
Chronotropic Incompetence in Non-Hospitalized Patients with Post-COVID-19 Syndrome


 , ,
, , 
Abstract
:1. Introduction
2. Material and Methods
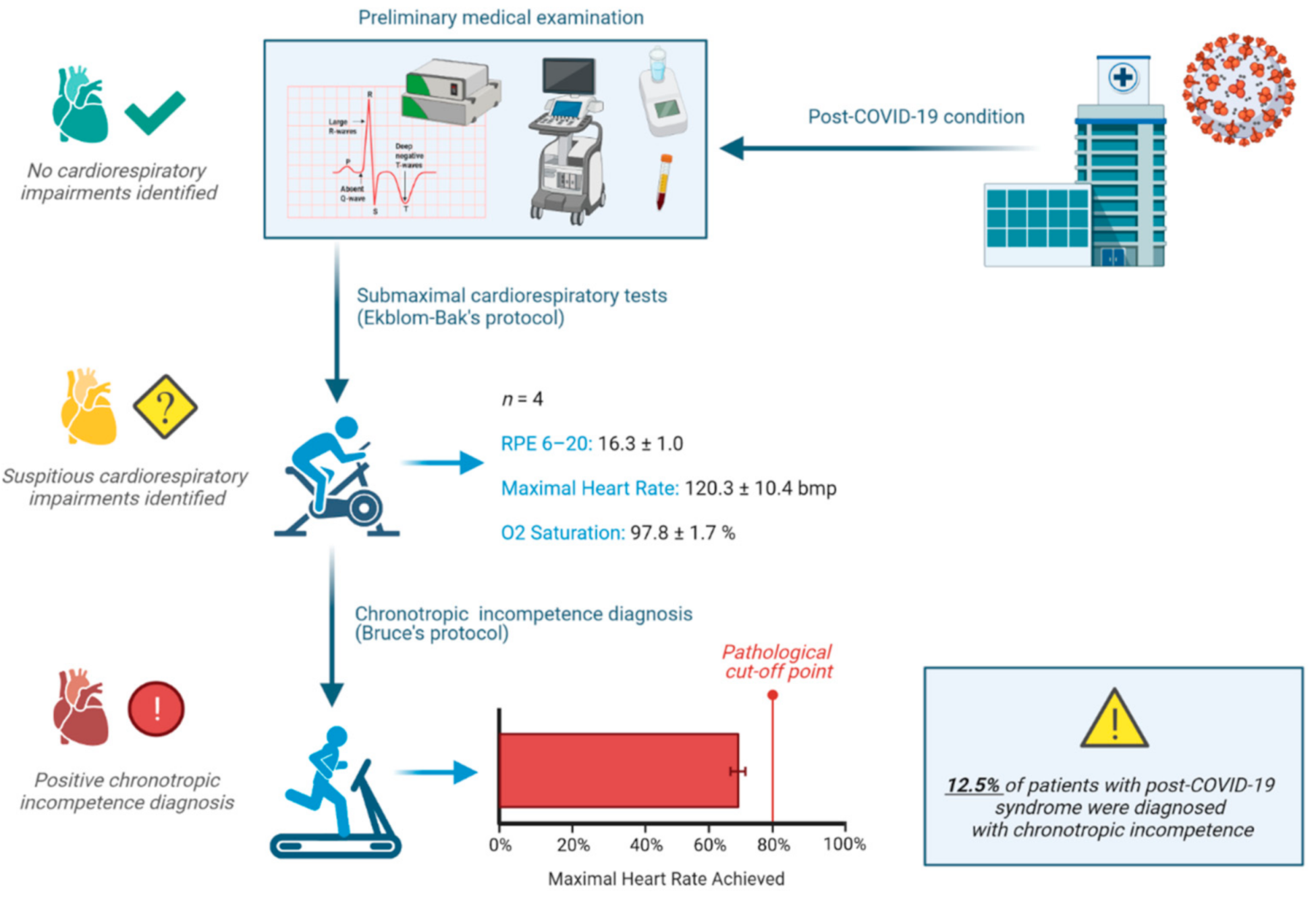
2.1. Experimental Design
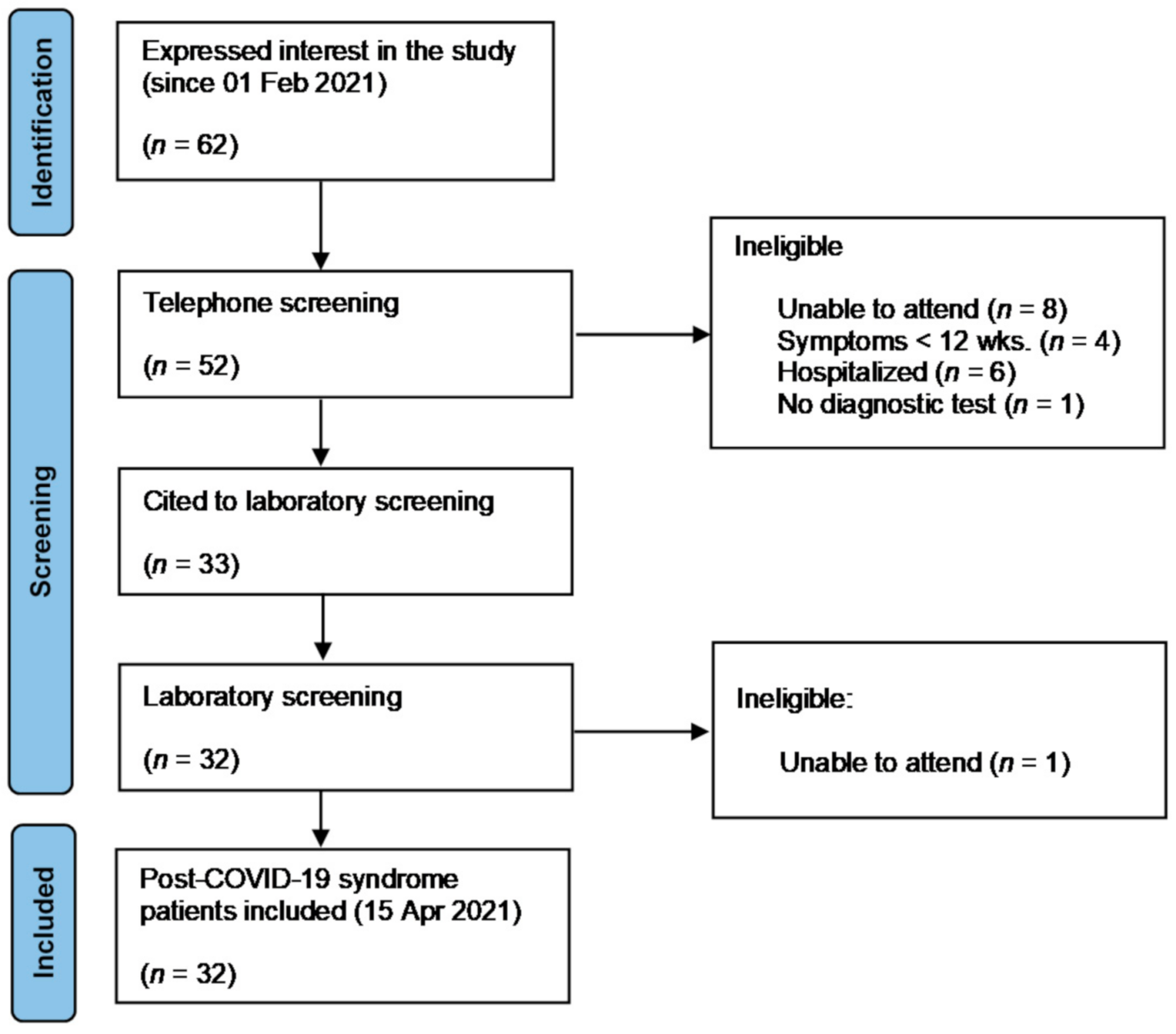
2.2. Participants
2.3. Echocardiography
2.4. Cardiorespiratory Fitness
2.5. Chronotropic Incompetence Diagnosis
2.6. Dyspnea, Fatigue, and Exercise Intolerance in Daily Living Activities
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lu, Y.; Li, X.; Geng, D.; Mei, N.; Wu, P.Y.; Huang, C.C.; Jia, T.; Zhao, Y.; Wang, D.; Xiao, A.; et al. Cerebral Micro-Structural Changes in COVID-19 Patients—An MRI-based 3-month Follow-up Study: A brief title: Cerebral Changes in COVID-19. EClinicalMedicine 2020, 25, 100484. [Google Scholar] [CrossRef] [PubMed]
- WHO Headquarters (HQ). A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus 2021. Available online: https://apps.who.int/iris/rest/bitstreams/1376291/retrieve (accessed on 19 October 2021).
