
State of Evidence on Oral Health Problems in Diabetic Patients: A Critical Review of the Literature



Abstract
:1. Introduction
2. Scientific Framework
3. Periodontitis
3.1. Mechanisms Linking DM and PD
3.1.1. Impact of DM on the Oral Microbiota
3.1.2. Pro-Inflammatory Mediators in Patients with PD and DM
3.1.3. Role of Advanced Glycation End Products (AGE) and Its Receptor (RAGE) in the Development of PD in Diabetes
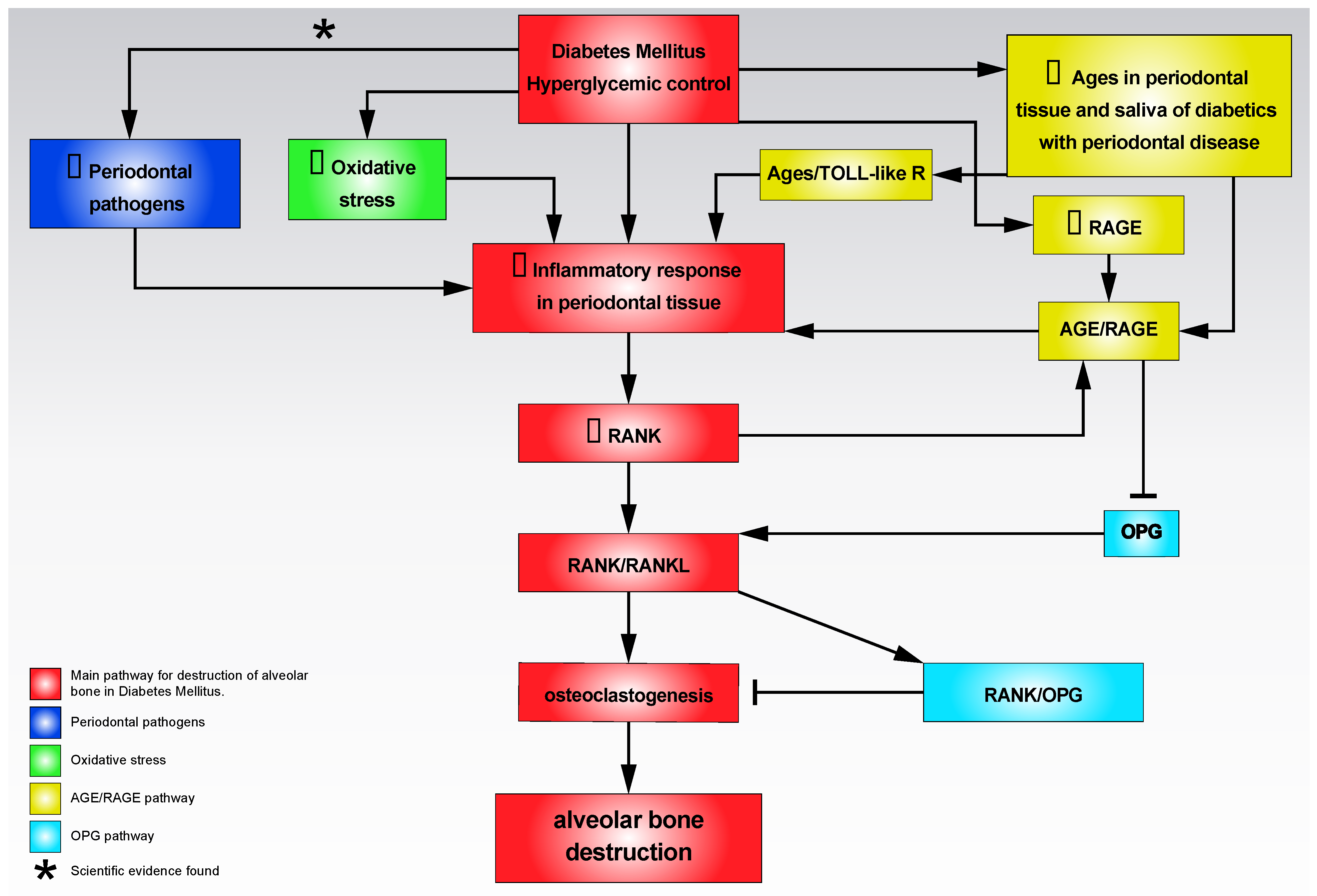
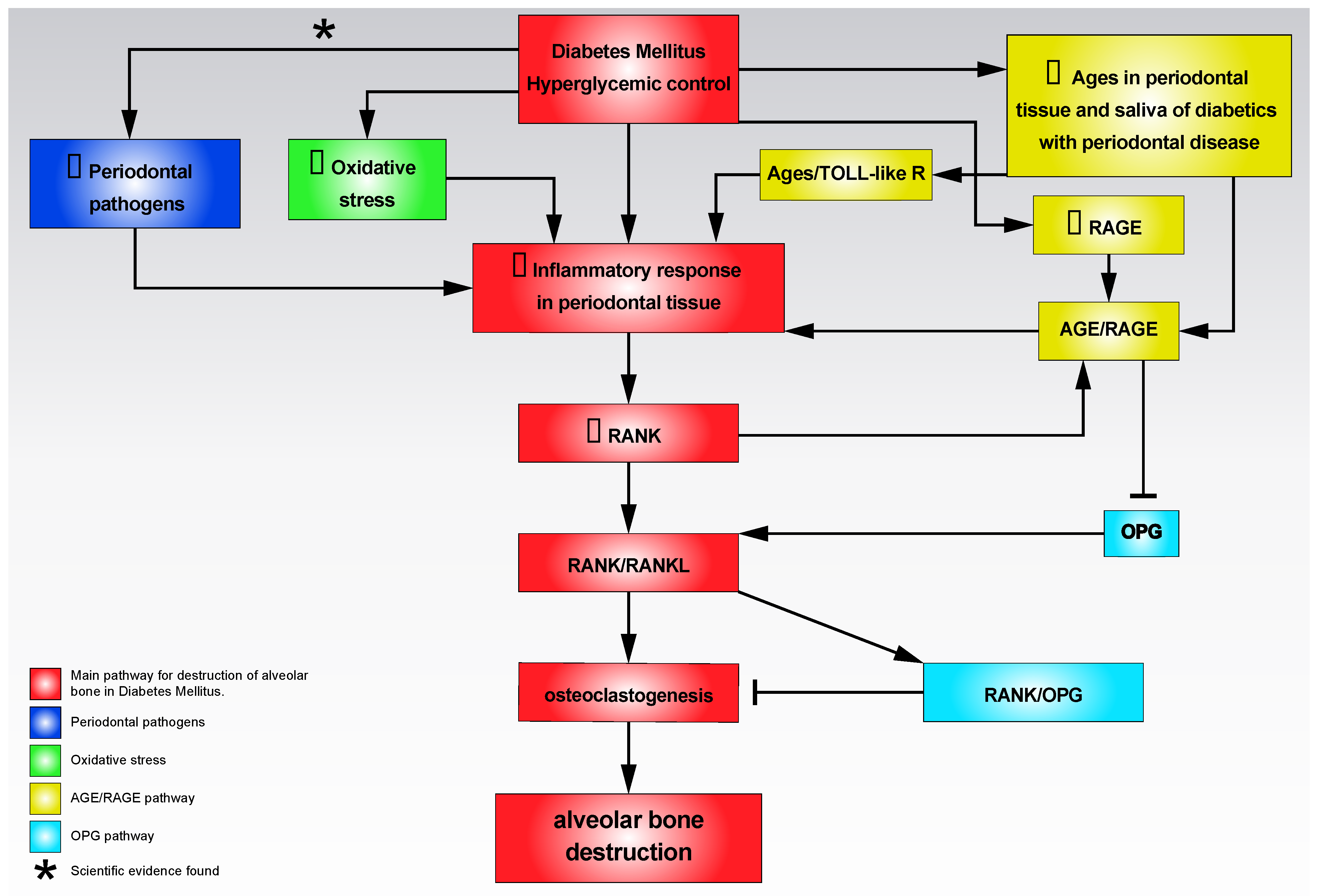
3.1.4. Role of Hyperglycemia in Bone Destruction in PD
3.2. DM Increases the Severity of PD
3.3. PD Worsens the Control and Prognosis of DM
3.4. Dental Implants, Peri-Implantitis, and DM
4. Oral Candidiasis
5. Oral Cancer and Oral Potentially Malignant Disorders
6. Other Oral Conditions Associated with DM
6.1. Dental Caries
6.2. Burning Mouth Syndrome (BMS)
6.3. Salivary Secretion Alterations
6.4. Taste Perception Alterations
6.5. Halitosis
6.6. Delayed Wound Healing
7. Need for an Interdisciplinary Team in the Care of Diabetic Patients in Relation to Their Oral Health. Information to the Diabetic Patients about Their Oral Health
7.1. Attitude of Primary Care Physicians and Specialists Involved in the Management of Diabetic Patients in Relation to Their Oral Health Care
- Clinicians should discuss with diabetic patients the importance of oral health in their disease in relation to the influence it exerts on the metabolic control of the disease and on the reduction of the risk of developing some of the potential complications of DM. Likewise, diabetic patient should be advised to periodically go to the dental clinic for review their oral status [69];
- Clinicians should screen for the main oral conditions that occur in diabetes. This screening should include the evaluation of the periodontal status through simple questions about the existence of spontaneous gingival bleeding or during mastication and brushing, the appearance of mobility or displacement of teeth, the loss of teeth, the presence of halitosis, and the existence of suppuration or periodontal abscesses. Likewise, the presence of erythematous or pseudomembranous candidiasis should be evaluated both through the presence of its symptoms (itching or oral pain) and its signs (oral mucosa affected by extensive red areas and imprecise limits or white areas in the form of lumps that come off easily when scraped with gauze);
- Clinicians should perform a scrutiny of salivary flow alterations, essentially questioning the patient about the presence of dry mouth symptoms and examining the oral mucosa (obvious absence of saliva or thick saliva, with a parchment-like appearance of the oral mucosa);
- Clinicians should refer diabetic patients to the dental office in the event of any oral health problem detected during control and follow-up visits;
- Clinicians should seek basic training in oral health that allows them to detect the presence of oral disorders that appear in diabetes.
7.2. Attitude of Dentists in the Management of Diabetic Patients in Relation to Their Oral Health Care
- Dentists should promote lifestyle changes on the habits of diabetic patients in order to exert a favorable impact on their oral and general health;
- Dentists must promote attitudes aimed at obtaining the maximum efficiency of oral care in diabetics [43,244]:
- -
- The medical history should be meticulous and detailed;
- -
- Communication with primary care physicians and other specialists involved in the care of diabetics should be fluid;
- -
- The intraoral examination should be meticulous looking for the frequent oral alterations in diabetics, with special reference to the signs and symptoms of PD, oral candidiasis, dry mouth and the presence of OPMD and oral cancer.
