
Obesity and Uncontrolled Diabetes Predict Depression in HF Patients

 ,
,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Data Collection
2.3. Depression Assessment
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data of HF Patients
3.2. Demographic and Clinical Data of the Patients with and without Depression
3.3. Biochemical and Echocardiographic Indices of Patients with and without Depression
3.4. Demographic and Clinical Data of Patients according to EF
3.5. Biochemical and Echocardiographic Indices of Patients according to EF
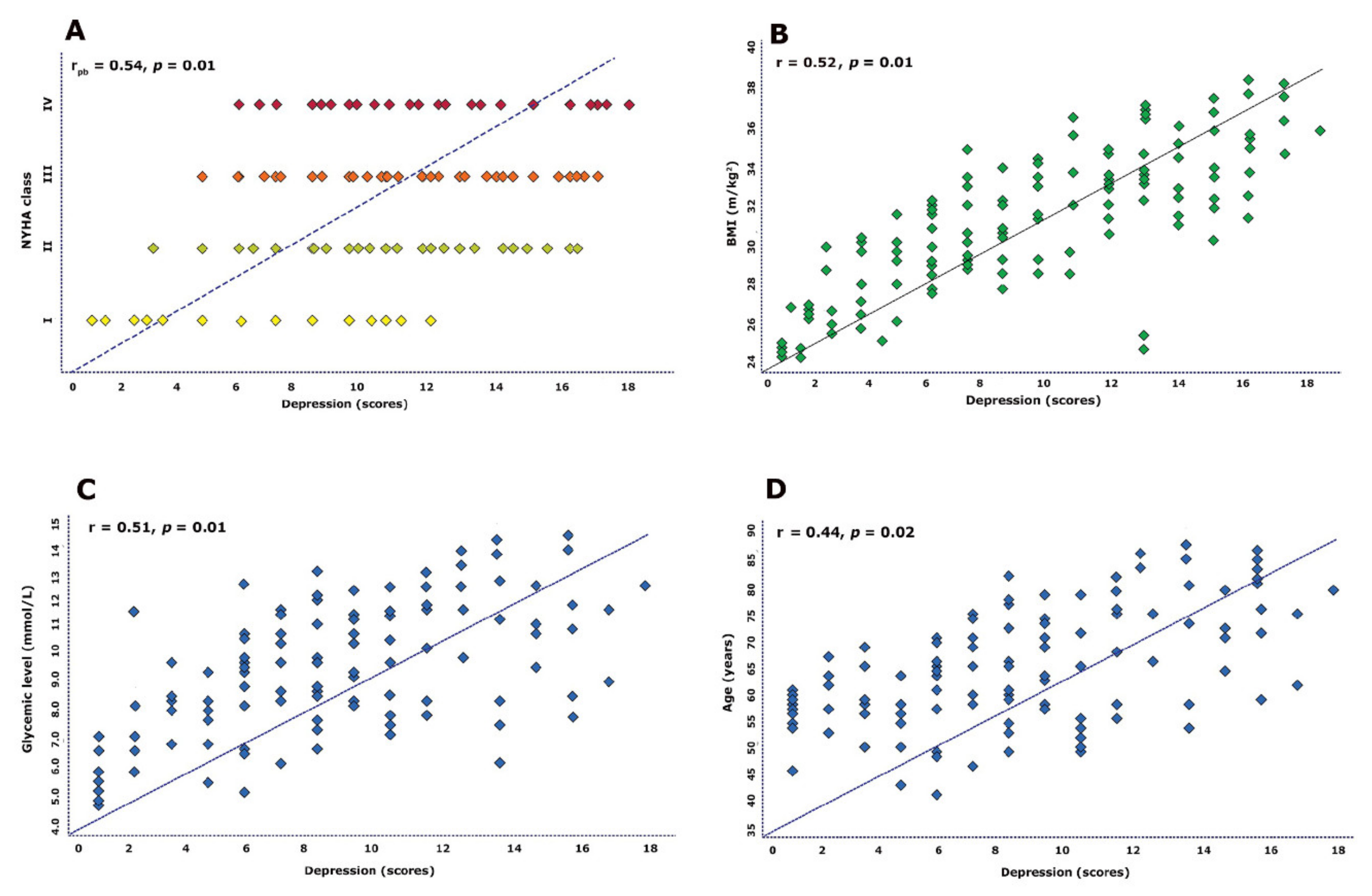
3.6. Correlation between Cardiovascular Risk Factors and Depression
3.7. Predictors of Depression in the Studied Cohort
4. Discussion
4.1. Findings
4.2. Data Interpretation
4.3. Clinical Implications
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bytyçi, I.; Bajraktari, G. Mortality in heart failure patients. Anadolu Kardiyol. Derg. 2015, 15, 63–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alves, T.C.; Rays, J.; Fraguas, R., Jr.; Wajngarten, M.; Telles, R.M.; Duran, F.L.; Meneghetti, J.C.; Robilotta, C.C.; Prando, S.; De Castro, C.C.; et al. Association between major depressive symptoms in heat failure and impaired regional cerebral blood flow in the medial temporal region: A study using 99tc-HMPAO single photon emission computerized tomography (SPECT). Psychol. Med. 2006, 36, 597–608. [Google Scholar] [CrossRef] [PubMed]
- Szyguła-Jurkiewicz, B.; Zakliczyński, M.; Ploch, M.; Mościński, M.; Partyka, R.; Wojnicz, R.; Zembala, M.; Polonski, L. Depression is the strongest predictor of long-term outcome in patients with chronic nonischemic heart failure. Pol. J. Cardio-Thorac. Surg. 2014, 11, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Rigas, A.; Farmakis, D.; Papingiotis, G.; Bakosis, G.; Parissis, J. Hypothalamic dysfunction in heart failure: Pathogenetic mechanisms and therapeutic implications. Fail. Rev. 2018, 23, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.A.; Chapa, D.W.; Friedmann, E.; Durden, C.; Ross, A.; Lee, M.C.; Lee, H.J. Depression in patients with heart failure: Prevalence, pathophysiological mechanisms, and treatment. Crit. Care Nurse 2008, 28, 40–55. [Google Scholar] [CrossRef] [PubMed]