- NICE (National Institute for Health and Care Excelence). COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19; 18 December 2020. Available online: https://pathways.nice.org.uk/ (accessed on 4 November 2021).
- UK Office for National Statistics. Prevalence of Ongoing Symptoms Following Coronavirus (COVID-19) Infection in the UK: 1 April 2021; UK Office for National Statistics: Newport, UK, 2021.
- Jimeno-Almazán, A.; Pallarés, J.G.; Buendía-Romero, Á.; Martínez-Cava, A.; Franco-López, F.; Sánchez-Alcaraz Martínez, B.J.; Bernal-Morel, E.; Courel-Ibáñez, J. Post-covid-19 syndrome and the potential benefits of exercise. Int. J. Environ. Res. Public Health 2021, 18, 5329. [Google Scholar] [CrossRef]
- Goldberger, A.L.S.P. UpToDate. Evaluation of Heart Rate Variability. Last Update 24 January 2020. Review 23 May 2021. Available online: https://www.uptodate.com/contents/evaluation-of-heart-rate-variability (accessed on 16 September 2021).
- Zhao, M.; Sun, L.; Liu, J.J.; Wang, H.; Miao, Y.; Zang, W.J. Vagal nerve modulation: A promising new therapeutic approach for cardiovascular diseases. Clin. Exp. Pharmacol. Physiol. 2012, 39, 701–705. [Google Scholar] [CrossRef]
- Natarajan, A.; Su, H.W.; Heneghan, C. Assessment of physiological signs associated with COVID-19 measured using wearable devices. Npj. Digit. Med. 2020, 3, 156. [Google Scholar] [CrossRef] [PubMed]
- Dani, M.; Dirksen, A.; Taraborrelli, P.; Torocastro, M.; Panagopoulos, D.; Sutton, R.; Lim, P.B. Autonomic dysfunction in ‘long COVID’: Rationale, physiology and management strategies. Clin. Med. J. R. Coll. Physicians Lond. 2021, 21, E63–E67. [Google Scholar] [CrossRef] [PubMed]
- Buchhorn, R.; Willaschek, C.; Baumann, C. SARS-CoV-2 infections and the autonomic nervous system. Monatsschr. Kinderheilkd. 2021, 169, 645–648. [Google Scholar] [CrossRef] [PubMed]
- Szekely, Y.; Lichter, Y.; Sadon, S.; Lupu, L.; Taieb, P.; Banai, A.; Sapir, O.; Granot, Y.; Hochstadt, A.; Friedman, S. Cardiorespiratory Abnormalities in Patients Recovering from Coronavirus Disease 2019. J. Am. Soc. Echocardiogr. 2021. Available online: https://linkinghub.elsevier.com/retrieve/pii/S089473172100701X (accessed on 13 September 2021). [CrossRef] [PubMed]
- Brubaker, P.H.; Kitzman, D.W. Chronotropic incompetence: Causes, consequences, and management. Circulation 2011, 123, 1010–1020. [Google Scholar] [CrossRef] [Green Version]
- Courel-Ibáñez, J.; the RECOVE Group. Rehabilitation for Post-COVID-19 Syndrome through a Supervised Exercise Intervention: The RECOVE Project [NCT04718506] 2021. Available online: https://clinicaltrials.gov/ct2/show/NCT04718506 (accessed on 28 March 2021).
- Human Performance & Sports Science. Available online: http://www.hpsportsscience.com/recove (accessed on 15 April 2021).