- The dental treatment of diabetics should focus on the control of acute infection, offering a therapy plan that is as less complex as possible. Likewise, emergencies in the dental clinic (hyperglycemia, hypoglycemia) must be recognized early and adequately managed. Considerations should be given to which are the most appropriate times to perform dental treatments and what should be the optimal duration of appointments, planning the treatment according to difficulties. Deep anesthesia and good pain and stress control should be provided during treatment;
- Dentists should advise and promote the replacement of missing teeth, the restoration of decayed teeth, and the implementation of preventive oral health habits;
- The dentist must be aware of the existence of the growing number of diabetics in the world [245], many of whom are undiagnosed [246,247]. Dental clinics could act as linkers involved in diabetes screening. In this sense, the suspicion of diabetes in a dental patient should prompt the dentist to request a check of glucose levels in venous blood and in case of alteration, the referral of the patient to his primary care physician for study and treatment if necessary [248];
- Dentists should seek basic training on DM and its complications.
7.3. Information Diabetic Patients Should Receive about Their Oral Health
- Diabetic patients should be given information about their oral health and its relationship to diabetes;
- Diabetic patients should receive information from dentists on the higher prevalence of PD in DM and on the negative consequences this has for the metabolic control of diabetes and on the presentation of complications of diabetes;
- Diabetic patients should receive information from dentists on habits and lifestyle that prevent the development of oral complications of diabetes;
- Diabetic patients should know that they are at risk of developing oral candidiasis;
- Diabetic patients should know that they are at risk of developing oral cancer and OPMD, through accurate, evidence-based information;
- Diabetic patients should know that they could develop alterations in salivary flow with dryness related to their disease;
- Diabetic patients should know the importance of making regular visits to the dental clinic;
- Diabetic patients must make commitments to their oral care.
7.4. Practical Measures and Recommendations to Follow in a Routine Dental Care Session
- Prior to dental treatment, a comprehensive medical history should be performed, singularly recording the type of diabetes, complications, treatment, and control status [249];
- International consensus guidelines state HbA1c levels <6.5% as the main parameter to measure and confirm an appropriate metabolic control [250];
- Pre-prandial blood glucose levels ranging between 70 and 130 mg/dL and post-prandial blood glucose levels < 180 mg/dL also should be confirmed to ensure an adequate metabolic control [250];
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Diedisheim, M.; Carcarino, E.; Vandiedonck, C.; Roussel, R.; Gautier, J.-F.; Venteclef, N. Regulation of inflammation in diabetes: From genetics to epigenomics evidence. Mol. Metab. 2020, 41, 101041. [Google Scholar] [CrossRef] [PubMed]
- Karolina, D.S.; Armugam, A.; Sepramaniam, S.; Jeyaseelan, K. miRNAs and diabetes mellitus. Expert Rev. Endocrinol. Metab. 2012, 7, 281–300. [Google Scholar] [CrossRef] [PubMed]
- Xie, Z.; Chang, C.; Huang, G.; Zhou, Z. The Role of Epigenetics in Type 1 Diabetes. Epigenet. Allergy Autoimmun. 2020, 1253, 223–257. [Google Scholar] [CrossRef]
- Florez, J.C.; Jablonski, K.A.; Bayley, N.; Pollin, T.I.; de Bakker, P.I.W.; Shuldiner, A.R.; Knowler, W.C.; Nathan, D.M.; Altshuler, D. TCF7L2 Polymorphisms and progression to diabetes in the diabetes prevention program. N. Engl. J. Med. 2006, 355, 241–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blake, R.; Trounce, I.A. Mitochondrial dysfunction and complications associated with diabetes. Biochim. Biophys. Acta-Gen. Subj. 2014, 1840, 1404–1412. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.; Rodrigues, M.; Henriques, M. Candida sp. Infections in patients with diabetes mellitus. J. Clin. Med. 2019, 8, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 89, S1–S8. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamey, P.-J.; Darwaza, A.; Fisher, B.M.; Samaranayake, L.P.; Macfarlane, T.W.; Frier, B.M. Secretor status, candidal carriage and candidal infection in patients with diabetes mellitus. J. Oral Pathol. Med. 1988, 17, 354–357. [Google Scholar] [CrossRef] [PubMed]
- Belazi, M.; Velegraki, A.; Fleva, A.; Gidarakou, I.; Papanaum, L.; Baka, D.; Daniilidou, N.; Karamitsos, D. Candidal overgrowth in diabetic patients: Potential predisposing factors. Mycoses 2005, 48, 192–196. [Google Scholar] [CrossRef]
- Chi, A.C.; Day, T.A.; Neville, B.W. Oral cavity and oropharyngeal squamous cell carcinoma-an update. CA Cancer J. Clin. 2015, 65, 401–421. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Garcia, P.; Roca-Rodriguez, M.D.M.; Aguilar-Diosdado, M.; Gonzalez-Moles, M.A. Diabetes mellitus and oral cancer/oral potentially malignant disorders: A systematic review and meta-analysis. Oral Dis. 2021, 27, 404–421. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S.; Kujan, O.; Aguirre-Urizar, J.M.; Bagan, J.V.; González-Moles, M.Á.; Kerr, A.R.; Lodi, G.; Mello, F.W.; Monteiro, L.; Ogden, G.R.; et al. Oral potentially malignant disorders: A consensus report from an international seminar on nomenclature and classification, convened by the WHO collaborating centre for oral cancer. Oral Dis. 2021, 27, 1862–1880. [Google Scholar] [CrossRef]
- D’Aiuto, F.; Gable, D.; Syed, Z.; Allen, Y.; Wanyonyi, K.L.; White, S.; Gallagher, J.E. Evidence summary: The relationship between oral diseases and diabetes. Br. Dent. J. 2017, 222, 944–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho, A.S.; Amaro, I.F.; Caramelo, F.; Paula, A.; Marto, C.M.; Ferreira, M.M.; Botelho, M.F.; Carrilho, E.V. Dental caries, diabetes mellitus, metabolic control and diabetes duration: A systematic review and meta-analysis. J. Esthet. Restor. Dent. 2020, 32, 291–309. [Google Scholar] [CrossRef]
- Scala, A.; Checchi, L.; Montevecchi, M.; Marini, I.; Giamberardino, M.A. Update on burning mouth syndrome: Overview and patient management. Crit. Rev. Oral Biol. Med. 2003, 14, 275–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, P.A.; Guggenheimer, J.; Orchard, T. Burning mouth syndrome and peripheral neuropathy in patients with type 1 diabetes mellitus. J. Diabetes Complicat. 2007, 21, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Guggenheimer, J.; Moore, P. Xerostomia. J. Am. Dent. Assoc. 2003, 134, 61–69. [Google Scholar] [CrossRef]
- Sreebny, L.M.; Yu, A.; Green, A.; Valdini, A. Xerostomia in diabetes mellitus. Diabetes Care 1992, 15, 900–904. [Google Scholar] [CrossRef] [PubMed]
- Stolbová, K.; Hahn, A.; Benes, B.; Andel, M.; Treslová, L. Gustometry of diabetes mellitus patients and obese patients. Int. Tinnitus J. 1999, 5, 135–140. [Google Scholar]
- Leite, R.S.; Marlow, N.M.; Fernandes, J.K.; Hermayer, K. Oral health and type 2 diabetes. Am. J. Med. Sci. 2013, 345, 271–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, R.; Haque, M. Oral health messiers: Diabetes mellitus relevance. Diabetes Metab. Syndr. Obes. Targets Ther. 2021, 14, 3001–3015. [Google Scholar] [CrossRef]
- Mohanty, S.; Mohanty, N.; Rath, S. Analysis of oral health complications in diabetic patients—A diagnostic perspective. J. Oral Res. 2018, 7, 278–281. [Google Scholar] [CrossRef] [Green Version]
- Jha, R.; Kalyani, P.; Bavishi, R. Oral manifestations of diabetes. J. Res. Med. Dent. Sci. 2014, 2, 6. [Google Scholar] [CrossRef]
- Sasaki, H.; Hirai, K.; M Martins, C.; Furusho, H.; Battaglino, R.; Hashimoto, K. Interrelationship between periapical lesion and systemic metabolic disorders. Curr. Pharm. Des. 2016, 22, 2204–2215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buranasin, P.; Mizutani, K.; Iwasaki, K.; Pawaputanon Na Mahasarakham, C.; Kido, D.; Takeda, K.; Izumi, Y. High glucose-induced oxidative stress impairs proliferation and migration of human gingival fibroblasts. PLoS ONE 2018, 13, e0201855. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Centre for Reviews and Disseminatio. CRD’s Guidance for Undertaking Reviews in Health Care. In Systematic Reviews; York Publishing Services Ltd.: Layerthorpe, UK, 2009. [Google Scholar]
- Lee, E.; Dobbins, M.; Decorby, K.; McRae, L.; Tirilis, D.; Husson, H. An optimal search filter for retrieving systematic reviews and meta-analyses. BMC Med. Res. Methodol. 2012, 12, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papapanou, P.N.; Lindhe, J. Epidemiology of periodontal diseases. In Clinical Periodontology and Implant Dentistry; Lang, N.P., Lindhe, J., Eds.; John Wiley Sons: Chichester, UK, 2015; pp. 125–168. [Google Scholar]
- Gotsman, I.; Lotan, C.; Soskolne, W.A.; Rassovsky, S.; Pugatsch, T.; Lapidus, L.; Novikov, Y.; Masrawa, S.; Stabholz, A. Periodontal destruction is associated with coronary artery disease and periodontal infection with acute coronary syndrome. J. Periodontol. 2007, 78, 849–858. [Google Scholar] [CrossRef] [Green Version]
- Jeffcoat, M.K.; Hauth, J.C.; Geurs, N.C.; Reddy, M.S.; Cliver, S.P.; Hodgkins, P.M.; Goldenberg, R.L. Periodontal disease and preterm birth: Results of a pilot intervention study. J. Periodontol. 2003, 74, 1214–1218. [Google Scholar] [CrossRef]
- Khader, Y.S.; Dauod, A.S.; El-Qaderi, S.S.; Alkafajei, A.; Batayha, W.Q. Periodontal status of diabetics compared with nondiabetics: A meta-analysis. J. Diabetes Complicat. 2006, 20, 59–68. [Google Scholar] [CrossRef]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Prim. 2017, 3, 17038. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, G.G.; Leite, F.R.M.; Vestergaard, P.; Scheutz, F.; López, R. Does diabetes increase the risk of periodontitis? A systematic review and meta-regression analysis of longitudinal prospective studies. Acta Diabetol. 2018, 55, 653–667. [Google Scholar] [CrossRef]
- Shlossman, M.; Knowler, W.C.; Pettitt, D.J.; Genco, R.J. Type 2 diabetes mellitus and periodontal disease. J. Am. Dent. Assoc. 1990, 121, 532–536. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R.G.; Shlossman, M.; Budding, L.M.; Pettitt, D.J.; Saad, M.F.; Genco, R.J.; Knowler, W.C. Periodontal disease and NIDDM in Pima Indians. Diabetes Care 1990, 13, 836–840. [Google Scholar] [CrossRef]
- Zheng, M.; Wang, C.; Ali, A.; Shih, Y.A.; Xie, Q.; Guo, C. Prevalence of periodontitis in people clinically diagnosed with diabetes mellitus: A meta-analysis of epidemiologic studies. Acta Diabetol. 2021, 58, 1307–1327. [Google Scholar] [CrossRef] [PubMed]
- Dicembrini, I.; Serni, L.; Monami, M.; Caliri, M.; Barbato, L.; Cairo, F.; Mannucci, E. Type 1 diabetes and periodontitis: Prevalence and periodontal destruction—A systematic review. Acta Diabetol. 2020, 57, 1405–1412. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Yuan, Y.; Liu, H.; Li, S.; Zhang, B.; Chen, W.; An, Z.; Chen, S.; Wu, Y.; Han, B.; et al. Epidemiologic relationship between periodontitis and type 2 diabetes mellitus. BMC Oral Health 2020, 20, 204. [Google Scholar] [CrossRef] [PubMed]
- Polak, D.; Sanui, T.; Nishimura, F.; Shapira, L. Diabetes as a risk factor for periodontal disease—plausible mechanisms. Periodontology 2000 2020, 83, 46–58. [Google Scholar] [CrossRef] [PubMed]
- Comprehensive medical evaluation and assessment of comorbidities: Standards of medical care in diabetes−2018. Diabetes Care 2018, 44, S28–S37.
