
Feasibility and Safety of Stentless Uretero-Intestinal Anastomosis in Radical Cystectomy with Ileal Orthotopic Neobladder


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Surgical Technique of UIA
2.4. Perioperative Management
2.5. Patient Follow-up Protocol
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Comperat, E.M.; Cowan, N.C.; Gakis, G.; Hernandez, V.; Linares Espinos, E.; Lorch, A.; Neuzillet, Y.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur. Urol. 2021, 79, 82–104. [Google Scholar] [CrossRef]
- Stein, J.P.; Lieskovsky, G.; Cote, R.; Groshen, S.; Feng, A.C.; Boyd, S.; Skinner, E.; Bochner, B.; Thangathurai, D.; Mikhail, M.; et al. Radical cystectomy in the treatment of invasive bladder cancer: Long-term results in 1054 patients. J. Clin. Oncol. 2001, 19, 666–675. [Google Scholar] [CrossRef]
- Ahmadi, H.; Skinner, E.C.; Simma-Chiang, V.; Miranda, G.; Cai, J.; Penson, D.F.; Daneshmand, S. Urinary functional outcome following radical cystoprostatectomy and ileal neobladder reconstruction in male patients. J. Urol. 2013, 189, 1782–1788. [Google Scholar] [CrossRef]
- Studer, U.E.; Burkhard, F.C.; Schumacher, M.; Kessler, T.M.; Thoeny, H.; Fleischmann, A.; Thalmann, G.N. Twenty years experience with an ileal orthotopic low pressure bladder substitute--lessons to be learned. J. Urol. 2006, 176, 161–166. [Google Scholar] [CrossRef]
- Lawrentschuk, N.; Colombo, R.; Hakenberg, O.W.; Lerner, S.P.; Mansson, W.; Sagalowsky, A.; Wirth, M.P. Prevention and management of complications following radical cystectomy for bladder cancer. Eur. Urol. 2010, 57, 983–1001. [Google Scholar] [CrossRef] [PubMed]
- Shimko, M.S.; Tollefson, M.K.; Umbreit, E.C.; Farmer, S.A.; Blute, M.L.; Frank, I. Long-term complications of conduit urinary diversion. J. Urol. 2011, 185, 562–567. [Google Scholar] [CrossRef]
- Shabsigh, A.; Korets, R.; Vora, K.C.; Brooks, C.M.; Cronin, A.M.; Savage, C.; Raj, G.; Bochner, B.H.; Dalbagni, G.; Herr, H.W.; et al. Defining early morbidity of radical cystectomy for patients with bladder cancer using a standardized reporting methodology. Eur. Urol. 2009, 55, 164–174. [Google Scholar] [CrossRef]
- Hautmann, R.E.; de Petriconi, R.C.; Volkmer, B.G. 25 years of experience with 1000 neobladders: Long-term complications. J. Urol. 2011, 185, 2207–2212. [Google Scholar] [CrossRef]