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef]
- Tyapochkin, K.; Kovaleva, M.; Smorodnikova, E.; Pravdin, P. Smartphone App Stress Assessments: Heart Rate variability vs Perceived Stress in a Large Group of Adults. medRxiv 2020. [Google Scholar] [CrossRef]
- Thomas, B.L.; Claassen, N.; Becker, P.; Viljoen, M. Validity of Commonly Used Heart Rate Variability Markers of Autonomic Nervous System Function. Neuropsychobiology 2019, 78, 14–26. [Google Scholar] [CrossRef]
- Björkman, F.; Ekblom-Bak, E.; Ekblom, Ö.; Ekblom, B. Validity of the revised Ekblom Bak cycle ergometer test in adults. Eur. J. Appl. Physiol. 2016, 116, 1627–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar] [PubMed]
- Pollock, M.L.; Bohannon, R.L.; Cooper, K.H.; Ayres, J.J.; Ward, A.; White, S.R.; Linnerud, A.C. A comparative analysis of four protocols for maximal treadmill stress testing. Am. Heart J. 1976, 92, 39–46. [Google Scholar] [CrossRef]
- Hulo, S.; Inamo, J.; Dehon, A.; Le Rouzic, O.; Edme, J.L.; Neviere, R. Chronotropic incompetence can limit exercise tolerance in COPD patients with lung hyperinflation. Int. J. COPD 2016, 11, 2553–2561. [Google Scholar] [CrossRef] [Green Version]
- Engeseth, K.; Hodnesdal, C.; Grundvold, I.; Liestøl, K.; Gjesdal, K.; Kjeldsen, S.E.; Erikssen, J.E.; Bodegard, J.; Skretteberg, P.T. Temporal reduction in chronotropic index predicts risk of cardiovascular death among healthy middle-aged men: A 28-year follow-up study. J. Am. Heart Assoc. 2016, 5, e004555. [Google Scholar] [CrossRef] [Green Version]
- Jackson, C. The Chalder Fatigue Scale (CFQ 11). Occup. Med. (Chic Ill) 2015, 65, 86. [Google Scholar] [CrossRef] [Green Version]
- Krupp, L.B.; Larocca, N.G.; Muir Nash, J.; Steinberg, A.D. The Fatigue Severity Scale: Application to Patients with Multiple Sclerosis and Systemic Lupus Erythematosus. Arch. Neurol. 1989, 46, 1121–1123. Available online: https://pubmed.ncbi.nlm.nih.gov/2803071/ (accessed on 19 August 2021). [CrossRef]
- Jason, L.A.; So, S.; Brown, A.A.; Sunnquist, M.; Evans, M. Test–retest reliability of the DePaul Symptom Questionnaire. Fatigue Biomed Health Behav. 2015, 3, 16–32. [Google Scholar] [CrossRef] [Green Version]
- Klok, F.A.; Boon, G.J.A.M.; Barco, S.; Endres, M.; Miranda Geelhoed, J.J.; Knauss, S.; Rezek, S.A.; Spruit, M.A.; Vehreschild, J.; Siegerink, B. The Post-COVID-19 Functional Status Scale: A Tool to Measure Functional Status over Time after COVID-19. Eur. Respir. J. 2020, 56, 2001494. Available online: https://pubmed.ncbi.nlm.nih.gov/32398306/ (accessed on 19 August 2021). [CrossRef]
- Mahler, D.A.; Wells, C.K. Evaluation of Clinical Methods for Rating Dyspnea. Chest 1988, 93, 580–586. Available online: https://pubmed.ncbi.nlm.nih.gov/3342669/ (accessed on 12 September 2021). [CrossRef] [Green Version]
- Singh, I.; Joseph, P.; Heerdt, P.M.; Cullinan, M.; Lutchmansingh, D.D.; Gulati, M.; Possick, J.D.; Systrom, D.M.; Waxman, A.B. Persistent Exertional Intolerance After COVID-19: Insights from Invasive Cardiopulmonary Exercise Testing. Chest 2021. online ahead of print. Available online: https://pubmed.ncbi.nlm.nih.gov/34389297/ (accessed on 13 September 2021). [CrossRef]