- Sanz, M.; Ceriello, A.; Buysschaert, M.; Chapple, I.; Demmer, R.T.; Graziani, F.; Herrera, D.; Jepsen, S.; Lione, L.; Madianos, P.; et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International diabetes Federation and the European Federation of Periodontology. Diabetes Res. Clin. Pract. 2018, 137, 231–241. [Google Scholar] [CrossRef]
- Taylor, J.J.; Preshaw, P.M.; Lalla, E. A review of the evidence for pathogenic mechanisms that may link periodontitis and diabetes. J. Clin. Periodontol. 2013, 40, S113–S134. [Google Scholar] [CrossRef]
- Casarin, R.; Barbagallo, A.; Meulman, T.; Santos, V.; Sallum, E.; Nociti, F.; Duarte, P.; Casati, M.; Goncalves, R. Subgingival biodiversity in subjects with uncontrolled type-2 diabetes and chronic periodontitis. J. Periodontal Res. 2013, 48, 30–36. [Google Scholar] [CrossRef]
- Aemaimanan, P.; Amimanan, P.; Taweechaisupapong, S. Quantification of key periodontal pathogens in insulin-dependent type 2 diabetic and non-diabetic patients with generalized chronic periodontitis. Anaerobe 2013, 22, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Merchant, A.T.; Shrestha, D.; Chaisson, C.; Choi, Y.H.; Hazlett, L.J.; Zhang, J. Association between serum antibodies to oral microorganisms and hyperglycemia in adults. J. Dent. Res. 2014, 93, 752–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demmer, R.T.; Jacobs, D.R., Jr.; Singh, R.; Zuk, A.; Rosenbaum, M.; Papapanou, P.N.; Desvarieux, M. Periodontal bacteria and prediabetes prevalence in ORIGINS: The oral infections, glucose intolerance, and insulin resistance study. J. Dent. Res. 2015, 94, 201s–211s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, V.; Abbas, A.K.; Fausto, N.; Aster, J.C. Cotran Robbins and Cotran Pathologic Basis of Disease; Elsevier: Amsterdam, The Netherlands, 2009; ISBN 1-4377-2015-3. [Google Scholar]
- Monje, A.; Catena, A.; Borgnakke, W.S. Association between diabetes mellitus/hyperglycaemia and peri-implant diseases: Systematic review and meta-analysis. J. Clin. Periodontol. 2017, 44, 636–648. [Google Scholar] [CrossRef]
- Duarte, P.M.; Bezerra, J.P.; Miranda, T.S.; Feres, M.; Chambrone, L.; Shaddox, L.M. Local levels of inflammatory mediators in uncontrolled type 2 diabetic subjects with chronic periodontitis. J. Clin. Periodontol. 2014, 41, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Shikama, Y.; Kudo, Y.; Ishimaru, N.; Funaki, M. Possible involvement of palmitate in pathogenesis of periodontitis. J. Cell. Physiol. 2015, 230, 2981–2989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, S.-L.; Lee, N.-G.; Chang, L.-Y.; Chen, Y.-T.; Lai, Y.-L. Stimulatory effects of glucose and porphyromonas gingivalis lipopolysaccharide on the secretion of inflammatory mediators from human macrophages. J. Periodontol. 2014, 85, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wu, Y.; Wang, B.; Yuan, X.; Fang, B. High levels of glucose induced the Caspase-3/PARP signaling pathway, leading to apoptosis in human periodontal ligament fibroblasts. Cell Biochem. Biophys. 2013, 66, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.C.; Kuo, H.C.; Chang, S.F.; Chen, H.J.; Lee, K.F.; Lin, T.H.; Huang, T.Y.; Choe, C.S.; Lin, L.T.; Chen, C.N. Regulation of ICAM-1 expression in gingival fibroblasts infected with high-glucose-treated P. gingivalis. Cell. Microbiol. 2013, 15, 1722–1734. [Google Scholar] [CrossRef]
- Xu, J.; Xiong, M.; Huang, B.; Chen, H. Advanced glycation end products upregulate the endoplasmic reticulum stress in human periodontal ligament cells. J. Periodontol. 2015, 86, 440–447. [Google Scholar] [CrossRef]
- Catalfamo, D.L.; Calderon, N.L.; Harden, S.W.; Sorenson, H.L.; Neiva, K.G.; Wallet, S.M. Augmented LPS responsiveness in type 1 diabetes-derived osteoclasts. J. Cell. Physiol. 2013, 228, 349–361. [Google Scholar] [CrossRef] [Green Version]
- Chang, P.C.; Chien, L.Y.; Chong, L.Y.; Kuo, Y.P.; Hsiao, J.K. Glycated matrix up-regulates inflammatory signaling similarly to Porphyromonas gingivalis lipopolysaccharide. J. Periodontal Res. 2013, 48, 184–193. [Google Scholar] [CrossRef]
- Kim, J.H.; Lee, D.E.; Choi, S.H.; Cha, J.H.; Bak, E.J.; Yoo, Y.J. Diabetic characteristics and alveolar bone loss in streptozotocin- and streptozotocin-nicotinamide-treated rats with periodontitis. J. Periodontal Res. 2014, 49, 792–800. [Google Scholar] [CrossRef] [PubMed]
- Ozlurk, A.; Bilgici, B.; Odyakmaz, S.; Konas, E. The relationship of periodontal disease severity to serum and GCF substance p levels in diabetics. Quintessence Int. 2012, 43, 587–58796. [Google Scholar]
- Jiang, S.Y.; Wei, C.C.; Shang, T.T.; Lian, Q.; Wu, C.X.; Deng, J.Y. High glucose induces inflammatory cytokine through protein kinase C-induced toll-like receptor 2 pathway in gingival fibroblasts. Biochem. Biophys. Res. Commun. 2012, 427, 666–670. [Google Scholar] [CrossRef] [PubMed]
- Bastos, A.S.; Graves, D.T.; Loureiro, A.P.D.M.; Júnior, C.R.; Abdalla, D.S.P.; Faulin, T.D.E.S.; Câmara, N.O.; Andriankaja, O.M.; Orrico, S.R.P. Lipid peroxidation is associated with the severity of periodontal disease and local inflammatory markers in patients with type 2 diabetes. J. Clin. Endocrinol. Metab. 2012, 97, E1353–E1362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamster, I.B.; Novak, M.J. Host mediators in gingival crevicular fluid: Implications for the pathogenesis of periodontal disease. Crit. Rev. Oral Biol. Med. 1992, 3, 31–60. [Google Scholar] [CrossRef]
- Wu, Y.; Liu, F.; Zhang, X.; Shu, L. Insulin modulates cytokines expression in human periodontal ligament cells. Arch. Oral Biol. 2014, 59, 1301–1306. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.-C.; Tsai, S.-C.; Chong, L.Y.; Kao, M.-J. N-Phenacylthiazolium Bromide Inhibits the Advanced Glycation End Product (AGE)–AGE receptor axis to modulate experimental periodontitis in Rats. J. Periodontol. 2014, 85, e268–e276. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Zhang, J.; Ni, J.; Ouyang, B.; Wang, D.; Luo, S.; Xie, B.; Xuan, D. Toll-Like Receptor 4–Mediated hyper-responsiveness of gingival epithelial cells to lipopolysaccharide in high-glucose environments. J. Periodontol. 2014, 85, 1620–1628. [Google Scholar] [CrossRef]
- Javed, F.; Al-Daghri, N.M.; Wang, H.L.; Wang, C.Y.; Al-Hezaimi, K. Short-term effects of non-surgical periodontal treatment on the gingival crevicular fluid cytokine profiles in sites with induced periodontal defects: A study on dogs with and without streptozotocin-induced diabetes. J. Periodontol. 2014, 85, 1589–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graves, D.T.; Li, J.; Cochran, D.L. Inflammation and uncoupling as mechanisms of periodontal bone loss. J. Dent. Res. 2011, 90, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Albert, D.A.; Ward, A.; Allweiss, P.; Graves, D.T.; Knowler, W.C.; Kunzel, C.; Leibel, R.L.; Novak, K.F.; Oates, T.W.; Papapanou, P.N.; et al. Diabetes and oral disease: Implications for health professionals. Ann. N. Y. Acad. Sci. 2012, 1255, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Bullon, P.; Morillo, J.M.; Ramirez-Tortosa, M.C.; Quiles, J.L.; Newman, H.N.; Battino, M. Metabolic syndrome and periodontitis: Is oxidative stress a common link? J. Dent. Res. 2009, 88, 503–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graves, D.T.; Naguib, G.; Lu, H.; Leone, C.; Hsue, H.; Krall, E. Inflammation is more persistent in type 1 diabetic mice. J. Dent. Res. 2005, 84, 324–328. [Google Scholar] [CrossRef]
- Martinon, F. Signaling by ROS drives inflammasome activation. Eur. J. Immunol. 2010, 40, 616–619. [Google Scholar] [CrossRef] [PubMed]
- Almeida, M.; Han, L.; Ambrogini, E.; Weinstein, R.S.; Manolagas, S.C. Glucocorticoids and tumor necrosis factor α increase oxidative stress and suppress Wnt protein signaling in osteoblasts. J. Biol. Chem. 2011, 286, 44326–44335. [Google Scholar] [CrossRef] [Green Version]
- Galli, C.; Passeri, G.; Macaluso, G.M. FoxOs, Wnts and oxidative stress-induced bone loss: New players in the periodontitis arena? J. Periodontal Res. 2011, 46, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Takeda, M.; Ojima, M.; Yoshioka, H.; Inaba, H.; Kogo, M.; Shizukuishi, S.; Nomura, M.; Amano, A. Relationship of serum advanced glycation end products with deterioration of periodontitis in type 2 diabetes patients. J. Periodontol. 2006, 77, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.M.; Weidman, E.; Lalla, E.; Yan, S.D.; Hori, O.; Cao, R.; Brett, J.G.; Lamster, I.B. Advanced glycation endproducts (AGEs) induce oxidant stress in the gingiva: A potential mechanism underlying accelerated periodontal disease associated with diabetes. J. Periodontal Res. 1996, 31, 508–515. [Google Scholar] [CrossRef]
- Yuan, K.; Chang, C.J.; Hsu, P.C.; Sun, H.S.; Tseng, C.C.; Wang, J.R. Detection of putative periodontal pathogens in non-insulin-dependent diabetes mellitus and non-diabetes mellitus by polymerase chain reaction. J. Periodontal Res. 2001, 36, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Goova, M.T.; Li, J.; Kislinger, T.; Qu, W.; Lu, Y.; Bucciarelli, L.G.; Nowygrod, S.; Wolf, B.M.; Caliste, X.; Yan, S.F.; et al. Blockade of receptor for advanced glycation end-products restores effective wound healing in diabetic mice. Am. J. Pathol. 2001, 159, 513–525. [Google Scholar] [CrossRef] [Green Version]
