
Early Coronary Angiography Is Associated with Improved 30-Day Outcomes among Patients with Out-of-Hospital Cardiac Arrest

 , , , , , ,
, , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Collection
2.3. EMS
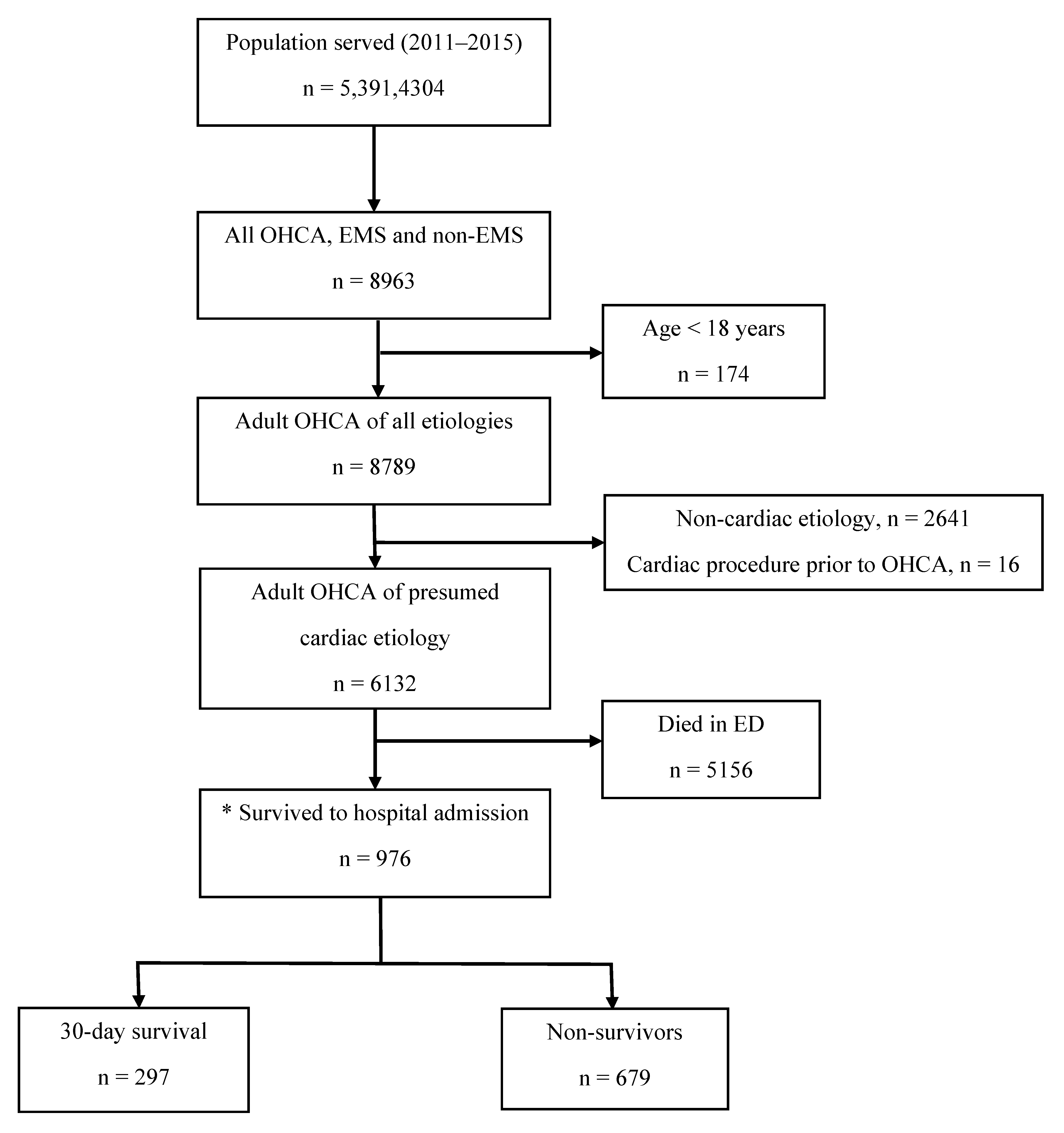
2.4. Study Population and Primary Exposure
2.5. Study Outcomes
2.6. Statistical Analysis
3. Results
3.1. Demographics, Event Characteristics and Outcomes
3.2. Prevalence of CAD
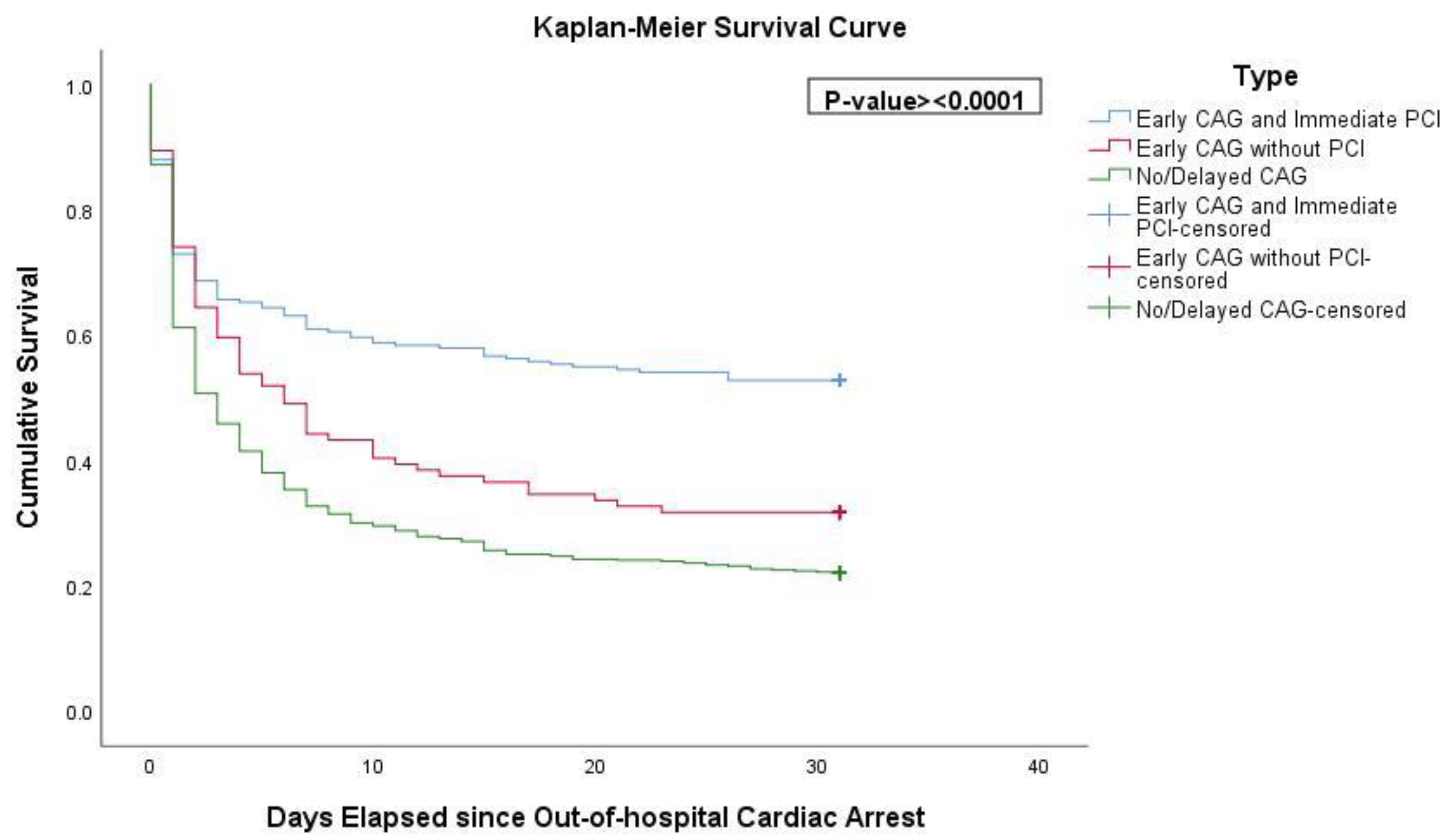
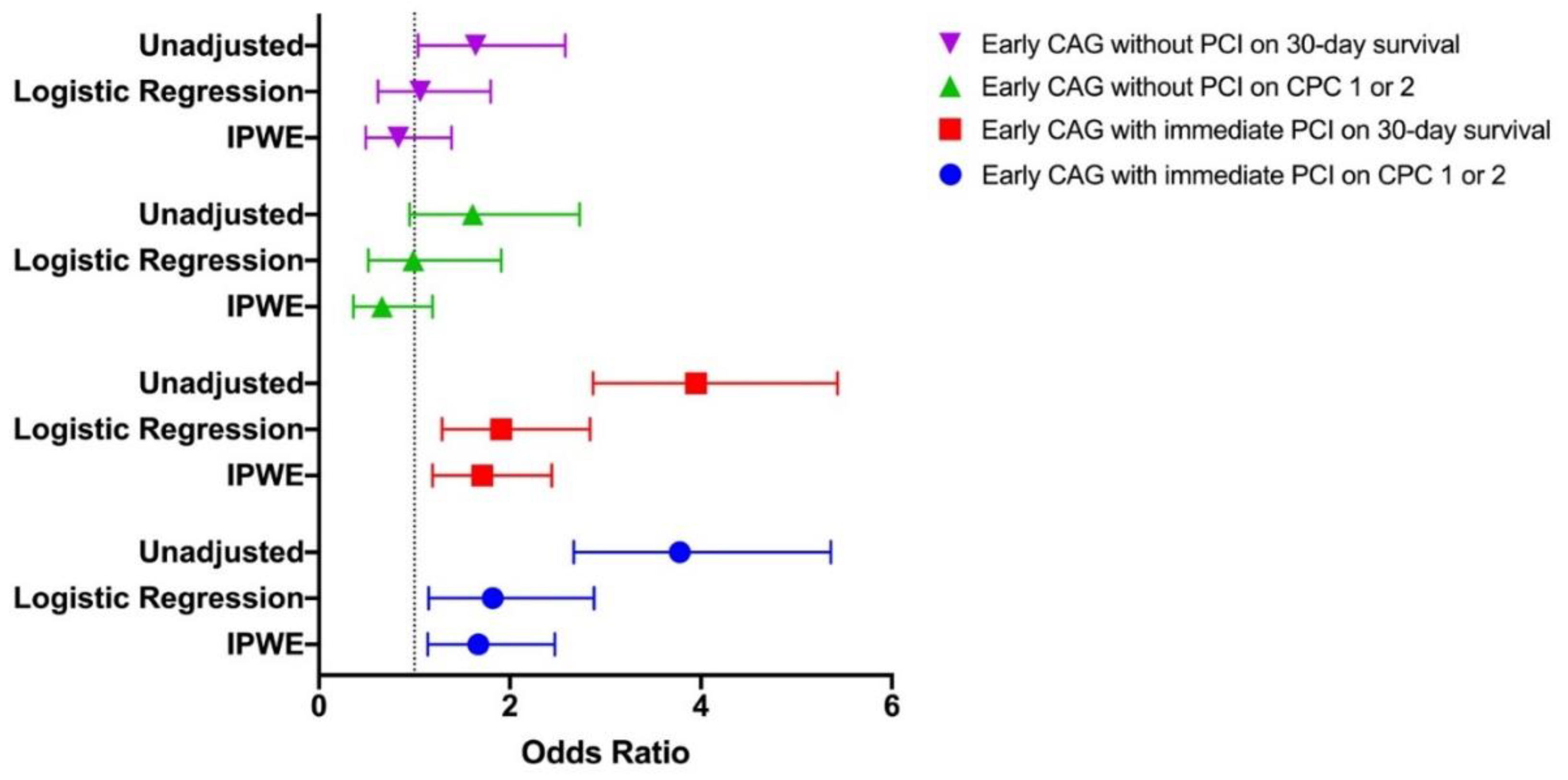
3.3. Survival and Neurological Outcomes
4. Discussion
4.1. Comparison of Findings with Prior Studies
4.2. Practice of Early CAG in Singapore
4.3. The Use of CABG as a Revascularization Strategy
4.4. Adverse Events
4.5. Clinical Implications
4.6. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berdowski, J.; Berg, R.A.; Tijssen, J.G.; Koster, R.W. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospective studies. Resuscitation 2010, 81, 1479–1487. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef]
- Beck, B.; Bray, J.; Cameron, P.; Smith, K.; Walker, T.; Grantham, H.; Hein, C.; Thorrowgood, M.; Smith, A.; Inoue, M.; et al. Regional variation in the characteristics, incidence and outcomes of out-of-hospital cardiac arrest in Australia and New Zealand: Results from the Aus-ROC Epistry. Resuscitation 2018, 