
Comprehensive Lifestyle Modification Influences Medium-Term and Artificially Induced Stress in Ulcerative Colitis—A Sub-Study within a Randomized Controlled Trial Using the Trier Social Stress Test

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Randomization
2.3. Participants
2.4. Intervention and Control
2.5. Long-Term Measures
2.6. Sub-Study: Trier Social Stress Test
2.6.1. Procedure
2.6.2. Measures
2.6.3. Sample Size Calculation and Statistical Analyses
3. Results
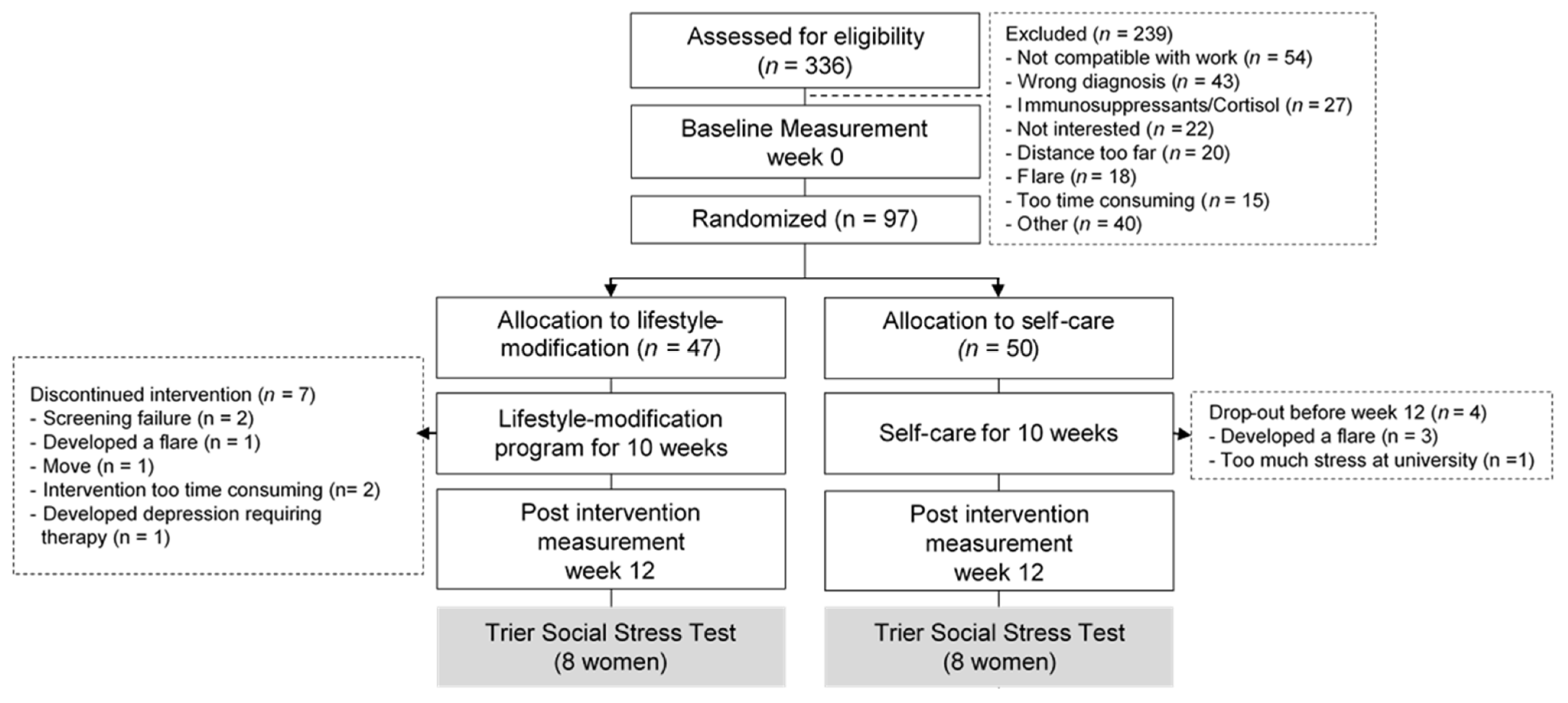
3.1. Participants
3.2. Perceived Stress, Anxiety, Depression, and Flourishing before and after the Interventions
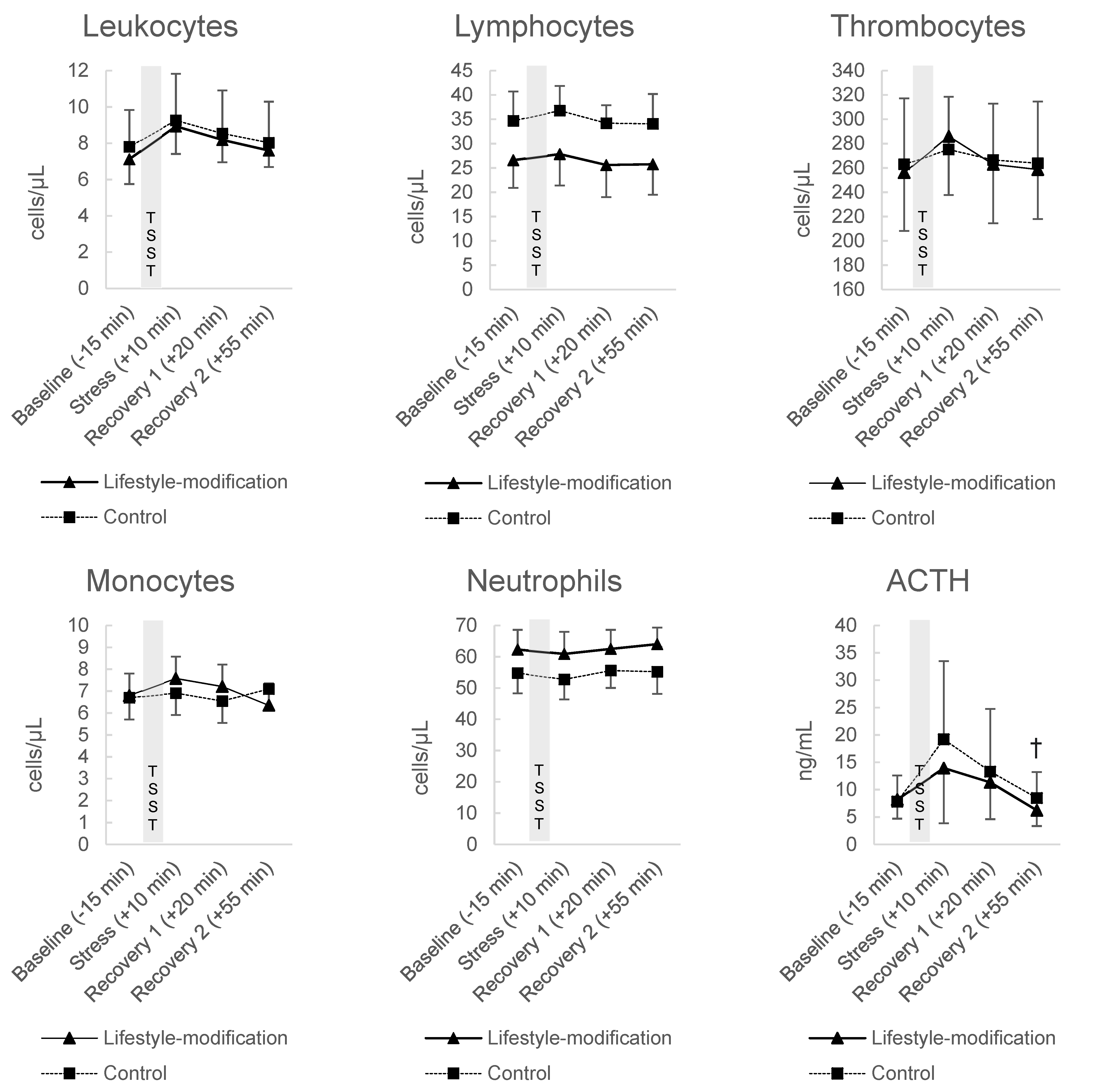
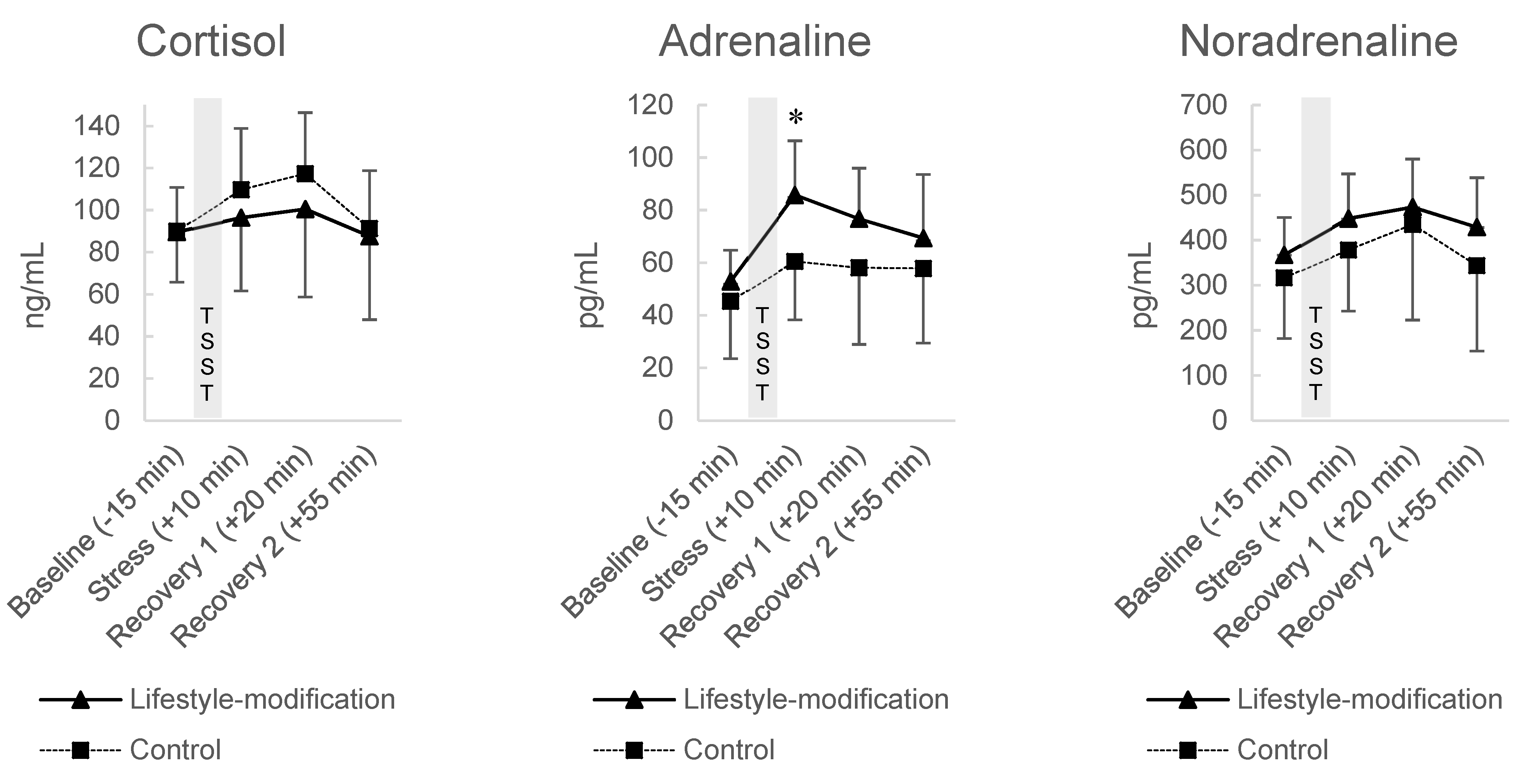
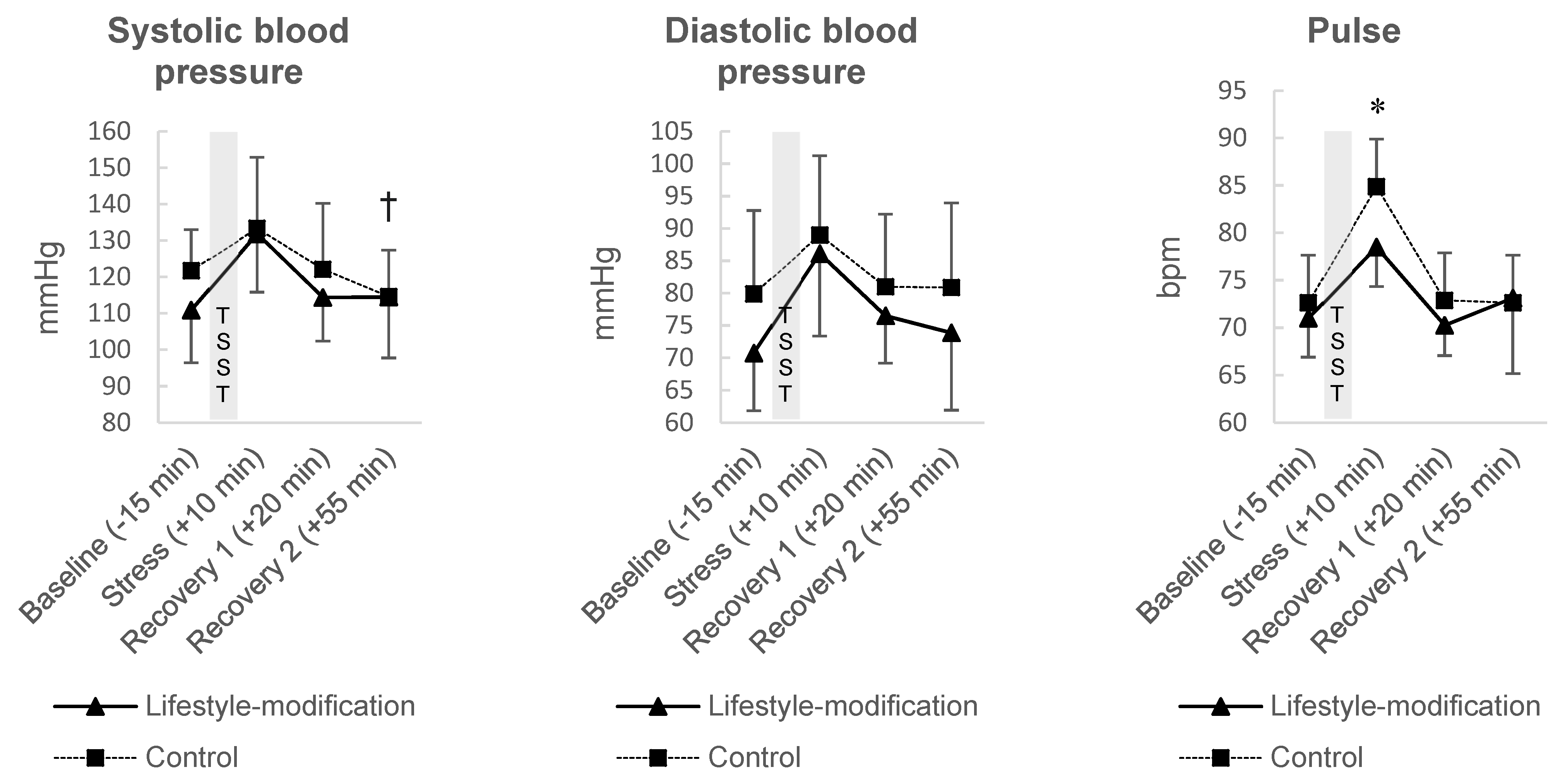
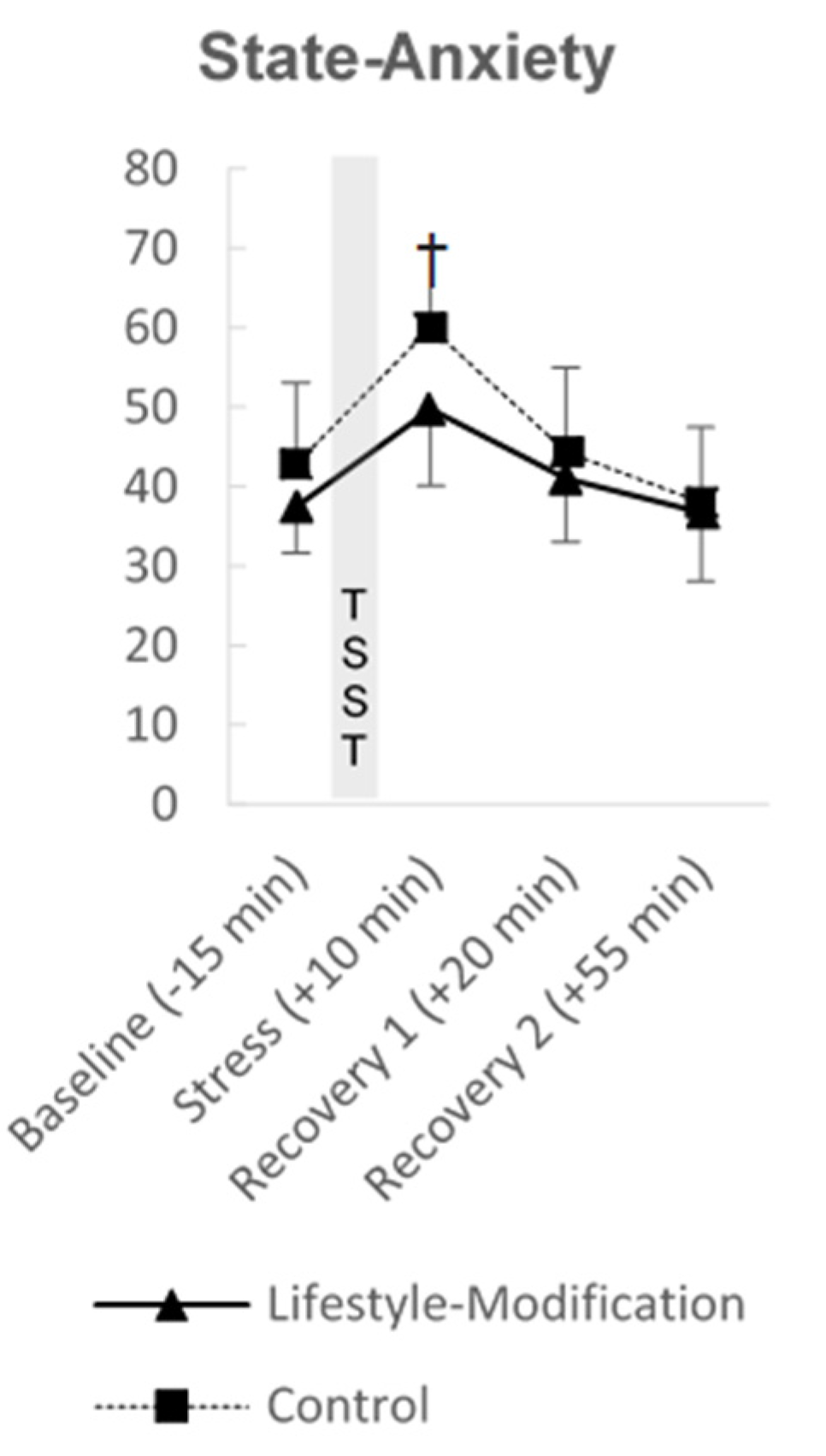
3.3. Responses to the TSST
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hauser, W.; Moser, G.; Klose, P.; Mikocka-Walus, A. Psychosocial issues in evidence-based guidelines on inflammatory bowel diseases: A review. World J. Gastroenterol. 2014, 20, 3663–3671. [Google Scholar] [CrossRef] [Green Version]
- Langhorst, J.; Hofstetter, A.; Wolfe, F.; Hauser, W. Short-term stress, but not mucosal healing nor depression was predictive for the risk of relapse in patients with ulcerative colitis: A prospective 12-month follow-up study. Inflamm. Bowel Dis. 2013, 19, 2380–2386. [Google Scholar] [CrossRef]
- Mawdsley, J.E.; Rampton, D.S. Psychological stress in IBD: New insights into pathogenic and therapeutic implications. Gut 2005, 54, 1481–1491. [Google Scholar] [CrossRef]
- Mayer, E.A. Psychological stress and colitis. Gut 2000, 46, 595. [Google Scholar] [CrossRef] [Green Version]
- Mikocka-Walus, A.; Knowles, S.R.; Keefer, L.; Graff, L. Controversies Revisited: A Systematic Review of the Comorbidity of Depression and Anxiety with Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2016, 22, 752–762. [Google Scholar] [CrossRef]