- Santana, R.B.; Xu, L.; Chase, H.B.; Amar, S.; Graves, D.T.; Trackman, P.C. A role for advanced glycation end products in diminished bone healing in type 1 diabetes. Diabetes 2003, 52, 1502–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rojo-Botello, N.R.; García-Hernández, A.L.; Moreno-Fierros, L. Expression of toll-like receptors 2, 4 and 9 is increased in gingival tissue from patients with type 2 diabetes and chronic periodontitis. J. Periodontal Res. 2012, 47, 62–73. [Google Scholar] [CrossRef]
- Veloso, C.A.; Fernandes, J.S.; Volpe, C.M.O.; Fagundes-Netto, F.S.; Reis, J.S.; Chaves, M.M.; Nogueira-Machado, J.A. TLR4 and RAGE: Similar routes leading to inflammation in type 2 diabetic patients. Diabetes Metab. 2011, 37, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Vieira Ribeiro, F.; de Mendonça, A.C.; Santos, V.R.; Bastos, M.F.; Figueiredo, L.C.; Duarte, P.M. Duarte Cytokines and bone-related factors in systemically healthy patients with chronic periodontitis and patients with type 2 diabetes and chronic periodontitis. J. Periodontol. 2011, 82, 1187–1196. [Google Scholar] [CrossRef] [PubMed]
- Santos, V.R.; Lima, J.A.; Gonçalves, T.E.D.; Bastos, M.F.; Figueiredo, L.C.; Shibli, J.A.; Duarte, P.M. Receptor activator of nuclear factor-kappa B ligand/osteoprotegerin ratio in sites of chronic periodontitis of subjects with poorly and well-controlled type 2 diabetes. J. Periodontol. 2010, 81, 1455–1465. [Google Scholar] [CrossRef] [PubMed]
- Shetty, B.; Divakar, D.D.; Al-Kheraif, A.A.; Alharbi, A.O.; Almutairi, M.S.T.; Alanazi, M.M. Role of PDT as an adjunct to SRP on whole salivary RANKL and OPG ratio in type-2 diabetic and normoglycemic individuals with chronic periodontitis. Photodiagn. Photodyn. Ther. 2021, 34. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.L.; Meng, H.X.; He, L.; Wang, X.E.; Zhang, L. The effects of initial periodontal therapy on the serum receptor activator of nuclear factor-κβ ligand/osteoprotegerin system in patients with type 2 diabetes mellitus and periodontitis. J. Periodontol. 2016, 87, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Mahamed, D.A.; Marleau, A.; Alnaeeli, M.; Singh, B.; Zhang, X.; Penninger, J.M.; Teng, Y.T.A. G(-) anaerobes-reactive CD4+ T-cells trigger RANKL-mediated enhanced alveolar bone loss in diabetic NOD mice. Diabetes 2005, 54, 1477–1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duarte, P.M.; De Oliveira, M.C.G.; Tambeli, C.H.; Parada, C.A.; Casati, M.Z.; Nociti Jr, F.H. Overexpression of interleukin-1beta and interleukin-6 may play an important role in periodontal breakdown in type 2 diabetic patients. J. Periodontal Res. 2007, 42, 377–381. [Google Scholar] [CrossRef]
- Drosatos-Tampakaki, Z.; Drosatos, K.; Siegelin, Y.; Gong, S.; Khan, S.; Van Dyke, T.; Goldberg, I.J.; Schulze, P.C.; Schulze-Späte, U. Palmitic acid and DGAT1 deficiency enhance osteoclastogenesis, while oleic acid-induced triglyceride formation prevents it. J. Bone Miner. Res. 2014, 29, 1183–1195. [Google Scholar] [CrossRef]
- Kayal, R.A.; Tsatsas, D.; Bauer, M.A.; Allen, B.; Al-Sebaei, M.O.; Kakar, S.; Leone, C.W.; Morgan, E.F.; Gerstenfeld, L.C.; Einhorn, T.A.; et al. Diminished bone formation during diabetic fracture healing is related to the premature resorption of cartilage associated with increased osteoclast activity. J. Bone Miner. Res. 2007, 22, 560–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Childs, L.M.; Paschalis, E.P.; Xing, L.; Dougall, W.C.; Anderson, D.; Boskey, A.L.; Puzas, J.E.; Rosier, R.N.; O’Keefe, R.J.; Boyce, B.F.; et al. In vivo RANK signaling blockade using the receptor activator of NF-κB:Fc effectively prevents and ameliorates wear debris-induced osteolysis via osteoclast depletion without inhibiting osteogenesis. J. Bone Miner. Res. 2002, 17, 192–199. [Google Scholar] [CrossRef]
- Cappellen, D.; Luong-Nguyen, N.H.; Bongiovanni, S.; Grenet, O.; Wanke, C.; Mira Šuša, M. Transcriptional program of mouse osteoclast differentiation governed by the macrophage colony-stimulating factor and the ligand for the receptor activator of NFκB. J. Biol. Chem. 2002, 277, 21971–21982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graves, D.T.; Alshabab, A.; Albiero, M.L.; Mattos, M.; Corrêa, J.D.; Chen, S.; Yang, Y. Osteocytes play an important role in experimental periodontitis in healthy and diabetic mice through expression of RANKL. J. Clin. Periodontol. 2018, 45, 285–292. [Google Scholar] [CrossRef]
- Yoshida, T.; Flegler, A.; Kozlov, A.; Stern, P.H. Direct inhibitory and indirect stimulatory effects of RAGE ligand S100 on sRANKL-induced osteoclastogenesis. J. Cell. Biochem. 2009, 107, 917–925. [Google Scholar] [CrossRef]
- Ding, K.H.; Wang, Z.Z.; Hamrick, M.W.; Deng, Z.B.; Zhou, L.; Kang, B.; Yan, S.L.; She, J.X.; Stern, D.M.; Isales, C.M.; et al. Disordered osteoclast formation in RAGE-deficient mouse establishes an essential role for RAGE in diabetes related bone loss. Biochem. Biophys. Res. Commun. 2006, 340, 1091–1097. [Google Scholar] [CrossRef]
- Miyata, T.; Kawai, R.; Taketomi, S.; Sprague, S.M. Possible involvement of advanced glycation end-products in bone resorption. Nephrol. Dial. Transplant. 1996, 11, 54–57. [Google Scholar] [CrossRef] [Green Version]
- Battancs, E.; Gheorghita, D.; Nyiraty, S.; Lengyel, C.; Eördegh, G.; Baráth, Z.; Várkonyi, T.; Antal, M. Periodontal disease in diabetes mellitus: A case–control study in smokers and non-smokers. Diabetes Ther. 2020, 11, 2715–2728. [Google Scholar] [CrossRef] [PubMed]
- Torrungruang, K.; Ongphiphadhanakul, B.; Jitpakdeebordin, S.; Sarujikumjornwatana, S. Mediation analysis of systemic inflammation on the association between periodontitis and glycaemic status. J. Clin. Periodontol. 2018, 45, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Noack, B.; Aslanhan, Z.; Boué, J.; Petig, C.; Teige, M.; Schaper, F.; Hoffmann, T.; Hannig, C. Potential association of paraoxonase-1, type 2 diabetes mellitus, and periodontitis. J. Periodontol. 2013, 84, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Winning, L.; Patterson, C.C.; Neville, C.E.; Kee, F.; Linden, G.J. Periodontitis and incident type 2 diabetes: A prospective cohort study. J. Clin. Periodontol. 2017, 44, 266–274. [Google Scholar] [CrossRef] [Green Version]
- Chokwiriyachit, A.; Dasanayake, A.P.; Suwannarong, W.; Hormdee, D.; Sumanonta, G.; Prasertchareonsuk, W.; Wara-Aswapati, N.; Combellick, J.; Pitiphat, W. Periodontitis and gestational diabetes mellitus in non-smoking females. J. Periodontol. 2013, 84, 857–862. [Google Scholar] [CrossRef]
- Hodge, P.J.; Robertson, D.; Paterson, K.; Smith, G.L.F.; Creanor, S.; Sherriff, A. Periodontitis in non-smoking type 1 diabetic adults: A cross-sectional study. J. Clin. Periodontol. 2012, 39, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Hintao, J.; Teanpaisan, R.; Chongsuvivatwong, V.; Dahlen, G.; Rattarasarn, C. Root surface and coronal caries in adults with type 2 diabetes mellitus. Community Dent. Oral Epidemiol. 2007, 35, 302–309. [Google Scholar] [CrossRef]
- Saremi, A.; Nelson, R.G.; Tulloch-Reid, M.; Hanson, R.L.; Sievers, M.L.; Taylor, G.W.; Knowler, W.C. Periodontal disease and mortality in type 2 diabetes. Diabetes Care 2005, 28, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, P.; Dietrich, T.; Ferro, C.J.; Cockwell, P.; Chapple, I.L.C. Association between periodontitis and mortality in stages 3-5 chronic kidney disease: NHANES III and linked mortality study. J. Clin. Periodontol. 2016, 43, 104–113. [Google Scholar] [CrossRef] [Green Version]
- Thorstensson, H. Medical status and complications in relation to periodontal disease experience in insulin-dependent diabetics. J. Clin. Periodontol. 1996, 23, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Shultis, W.A.; Weil, E.J.; Looker, H.C.; Curtis, J.M.; Shlossman, M.; Genco, R.J.; Knowler, W.C.; Nelson, R.G. Effect of periodontitis on overt nephropathy and end-stage renal disease in type 2 diabetes. Diabetes Care 2007, 30, 306–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demmer, R.T.; Jacobs, D.R.; Desvarieux, M. Periodontal disease and incident type 2 diabetes: Results from the first national health and nutrition examination survey and its epidemiologic follow-up study. Diabetes Care 2008, 31, 1373–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graziani, F.; Gennai, S.; Solini, A.; Petrini, M. A systematic review and meta-analysis of epidemiologic observational evidence on the effect of periodontitis on diabetes An update of the EFP-AAP review. J. Clin. Periodontol. 2018, 45, 167–187. [Google Scholar] [CrossRef]
- Simpson, T.C.; Weldon, J.C.; Worthington, H.V.; Needleman, I.; Wild, S.H.; Moles, D.R.; Stevenson, B.; Furness, S.; Iheozor-Ejiofor, Z. Treatment of periodontal disease for glycaemic control in people with diabetes mellitus. Cochrane Database Syst. Rev. 2015, 1–138. [Google Scholar] [CrossRef] [PubMed]
- Madianos, P.N.; Koromantzos, P.A. An update of the evidence on the potential impact of periodontal therapy on diabetes outcomes. J. Clin. Periodontol. 2018, 45, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.; Nair, M.; Angelov, N.; Lalla, E.; Lee, C. Impact of diabetes on clinical periodontal outcomes following non-surgical periodontal therapy. J. Clin. Periodontol. 2019, 46, 206–217. [Google Scholar] [CrossRef]
- Borgnakke, W.S.; Yelostalo, P.V.; Taylor, G.W.; Genco, R.J. Effect of periodontal disease on diabetes: Systematic review of epidemiologic observational evidence. J. Periodontol. 2013, 84, S135–S152. [Google Scholar] [CrossRef] [Green Version]