- Shah, S.H.; Movassaghi, K.; Skinner, D.; Dalag, L.; Miranda, G.; Cai, J.; Schuckman, A.; Daneshmand, S.; Djaladat, H. Ureteroenteric Strictures After Open Radical Cystectomy and Urinary Diversion: The University of Southern California Experience. Urology 2015, 86, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.Y.; Boorjian, S.A.; Westerman, M.B.; Tarrell, R.F.; Thapa, P.; Viers, B.R. Persistent, long-term risk for ureteroenteric anastomotic stricture formation: The case for long term follow-up. Transl. Androl. Urol. 2020, 9, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Goh, A.C.; Belarmino, A.; Patel, N.A.; Sun, T.; Sedrakyan, A.; Bochner, B.H.; Hu, J.C. A Population-based Study of Ureteroenteric Strictures After Open and Robot-assisted Radical Cystectomy. Urology 2020, 135, 57–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amin, K.A.; Vertosick, E.A.; Stearns, G.; Fathollahi, A.; Sjoberg, D.D.; Donat, M.S.; Herr, H.; Bochner, B.; Dalbagni, G.; Sandhu, J.S. Predictors of Benign Ureteroenteric Anastomotic Strictures After Radical Cystectomy and Urinary Diversion. Urology 2020, 144, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Large, M.C.; Cohn, J.A.; Kiriluk, K.J.; Dangle, P.; Richards, K.A.; Smith, N.D.; Steinberg, G.D. The impact of running versus interrupted anastomosis on ureterointestinal stricture rate after radical cystectomy. J. Urol. 2013, 190, 923–927. [Google Scholar] [CrossRef]
- Jarowenko, M.V.; Bennett, A.H. Use of single J urinary diversion stents in intestinal urinary diversion. Urology 1983, 22, 369–370. [Google Scholar] [CrossRef]
- Regan, J.B.; Barrett, D.M. Stented versus nonstented ureteroileal anastomoses: Is there a difference with regard to leak and stricture? J. Urol. 1985, 134, 1101–1103. [Google Scholar] [CrossRef]
- Mullins, J.K.; Guzzo, T.J.; Ball, M.W.; Pierorazio, P.M.; Eifler, J.; Jarrett, T.W.; Schoenberg, M.P.; Bivalacqua, T.J. Ureteral stents placed at the time of urinary diversion decreases postoperative morbidity. Urol. Int. 2012, 88, 66–70. [Google Scholar] [CrossRef] [Green Version]
- Mattei, A.; Birkhaeuser, F.D.; Baermann, C.; Warncke, S.H.; Studer, U.E. To stent or not to stent perioperatively the ureteroileal anastomosis of ileal orthotopic bladder substitutes and ileal conduits? Results of a prospective randomized trial. J. Urol. 2008, 179, 582–586. [Google Scholar] [CrossRef]