126, 49–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gräsner, J.T.; Lefering, R.; Koster, R.W.; Masterson, S.; Böttiger, B.W.; Herlitz, J.; Wnent, J.; Tjelmeland, I.B.; Ortiz, F.R.; Maurer, H.; et al. EuReCa ONE-27 Nations, ONE Europe, ONE Registry: A prospective one month analysis of out-of-hospital cardiac arrest outcomes in 27 countries in Europe. Resuscitation 2016, 105, 188–195. [Google Scholar] [CrossRef] [Green Version]
- Dumas, F.; Cariou, A.; Manzo-Silberman, S.; Grimaldi, D.; Vivien, B.; Rosencher, J.; Empana, J.P.; Carli, P.; Mira, J.P.; Jouven, X.; et al. Immediate percutaneous coronary intervention is associated with better survival after out-of-hospital cardiac arrest: Insights from the PROCAT (Parisian Region Out of hospital Cardiac ArresT) registry. Circ. Cardiovasc. Interv. 2010, 3, 200–207. [Google Scholar] [CrossRef] [Green Version]
- Spaulding, C.M.; Joly, L.M.; Rosenberg, A.; Monchi, M.; Weber, S.N.; Dhainaut, J.F.; Carli, P. Immediate coronary angiography in survivors of out-of-hospital cardiac arrest. N. Engl. J. Med. 1997, 336, 1629–1633. [Google Scholar] [CrossRef]
- Khan, M.S.; Shah, S.; Mubashir, A.; Khan, A.R.; Fatima, K.; Schenone, A.L.; Khosa, F.; Samady, H.; Menon, V. Early coronary angiography in patients resuscitated from out of hospital cardiac arrest without ST-segment elevation: A systematic review and meta-analysis. Resuscitation 2017, 121, 127–134. [Google Scholar] [CrossRef]