- Baratto, C.; Caravita, S.; Faini, A.; Perego, G.B.; Senni, M.; Badano, L.P.; Parati, G. Impact of COVID-19 on exercise pathophysiology: A combined cardiopulmonary and echocardiographic exercise study. J. Appl. Physiol. 2021, 130, 1470–1478. [Google Scholar] [CrossRef]
- Del Rio, R.; Marcus, N.J.; Inestrosa, N.C. Potential Role of Autonomic Dysfunction in Covid-19 Morbidity and Mortality. Front Physiol. 2020, 11, 561749. [Google Scholar] [CrossRef] [PubMed]
- Lam, G.Y.; Befus, A.D.; Damant, R.W.; Ferrara, G.; Fuhr, D.P.; Stickland, M.K.; Varughese, R.A.; Wong, E.Y.; Smith, M.P. Exertional Intolerance and Dyspnea with Preserved Lung Function: An Emerging Long COVID Phenotype? Respir. Res. 2021, 22, 222. Available online: https://pubmed.ncbi.nlm.nih.gov/34362372/ (accessed on 13 September 2021). [CrossRef] [PubMed]
- Nasserie, T.; Hittle, M.; Goodman, S.N. Assessment of the Frequency and Variety of Persistent Symptoms among Patients with COVID-19: A Systematic Review. JAMA Netw. Open 2021, 4, e2111417. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, F.M.; Lam, K.; Sounderajah, V.; Clarke, J.M.; Ashrafian, H.; Darzi, A. Characteristics and predictors of acute and chronic post-COVID syndrome: A systematic review and meta-analysis. EClinicalMedicine 2021, 36, 100899. [Google Scholar] [CrossRef]
- Kaliyaperumal, D.; Rk, K.; Alagesan, M.; Ramalingam, S. Characterization of Cardiac Autonomic Function in COVID-19 Using Heart Rate Variability: A Hospital Based Preliminary Observational Study. J. Basic Clin. Physiol. Pharmacol. 2021, 32, 247–253. Available online: https://www.degruyter.com/document/doi/10.1515/jbcpp-2020-0378/html (accessed on 20 October 2021). [CrossRef]
- Hasty, F.; García, G.; Dávila, H.; Wittels, S.H.; Hendricks, S.; Chong, S. Heart Rate Variability as a Possible Predictive Marker for Acute Inflammatory Response in COVID-19 Patients. Mil. Med. 2021, 186, e34–e38. Available online: https://academic.oup.com/milmed/article/186/1-2/e34/5989059 (accessed on 2 November 2021). [CrossRef]
- Bourdillon, N.; Yazdani, S.; Schmitt, L.; Millet, G.P. Effects of COVID-19 Lockdown on Heart Rate Variability. PLoS ONE 2020, 15, e0242303. Available online: https://pubmed.ncbi.nlm.nih.gov/33180839/ (accessed on 2 November 2021). [CrossRef]



{kind=link}
{kind=link}
| Variable | Variable | ||
|---|---|---|---|
| Age (years) | 44.7 ± 10.9 | Total mean symptoms (n) | 6.8 ± 3.3 |
| Sex (n) | Symptom’s length (weeks) | 23.1 ± 13.6 | |
| Male | 10 (31.3) | Symptoms | |
| Female | 22 (68.8) | Fatigue | 26 (81.3) |
| Body composition | Dyspnea | 18 (56.3) | |
| Body mass (kg) | 72.3 ± 14.8 | Lack of concentration | 18 (56.3) |
| Height (m) | 1.66 ± 0.10 | Memory problems or confusion | 17 (53.1) |
| BMI (kg·m−2) | 26.0 ± 4.4 | Low mood | 17 (53.1) |
| Fat mass (%) | 30.6 ± 8.3 | Brain fog | 17 (53.1) |
| Lean body mass (kg) | 49.9 ± 11.6 | Insomnia or sleep disturbances | 17 (53.1) |
| Comorbidity (n) | Headache | 13 (40.6) | |
| Psychiatric conditions | 12 (37.5) | Myalgia | 10 (31.3) |
| Asthma | 5 (15.6) | Anxiety | 10 (31.3) |
| Hypertension | 2 (6.3) | Loss of smell/taste | 9 (28.1) |
| Structural heart disease | 2 (6.3) | Hair loss | 8 (25.0) |
| COPD | 1 (3.1) | Chest pain | 8 (25.0) |