- Engebretson, S.; Kocher, T. Evidence that periodontal treatment improves diabetes outcomes: A systematic review and meta-analysis. J. Clin. Periodontol. 2013, 40, S153–S163. [Google Scholar] [CrossRef]
- Li, Q.; Hao, S.; Fang, J.; Xie, J.; Kong, X.H.; Yang, J.X. Effect of non-surgical periodontal treatment on glycemic control of patients with diabetes: A meta-analysis of randomized controlled trials. Trials 2015, 16, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sgolastra, F.; Severino, M.; Pietropaoli, D.; Gatto, R.; Monaco, A. Effectiveness of periodontal treatment to improve metabolic control in patients with chronic periodontitis and type 2 diabetes: A meta-analysis of randomized clinical trials. J. Periodontol. 2013, 84, 958–973. [Google Scholar] [CrossRef]
- Corbella, S.; Francetti, L.; Taschieri, S.; De Siena, F.; Fabbro, M. Del Effect of periodontal treatment on glycemic control of patients with diabetes: A systematic review and meta-analysis. J. Diabetes Investig. 2013, 4, 502–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.F.; Jen, I.A.; Chou, C.; Lei, Y.P. Effects of periodontal therapy on metabolic control in patients with type 2 diabetes mellitus and periodontal disease: A meta-analysis. Medicine 2014, 93, e292. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Feng, M.; Zhang, M.; Zhang, Y.; Cao, M.; Bian, L.; Guan, Q.; Song, K. Effects of periodontal treatment on glycemic control in type 2 diabetic patients: A meta-analysis of randomized controlled trials. Chin. J. Physiol. 2014, 57, 305–314. [Google Scholar] [CrossRef] [Green Version]
- Artese, H.P.C.; Foz, A.M.; Rabelo, M.D.S.; Gomes, G.H.; Orlandi, M.; Suvan, J.; D’Aiuto, F.; Romito, G.A. Periodontal therapy and systemic inflammation in type 2 diabetes mellitus: A meta-analysis. PLoS ONE 2015, 10, e0128344. [Google Scholar] [CrossRef] [Green Version]
- Baeza, M.; Morales, A.; Cisterna, C.; Cavalla, F.; Jara, G.; Isamitt, Y.; Pino, P.; Gamonal, J. Effect of periodontal treatment in patients with periodontitis and diabetes: Systematic review and meta-analysis. J. Appl. Oral Sci. 2020, 28, e20190248. [Google Scholar] [CrossRef]
- McGrath, C.; Bedi, R. Can dentures improve the quality of life of those who have experienced considerable tooth loss? J. Dent. 2001, 29, 243–246. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Diabetes and oral implant failure: A systematic review. J. Dent. Res. 2014, 93, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Javed, F.; Romanos, G.E. Impact of diabetes mellitus and glycemic control on the osseointegration of dental implants: A systematic literature review. J. Periodontol. 2009, 80, 1719–1730. [Google Scholar] [CrossRef] [PubMed]
- Oates, T.W.; Huynh-Ba, G.; Vargas, A.; Alexander, P.; Feine, J. A critical review of diabetes, glycemic control, and dental implant therapy. Clin. Oral Implants Res. 2013, 24, 117–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bornstein, M.M.; Cionca, N.; Mombelli, A. Systemic conditions and treatments as risks for implant therapy. Int. J. Oral Maxillofac. Implant. 2009, 24, 12–27. [Google Scholar]
- Mombelli, A.; Cionca, N. Systemic diseases affecting osseointegration therapy. Clin. Oral Implant. Res. 2006, 17, 97–103. [Google Scholar] [CrossRef]
- Chen, H.; Liu, N.; Xu, X.; Qu, X.; Lu, E. Smoking, radiotherapy, diabetes and osteoporosis as risk factors for dental implant failure: A meta-analysis. PLoS ONE 2013, 8, e71955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graves, D.T.; Ding, Z.; Yang, Y. The impact of diabetes on periodontal diseases. Periodontol. 2000 2020, 82, 214–224. [Google Scholar] [CrossRef]
- Jiang, X.; Zhu, Y.; Liu, Z.; Tian, Z.; Zhu, S. Association between diabetes and dental implant complications: A systematic review and meta-analysis. Acta Odontol. Scand. 2021, 79, 9–18. [Google Scholar] [CrossRef]
- Dowell, S.; Oates, T.W.; Robinson, M. Implant success in people with type 2 diabetes mellitus with varying glycemic control: A pilot study. J. Am. Dent. Assoc. 2007, 138, 355–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tawil, G.; Younan, R.; Azar, P.; Sleilati, G. Conventional and advanced implant treatment in the type II diabetic patient: Surgical protocol and long-term clinical results. Int. J. Oral Maxillofac. Implant. 2008, 23, 744–752. [Google Scholar]
- Oates, T.W.; Dowell, S.; Robinson, M.; McMahan, C.A. Glycemic control and implant stabilization in type 2 diabetes mellitus. J. Dent. Res. 2009, 88, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Turkyilmaz, I. One-year clinical outcome of dental implants placed in patients with type 2 diabetes mellitus: A case series. Implant Dent. 2010, 19, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.-J.; Liu, W.-L.; Lin, H.-L.; Lai, C.-C. Epidemiology and prognostic factors of candidemia in elderly patients. Geriatr. Gerontol. Int. 2015, 15, 688–693. [Google Scholar] [CrossRef]
- Darwazeh, A.M.G.; Lamey, P.-J.; Samaranayake, L.P.; Macfarlane, T.W.; FIisher, B.M.; Macrury, S.M.; Maccuish, A.C. The relationship between colonisation, secretor status and in-vitro adhesion of Candida albicans to buccal epithelial cells from diabetics. J. Med. Microbiol. 1990, 33, 43–49. [Google Scholar] [CrossRef]
- Gonçalves, R.H.P.; Miranda, E.T.; Zaia, J.E.; Giannini, M.J.S.M. Species diversity of yeast in oral colonization of insulin-treated diabetes mellitus patients. Mycopathologia 2006, 162, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Gudlaugsson, O.; Gillespie, S.; Lee, K.; Berg, J.V.; Hu, J.; Messer, S.; Herwaldt, L.; Pfaller, M.; Diekema, D. Attributable Mortality of Nosocomial Candidemia, Revisited. Clin. Infect. Dis. 2003, 37, 1172–1177. [Google Scholar] [CrossRef] [PubMed]
- Kumar, B.V.; Padshetty, N.S.; Bai, K.Y.; Rao, M.S. Prevalence of Candida in the oral cavity of diabetic subjects. J. Assoc. Physicians India 2005, 53, 599–602. [Google Scholar] [PubMed]
- Aitken-Saavedra, J.; Lund, R.G.; González, J.; Huenchunao, R.; Perez-Vallespir, I.; Morales-Bozo, I.; Urzúa, B.; Tarquinio, S.C.; Maturana-Ramírez, A.; Martos, J.; et al. Diversity, frequency and antifungal resistance of Candida species in patients with type 2 diabetes mellitus. Acta Odontol. Scand. 2018, 76, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Javed, F.; Klingspor, L.; Sundin, U.; Altamash, M.; Klinge, B.; Engström, P.-E. Periodontal conditions, oral Candida albicans and salivary proteins in type 2 diabetic subjects with emphasis on gender. BMC Oral Health 2009, 9, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulu, A.; Kassu, A.; Anagaw, B.; Moges, B.; Gelaw, A.; Alemayehu, M.; Belyhun, Y.; Biadglegne, F.; Hurissa, Z.; Moges, F.; et al. Frequent detection of ‘azole’ resistant Candida species among late presenting AIDS patients in northwest Ethiopia. BMC Infect. Dis. 2013, 13, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goregen, M.; Miloglu, O.; Buyukkurt, M.C.; Caglayan, F.; Aktas, A.E. Median rhomboid glossitis: A clinical and microbiological study. Eur. J. Dent. 2011, 5, 367–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arendorf, T.M.; Walker, D.M. Tobacco smoking and denture wearing as local aetiological factors in median rhomboid glossitis. Int. J. Oral Surg. 1984, 13, 411–415. [Google Scholar] [CrossRef]
- Flaitz, C.M.; Nichols, C.M.; Hicks, M.J. An overview of the oral manifestations of AIDS-related Kaposi’s sarcoma. Compend. Contin. Educ. Dent. 1995, 16, 136–138. [Google Scholar] [PubMed]
- Darwazeh, A.M.G.; MacFarlane, T.W.; McCuish, A.; Lamey, P.-J. Mixed salivary glucose levels and candidal carriage in patients with diabetes mellitus. J. Oral Pathol. Med. 1991, 20, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Reinhart, H.; Muller, G.; Sobel, J.D. Specificity and mechanism of in vitro adherence of Candida albicans. Ann. Clin. Lab. Sci. 1985, 15, 406–413. [Google Scholar] [PubMed]
- Naik, R.; Ahmed Mujib, B.R.; Raaju, U.R.; Telagi, N. Assesing oral candidal carriage with mixed salivary glucose levels as non-invasive diagnostic tool in type-2 Diabetics of Davangere, Karnataka, India. J. Clin. Diagn. Res. 2014, 8, ZC69. [Google Scholar] [CrossRef] [PubMed]
- Sashikumar, R.; Kannan, R. Salivary glucose levels and oral candidal carriage in type II diabetics. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodont. 2010, 109, 706–711. [Google Scholar] [CrossRef]
- Geerlings, S.E.; Hoepelman, A.I. Immune dysfunction in patients with diabetes mellitus (DM). FEMS Immunol. Med. Microbiol. 1999, 26, 259–265. [Google Scholar] [CrossRef]
- Ferguson, D. The physiology and biology of saliva. In Color Atlas and Text of Salivary Gland: Disease, Disorders and Surgery; Wolfe Pub Ltd.: London, UK, 1995; pp. 40–48. [Google Scholar]
- Dorocka-Bobkowska, B.; Budtz-Jorgensen, E.; WlSoch, S. Non-insulin-dependent diabetes mellitus as a risk factor for denture stomatitis. J. Oral Pathol. Med. 1996, 25, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Balan, P.; B Gogineni, S.; Kumari N, S.; Shetty, V.; Lakshman Rangare, A.; L Castelino, R.; Areekat K, F. Candida carriage rate and growth characteristics of saliva in diabetes mellitus patients: A case‒control study. J. Dent. Res. Dent. Clin. Dent. Prospects 2015, 9, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Samaranayake, L.P.; Hughes, A.; Weetman, D.A.; MacFarlane, T.W. Growth and acid production of Candida species in human saliva supplemented with glucose. J. Oral Pathol. Med. 1986, 15, 251–254. [Google Scholar] [CrossRef]
