholar] [CrossRef]
- Lommatzsch, C.; Heinz, C.; Koch, J.M.; Heimes-Bussmann, B.; Hahn, U.; Grisanti, S. Does the Foveal Avascular Zone Change in Glaucoma? Klin. Monbl. Augenheilkd. 2020, 237, 879–888. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | p-Value 1 |
|---|---|---|
| Patients (n) | 70 | |
| Sex (male:female % (n)) | 46:54% (32:38) | |
| Glaucoma | 45:55% (14:17) | |
| Healthy | 46:54% (18:21) | |
| Eye (right:left % (n)) | 56:44% (39:31) | |
| Diagnosis (glaucoma: healthy % (n)) | 44:56% (31:39) | |
| Stage 1 (% of glaucoma (n)) | 71.0% (22) | |
| Stage 2 (% of glaucoma (n)) | 29.0% (9) | |
| Age (mean ± SD (y)) | 63.0 ± 13.1 | |
| Glaucoma | 63.8 ± 14.0 | 0.64 |
| Glaucoma stage 1 | 64.7 ± 14.8 | 0.52 |
| Glaucoma stage 2 | 61.8 ± 12.5 | 0.90 |
| Healthy | 62.4 ± 12.5 | |
| BCVA (median ± IQR (LogMar)) | 0.1 ± 0.1 | |
| Glaucoma | 0.1 ± 0.2 | 0.23 |
| Healthy | 0.0 ± 0.1 | |
| IOP (mean ± SD (mm Hg)) | 13.6 ± 3.0 | |
| Glaucoma | 12.7 ± 2.0 | 0.066 |
| Healthy | 14.1 ± 3.2 | |
| Linear CDR * (median ± IQR) | 0.7 ± 0.3 | |
| Perimetry (MD) * (mean ± SD (dB)) | 2.0 ± 4.3 |
| Macular Segment | Mean Thickness (µm) ± SD | ANOVA Summary | Adjusted p-Value | ||||
|---|---|---|---|---|---|---|---|
| Controls | Glaucoma Stage 1 (GS1) | Glaucoma Stage 2 (GS2) | F | p-Value | Controls vs. GS2 | GS1 vs. GS2 | |
| Retina | |||||||
| Inner superior (S1) | 335.4 ± 20.0 | 337.2 ± 21.0 | 314.2 ± 20.5 | 4.54 | 0.014 | 0.018 | 0.016 |
| Outer superior (S2) | 333.6 ± 18.8 | 333.0 ± 18.0 | 311.8 ± 28.7 | 4.59 | 0.014 | 0.012 | 0.024 |
| Inner inferior (I1) | 337.0 ± 14.9 | 333.5 ± 20.9 | 301.8 ± 23.1 | 14.1 | <0.0001 | <0.0001 | 0.0001 |
| Outer inferior (I2) | 327.6 ± 8.7 | 327.5 ± 17.9 | 305.7 ± 17.9 | 5.57 | 0.0058 | 0.0054 | 0.010 |
| Ganglion cell layer | |||||||
| Inner superior (S1) | 47.6 ± 9.6 | 48.1 ± 9.8 | 31.1 ± 10.3 | 11.8 | <0.0001 | <0.0001 | <0.0001 |
| Outer superior (S2) | 47.9 ± 7.4 | 45.8 ± 5.1 | 30.6 ± 9.4 | 23.3 | <0.0001 | <0.0001 | <0.0001 |
| Inner inferior (I1) | 49.4 ± 7.2 | 44.5 ± 11.1 | 23.9 ± 12.2 | 27.7 | <0.0001 | <0.0001 | <0.0001 |
| Outer inferior (I2) | 47.7 ± 5.9 | 45.8 ± 8.2 | 28.2 ± 9.1 | 28.1 | <0.0001 | <0.0001 | <0.0001 |
| Inner plexiform layer | |||||||
| Inner superior (S1) | 39.8 ± 5.5 | 39.8 ± 5.1 | 30.1 ± 6.8 | 11.9 | <0.0001 | <0.0001 | 0.0001 |
| Outer superior (S2) | 38.3 ± 4.8 | 37.3 ± 4.1 | 27.7 ± 7.3 | 16.8 | <0.0001 | <0.0001 | <0.0001 |
| Inner inferior (I1) | 40.3 ± 4.2 | 38.0 ± 6.1 | 27.4 ± 8.3 | 19.8 | <0.0001 | <0.0001 | <0.0001 |
| Outer inferior (I2) | 37.7 ± 4.4 | 37.2 ± 5.2 | 27.2 ± 5.4 | 18.5 | <0.0001 | <0.0001 | <0.0001 |
| Controls | Glaucoma | p-Value | Glaucoma Stage 1 | Glaucoma Stage 2 | |