- Kolwijck, E.; Seegers, A.E.M.; Tops, S.C.M.; van der Heijden, A.G.; Sedelaar, J.P.M.; Ten Oever, J. Incidence and microbiology of post-operative infections after radical cystectomy and ureteral stent removal; a retrospective cohort study. BMC Infect. Dis. 2019, 19, 303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donat, S.M.; Tan, K.S.; Jibara, G.; Dalbagni, G.; Carlon, V.A.; Sandhu, J. Intraoperative Ureteral Stent Use at Radical Cystectomy is Associated with Higher 30-Day Complication Rates. J. Urol. 2021, 205, 483–490. [Google Scholar] [CrossRef]
- Song, W.; Yoon, H.S.; Kim, K.H.; Yoon, H.; Chung, W.S.; Sim, B.S.; Lee, D.H. Role of bowel suspension technique to prevent early intestinal obstruction after radical cystectomy with ileal orthotopic neobladder: A retrospective cohort study. Int. J. Surg. 2018, 55, 9–14. [Google Scholar] [CrossRef]
- Kouba, E.; Sands, M.; Lentz, A.; Wallen, E.; Pruthi, R.S. A comparison of the Bricker versus Wallace ureteroileal anastomosis in patients undergoing urinary diversion for bladder cancer. J. Urol. 2007, 178, 945–948. [Google Scholar] [CrossRef] [PubMed]
- Tal, R.; Sivan, B.; Kedar, D.; Baniel, J. Management of benign ureteral strictures following radical cystectomy and urinary diversion for bladder cancer. J. Urol. 2007, 178, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Nassar, O.A.; Alsafa, M.E. Experience with ureteroenteric strictures after radical cystectomy and diversion: Open surgical revision. Urology 2011, 78, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Malangone-Monaco, E.; Wilson, K.; Diakun, D.; Tayama, D.; Satram, S.; Ogale, S. Cost of cystectomy-related complications in patients with bladder cancer in the United States. Curr. Med. Res. Opin. 2020, 36, 1177–1185. [Google Scholar] [CrossRef]
- Haider, M.; Ladurner, C.; Mayr, R.; Tandogdu, Z.; Fritsche, H.M.; Fradet, V.; Comploj, E.; Pycha, A.; Lemire, F.; Lacombe, L.; et al. Use and duration of antibiotic prophylaxis and the rate of urinary tract infection after radical cystectomy for bladder cancer: Results of a multicentric series. Urol. Oncol. 2019, 37, 300.e309–300.e315. [Google Scholar] [CrossRef]