- Samaranayake, L.P.; MacFarlane, T.W. Factors affecting the in-vitro adherence of the fungal oral pathogen Candida albicans to epithelial cells of human origin. Arch. Oral Biol. 1982, 27, 869–873. [Google Scholar] [CrossRef]
- Pallavan, B.; Ramesh, V.; Dhanasekaran, B.P.; Oza, N.; Indu, S.; Govindarajan, V. Comparison and correlation of candidal colonization in diabetic patients and normal individuals. J. Diabetes Metab. Disord. 2014, 13, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantri, S.S.; Parkhedkar, R.D.; Mantri, S.P. Candida colonisation and the efficacy of chlorhexidine gluconate on soft silicone-lined dentures of diabetic and non-diabetic patients. Gerodontology 2013, 30, 288–295. [Google Scholar] [CrossRef]
- Malic, S.; Hill, K.E.; Ralphs, J.R.; Hayes, A.; Thomas, D.W.; Potts, A.J.; Williams, D.W. Characterization of Candida albicans infection of an in vitro oral epithelial model using confocal laser scanning microscopy. Oral Microbiol. Immunol. 2007, 22, 188–194. [Google Scholar] [CrossRef]
- Wang, J.; Ohshima, T.; Yasunari, U.; Namikoshi, S.; Yoshihara, A.; Miyazaki, H.; Maeda, N. The carriage of Candida species on the dorsal surface of the tongue: The correlation with the dental, periodontal and prosthetic status in elderly subjects. Gerodontology 2006, 23, 157–163. [Google Scholar] [CrossRef] [PubMed]
- de Carvalho Bianchi, C.M.P.; Bianchi, H.A.; Tadano, T.; de Paula, C.R.; Hoffmann-Santos, H.D.; Leite, D.P., Jr.; Hahn, R.C. Factors related to oral candidiasis in elderly users and non-users of removable dental prostheses. Rev. Inst. Med. Trop. Sao Paulo 2016, 58, 17. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, M.B.R.; Lago, E.C. Oral changes in elderly from an association center. Rev. Para. Med. V 2010, 24, 35–41. [Google Scholar]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Giovannucci, E.; Harlan, D.M.; Archer, M.C.; Bergenstal, R.M.; Gapstur, S.M.; Habel, L.A.; Pollak, M.; Regensteiner, J.G.; Yee, D. Diabetes and cancer: A consensus report. CA. Cancer J. Clin. 2010, 60, 207–221. [Google Scholar] [CrossRef] [Green Version]
- Pollak, M.N. Insulin-like growth factors and neoplasia. Biol. IGF-1 Its Interact. Insul. Health Malig. States 2008, 262, 84–98. [Google Scholar] [CrossRef]
- Ramos-García, P.; Gil-Montoya, J.A.; Scully, C.; Ayén, A.; González-Ruiz, L.; Navarro-Triviño, F.J.; González-Moles, M.A. An update on the implications of cyclin D1 in oral carcinogenesis. Oral Dis. 2017, 23, 897–912. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Dominy, J.E.; Choi, Y.J.; Jurczak, M.; Tolliday, N.; Camporez, J.P.; Chim, H.; Lim, J.-H.; Ruan, H.-B.; Yang, X.; et al. Cyclin D1–Cdk4 controls glucose metabolism independently of cell cycle progression. Nature 2014, 510, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Ramos-García, P.; González-Moles, M.Á.; Ayén, Á.; González-Ruiz, L.; Ruiz-Ávila, I.; Lenouvel, D.; Gil-Montoya, J.A.; Bravo, M. Asymmetrical proliferative pattern loss linked to cyclin D1 overexpression in adjacent non-tumour epithelium in oral squamous cell carcinoma. Arch. Oral Biol. 2019, 97, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Ramos-García, P.; González-Moles, M.Á.; González-Ruiz, L.; Ayén, Á.; Ruiz-Ávila, I.; Bravo, M.; Gil-Montoya, J.A. Clinicopathological significance of tumor cyclin D1 expression in oral cancer. Arch. Oral Biol. 2019, 99, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Asmat, U.; Abad, K.; Ismail, K. Diabetes mellitus and oxidative stress—A concise review. Saudi Pharm. J. 2016, 24, 547–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [Green Version]
- Hahn, T.; Barth, S.; Hofmann, W.; Reich, O.; Lang, I.; Desoye, G. Hyperglycemia regulates the glucose-transport system of clonal choriocarcinoma cells in vitro. A potential molecular mechanism contributing to the adjunct effect of glucose in tumor therapy. Int. J. Cancer 1998, 78, 353–360. [Google Scholar] [CrossRef]
- Han, L.; Ma, Q.; Li, J.; Liu, H.; Li, W.; Ma, G.; Xu, Q.; Zhou, S.; Wu, E. High glucose promotes pancreatic cancer cell proliferation via the induction of EGF expression and transactivation of EGFR. PLoS ONE 2011, 6, e27074. [Google Scholar] [CrossRef]
- Okumura, M.; Yamamoto, M.; Sakuma, H.; Kojima, T.; Maruyama, T.; Jamali, M.; Cooper, D.R.; Yasuda, K. Leptin and high glucose stimulate cell proliferation in MCF-7 human breast cancer cells: Reciprocal involvement of PKC-α and PPAR expression. Biochim. Biophys. Acta-Mol. Cell Res. 2002, 1592, 107–116. [Google Scholar] [CrossRef] [Green Version]
- Barone, B.B.; Yeh, H.C.; Snyder, C.F.; Peairs, K.S.; Stein, K.B.; Derr, R.L.; Wolff, A.C.; Brancati, F.L. Long-term all-cause mortality in cancer patients with preexisting diabetes mellitus: A systematic review and meta-analysis. JAMA 2008, 300, 2754–2764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seshasai, S.R.K.; Kaptoge, S.; Thompson, A.; Di Angelantonio, E.; Gao, P.; Sarwar, N.; Whincup, P.H.; Mukamal, K.J.; Gillum, R.F.; Holme, I.; et al. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N. Engl. J. Med. 2011, 364, 829–841. [Google Scholar] [CrossRef] [Green Version]
- Van De Poll-Franse, L.V.; Houterman, S.; Janssen-Heijnen, M.L.G.; Dercksen, M.W.; Coebergh, J.W.W.; Haak, H.R. Less aggressive treatment and worse overall survival in cancer patients with diabetes: A large population based analysis. Int. J. Cancer 2007, 120, 1986–1992. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Kim, S.Y.; Nam, S.Y.; Choi, S.-H.; Choi, J.W.; Roh, J.-L. Risk factors of surgical site infection in patients undergoing major oncological surgery for head and neck cancer. Oral Oncol. 2011, 47, 528–531. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S.; Johnson, N.W.; van der Waal, I. Nomenclature and classification of potentially malignant disorders of the oral mucosa. J. Oral Pathol. Med. 2007, 36, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Aguirre-Urizar, J.M.; Lafuente-Ibáñez de Mendoza, I.; Warnakulasuriya, S. Malignant transformation of oral leukoplakia: Systematic review and meta-analysis of the last 5 years. Oral Dis. 2021, 27, 1881–1895. [Google Scholar] [CrossRef]
- Warnakulasuriya, S.; Ariyawardana, A. Malignant transformation of oral leukoplakia: A systematic review of observational studies. J. Oral Pathol. Med. 2016, 45, 155–166. [Google Scholar] [CrossRef] [PubMed]
- González-Moles, M.Á.; Ruiz-Ávila, I.; González-Ruiz, L.; Ayén, Á.; Gil-Montoya, J.A.; Ramos-García, P. Malignant transformation risk of oral lichen planus: A systematic review and comprehensive meta-analysis. Oral Oncol. 2019, 96, 121–130. [Google Scholar] [CrossRef] [PubMed]
- González-Moles, M.Á.; Ramos-García, P.; Warnakulasuriya, S. An appraisal of highest quality studies reporting malignant transformation of oral lichen planus based on a systematic review. Oral Dis. 2020. [Google Scholar] [CrossRef]
- Ramos-García, P.; Gonzalez-Moles, M.A.; Warnakulasuriya, S. Oral cancer development in lichen planus and related conditions-3.0 evidence level-: A systematic review of systematic reviews. Oral Dis. 2021, 27, 1908–1918. [Google Scholar] [CrossRef] [PubMed]
- Ramos-García, P.; González-Moles, M.Á.; Mello, F.W.; Bagan, J.V.; Warnakulasuriya, S. Malignant transformation of oral proliferative verrucous leukoplakia: A systematic review and meta-analysis. Oral Dis. 2021, 27, 1896–1907. [Google Scholar] [CrossRef] [PubMed]
- González-Moles, M.Á.; Ramos-García, P.; Warnakulasuriya, S. A scoping review on gaps in the diagnostic criteria for proliferative verrucous leukoplakia: A conceptual proposal and diagnostic evidence-based criteria. Cancers 2021, 13, 3669. [Google Scholar] [CrossRef]
- González-Moles, M.Á.; Warnakulasuriya, S.; Ramos-García, P. Prognosis parameters of oral carcinomas developed in proliferative verrucous leukoplakia: A systematic review and meta-analysis. Cancers 2021, 13, 4843. [Google Scholar] [CrossRef]
- Iocca, O.; Sollecito, T.P.; Alawi, F.; Weinstein, G.S.; Newman, J.G.; De Virgilio, A.; Di Maio, P.; Spriano, G.; Pardiñas López, S.; Shanti, R.M. Potentially malignant disorders of the oral cavity and oral dysplasia: A systematic review and meta-analysis of malignant transformation rate by subtype. Head Neck 2019, 42, 539–555. [Google Scholar] [CrossRef]
- Dancyger, A.; Heard, V.; Huang, B.; Suley, C.; Tang, D.; Ariyawardana, A. Malignant transformation of actinic cheilitis: A systematic review of observational studies. J. Investig. Clin. Dent. 2018, 9, e12343. [Google Scholar] [CrossRef] [PubMed]
- González-Moles, M.Á.; Warnakulasuriya, S.; González-Ruiz, I.; González-Ruiz, L.; Ayén, Á.; Lenouvel, D.; Ruiz-Ávila, I.; Ramos-García, P. Worldwide prevalence of oral lichen planus: A systematic review and meta-analysis. Oral Dis. 2020, 27, 813–828. [Google Scholar] [CrossRef] [PubMed]
- Otero Rey, E.M.; Yáñez-Busto, A.; Rosa Henriques, I.F.; López-López, J.; Blanco-Carrión, A. Lichen planus and diabetes mellitus: Systematic review and meta-analysis. Oral Dis. 2019, 25, 1253–1264. [Google Scholar] [CrossRef]
- Ismail, A.F.; McGrath, C.P.; Yiu, C.K.Y. Oral health of children with type 1 diabetes mellitus: A systematic review. Diabetes Res. Clin. Pract. 2015, 108, 369–381. [Google Scholar] [CrossRef]
- Mauri-Obradors, E.; Estrugo-Devesa, A.; Jane-Salas, E.; Vinas, M.; Lopez-Lopez, J. Oral manifestations of diabetes mellitus. A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2017, 22, e586. [Google Scholar] [CrossRef]