- Khera, R.; CarlLee, S.; Blevins, A.; Schweizer, M.; Girotra, S. Early coronary angiography and survival after out-of-hospital cardiac arrest: A systematic review and meta-analysis. Open Heart 2018, 5, e000809. [Google Scholar] [CrossRef] [Green Version]
- Camuglia, A.C.; Randhawa, V.K.; Lavi, S.; Walters, D.L. Cardiac catheterization is associated with superior outcomes for survivors of out of hospital cardiac arrest: Review and meta-analysis. Resuscitation 2014, 85, 1533–1540. [Google Scholar] [CrossRef]
- Lemkes, J.S.; Janssens, G.N.; van der Hoeven, N.W.; Jewbali, L.; Dubois, E.A.; Meuwissen, M.; Rijpstra, T.A.; Bosker, H.A.; Blans, M.J.; Bleeker, G.B.; et al. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. N. Engl. J. Med. 2019, 380, 1397–1407. [Google Scholar] [CrossRef]
- Verma, B.R.; Sharma, V.; Shekhar, S.; Kaur, M.; Khubber, S.; Bansal, A.; Singh, J.; Ahuja, K.R.; Nazir, S.; Chetrit, M.; et al. Coronary Angiography in Patients with out-of-Hospital Cardiac Arrest without ST-Segment Elevation. JACC Cardiovasc. Interv. 2020, 13, 2193–2205. [Google Scholar] [CrossRef]