- Vetterlein, M.W.; Klemm, J.; Gild, P.; Bradtke, M.; Soave, A.; Dahlem, R.; Fisch, M.; Rink, M. Improving Estimates of Perioperative Morbidity After Radical Cystectomy Using the European Association of Urology Quality Criteria for Standardized Reporting and Introducing the Comprehensive Complication Index. Eur. Urol. 2020, 77, 55–65. [Google Scholar] [CrossRef]
- Parekh, D.J.; Reis, I.M.; Castle, E.P.; Gonzalgo, M.L.; Woods, M.E.; Svatek, R.S.; Weizer, A.Z.; Konety, B.R.; Tollefson, M.; Krupski, T.L.; et al. Robot-assisted radical cystectomy versus open radical cystectomy in patients with bladder cancer (RAZOR): An open-label, randomised, phase 3, non-inferiority trial. Lancet 2018, 391, 2525–2536. [Google Scholar] [CrossRef]
- Hirobe, M.; Tanaka, T.; Shindo, T.; Ichihara, K.; Hotta, H.; Takahashi, A.; Kato, R.; Yanase, M.; Matsukawa, M.; Itoh, N.; et al. Complications within 90 days after radical cystectomy for bladder cancer: Results of a multicenter prospective study in Japan. Int. J. Clin. Oncol. 2018, 23, 734–741. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Total | Uretero-Intestinal Anastomosis Stricture | p | |
|---|---|---|---|---|
| Yes | No | |||
| No. of patients | 403 (100.0) | 39 (9.7) | 364 (90.3) | |
| Age at surgery, years | 0.622 | |||
| Median (range) | 66.0 (27.0–84.0) | 67.0 (34.0–81.0) | 66.0 (27.0–84.0) | |
| Mean (SD) | 63.9 (10.3) | 64.7 (10.2) | 63.8 (10.4) | |
| Sex, N (%) | 0.493 | |||
| Male | 336 (83.4) | 31 (79.5) | 305 (83.8) | |
| Female | 67 (16.6) | 8 (20.5) | 59 (16.2) | |
| Body mass index, kg/m2 | 0.068 | |||
| Median (range) | 24.0 (15.0–38.7) | 25.3 (17.3–31.6) | 23.9 (15.0–38.7) | |
| Mean (SD) | 24.2 (3.2) | 25.1 (3.4) | 24.1 (3.2) | |
| Diabetes mellitus, N (%) | 0.017 | |||
| Yes | 69 (17.1) | 12 (30.8) | 57 (15.7) | |
| No | 334 (82.9) | 27 (69.2) | 307 (84.3) | |
| ASA score, N (%) | 0.119 | |||
| 1 | 53 (13.2) | 2 (5.1) | 51 (14.0) | |
| 2–3 | 350 (86.8) | 37 (94.9) | 313 (86.0) | |
| Neoadjuvant chemotherapy, n (%) | < 0.001 | |||
| Yes | 48 (11.9) | 12 (30.8) | 36 (9.9) | |
| No | 355 (88.1) | 27 (69.2) | 328 (90.1) | |
| Preoperative radiotherapy, n (%) | 0.400 | |||
| Yes | 5 (1.2) | 1 (2.6) | 4 (1.1) | |
| No | 398 (98.8) | 38 (97.4) | 360 (98.9) | |
| Operation time, min | 0.051 | |||
| Median (range) | 265.0 (175.0–480.0) | 275.0 (195.0–455.0) | 265.0 (175.0–480.0) | |
| Mean (SD) | 271.4 (46.9) | 285.4 (55.2) | 269.9 (45.8) | |
| Estimated blood loss, mL | 0.225 | |||
| Median (range) | 500.0 (100.0–2200.0) | 500.0 (200.0–1500.0) | 475.0 (100.0–2200.0) | |