- Engler, H.; Elsenbruch, S.; Rebernik, L.; Kocke, J.; Cramer, H.; Schols, M.; Langhorst, J. Stress burden and neuroendocrine regulation of cytokine production in patients with ulcerative colitis in remission. Psychoneuroendocrinology 2018, 98, 101–107. [Google Scholar] [CrossRef]
- Langhorst, J.; Anthonisen, I.B.; Steder-Neukamm, U.; Ludtke, R.; Spahn, G.; Michalsen, A.; Dobos, G.J. Amount of systemic steroid medication is a strong predictor for the use of complementary and alternative medicine in patients with inflammatory bowel disease: Results from a German national survey. Inflamm. Bowel Dis. 2005, 11, 287–295. [Google Scholar] [CrossRef]
- Langhorst, J.; Anthonisen, I.B.; Steder-Neukamm, U.; Luedtke, R.; Spahn, G.; Michalsen, A.; Dobos, G.J. Patterns of complementary and alternative medicine (CAM) use in patients with inflammatory bowel disease: Perceived stress is a potential indicator for CAM use. Complementary Ther. Med. 2007, 15, 30–37. [Google Scholar] [CrossRef]
- Keefer, L.; Kane, S.V. Considering the Bidirectional Pathways Between Depression and IBD: Recommendations for Comprehensive IBD Care. Gastroenterol. Hepatol. 2017, 13, 164–169. [Google Scholar]
- Mikocka-Walus, A.A.; Turnbull, D.A.; Moulding, N.T.; Wilson, I.G.; Andrews, J.M.; Holtmann, G.J. Controversies surrounding the comorbidity of depression and anxiety in inflammatory bowel disease patients: A literature review. Inflamm. Bowel Dis. 2007, 13, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Luo, H.; Sun, Y.; Li, Y.; Lv, H.; Sheng, L.; Wang, L.; Qian, J. Perceived stress and inappropriate coping behaviors associated with poorer quality of life and prognosis in patients with ulcerative colitis. J. Psychosom. Res. 2018, 113, 66–71. [Google Scholar] [CrossRef]
- Agostini, A.; Ballotta, D.; Righi, S.; Moretti, M.; Bertani, A.; Scarcelli, A.; Sartini, A.; Ercolani, M.; Nichelli, P.; Campieri, M.; et al. Stress and brain functional changes in patients with Crohn’s disease: A functional magnetic resonance imaging study. Neurogastroenterol. Motil. Off. J. Eur. Gastrointest. Motil. Soc. 2017, 29, 1–10. [Google Scholar] [CrossRef]