- Norra, C.; Skobel, E.C.; Arndt, M.; Schauerte, P. High impact of depression in heart failure: Early diagnosis and treatment options. Int. J. Cardiol. 2008, 125, 220–231. [Google Scholar] [CrossRef]
- Pintor, L. Heart failure and depression, an often-neglected combination. Rev. Esp. Cardiol. 2006, 59, 761–765. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S. ESC Scientific Document Group. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [PubMed]
- Steinhaus, M.E.; Buller, L.T.; Romero, J.A.; Lee, Y.Y.; Figgie, M.P.; McLawhorn, A.S. Body Mass Index Classification Is Independently Associated with Health-Related Quality of Life after Primary Total Knee Arthroplasty: An Institutional Registry-Based Study. J. Knee Surg. 2020, 33, 399–409. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Rozanski, A.; Blumenthal, J.A.; Kaplan, J. Impact of psychological factors on the pathogenesis of cardiovascular disease and implications for therapy. Circulation 1999, 99, 2192–2217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carney, R.M.; Freedland, K.E. Depression and coronary heart disease. Nat. Rev. Cardiol. 2017, 14, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Rutledge, T.; Reis, V.A.; Linke, S.E.; Greenberg, B.H.; Mills, P.J. Depression in heart failure a meta-analytic review of prevalence, intervention effects, and associations with clinical outcomes. J. Am. Coll. Cardiol. 2006, 48, 1527–1537. [Google Scholar] [CrossRef] [Green Version]
- Celano, C.M.; Villegas, A.C.; Albanese, A.M.; Gaggin, H.K.; Huffman, J.C. Depression and Anxiety in Heart Failure: A Review. Harv. Rev. Psychiatry 2018, 26, 175–184. [Google Scholar] [CrossRef]
- Faris, R.; Purcell, H.; Henein, M.Y.; Coats, A.J. Clinical depression is common and significantly associated with reduced survival in patients with non-ischaemic heart failure. Eur. J. Heart Fail. 2002, 4, 541–551. [Google Scholar] [CrossRef] [Green Version]