| Mean (SD) | 520.9 (279.2) | 572.6 (311.9) | 515.4 (275.4) | |
| Pathologic T stage, N (%) | 0.102 | |||
| ≤pT2 (organ confined) | 255 (63.3) | 20 (51.3) | 235 (64.6) | |
| ≥pT3 (locally advanced) | 148 (36.7) | 19 (48.7) | 129 (35.4) | |
| Pathologic N stage, N (%) | 0.344 | |||
| N0/Nx | 304 (75.4) | 27 (69.2) | 277 (76.1) | |
| N1–3 | 99 (24.6) | 12 (30.8) | 87 (23.9) | |
| Surgical margin status, N (%) | 0.196 | |||
| Positive | 64 (15.9) | 9 (23.1) | 55 (15.1) | |
| Negative | 339 (84.1) | 30 (76.9) | 309 (84.9) | |
| Hospital stay, days | 0.287 | |||
| Median (range) | 15.0 (6.0–51.0) | 16.0 (13.0–36.0) | 15.0 (6.0–51.0) | |
| Mean (SD) | 17.7 (6.8) | 18.8 (5.9) | 17.6 (6.9) | |
| Adjuvant chemotherapy, n (%) | 0.717 | |||
| Yes | 175 (43.4) | 18 (46.2) | 157 (43.1) | |
| No | 228 (56.6) | 21 (53.8) | 207 (56.9) | |
| Renal units, n (%) | ||||
| Bilateral | 387 (96.0) | |||
| Left only | 9 (2.2) | |||
| Right only | 7 (1.8) | |||
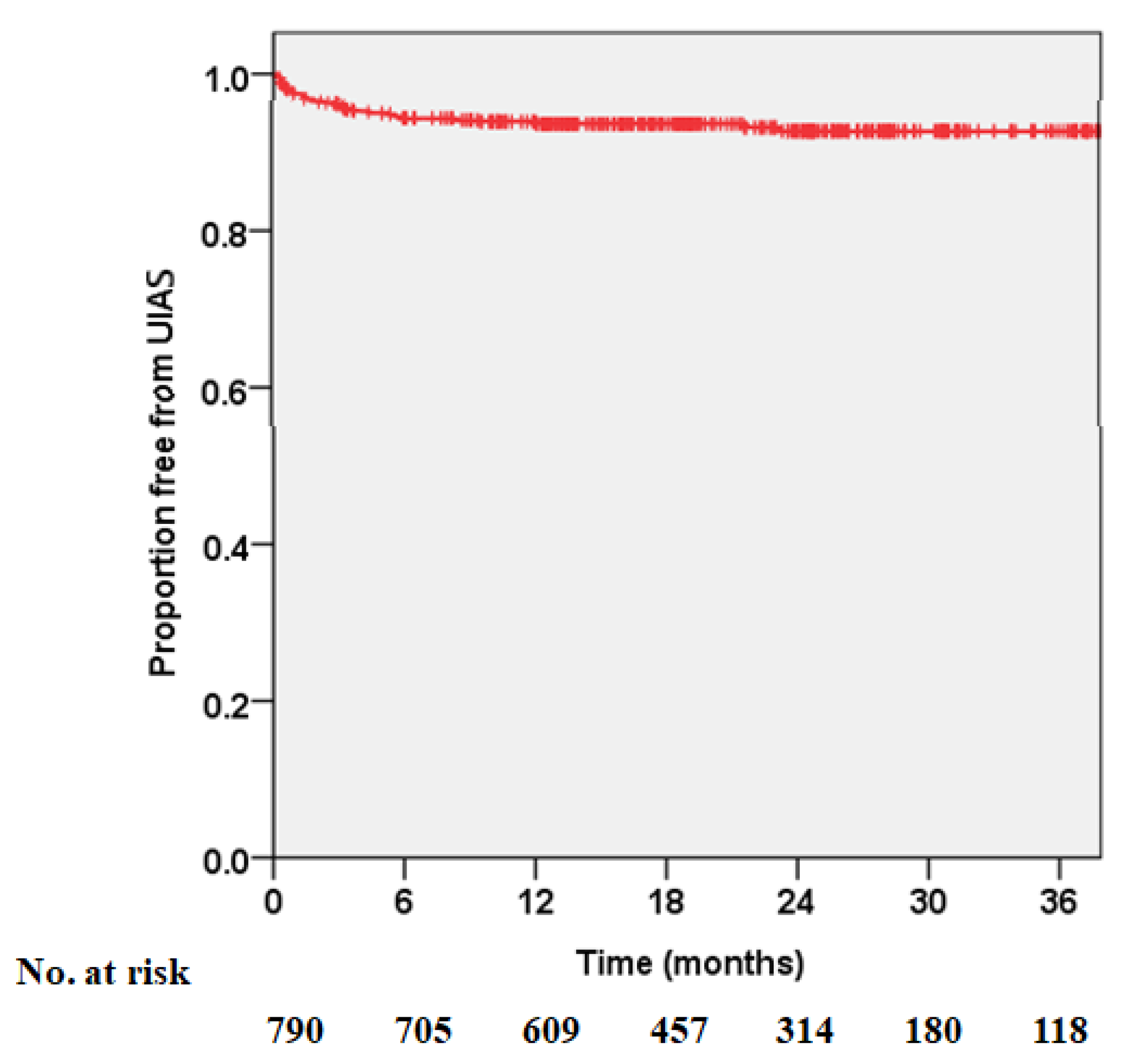
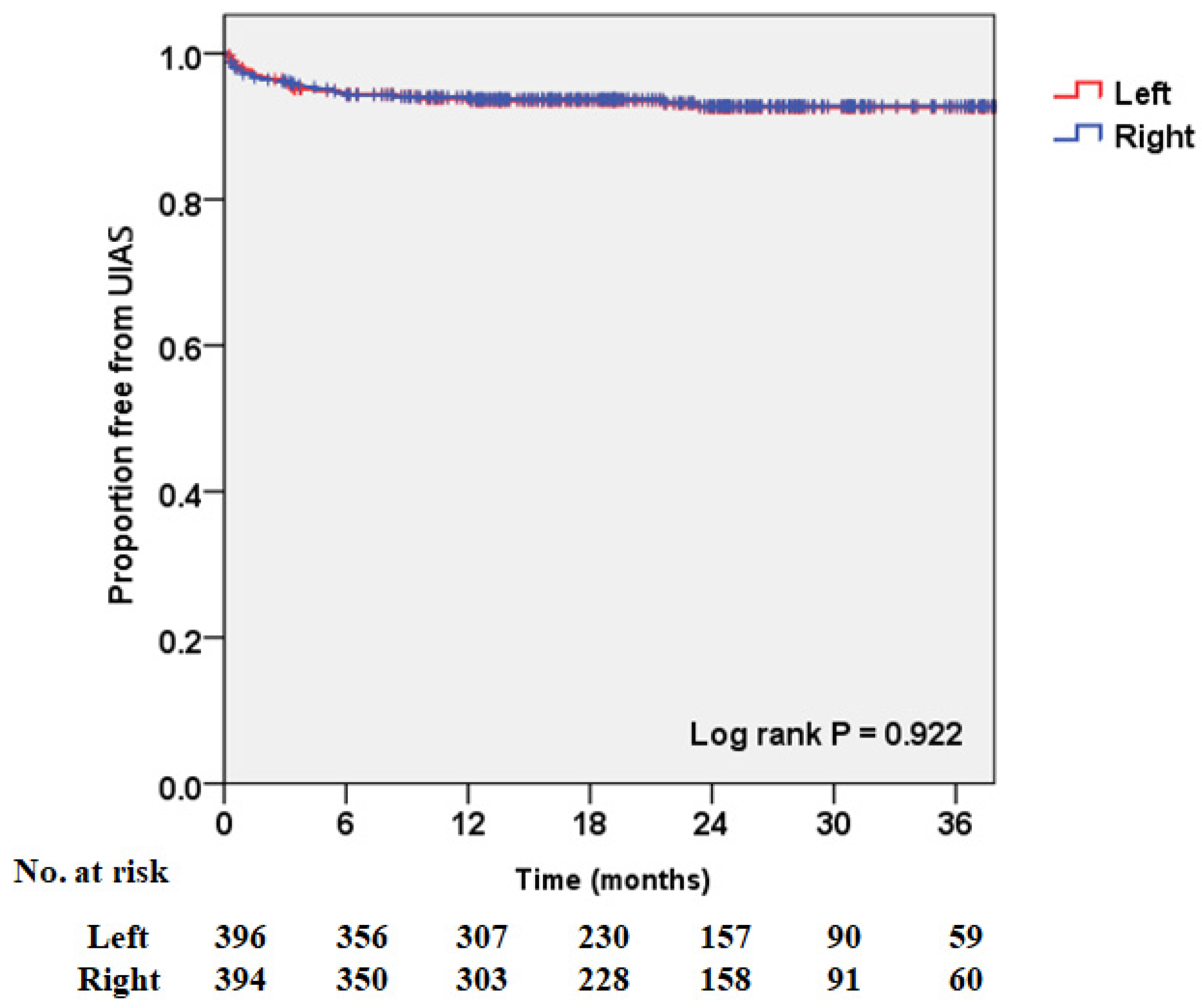
| Laterality of stricture, n (%) | ||||
| Left only | 13 (33.3) | |||
| Right only | 12 (30.8) | |||
| Bilateral | 14 (35.9) | |||
| Follow-up, months | 0.329 | |||
| Median (range) | 24.3 (2.9–56.7) | 24.4 (12.2–29.0) | 24.0 (2.9–56.7) | |
| Mean (SD) | 24.4 (11.3) | 23.6 (3.7) | 24.5 (11.8) | |
| Study | Amin et al. [12] | Goh et al. [11] | Yang et al. [10] | Shah et al. [9] | Shimko et al. [6] | Hautmann et al. [8] | Shabsigh et al. [7] | Current Study |
|---|---|---|---|---|---|---|---|---|
| Study interval | 1995–2014 | 2009–2014 | 1980–2008 | 1971–2008 | 1980–1998 | 1986–2008 | 1995–2005 | 2014–2018 |
| No. of patients | 2888 | 1449 | 2285 | 1964 | 1057 | 923 | 1142 | 403 |
| Male, % | 74.1 | 79.9 | 81.4 | NA | 79.7 | 86.1 | 75.5 | 83.4 |
| Age, year | ||||||||
| Median (range) | 68 (60–75) * | NA | 68 (62–75) * | NA | 69 (31–92) | NA | 68 (60–75) * | 66 (27–84) |
| BMI, kg/m2 | ||||||||
| Median (range) | 28 (25–30) * | NA | 27.0(24–30) * | NA | NA | NA | 27.1(24–30) * | 24.0(15.0–38.7) |
| Neobladder, % | 33.6 | 7.9 | 21.6 | 80.2 | 0 | 100 | 36.6 | 100 |
| UIAS | ||||||||
| Renal units, n (%) | NA | NA | NA | 51 (NA) | NA | NA | NA | 53 (6.7) |
| Patients, % | 4.3 | 4.2–8.3 | 8.4 | 2.5 | 11.5 | 11.1 | 3.9 | 9.7 |
| Male, % | NA | NA | 82.3 | 85.7 | NA | NA | NA | 79.5 |