- Agostini, A.; Filippini, N.; Benuzzi, F.; Bertani, A.; Scarcelli, A.; Leoni, C.; Farinelli, V.; Riso, D.; Tambasco, R.; Calabrese, C.; et al. Functional magnetic resonance imaging study reveals differences in the habituation to psychological stress in patients with Crohn’s disease versus healthy controls. J. Behav. Med. 2013, 36, 477–487. [Google Scholar] [CrossRef]
- Farhadi, A.; Keshavarzian, A.; Van de Kar, L.D.; Jakate, S.; Domm, A.; Zhang, L.; Shaikh, M.; Banan, A.; Fields, J.Z. Heightened responses to stressors in patients with inflammatory bowel disease. Am. J. Gastroenterol. 2005, 100, 1796–1804. [Google Scholar] [CrossRef]
- Labanski, A.; Langhorst, J.; Engler, H.; Elsenbruch, S. Stress and the brain-gut axis in functional and chronic-inflammatory gastrointestinal diseases: A transdisciplinary challenge. Psychoneuroendocrinology 2020, 111, 104501. [Google Scholar] [CrossRef] [PubMed]
- Dusek, J.A.; Otu, H.H.; Wohlhueter, A.L.; Bhasin, M.; Zerbini, L.F.; Joseph, M.G.; Benson, H.; Libermann, T.A. Genomic counter-stress changes induced by the relaxation response. PLoS ONE 2008, 3, e2576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, B.; Bhasin, M.; Jacquart, J.; Scult, M.A.; Slipp, L.; Riklin, E.I.K.; Lepoutre, V.; Comosa, N.; Norton, B.-A.; Dassatti, A.; et al. Genomic and Clinical Effects Associated with a Relaxation Response Mind-Body Intervention in Patients with Irritable Bowel Syndrome and Inflammatory Bowel Disease. PLoS ONE 2015, 10, e0123861. [Google Scholar] [CrossRef] [PubMed]
- Cramer, H.; Schäfer, M.; Schöls, M.; Köcke, J.; Elsenbruch, S.; Lauche, R.; Engler, H.; Dobos, G.; Langhorst, J. Randomised clinical trial: Yoga vs written self-care advice for ulcerative colitis. Aliment. Pharmacol. Ther. 2017, 45, 1379–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koch, A.K.; Schöls, M.; Langhorst, J.; Dobos, G.; Cramer, H. Perceived stress mediates the effect of yoga on quality of life and disease activity in ulcerative colitis. Secondary analysis of a randomized controlled trial. J. Psychosom. Res. 2020, 130, 109917. [Google Scholar] [CrossRef]