| Diabetes | 1 (3.1) | Dizziness | 7 (21.9) |
| Toxic habits (n) | Low-grade fever | 7 (21.9) | |
| Alcohol | 3 (9.4) | Palpitations | 5 (15.6) |
| Active smoker | 2 (6.3) | Weight loss | 5 (15.6) |
| Former smoker | 9 (28.1) | Cough | 4 (12.5) |
| Medication (n) | Diarrhea | 4 (12.5) | |
| Taking medication | 25 (78.1) | Abdominal pain | 3 (9.4) |
| Antidepressants | 13 (40.6) | Loss appetite | 3 (9.4) |
| Benzodiazepines | 11 (34.4) | Nausea and/or vomiting | 2 (6.3) |
| Bronchodilators | 7 (21.9) | Evolution | |
| Fluctuating course | 19 (59.4) | ||
| Progressive improvement | 23 (71.9) |
| Age, Sex | Main Symptoms | Symptoms (Length in Weeks) | HRV-RMSSD (ms) | Estimated HRmax (bpm) | Test HRmax (bpm) | CI (% HRmax) |
|---|---|---|---|---|---|---|
| 52, female | Cephalea, mental fog, cognitive impairment, anosmia, ageusia, dyspnea | 9 (20) | 55.1 | 173 | 102 | Positive (62.1) |
| 30, male | Cephalea, anosmia/dysgeusia, dyspnea, fatigue | 7 (17) | 75.9 | 186 | 121 | Positive (71.0) |
| 50, male | Mental fog, anosmia/dysgeusia, fatigue | 3 (18) | 82.4 | 174 | 126 | Positive (72.9) |
| 47, male | Dyspnea, fatigue | 2 (12) | 32.4 | 177 | 128 | Positive (72.3) |
| Variable | All | Positive Chronotropic Diagnosed | Negative Chronotropic Diagnosed | Sig. (p) |
|---|---|---|---|---|
| Echocardiography | ||||
| LVEF (%) | 62.7 ± 3.7 | 59.7 ± 2.6 | 63.1 ± 3.7 | 0.070 |
| RV-TAPSE (mm) | 22.9 ± 2.3 | 23.5 ± 2.7 | 22.8 ± 2.3 | 0.671 |
| LVEDV (cm3/m2) | 42.8 ± 5.0 | 42.1 ± 4.6 | 42.9 ± 5.1 | 0.769 |
| E/A (cm·s−1) | 1.2 ± 0.4 | 1.2 ± 0.4 | 1.1 ± 0.4 | 0.936 |
| Fatigue and exercise intolerance | ||||
| CFQ-11 Likert | 21.9 ± 7.3 | 20 ± 13.1 | 22.1 ± 6.7 | 0.805 |
| CFQ-11 bimodal | 7.7 ± 3.0 | 6.6 ± 3.5 | 7.8 ± 2.9 | 0.612 |
| FSS | 5.3 ± 1.2 | 6.2 ± 1.3 | 5.2 ± 1.2 | 0.344 |
| DSQ-14 frequency | 30.4 ± 8.9 | 33.6 ± 7.2 | 30.1 ± 9.1 | 0.498 |
| DSQ-14 severity | 26.1 ± 9.3 | 32.6 ± 10.0 | 25.4 ± 9.1 | 0.209 |
| DSQ-14 0–100 | 54.8 ± 20.2 | 49.7 ± 35.8 | 55.6 ± 18.0 | 0.597 |
| PCFS | 2.4 ± 1.0 | 1.5 ± 0.7 | 2.5 ± 1.0 | 0.162 |
| mMRC | 1.3 ± 0.9 | 2.0 ± 1.0 | 1.3 ± 0.9 | 0.361 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jimeno-Almazán, A.; Pallarés, J.G.; Buendía-Romero, Á.; Martínez-Cava, A.; Courel-Ibáñez, J. Chronotropic Incompetence in Non-Hospitalized Patients with Post-COVID-19 Syndrome. J. Clin. Med. 2021, 10, 5434. https://doi.org/10.3390/jcm10225434
Jimeno-Almazán A, Pallarés JG, Buendía-Romero Á, Martínez-Cava A, Courel-Ibáñez J. Chronotropic Incompetence in Non-Hospitalized Patients with Post-COVID-19 Syndrome. Journal of Clinical Medicine. 2021; 10(22):5434. https://doi.org/10.3390/jcm10225434
Chicago/Turabian StyleJimeno-Almazán, Amaya, Jesús G. Pallarés, Ángel Buendía-Romero, Alejandro Martínez-Cava, and Javier Courel-Ibáñez. 2021. "Chronotropic Incompetence in Non-Hospitalized Patients with Post-COVID-19 Syndrome" Journal of Clinical Medicine 10, no. 22: 5434. https://doi.org/10.3390/jcm10225434
APA StyleJimeno-Almazán, A., Pallarés, J. G., Buendía-Romero, Á., Martínez-Cava, A., & Courel-Ibáñez, J. (2021). Chronotropic Incompetence in Non-Hospitalized Patients with Post-COVID-19 Syndrome. Journal of Clinical Medicine, 10(22), 5434. https://doi.org/10.3390/jcm10225434