- Bharateesh, J.V.; Ahmed, M.; Kokila, G. Diabetes and oral health: A case-control study. Int. J. Prev. Med. 2012, 3, 806–809. [Google Scholar] [PubMed]
- Meurman, J.H.; Collin, H.L.; Niskanen, L.; Töyry, J.; Alakuijala, P.; Keinänen, S.; Uusitupa, M. Saliva in non-insulin-dependent diabetic patients and control subjects: The role of the autonomic nervous system. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1998, 86, 69–76. [Google Scholar] [CrossRef]
- Bookout, G.P.; Ladd, M.; Short, R.E. Burning Mouth Syndrome.; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Verhulst, M.J.L.; Loos, B.G.; Gerdes, V.E.A.; Teeuw, W.J. Evaluating all potential oral complications of diabetes mellitus. Front. Endocrinol. (Lausanne) 2019, 10, 56. [Google Scholar] [CrossRef] [PubMed]
- Collin, H.-L.; Niskanen, L.; Uusitupa, M.; Töyry, J.; Collin, P.; Koivisto, A.-M.; Viinamäki, H.; Meurman, J.H. Oral symptoms and signs in elderly patients with type 2 diabetes mellitus. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2000, 90, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Eltas, A.; Tozoğlu, Ü.; Keleş, M.; Canakci, V. Assessment of oral health in peritoneal dialysis patients with and without diabetes mellitus. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2012, 32, 81–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vesterinen, M.; Ruokonen, H.; Furuholm, J.; Honkanen, E.; Meurman, J.H. Clinical questionnaire study of oral health care and symptoms in diabetic vs. non-diabetic predialysis chronic kidney disease patients. Clin. Oral Investig. 2012, 16, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Bültzingslöwen, V.I.; Sollecito, T.P.; Fox, P.C.; Daniels, T.; Jonsson, R.; Lockhart, P.B.; Wray, D.; Brennan, M.T.; Carrozzo, M.; Gandera, B.; et al. Salivary dysfunction associated with systemic diseases: Systematic review and clinical management recommendations. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 103, S57.e1–S57.e15. [Google Scholar] [CrossRef]
- Orellana, M.F.; Lagravère, M.O.; Boychuk, D.G.; Major, P.W.; Flores-Mir, C.; Ortho, C. Prevalence of xerostomia in population-based samples: A systematic review. J. Public Health Dent. 2006, 66, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Moore, P.A.; Guggenheimer, J.; Etzel, K.R.; Weyant, R.J.; Orchard, T. Type 1 diabetes mellitus, xerostomia, and salivary flow rates. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2001, 92, 281–291. [Google Scholar] [CrossRef]
- Ben-Aryeh, H.; Cohen, M.; Kanter, Y.; Szargel, R.; Laufer, D. Salivary composition in diabetic patients. J. Diabet. Complicat. 1988, 2, 96–99. [Google Scholar] [CrossRef]
- López, M.E.; Colloca, M.E.; Páez, R.G.; Schallmach, J.N.; Koss, M.A.; Chervonagura, A. Salivary characteristics of diabetic children. Braz. Dent. J. 2003, 14, 26–31. [Google Scholar] [CrossRef] [Green Version]
- Mata, A.D.; Marques, D.; Rocha, S.; Francisco, H.; Santos, C.; Mesquita, M.F.; Singh, J. Effects of diabetes mellitus on salivary secretion and its composition in the human. Mol. Cell. Biochem. 2004, 261, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Karjalainen, K.M. Salivary factors in children and adolescents with insulin-dependent diabetes mellitus. Pediatr. Dent. 1996, 18, 306–307. [Google Scholar]
- Malicka, B.; Kaczmarek, U.; Skośkiewicz-Malinowska, K. Prevalence of xerostomia and the salivary flow rate in diabetic patients. Adv. Clin. Exp. Med. 2014, 23, 225–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasconcelos, A.C.U.; Soares, M.S.M.; Almeida, P.C.; Soares, T.C. Comparative study of the concentration of salivary and blood glucose in type 2 diabetic patients. J. Oral Sci. 2010, 52, 293–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montaldo, L.; Montaldo, P.; Papa, A.; Caramico, N.; Toro, G. Effects of saliva substitutes on oral status in patients with Type 2 diabetes. Diabet. Med. 2010, 27, 1280–1283. [Google Scholar] [CrossRef] [PubMed]
- Lasisi, T.J.; Fasanmade, A.A. Salivary flow and composition in diabetic and non-diabetic subjects. Niger. J. Physiol. Sci. 2012, 27, 79–82. [Google Scholar] [PubMed]
- Chávez, E.M.; Borrell, L.N.; Taylor, G.W.; Ship, J.A. A longitudinal analysis of salivary flow in control subjects and older adults with type 2 diabetes. Oral Surgery Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2001, 91, 166–173. [Google Scholar] [CrossRef]
- Chavez, E.M.; Taylor, G.W.; Borrell, L.N.; Ship, J.A. Salivary function and glycemic control in older persons with diabetes. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2000, 89, 305–311. [Google Scholar] [CrossRef]
- Jawed, M.; Khan, R.N.; Shahid, S.M.; Azhar, A. protective effects of salivary factors in dental caries in diabetic patients of Pakistan. Exp. Diabetes Res. 2012, 2012, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, G.E.; Sundberg, H.E.; Fjellstrom, C.A.; Wikblad, K.F. Type 2 diabetes and oral health. Diabetes Res. Clin. Pract. 2000, 50, 27–34. [Google Scholar] [CrossRef]
- Kao, C.-H.; Tsai, S.-C.; Sun, S.-S. Scintigraphic evidence of poor salivary function in type 2 diabetes. Diabetes Care 2001, 24, 952–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khovidhunkit, S.O.P.; Suwantuntula, T.; Thaweboon, S.; Mitrirattanakul, S.; Chomkhakhai, U.; Khovidhunkit, W. Xerostomia, hyposalivation, and oral microbiota in type 2 diabetic patients: A preliminary study. J. Med. Assoc. Thail. 2009, 92, 1220–1228. [Google Scholar]
- Lin, C.-C.; Sun, S.-S.; Kao, A.; Lee, C.-C. Impaired salivary function in patients with noninsulin-dependent diabetes mellitus with xerostomia. J. Diabetes Complicat. 2002, 16, 176–179. [Google Scholar] [CrossRef]
- Quirino, M.R.; Birman, E.G.; Paula, C.R. Oral manifestations of diabetes mellitus in controlled and uncontrolled patients. Braz. Dent. J. 1995, 6, 131–136. [Google Scholar] [PubMed]
- Newrick, P.G.; Bowman, C.; Green, D.; O’Brien, I.A.D.; Porter, S.R.; Scully, C.; Corrall, R.J.M. Parotid salivary secretion in diabetic autonomic neuropathy. J. Diabet. Complicat. 1991, 5, 35–37. [Google Scholar] [CrossRef]
- Sandberg, G.E.; Wikblad, K.F. Oral dryness and peripheral neuropathy in subjects with type 2 diabetes. J. Diabetes Complicat. 2003, 17, 192–198. [Google Scholar] [CrossRef]
- Lamey, P. -J.; Fisher, B.M.; Frier, B.M. The effects of diabetes and autonomic neuropathy on parotid salivary flow in man. Diabet. Med. 1986, 3, 537–540. [Google Scholar] [CrossRef]
- Scully Cbe, C. Drug effects on salivary glands: Dry mouth. Oral Dis. 2003, 9, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, M.M.; D’Epiro, T.T.S.; Bernardi, L.; Fossati, A.C.M.; dos Santos, M.F.; Lamers, M.L. Long-and short-term diabetes mellitus type 1 modify young and elder rat salivary glands morphology. Arch. Oral Biol. 2017, 73, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Carda, C.; Carranza, M.; Arriaga, A.; Díaz, A.; Peydró, A.; Gomez De Ferraris, M.E. Structural differences between alcoholic and diabetic parotid sialosis. Med. Oral Patol. Oral Cir. Bucal 2005, 10, 309–314. [Google Scholar]
- Russotto, S.B. Asymptomatic parotid gland enlargement in diabetes mellitus. Oral Surg. Oral Med. Oral Pathol. 1981, 52, 594–598. [Google Scholar] [CrossRef]
- Alves, M.; Calegari, V.C.; Cunha, D.A.; Saad, M.J.A.; Velloso, L.A.; Rocha, E.M. Increased expression of advanced glycation end-products and their receptor, and activation of nuclear factor kappa-B in lacrimal glands of diabetic rats. Diabetologia 2005, 48, 2675–2681. [Google Scholar] [CrossRef] [Green Version]
- Fukuoka, C.Y.; Simões, A.; Uchiyama, T.; Arana-Chavez, V.E.; Abiko, Y.; Kuboyama, N.; Bhawal, U.K. The effects of low-power laser irradiation on inflammation and apoptosis in submandibular glands of diabetes-induced rats. PLoS ONE 2017, 12, e0169443. [Google Scholar] [CrossRef] [PubMed]
- Ship, J.A.; Fischer, D.J. The relationship between dehydration and parotid salivary gland function in young and older healthy adults. J. Gerontol. Ser. A: Biol. Sci. Med. Sci. 1997, 52, M310–M319. [Google Scholar] [CrossRef] [Green Version]
- Sreebny, L.M.; Schwartz, S.S. A reference guide to drugs and dry mouth. Gerodontology 1986, 5, 75–99. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, R.; Deepa, M.G.; Sruthi, A.K.; Kuruvila, C.; Priya, S.; Sunil, S.; Roopesh, G. Roopesh evaluation of oral health in type II diabetes mellitus patients. Oral Maxillofac. Pathol. J. 2015, 6, 525–531. [Google Scholar]
- Kamaraj, D.R.; Bhushan, K.S.; Laxman, V.K.; Mathew, J. Detection of odoriferous subgingival and tongue microbiota in diabetic and nondiabetic patients with oral malodor using polymerase chain reaction. Indian J. Dent. Res. 2011, 22, 260–265. [Google Scholar] [CrossRef]
- Koshimune, S.; Awano, S.; Gohara, K.; Kurihara, E.; Ansai, T.; Takehara, T. Low salivary flow and volatile sulfur compounds in mouth air. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 96, 38–41. [Google Scholar] [CrossRef]
- Al-Zahrani, M.S.; Zawawi, K.H.; Austah, O.N.; Al-Ghamdi, H.S. Self reported halitosis in relation to glycated hemoglobin level in diabetic patients. Open Dent. J. 2011, 5, 154–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wray, L. The diabetic patient and dental treatment: An update. Br. Dent. J. 2011, 211, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Ship, J. Diabetes and oral health. J. Am. Dent. Assoc. 2003, 134, 4S–10S. [Google Scholar] [CrossRef]