- Bonaz, B.L.; Bernstein, C.N. Brain-gut interactions in inflammatory bowel disease. Gastroenterology 2013, 144, 36–49. [Google Scholar] [CrossRef] [Green Version]
- Elsenbruch, S.; Langhorst, J.; Popkirowa, K.; Muller, T.; Luedtke, R.; Franken, U.; Paul, A.; Spahn, G.; Michalsen, A.; Janssen, O.E.; et al. Effects of mind-body therapy on quality of life and neuroendocrine and cellular immune functions in patients with ulcerative colitis. Psychother. Psychosom. 2005, 74, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Langhorst, J.; Mueller, T.; Luedtke, R.; Franken, U.; Paul, A.; Michalsen, A.; Schedlowski, M.; Dobos, G.J.; Elsenbruch, S. Effects of a comprehensive lifestyle modification program on quality-of-life in patients with ulcerative colitis: A twelve-month follow-up. Scand. J. Gastroenterol. 2007, 42, 734–745. [Google Scholar] [CrossRef]
- Paul, A.; Lauche, R.; Cramer, H.; Altner, N.; Langhorst, J.; Dobos, G.J. An Integrative Day Care Clinic for chronically ill patients: Concept and case presentation. Eur. J. Integr. Med. 2012, 4, e455–e459. [Google Scholar] [CrossRef]
- Allen, A.P.; Kennedy, P.J.; Dockray, S.; Cryan, J.F.; Dinan, T.G.; Clarke, G. The Trier Social Stress Test: Principles and practice. Neurobiol. Stress 2017, 6, 113–126. [Google Scholar] [CrossRef] [Green Version]
- Langhorst, J.; Schöls, M.; Cinar, Z.; Eilert, R.; Kofink, K.; Paul, A.; Zempel, C.; Elsenbruch, S.; Lauche, R.; Ahmed, M.; et al. Comprehensive Lifestyle-Modification in Patients with Ulcerative Colitis–A Randomized Controlled Trial. J. Clin. Med. 2020, 9, 3087. [Google Scholar] [CrossRef] [PubMed]