- Jiang, W.; Kuchibhatla, M.; Clary, G.L.; Cuffe, M.S.; Christopher, E.J.; Alexander, J.D.; Califf, R.M.; Krishnan, R.R.; O’Connor, C.M. Relationship between depressive symptoms and long-term mortality in patients with heart failure. Am. Heart J. 2007, 154, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Konstam, V.; Moser, D.K.; De Jong, M.J. Depression and anxiety in heart failure. J. Card Fail. 2005, 11, 455–463. [Google Scholar] [CrossRef]
- Celik, E.; Cay, S.; Sensoy, B.; Murat, S.; Oksuz, F.; Cankurt, T.; Ali Mendi, M. Heart Failure Functional Class Associated with Depression Severity But Not Anxiety Severity. Acta Cardiol. Sin. 2016, 32, 55–61. [Google Scholar]
- Nichols, G.A.; Moler, E.J. Cardiovascular disease, heart failure, chronic kidney disease and depression independently increase the risk of incident diabetes. Diabetologia 2011, 54, 523–526. [Google Scholar] [CrossRef] [Green Version]
- Anderson, R.J.; Freedland, K.E.; Clouse, R.E.; Lustman, P.J. The prevalence of comorbid depression in adults with diabetes: A meta-analysis. Diabetes Care 2001, 24, 1069–1078. [Google Scholar] [CrossRef] [Green Version]
- Heo, S.; Moser, D.K.; Pressler, S.J.; Dunbar, S.B.; Lee, K.S.; Kim, J.; Lennie, T.A. Association between obesity and heart failure symptoms in male and female patients. Clin. Obes. 2017, 7, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Batalli, A.; Ibrahimi, P.; Bytyçi, I.; Ahmeti, A.; Haliti, E.; Elezi, S.; Henein, M.Y.; Bajraktari, G. Different determinants of exercise capacity in HFpEF compared to HFrEF. Cardiovasc. Ultrasound 2017, 15, 12. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | HFrEF without Depression (n = 81) | HFrEF with Depression (n = 23) | p Value | HFpEF without Depression (n = 37) | HFpEF with Depression (n = 10) | p Value |
|---|---|---|---|---|---|---|
| Clinical indices | ||||||
| Age | 71.1 ± 11 | 68.2 ± 10 | 0.12 | 60.1 ± 12 | 68.2 ± 11 | 0.04 |
| Sex (female, %) | 41 (50.6) | 14 (60.8) | 0.03 | 18 (48.6) | 6 (60) | 0.01 |
| Smoking (n, %) | 21 (25.9) | 5 (21.7) | 0.12 | 8 (21.6) | 2 (20) | 0.33 |
| BMI (m/kg2) | 26.3 ± 3.5 | 30.4 ± 2.9 | 0.04 | 27.9 ± 3.3 | 28.8 ± 4.4 | 0.13 |
| Underweight (n, %) | 1 (1.23) | 0 (0) | 0.04 | 0 (0) | 0 (0) | 0.77 |
| Normal weight (n, %) | 29 (35.8) | 11 (47.8) | 0.03 | 13 (43.2) | 4 (40) | 0.31 |