- Kern, K.B.; Radsel, P.; Jentzer, J.C.; Seder, D.B.; Lee, K.S.; Lotun, K.; Janardhanan, R.; Stub, D.; Hsu, C.H.; Noc, M. Randomized Pilot Clinical Trial of Early Coronary Angiography Versus No Early Coronary Angiography after Cardiac Arrest without ST-Segment Elevation: The PEARL Study. Circulation 2020, 142, 2002–2012. [Google Scholar] [CrossRef] [PubMed]
- Elfwén, L.; Lagedal, R.; Nordberg, P.; James, S.; Oldgren, J.; Böhm, F.; Lundgren, P.; Rylander, C.; van der Linden, J.; Hollenberg, J.; et al. Direct or subacute coronary angiography in out-of-hospital cardiac arrest (DISCO)-An initial pilot-study of a randomized clinical trial. Resuscitation 2019, 139, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Desch, S.; Freund, A.; Akin, I.; Behnes, M.; Preusch, M.R.; Zelniker, T.A.; Skurk, C.; Landmesser, U.; Graf, T.; Eitel, I.; et al. Angiography after Out-of-Hospital Cardiac Arrest without ST-Segment Elevation. N. Engl. J. Med. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Callaway, C.W.; Donnino, M.W.; Fink, E.L.; Geocadin, R.G.; Golan, E.; Kern, K.B.; Leary, M.; Meurer, W.J.; Peberdy, M.A.; Thompson, T.M.; et al. Part 8: Post-Cardiac Arrest Care: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S465–S482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Statistics Singapore. Population Trends. Available online: https://www.singstat.gov.sg/-/media/files/publications/population/population2020.pdf (accessed on 13 October 2020).