- Dedovic, K.; Wadiwalla, M.; Engert, V.; Pruessner, J.C. The role of sex and gender socialization in stress reactivity. Dev. Psychol. 2009, 45, 45–55. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Klein, E.M.; Brahler, E.; Dreier, M.; Reinecke, L.; Muller, K.W.; Schmutzer, G.; Wolfling, K.; Beutel, M.E. The German version of the Perceived Stress Scale—Psychometric characteristics in a representative German community sample. BMC Psychiatry 2016, 16, 159. [Google Scholar] [CrossRef] [Green Version]
- Petermann, F. Hospital Anxiety and Depression Scale, Deutsche Version (HADS-D). Z. Für Psychiatr. Psychol. Und Psychother. 2011, 59, 251–253. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Diener, E.; Wirtz, D.; Biswas-Diener, R.; Tov, W.; Kim-Prieto, C.; Choi, D.-W.; Oishi, S. New measures of well-being. In Assessing Well-Being: The Collected Works of Ed Diener; Springer Science + Business Media: New York, NY, USA, 2009; pp. 247–266. [Google Scholar] [CrossRef]
- Esch, T.; Jose, G.; Gimpel, C.; von Scheidt, C.; Michalsen, A. Die Flourishing Scale (FS) von Diener et al. liegt jetzt in einer autorisierten deutschen Fassung (FS-D) vor: Einsatz bei einer Mind-Body-medizinischen Fragestellung. Complement. Med. Res. 2013, 20, 267–275. [Google Scholar] [CrossRef]
- Kirschbaum, C.; Pirke, K.M.; Hellhammer, D.H. The ‘Trier Social Stress Test’—A tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology 1993, 28, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Laux, L.; Glanzmann, P.; Schaffner, P.; Spielberger, C.D. Das State-Trait-Angstinventar (Testmappe mit Handanweisungen, Fragebogen STAI-G Form X1 und Fragebogen STAI-G form X2); Beltz: Weinheim, Germany, 1981. [Google Scholar]
- Gaab, J.; Blättler, N.; Menzi, T.; Pabst, B.; Stoyer, S.; Ehlert, U. Randomized controlled evaluation of the effects of cognitive–behavioral stress management on cortisol responses to acute stress in healthy subjects. Psychoneuroendocrinology 2003, 28, 767–779. [Google Scholar] [CrossRef]