| Laterality, % | ||||||||
| Left only | 53.7 | NA | 53.1 | 66.0 | NA | NA | NA | 33.3 |
| Right only | 40.7 | NA | 28.1 | 29.0 | NA | NA | NA | 30.8 |
| Bilateral | 5.7 | NA | 18.8 | 5.0 | NA | NA | NA | 35.9 |
| Study | Malangone-Monaco et al. [24] (2020) | Vetterlein et al. [26] (2020) | Haider et al. [25] (2019) | Parekh et al. [27] (2018) | Hirobe et al. [28] (2018) | Current Study |
|---|---|---|---|---|---|---|
| Study design | Retrospective | Retrospective | Retrospective | Multicenter randomized controlled trial | Prospective | Retrospective |
| Study interval | 2005–2015 | 2009–2017 | 2009–2015 | 2011–2014 | 2010–2014 | 2014–2018 |
| No. of patients | 4648 | 506 | 217 | 152 | 185 | 403 |
| Male, % | 78.7 | 79.0 | 78.3 | 84.0 | 79.4 | 83.4 |
| Age, year | ||||||
| Median (range) | 67.6 (NA) | 69 (62–74) * | 72 (64–78.5) * | 67 (37–85) | 72 (39–89) | 66 (27–84) |
| BMI, kg/m2 | 26.1 | 28.2 | 23.4 | 24.0 | ||
| Median (range) | NA | 26 (24–29) * | (23.2–29.7) * | (24.9–31.7) * | (15.2–34.2) | (15.0–38.7) |
| Neobladder, % | NA | 27 | 28.1 | 20.0 | 8.1 | 100 |
| Complications, % | ||||||
| Paralytic ileus | 15.8 | 7.1 | NA | 20.0 | 22.2 | 26.1 |
| Febrile UTI | 25.3 | 62.0 | 19.4 | 26.0 | 29.7 | 14.1 |
| Urine leak at UIA | NA | 2.0 | NA | 3.0 | 2.7 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.U.; Lee, J.H.; Lee, D.H.; Song, W. Feasibility and Safety of Stentless Uretero-Intestinal Anastomosis in Radical Cystectomy with Ileal Orthotopic Neobladder. J. Clin. Med. 2021, 10, 5372. https://doi.org/10.3390/jcm10225372
Lee CU, Lee JH, Lee DH, Song W. Feasibility and Safety of Stentless Uretero-Intestinal Anastomosis in Radical Cystectomy with Ileal Orthotopic Neobladder. Journal of Clinical Medicine. 2021; 10(22):5372. https://doi.org/10.3390/jcm10225372
Chicago/Turabian StyleLee, Chung Un, Jong Hoon Lee, Dong Hyeon Lee, and Wan Song. 2021. "Feasibility and Safety of Stentless Uretero-Intestinal Anastomosis in Radical Cystectomy with Ileal Orthotopic Neobladder" Journal of Clinical Medicine 10, no. 22: 5372. https://doi.org/10.3390/jcm10225372
APA StyleLee, C. U., Lee, J. H., Lee, D. H., & Song, W. (2021). Feasibility and Safety of Stentless Uretero-Intestinal Anastomosis in Radical Cystectomy with Ileal Orthotopic Neobladder. Journal of Clinical Medicine, 10(22), 5372. https://doi.org/10.3390/jcm10225372