- Siddiqi, A.; Zafar, S.; Sharma, A.; Quaranta, A. Diabetes mellitus and periodontal disease: The call for interprofessional education and interprofessional collaborative care—A systematic review of the literature. J. Interprof. Care 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, A.; Zafar, S.; Sharma, A.; Quaranta, A. Diabetic patients’ knowledge of the bidirectional link: Are dental health care professionals effectively conveying the message? Aust. Dent. J. 2019, 64, 312–326. [Google Scholar] [CrossRef] [PubMed]
- Allen, E.M.; Ziada, H.M.; O’Halloran, D.; Clerehugh, V.; Allen, P.F. Attitudes, awareness and oral health-related quality of life in patients with diabetes. J. Oral Rehabil. 2008, 35, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Tomar, S.L.; Lester, A. Dental and other health care visits among U.S. adults with diabetes. Diabetes Care 2000, 23, 1505–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandberg, G.E.; Sundberg, H.E.; Wikblad, K.F. A controlled study of oral self-care and self-perceived oral health in type 2 diabetic patients. Acta Odontol. Scand. 2001, 59, 28–33. [Google Scholar] [CrossRef]
- Moore, P.A.; Orchard, T.; Guggenheimer, J.; Weyant, R.J. Diabetes and oral health promotion: A survey of disease prevention behaviors. J. Am. Dent. Assoc. 2000, 131, 1333–1341. [Google Scholar] [CrossRef] [PubMed]
- Jansson, H.; Lindholm, E.; Lindh, C.; Groop, L.; Bratthall, G. Type 2 diabetes and risk for periodontal disease: A role for dental health awareness. J. Clin. Periodontol. 2006, 33, 408–414. [Google Scholar] [PubMed]
- Al Habashneh, R.; Khader, Y.; Hammad, M.M.; Almuradi, M. Knowledge and awareness about diabetes and periodontal health among Jordanians. J. Diabetes Complicat. 2010, 24, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.C.; Genco, R. Diabetes and periodontal diseases: Consensus report of the Joint EFP/AAP workshop on periodontitis and systemic diseases. J. Periodontol. 2013, 84, S106–S112. [Google Scholar] [CrossRef]
- Ogurtsova, K.; da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Estrich, C.G.; Araujo, M.W.B.; Lipman, R.D. Prediabetes and diabetes screening in dental care settings: NHANES 2013 to 2016. JDR Clin. Transl. Res. 2019, 4, 76–85. [Google Scholar] [CrossRef]
- Beagley, J.; Guariguata, L.; Weil, C.; Motala, A.A. Global estimates of undiagnosed diabetes in adults. Diabetes Res. Clin. Pract. 2014, 103, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.; Ouanounou, A. Diagnosis, management, and dental considerations for the diabetic patient. J. Can. Dent. Assoc. 2020, 86, k8. [Google Scholar] [PubMed]
- Marti Alamo, S.; Jimenez Soriano, Y.; Sarrion Perez, M. Dental considerations for the patient with diabetes. J. Clin. Exp. Dent. 2011, 3, e25–e30. [Google Scholar] [CrossRef]
- Nathan, D.M.; Buse, J.B.; Davidson, M.B.; Ferrannini, E.; Holman, R.R.; Sherwin, R.; Zinman, B.; American Diabetes Association. European association for study of diabetes medical management of hyperglycemia in type 2 diabetes: A consensus algorithm for the initiation and adjustment of therapy: A consensus statement of the American diabetes association and the European association for the study of diabetes. Diabetes Care 2009, 32, 193–203. [Google Scholar] [CrossRef] [Green Version]
- Bergman, S.A. Perioperative management of the diabetic patient. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 103, 731–737. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Oral Manifestations | Description | References |
|---|---|---|
| Periodontitis | The concept of periodontitis refers to a chronic inflammatory process characterized by microbially-associated, host-mediated inflammation that results in loss of periodontal attachment (i.e., by loss of marginal periodontal ligament fibers, apical migration of the junctional epithelium, and apical spread of the bacterial biofilm along the root surface of teeth). Initially, bacterial biofilm formation begins gingival inflammation (i.e., dental-biofilm induced gingivitis) with periodontitis initiation and progression. Furthermore, a multifactorial origin influenced by additional risk factors, such as smoking, is now supported on the immunoinflammatory bases of periodontitis. The relationship between periodontitis and DM (i.e., high prevalence and magnitude of association) is based on a solid evidence level. | [7,8] |
| Oral candidiasis | Fungal infections, particularly by species of the genus Candida sp. Common clinical manifestations are the presence of extensive reddened areas (erythematous candidiasis) along the oral mucosa, generally associated with patchy lingual depapillation and commissural cheilitis. DM patients may present whitish lumps, similar to milk or yogurt clots (speudomembranous candidiasis). Oral candidiasis is usually symptomatic, causing discomfort, burning, or frank pain. | [9,10] |
| Oral cancer | Oral cancer is the malignant neoplasm affecting lips, oral cavity, or oropharynx. Oral squamous cell carcinoma represents around 90% cases and has a 5-year mortality rate of 50%. The reasons for the increased development of oral cancer in diabetics are not well known, although clinical, biochemical, and molecular reasons have been proposed. | [11,12] |
| Oral potentially malignant disorders (OPMD) | OPMDs are a significant group of mucosal disorders that may have an increased susceptibility to develop oral cancer, which are essentially oral leukoplakia, oral lichen planus (OLP), proliferative verrucous leukoplakia, erythroplakia and actinic cheilitis. Leukoplakia and OLP—both prevalent OPMDs, associated with considerable malignant transformation rates—have a higher prevalence in subjects with DM than in general population. | [12,13] |
| Dental caries | Dental caries also known as tooth decays are caused by a breakdown of the tooth tissues. This breakdown is the result of dental plaque’s bacterias on teeth that produce acid destroying tooth tissues (e.g., enamel) and results in tooth decay. Diabetic patients, as a consequence of a series of associated oral conditions—xerostomia, high levels of dental plaque, etc.—would be more predisposed to the development of dental caries. | [14,15] |
| Burning mouth syndrome (BMS) | BMS is an atypical chronic pain essentially characterized by the presence of a burning sensation, stinging, or frank pain that is located mainly on the tongue, lips, and palate, although it can spread to any other location, without that there are recognizable mucosal lesions that may justify this condition. BMS seems to present an increased prevalence in patients with DM compared to healthy subjects. It could be associated with the peripheral neuropathy frequently reported in diabetic patients. | [16,17] |
| Salivary secretion alterations | Alterations in salivary secretion are generically known by the term “dry mouth”, which however refers to two different processes, the first related to an objective reduction of salivary flow due to salivary hypofunction (i.e., unstimulated whole saliva flow rate of <0.1 mL/min); and the second, the subjective sensation of lack of saliva in the absence of flow disorders. Dry mouth is one of the most common complaints in diabetic patients, with a partially unknown pathophysiology, which could be related to diabetic neuropathy of parotid gland, pathologic alterations in the salivary glands structure (e.g., vacuolization or acinar atrophy), or hyperglycemia and poorly controlled DM. | [18,19] |
| Taste perception alterations | Taste perception alterations, mainly hypogeusia (i.e., a partial loss of taste) have been reported in patients with DM. The reasons for the increased development of taste perception alterations in diabetics are not well known, although it has been proposed that it could be associated with the peripheral neuropathy frequently reported in diabetic patients. | [20,21] |
| Halitosis | Halitosis is a symptom where a person has bad breath. It can be caused by bad oral health, singularly dental care, caries, or periodontitis. Patients with DM are predisposed to halitosis, probably related to the frequent prevalence of these diseases in diabetic patients. | [22,23] |
| Delayed wound healing | Delayed wound healing is a complication in diabetics after oral surgery, especially in patients with poorly controlled DM. The probable cause of delayed wound healing is damaged small terminal vessels, responsible of reduced blood flow, with an insufficient supply of cellular nutrients through the blood circulation, decreased inflammatory and immune response. | [24,25,26] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Moles, M.Á.; Ramos-García, P. State of Evidence on Oral Health Problems in Diabetic Patients: A Critical Review of the Literature. J. Clin. Med. 2021, 10, 5383. https://doi.org/10.3390/jcm10225383
González-Moles MÁ, Ramos-García P. State of Evidence on Oral Health Problems in Diabetic Patients: A Critical Review of the Literature. Journal of Clinical Medicine. 2021; 10(22):5383. https://doi.org/10.3390/jcm10225383
Chicago/Turabian StyleGonzález-Moles, Miguel Ángel, and Pablo Ramos-García. 2021. "State of Evidence on Oral Health Problems in Diabetic Patients: A Critical Review of the Literature" Journal of Clinical Medicine 10, no. 22: 5383. https://doi.org/10.3390/jcm10225383
APA StyleGonzález-Moles, M. Á., & Ramos-García, P. (2021). State of Evidence on Oral Health Problems in Diabetic Patients: A Critical Review of the Literature. Journal of Clinical Medicine, 10(22), 5383. https://doi.org/10.3390/jcm10225383