- Milne, B.; Joachim, G.; Niedhardt, J. A stress management programme for inflammatory bowel disease patients. J. Adv. Nurs. 1986, 11, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Langhorst, J.; Cobelens, P.M.; Kavelaars, A.; Heijnen, C.J.; Benson, S.; Rifaie, N.; Dobos, G.J.; Schedlowski, M.; Elsenbruch, S. Stress-related peripheral neuroendocrine-immune interactions in women with ulcerative colitis. Psychoneuroendocrinology 2007, 32, 1086–1096. [Google Scholar] [CrossRef]
- Hoffman, J.W.; Benson, H.; Arns, P.A.; Stainbrook, G.L.; Landsberg, G.L.; Young, J.B.; Gill, A. Reduced sympathetic nervous system responsivity associated with the relaxation response. Science 1982, 215, 190–192. [Google Scholar] [CrossRef]
- Craske, M.G.; Wolitzky-Taylor, K.B.; Labus, J.; Wu, S.; Frese, M.; Mayer, E.A.; Naliboff, B.D. A cognitive-behavioral treatment for irritable bowel syndrome using interoceptive exposure to visceral sensations. Behav. Res. Ther. 2011, 49, 413–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ljótsson, B.; Hesser, H.; Andersson, E.; Lackner, J.M.; El Alaoui, S.; Falk, L.; Aspvall, K.; Fransson, J.; Hammarlund, K.; Löfström, A.; et al. Provoking symptoms to relieve symptoms: A randomized controlled dismantling study of exposure therapy in irritable bowel syndrome. Behav. Res. Ther. 2014, 55, 27–39. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lifestyle Modification (n = 47) | Lifestyle Modification TSST (n = 8) | Control (n = 50) | Control TSST (n = 8) | |
|---|---|---|---|---|
| Age years | 50.28 ± 11.90 (18–74) | 44.6 ± 14.3 (18–57) | 45.54 ± 12.49 (19–71) | 49.25 ± 4.30 (43–57) |
| Female n (%) | 34 (72.3) | 8 (100) | 35 (70) | 8 (100) |
| Weight | 72.79 ± 14.90 (52–100) | 71.13 ± 12.87 (62–97) | 70.24 ± 16.86 (49.6–150) | 61.19 ± 9.72 (51–79) |
| Height | 171.19 ± 9.05 (152–196) | 173.88 ± 6.11 (167–183) | 173.76 ± 9.94 (156–197) | 169.00 ± 4.00 (164–176) |
| Anamnestic pattern n (%) | ||||
| Proctitis | 14 (29.8) | 1 (12.5) | 15 (30) | 3 (37.5) |
| Left-sided colitis | 17 (36.2) | 4 (50) | 15 (30) | 2 (25) |
| Pancolitis | 13 (27.7) | 3 (37.5) | 17 (34) | 3 (37.5) |