- Ong, M.E.; Shin, S.D.; Tanaka, H.; Ma, M.H.; Khruekarnchana, P.; Hisamuddin, N.; Atilla, R.; Middleton, P.; Kajino, K.; Leong, B.S.; et al. Pan-Asian Resuscitation Outcomes Study (PAROS): Rationale, methodology, and implementation. Acad. Emerg. Med. 2011, 18, 890–897. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Jacobs, I.G.; Nadkarni, V.M.; Berg, R.A.; Bhanji, F.; Biarent, D.; Bossaert, L.L.; Brett, S.J.; Chamberlain, D.; de Caen, A.R.; et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: Update of the Utstein Resuscitation Registry Templates for Out-of-Hospital Cardiac Arrest: A statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Circulation 2015, 132, 1286–1300. [Google Scholar] [CrossRef]
- Loh, J.P.; Tan, L.L.; Zheng, H.; Lau, Y.H.; Chan, S.P.; Tan, K.B.; Chua, T.; Tan, H.C.; Foo, D.; Lee, C.W.; et al. First Medical Contact-to-Device Time and Heart Failure Outcomes among Patients Undergoing Primary Percutaneous Coronary Intervention. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004699. [Google Scholar] [CrossRef]
- Lim, S.L.; Smith, K.; Dyson, K.; Chan, S.P.; Earnest, A.; Nair, R.; Bernard, S.; Leong, B.S.; Arulanandam, S.; Ng, Y.Y.; et al. Incidence and outcomes of out-of-hospital cardiac arrest in Singapore and Victoria: A collaborative study. J. Am. Heart Assoc. 2020, 9, e015981. [Google Scholar] [CrossRef] [PubMed]
- Geri, G.; Dumas, F.; Bougouin, W.; Varenne, O.; Daviaud, F.; Pène, F.; Lamhaut, L.; Chiche, J.D.; Spaulding, C.; Mira, J.P.; et al. Immediate Percutaneous Coronary Intervention Is Associated with Improved Short- and Long-Term Survival after out-of-Hospital Cardiac Arrest. Circ. Cardiovasc. Interv. 2015, 8, e002303. [Google Scholar] [CrossRef] [Green Version]
- Jentzer, J.C.; Scutella, M.; Pike, F.; Fitzgibbon, J.; Krehel, N.M.; Kowalski, L.; Callaway, C.W.; Rittenberger, J.C.; Reynolds, J.C.; Barsness, G.W.; et al. Early coronary angiography and percutaneous coronary intervention are associated with improved outcomes after out of hospital cardiac arrest. Resuscitation 2018, 123, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Vyas, A.; Chan, P.S.; Cram, P.; Nallamothu, B.K.; McNally, B.; Girotra, S. Early Coronary Angiography and Survival after out-of-Hospital Cardiac Arrest. Circ. Cardiovasc. Interv. 2015, 8, e002321. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.J.; Ro, Y.S.; Shin, S.D.; Song, K.J.; Ahn, K.O.; Hong, S.O.; Kim, Y.T. Association of emergent and elective percutaneous coronary intervention with neurological outcome and survival after out-of-hospital cardiac arrest in patients with and without a history of heart disease. Resuscitation 2015, 97, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Sideris, G.; Voicu, S.; Yannopoulos, D.; Dillinger, J.G.; Adjedj, J.; Deye, N.; Gueye, P.; Manzo-Silberman, S.; Malissin, I.; Logeart, D.; et al. Favourable 5-year postdischarge survival of comatose patients resuscitated from out-of-hospital cardiac arrest, managed with immediate coronary angiogram on admission. Eur. Heart J. Acute Cardiovasc. Care 2014, 3, 183–191. [Google Scholar] [CrossRef]