| Overweight (n, %) | 29 (35.8) | 10 (43.5) | 0.04 | 15 (40.5) | 5 (50) | 0.003 |
| Obese (n, %) | 21 (25.9) | 8 (34.7) | 0.02 | 10 (27.0) | 4 (40) | 0.002 |
| SBP (mmHg) | 106 ± 15 | 108 ± 14 | 0.63 | 111 ± 16 | 109 ± 14 | 0.70 |
| DBP (mmHg) | 78.1 ± 10 | 75 ± 13 | 0.32 | 83 ± 12 | 78 ± 16 | 0.52 |
| HR (beats/min) | 75 ± 10 | 73 ± 11 | 0.31 | 76 ± 13 | 74 ± 10 | 0.41 |
| NYHA class | 1.8 ± 1.0 | 2.9 ± 1.1 | 0.02 | 1.8 ± 0.9 | 2.9 ± 1.1 | 0.03 |
| Comorbidities | ||||||
| AH (n, %) | 56 (69.1) | 14 (60.9) | 0.08 | 24 (64.8) | 6 (60) | 0.10 |
| DM (n, %) | 39 (48.1) | 13 (56.5) | 0.04 | 16 (43.1) | 5 (50) | 0.03 |
| Dyslipidemia | 23 (28.4) | 7 (30.4) | 0.51 | 10 (27.0) | 3 (30) | 0.61 |
| CHD (n, %) | 41 (50.6) | 12 (52.2) | 0.21 | 14 (37.8) | 4 (40) | 0.33 |
| AF (n, %) | 40 (51.8) | 15 (65.2) | 0.01 | 12 (32.4) | 4 (40) | 0.03 |
| Drugs | ||||||
| Aspirin (n, %) | 64 (79.1) | 18 (78.2) | 0.27 | 28 (75.7) | 8 (80) | 0.47 |
| ACE/ARBs (n, %) | 67 (82.7) | 19 (82.6) | 0.55 | 30 (81.1) | 8 (80) | 0.35 |
| Diuretics (n, %) | 58 (71.6) | 20 (86.9) | 0.001 | 22 (59.5) | 7 (70) | 0.02 |
| BB (n, %) | 64 (79.1) | 19 (78.2) | 0.20 | 26 (70.3) | 7 (70) | 0.80 |
| CCB (n, %) | 11 (13.6) | 3 (13.1) | 0.51 | 7 (18.9) | 2 (20) | 0.33 |
| Antiarrhythmic (n, %) | 14 (17.3) | 5 (21.7) | 0.21 | 6 (16.2) | 2 (20) | 0.09 |
| Anticoagulation (n, %) | 15 (18.5) | 7 (30.4) | 0.01 | 4 (10.8) | 1 (10) | 0.21 |
| Statins (n, %) | 29 (29.6) | 7 (30.4) | 0.41 | 6 (16.2) | 1 (10) | 0.11 |
| Variable | HFrEF without Depression (n = 81) | HFrEF with Depression (n = 23) | p Value | HFpEF without Depression (n = 37) | HFpEF with Depression (n = 10) | p Value |
|---|---|---|---|---|---|---|
| Laboratory data | ||||||
| Glucose (mmol/L) | 5.9 ± 2.2 | 5.6 ± 1.2 | 0.02 | 5.6 ± 1.2 | 8.2 ± 3.2 | 0.02 |
| Urea (mmol/L) | 9.4 ± 5.6 | 16.1 ± 6.2 | 0.03 | 8.3 ± 4.2 | 14 ± 5.1 | 0.04 |
| Creatinine (umol/L) | 125 ± 11 | 165 ± 25 | 0.01 | 123 ± 11 | 145 ± 19 | 0.02 |
| Bilirubin (mg/dL) | 4.1 ± 1.1 | 5.5 ± 1.1 | 0.21 | 3.8 ± 1.3 | 4.9 ± 1.3 | 0.33 |
| ALT (U/L) | 30 ± 10 | 37 ± 11 | 0.32 | 34 ± 11 | 30 ± 10 | 0.18 |
| AST (U/L) | 33 ± 13 | 28 ± 10 | 0.51 | 30 ± 10 | 28 ± 14 | 0.31 |