| Missing | 3 (6.4) | 0 (0) | 3 (6) | 0 (0) |
| Time since diagnosis years | 18.04 ± 12.00 (2–46) | 10.50 ± 7.95 (2–24) | 14.76 ± 10.99 (1–43) | 12.63 ± 4.03 (5–17) |
| Prior integrative medicine inpatient treatment at Kliniken Essen-Mitte n (%) | 13 (27.7) | 2 (25) | 12 (24) | 1 (12.5) |
| Prior integrative medicine day-care treatment at Kliniken Essen-Mitte n (%) | 7 (14.9) | 2 (25) | 3 (6) | 1 (12.5) |
| Smokers n (%) | 2 (4.3) | 1 (12.5) | 3 (6) | 1 (12.5) |
| Married n (%) | 33 (70.2) | 6 (75) | 39 (78) | 6 (75) |
| Education n (%) | ||||
| Secondary school | 17 (36.1) | 3 (37.5) | 11 (22) | 3 (37.5) |
| High school (“Abitur”) | 12 (25.6) | 4 (50) | 14 (28) | 2 (25) |
| University degree | 18 (38.3) | 1 (12.5) | 25 (50) | 3 (37.5) |
| Medication intake n (%) | ||||
| Steroids, Azathioprine, Biologicals | 9 (19.2) | 4 (50) | 7 (14) | 1 (12.5) |
| Mesalazine | 33 (70.2) | 7 (87.5) | 34 (68) | 7 (87.5) |
| Herbal medicine | 7 (14.9) | 0 (0) | 15 (30) | 1 (12.5) |
| Other | 8 (17) | 0 (0) | 12 (24) | 2 (25) |
| n | Baseline | Week 12 | Week 24 | Week 48 | Group Differences Week 12 | Group Differences Week 24 | Group Differences Week 48 | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| p | η2p | p | η2p | p | η2p | ||||||
| Perceived Stress (PSS-10) | |||||||||||
| Lifestyle-modification | 47 | 22.30 ± 5.60 | 14.00 ± 6.38 | 15.76 ± 6.44 | 13.75 ± 7.20 | <0.001 | 0.148 | 0.023 | 0.054 | 0.060 | 0.037 |
| Control | 50 | 22.20 ± 6.66 | 18.59 ± 6.89 | 18.47 ± 6.29 | 16.05 ± 6.80 | ||||||
| Anxiety (HADS_A) | |||||||||||
| Lifestyle-modification | 47 | 10.30 ± 4.33 | 6.67 ± 3.84 | 7.61 ± 4.26 | 6.46 ± 3.98 | 0.075 | 0.033 | 0.824 | 0.001 | 0.627 | 0.003 |
| Control | 50 | 9.81 ± 4.16 | 7.45 ± 3.55 | 7.55 ± 3.48 | 6.55 ± 3.20 | ||||||
| Depression (HADS_D) | |||||||||||
| Lifestyle-modification | 47 | 6.78 ± 3.84 | 4.74 ± 3.39 | 5.57 ± 3.52 | 4.45 ± 3.46 | 0.146 | 0.022 | 0.430 | 0.007 | 0.764 | 0.001 |
| Control | 50 | 7.00 ± 3.48 | 5.81 ± 3.91 | 6.18 ± 3.59 | 4.74 ± 3.36 | ||||||