- Cronier, P.; Vignon, P.; Bouferrache, K.; Aegerter, P.; Charron, C.; Templier, F.; Castro, S.; El Mahmoud, R.; Lory, C.; Pichon, N.; et al. Impact of routine percutaneous coronary intervention after out-of-hospital cardiac arrest due to ventricular fibrillation. Crit Care 2011, 15, R122. [Google Scholar] [CrossRef] [Green Version]
- Wijesekera, V.A.; Mullany, D.V.; Tjahjadi, C.A.; Walters, D.L. Routine angiography in survivors of out of hospital cardiac arrest with return of spontaneous circulation: A single site registry. BMC Cardiovasc. Disord. 2014, 14, 30. [Google Scholar] [CrossRef] [Green Version]
- Kern, K.B.; Lotun, K.; Patel, N.; Mooney, M.R.; Hollenbeck, R.D.; McPherson, J.A.; McMullan, P.W.; Unger, B.; Hsu, C.H.; Seder, D.B.; et al. Outcomes of Comatose Cardiac Arrest Survivors with and without ST-Segment Elevation Myocardial Infarction: Importance of Coronary Angiography. JACC Cardiovasc. Interv. 2015, 8, 1031–1040. [Google Scholar] [CrossRef] [Green Version]
- Neumar, R.W.; Nolan, J.P.; Adrie, C.; Aibiki, M.; Berg, R.A.; Böttiger, B.W.; Callaway, C.; Clark, R.S.; Geocadin, R.G.; Jauch, E.C.; et al. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation 2008, 118, 2452–2483. [Google Scholar] [CrossRef] [Green Version]
- O′Connor, R.E.; Bossaert, L.; Arntz, H.R.; Brooks, S.C.; Diercks, D.; Feitosa-Filho, G.; Nolan, J.P.; Vanden Hoek, T.L.; Walters, D.L.; Wong, A.; et al. Acute Coronary Syndrome Chapter Collaborators. Part 9: Acute coronary syndromes: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation 2010, 122, S422–S465. [Google Scholar] [CrossRef] [Green Version]
- Zipes, D.P.; Camm, A.J.; Borggrefe, M.; Buxton, A.E.; Chaitman, B.; Fromer, M.; Gregoratos, G.; Klein, G.; Moss, A.J.; Myerburg, R.J.; et al. ACC/AHA/ESC 2006 Guidelines for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (writing committee to develop Guidelines for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): Developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation 2006, 114, e385–e484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dankiewicz, J.; Nielsen, N.; Annborn, M.; Cronberg, T.; Erlinge, D.; Gasche, Y.; Hassager, C.; Kjaergaard, J.; Pellis, T.; Friberg, H. Survival in patients without acute ST elevation after cardiac arrest and association with early coronary angiography: A post hoc analysis from the TTM trial. Intensive Care Med. 2015, 41, 856–864. [Google Scholar] [CrossRef] [PubMed]
- Baldi, E.; Schnaubelt, S.; Caputo, M.L.; Klersy, C.; Clodi, C.; Bruno, J.; Compagnoni, S.; Benvenuti, C.; Domanovits, H.; Burkart, R.; et al. Association of Timing of Electrocardiogram Acquisition after Return of Spontaneous Circulation with Coronary Angiography Findings in Patients with out-of-Hospital Cardiac Arrest. JAMA Netw. Open 2021, 4, e2032875. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Early CAG (n = 337) | No/Delayed CAG (n = 639) | p Value * | |
|---|---|---|---|
| Demographics | |||