|---|---|---|---|---|---|
| FAZ area (mm2) | 0.28 ± 0.11 | 0.31 ± 0.16 | 0.37 | 0.29 ± 0.13 | 0.34 ± 0.23 |
| Superior plexus VD (%) | 27.0 ± 5.8 | 26.1 ± 8.6 | 0.58 | 29.0 ± 7.4 | 19.0 ± 7.4 |
| Deep plexus VD (%) | 25.8 ± 5.4 | 24.7 ± 6.4 | 0.42 | 26.7 ± 5.7 | 19.8 ± 5.7 |
| F of ANOVA | p-Value | Mean Difference | 95% CI | Adjusted p-Value | |
|---|---|---|---|---|---|
| FAZ (mm2) | 0.84 | 0.44 | |||
| Controls vs. GS1 | −0.015 | −0.10 to 0.071 | 0.91 | ||
| Controls vs. GS2 | −0.064 | −0.18 to 0.055 | 0.40 | ||
| GS1 vs. GS2 | −0.050 | −0.18 to 0.078 | 0.62 | ||
| Superior plexus (%) | 7.8 | 0.0011 | |||
| Controls vs. GS1 | −1.9 | −6.1 to 2.3 | 0.52 | ||
| Controls vs. GS2 | 8.0 | 2.2 to 13.8 | 0.0040 | ||
| GS1 vs. GS2 | 9.9 | 3.8 to 16.1 | 0.0008 | ||
| Deep plexus (%) | 5.3 | 0.0072 | |||
| Controls vs. GS1 | −0.85 | −4.4 to 2.7 | 0.83 | ||
| Controls vs. GS2 | 6.1 | 1.1 to 11.0 | 0.0120 | ||
| GS1 vs. GS2 | 6.9 | 1.6 to 12.2 | 0.0069 |
| Parameter Estimate | 95% CI | R2 | p-Value | |
|---|---|---|---|---|
| FAZ | 0.78 | −0.50 to 2.1 | 0.021 | 0.23 |
| Superior plexus | −0.024 | −0.048 to −0.00079 | 0.059 | 0.043 |
| Deep plexus | −0.029 | −0.058 to −0.00075 | 0.058 | 0.045 |
| Parameter Estimate | 95% CI | R2 | |
|---|---|---|---|
| T2 of GCL → superficial plexus vascular density | |||
| Controls | 0.41 | 0.16 to 0.66 | 0.23 |
| Glaucoma stage 1 | 0.57 | 0.24 to 0.89 | 0.40 |
| Glaucoma stage 2 | 0.56 | 0.28 to 0.84 | 0.76 |
| N2 of IPL → deep plexus vascular density | |||
| Controls | 0.19 | −0.19 to 0.57 | 0.027 |
| Glaucoma stage 1 | 0.43 | −0.18 to 1.0 | 0.097 |
| Glaucoma stage 2 | 0.74 | 0.27 to 1.0 | 0.66 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lever, M.; Glaser, M.; Chen, Y.; Halfwassen, C.; Unterlauft, J.D.; Bechrakis, N.E.; Böhm, M.R.R. Microvascular and Structural Alterations of the Macula in Early to Moderate Glaucoma: An Optical Coherence Tomography-Angiography Study. J. Clin. Med. 2021, 10, 5017. https://doi.org/10.3390/jcm10215017
Lever M, Glaser M, Chen Y, Halfwassen C, Unterlauft JD, Bechrakis NE, Böhm MRR. Microvascular and Structural Alterations of the Macula in Early to Moderate Glaucoma: An Optical Coherence Tomography-Angiography Study. Journal of Clinical Medicine. 2021; 10(21):5017. https://doi.org/10.3390/jcm10215017
Chicago/Turabian StyleLever, Mael, Moritz Glaser, Ying Chen, Christian Halfwassen, Jan Darius Unterlauft, Nikolaos E. Bechrakis, and Michael R. R. Böhm. 2021. "Microvascular and Structural Alterations of the Macula in Early to Moderate Glaucoma: An Optical Coherence Tomography-Angiography Study" Journal of Clinical Medicine 10, no. 21: 5017. https://doi.org/10.3390/jcm10215017