| Flourishing | |||||||||||
| Lifestyle-modification | 36 | 42.06 ± 8.69 | 43.77 ± 6.32 | - | 45.59 ± 6.11 | 0.247 | 0.018 | - | - | 0.006 | 0.100 |
| Control | 41 | 41.98 ± 5.89 | 42.41 ± 5.24 | - | 41.65 ± 6.26 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koch, A.K.; Schöls, M.; Haller, H.; Anheyer, D.; Cinar, Z.; Eilert, R.; Kofink, K.; Engler, H.; Elsenbruch, S.; Cramer, H.; et al. Comprehensive Lifestyle Modification Influences Medium-Term and Artificially Induced Stress in Ulcerative Colitis—A Sub-Study within a Randomized Controlled Trial Using the Trier Social Stress Test. J. Clin. Med. 2021, 10, 5070. https://doi.org/10.3390/jcm10215070
Koch AK, Schöls M, Haller H, Anheyer D, Cinar Z, Eilert R, Kofink K, Engler H, Elsenbruch S, Cramer H, et al. Comprehensive Lifestyle Modification Influences Medium-Term and Artificially Induced Stress in Ulcerative Colitis—A Sub-Study within a Randomized Controlled Trial Using the Trier Social Stress Test. Journal of Clinical Medicine. 2021; 10(21):5070. https://doi.org/10.3390/jcm10215070
Chicago/Turabian StyleKoch, Anna K., Margarita Schöls, Heidemarie Haller, Dennis Anheyer, Zehra Cinar, Ronja Eilert, Kerstin Kofink, Harald Engler, Sigrid Elsenbruch, Holger Cramer, and et al. 2021. "Comprehensive Lifestyle Modification Influences Medium-Term and Artificially Induced Stress in Ulcerative Colitis—A Sub-Study within a Randomized Controlled Trial Using the Trier Social Stress Test" Journal of Clinical Medicine 10, no. 21: 5070. https://doi.org/10.3390/jcm10215070
APA StyleKoch, A. K., Schöls, M., Haller, H., Anheyer, D., Cinar, Z., Eilert, R., Kofink, K., Engler, H., Elsenbruch, S., Cramer, H., Dobos, G., & Langhorst, J. (2021). Comprehensive Lifestyle Modification Influences Medium-Term and Artificially Induced Stress in Ulcerative Colitis—A Sub-Study within a Randomized Controlled Trial Using the Trier Social Stress Test. Journal of Clinical Medicine, 10(21), 5070. https://doi.org/10.3390/jcm10215070