| Mean age (yrs), mean (SD) | 60.2 (12.1) | 65.8 (13.5) | <0.001 |
| Male sex, n (%) | 290 (86.1) | 429 (67.1) | <0.001 |
Ethnicity
| 209 (62.0) 44 (13.1) 57 (16.9) 27 (8.0) | 420 (65.7) 108 (16.9) 85 (13.3) 26 (4.1) | 0.013 |
| Medical History | |||
| Hypertension, n (%) | 183 (54.3) | 401 (62.8) | 0.013 |
| Diabetes mellitus, n (%) | 99 (29.4) | 280 (43.8) | <0.001 |
| Hyperlipidemia, n (%) | 136 (40.4) | 306 (47.9) | 0.029 |
| Heart disease, n (%) | 140 (41.5) | 377 (59.0) | <0.001 |
| Renal disease, n (%) | 33 (9.8) | 142 (22.2) | <0.001 |
| Respiratory disease, n (%) | 19 (5.6) | 88 (13.8) | <0.001 |
| Stroke, n (%) | 20 (5.9) | 89 (13.9) | <0.001 |
| Event information | |||
| Arrest at home residence, n (%) | 150 (44.5) | 419 (65.6) | <0.001 |
| Witnessed arrest, n (%) | 273 (81.0) | 477 (74.6) | 0.031 |
| Initial shockable rhythm, n (%) ** | 234 (69.4) | 227 (35.5) | <0.001 |
| Pre-hospital interventions | |||
| Bystander CPR, n (%) | 169 (50.1) | 281 (44.0) | 0.076 |
| Bystander AED, n (%) | 17 (5.0) | 23 (3.6) | 0.812 |
| Pre-hospital ROSC, n (%) | 140 (41.5) | 149 (23.3) | <0.001 |
| Timings | |||
| EMS response time (min), median (IQR) | 7.7 (6.2,9.8) | 8.0 (6.4,10.1) | 0.108 |
| No-flow time (min), median (IQR) | 11.8 (6.0,16.0) | 12.7 (8.0,18.0) | 0.005 |
| Low-flow time (min), median (IQR) | 7.6 (3.3,16.1) | 9.7 (5.8,17.8) | 0.069 |
| CA to CPR > 4 min, n(%) *** | 254 (79.9) | 516 (85.3) | 0.045 |
| CPR to ROSC > 20 min, n(%) **** | 16 (12.7) | 24 (19.4) | 0.207 |
| Hospital interventions | |||
| Epinephrine administration, n (%) | 180 (53.4) | 323 (50.5) | 0.433 |
| ECMO, n (%) | 4 (1.2) | 2 (0.3) | 0.219 |
| TTM, n (%) | 121 (35.9) | 137 (21.4) | <0.001 |
| Outcomes | |||
| 30-day survival, n (%) | 156 (46.3) | 141 (22.1) | <0.001 |
| Survival with CPC 1 or 2, n (%) | 108 (32.0) | 87 (13.6) | <0.001 |
| Early CAG (n = 337) | Delayed CAG (n = 64) | p-Value * | |
|---|---|---|---|
Severity of coronary artery disease
| 36 (10.7) 88 (26.1) 66 (19.6) 147 (43.6) | 13 (20.3) 17 (26.6) 15 (23.4) 19 (29.7) | 0.072 |
| Presence of thrombus ** | 59(32.8%) | 10(31.3%) | 1.000 |
Revascularization treatment
| 230 (68.2) 8 (2.4) 99 (29.4) | 32 (50.0) 2 (3.1) 30 (46.9) | 0.018 |
Antiplatelet therapy ***
| 175 (83.3) 100 (47.6) 72 (34.3) | 31 (93.9) 21 (63.6) 5 (15.2) | 0.188 0.128 0.046 |
| ∆Procedural success | 214 (91.8) | 28 (87.5) | 0.628 |
| IABP **** | 48 (14.2) | 5 (7.8) | 0.234 |
| ECMO **** | 12 (3.6) | 2 (3.1) | 1.000 |
Complications **
| 5 (2.0) 42 (17.1) 4 (1.6) 0 (0.0) | 0 (0.0) 3 (5.8) 1 (1.9) 0 (0.0) | 0.300 0.039 0.880 NA |
| (a): Early CAG regardless of revascularization. | ||||
| 30-Day Survival | Discharged with CPC 1 or 2 | |||
| Variable | Adjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value |
| Age | 0.98 (0.97,0.99) | 0.001 | 0.96 (0.95,0.98) | <0.001 |
| Male sex | 1.01 (0.67,1.52) | 0.956 | 1.37 (0.82,2.29) | 0.230 |
| Heart disease | 0.60 (0.42,0.84) | 0.004 | 0.80 (0.53,1.22) | 0.307 |
| Arrest at home | 0.52 (0.37,0.73) | <0.001 | 0.46 (0.31,0.69) | <0.001 |
| Witnessed arrest | 1.39 (0.90,2.16) | 0.139 | 1.35 (0.77,2.38) | 0.296 |
| Initial shockable rhythm | 5.72 (3.96,8.26) | <0.001 | 6.24 (3.88,10.04) | <0.001 |
| Bystander CPR | 1.19 (0.83,1.71) | 0.345 | 1.69 (1.08,2.64) | 0.021 |
| CA to CPR >4 min | 0.72 (0.43,1.18) | 0.190 | 0.36 (0.20,0.64) | 0.001 |
| Epinephrine administration | 0.29 (0.21,0.41) | <0.001 | 0.14 (0.09,0.22) | <0.001 |
| Early CAG | 1.59 (1.12,2.26) | 0.010 | 1.54 (1.01,2.34) | 0.045 |
| (b) Early CAG with and without immediate PCI. | ||||
| 30-Day Survival | Discharged with CPC 1 or 2 | |||
| Variable | Adjusted or (95% CI) | p-Value | Adjusted or (95% CI) | p-Value |
| Age | 0.98 (0.97,0.99) | 0.001 | 0.96 (0.95,0.98) | <0.001 |
| Male sex | 1.00 (0.67,1.51) | 0.984 | 1.35 (0.81,2.27) | 0.255 |
| Heart disease | 0.63 (0.44,0.89) | 0.010 | 0.85 (0.55,1.30) | 0.451 |
| Arrest at home | 0.53 (0.38,0.74) | <0.001 | 0.46 (0.31,0.70) | <0.001 |
| Witnessed arrest | 1.38 (0.89,2.13) | 0.155 | 1.33 (0.76,2.35) | 0.320 |
| Initial shockable rhythm | 5.64 (3.90,8.16) | <0.001 | 6.17 (3.83,9.95) | <0.001 |
| Bystander CPR | 1.19 (0.83,1.71) | 0.337 | 1.72 (1.10,2.69) | 0.018 |
| CA to CPR >4 min | 0.73 (0.44,1.22) | 0.229 | 0.37 (0.20,0.66) | 0.001 |
| Epinephrine administration | 0.29 (0.21,0.41) | <0.001 | 0.14 (0.09,0.22) | <0.001 |
| Coronary interventions | ||||
| -No or delayed CAG | Reference | Reference | ||
| -Early CAG without PCI | 1.06 (0.62,1.80) | 0.843 | 0.99 (0.52,1.91) | 0.984 |
| -Early CAG with immediate PCI | 1.91 (1.29,2.84) | 0.001 | 1.82 (1.15,2.88) | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, S.L.; Lau, Y.H.; Chan, M.Y.; Chua, T.; Tan, H.C.; Foo, D.; Lim, Z.Y.; Liew, B.W.; Shahidah, N.; Mao, D.R.; et al. Early Coronary Angiography Is Associated with Improved 30-Day Outcomes among Patients with Out-of-Hospital Cardiac Arrest. J. Clin. Med. 2021, 10, 5191. https://doi.org/10.3390/jcm10215191
Lim SL, Lau YH, Chan MY, Chua T, Tan HC, Foo D, Lim ZY, Liew BW, Shahidah N, Mao DR, et al. Early Coronary Angiography Is Associated with Improved 30-Day Outcomes among Patients with Out-of-Hospital Cardiac Arrest. Journal of Clinical Medicine. 2021; 10(21):5191. https://doi.org/10.3390/jcm10215191
Chicago/Turabian StyleLim, Shir Lynn, Yee How Lau, Mark Y. Chan, Terrance Chua, Huay Cheem Tan, David Foo, Zhan Yun Lim, Boon Wah Liew, Nur Shahidah, Desmond R. Mao, and et al. 2021. "Early Coronary Angiography Is Associated with Improved 30-Day Outcomes among Patients with Out-of-Hospital Cardiac Arrest" Journal of Clinical Medicine 10, no. 21: 5191. https://doi.org/10.3390/jcm10215191
APA StyleLim, S. L., Lau, Y. H., Chan, M. Y., Chua, T., Tan, H. C., Foo, D., Lim, Z. Y., Liew, B. W., Shahidah, N., Mao, D. R., Cheah, S. O., Chia, M. Y. C., Gan, H. N., Leong, B. S. H., Ng, Y. Y., Yeo, K. K., & Ong, M. E. H. (2021). Early Coronary Angiography Is Associated with Improved 30-Day Outcomes among Patients with Out-of-Hospital Cardiac Arrest. Journal of Clinical Medicine, 10(21), 5191. https://doi.org/10.3390/jcm10215191