| Albumin (g/L) | 30.3 ± 8.5 | 33 ± 9.1 | 0.24 | 31 ± 10 | 33 ± 9.6 | 0.32 |
| Protein (g/L) | 59 ± 11 | 61 ± 10 | 0.24 | 62 ± 10 | 64 ± 11 | 0.28 |
| Cholesterol (mmol/L) | 6.8± 3.2 | 6.2 ± 3.1 | 0.22 | 5.9 ± 3.5 | 6.8 ± 3.1 | 0.38 |
| Triglyceride (mmol/L) | 1.9 ± 0.8 | 2.1 ± 0.9 | 0.31 | 1.9 ± 0.8 | 2.2 ± 0.7 | 0.22 |
| WBC (103/mm3) | 9.4 ± 4.3 | 8.2 ± 4.6 | 0.29 | 9.2 ± 4.6 | 8.9 ± 3.4 | 0.37 |
| RBC (106/mm3) | 3.9 ± 1.2 | 4.4 ± 1.2 | 0.23 | 4.1 ± 1.2 | 4.7 ± 1.1 | 0.38 |
| Platelet (103/mm3 | 212± 23 | 217± 22 | 0.21 | 209± 21 | 215 ± 25 | 0.11 |
| Iron (umol/L) | 8.8 ± 2.8 | 13.1 ± 3.1 | 0.03 | 10.2 ± 3.1 | 9.9 ± 2.5 | 0.20 |
| Variable | HFrEF without Depression (n = 81) | HFrEF with Depression (n = 23) | p Value | HFpEF without Depression (n = 37) | HFpEF with Depression (n = 10) | p Value |
|---|---|---|---|---|---|---|
| LV EDD (cm) | 5.7 ± 0.6 | 6.1 ± 0.7 | 0.10 | 5.1 ± 0.4 | 5.3 ± 0.6 | 0.33 |
| LV ESD (cm) | 3.5 ± 0.4 | 3.9 ± 0.4 | 0.21 | 3.6 ± 0.4 | 3.8 ± 0.5 | 0.23 |
| IVSd (cm) | 1.1 ± 0.1 | 1.0 ± 0.1 | 0.30 | 1.1 ± 0.1 | 1.2 ± 0.2 | 0.38 |
| LVPWd (cm) | 1.1 ± 0.2 | 1.1 ± 0.2 | 0.18 | 1.0 ± 0.1 | 1.1 ± 0.2 | 0.29 |
| LV EF (%) | 36 ± 2.8 | 34 ± 3.5 | 0.44 | 53 ± 2.9 | 55 ± 4.3 | 0.51 |
| LA diameter (cm) | 4.4 ± 4.4 | 4.6 ± 4.2 | 0.10 | 4.1 ± 3.9 | 4.2 ± 5.6 | 0.12 |
| RA diameter (cm) | 3.7 ± 1.4 | 3.8 ± 1.5 | 0.23 | 3.4 ± 1.6 | 3.5 ± 1.3 | 0.28 |
| RV diameter (cm) | 3.3 ± 1.2 | 3.5 ± 1.2 | 0.55 | 3.1 ± 1.1 | 3.2 ± 1.3 | 0.44 |
| Variable | Univariate Predictors OR (95% CI) | p Value | Multivariate Predictors OR (95% CI) | p Value |
|---|---|---|---|---|
| HF patients | ||||
| Age | 1.231(1.051 to 2.401) | 0.03 | 1.362 (0.989 to 3.824) | 0.10 |
| Female gender | 2.735 (1.337 to 5.595) | 0.04 | 1.562 (0.809 to 4.024) | 0.22 |
| NYHA class > II | 2.035 (1.437 to 4.595) | 0.01 | 2.103 (1.389 to 4.700) | 0.01 |
| AH | 1.018 (0.509 to 3.903) | 0.61 | ||
| CHD | 1.141 (0.819 to 3.898) | 0.11 | ||
| BMI | 1.201 (0.909 to 4.108) | 0.10 | ||
| BMI ≥ 30 kg/m2 | 1.630 (1.207 to 3.803) | 0.01 | 1.890 (1.199 to 3.551) | 0.02 |
| Diabetes | 1.105 (0.895 to 3.796) | 0.09 | ||
| Glycemic level ≥ 8.5 mmol/L | 2.105 (1.405 to 3.796) | 0.001 | 2.802 (1.709 to 5.077) | 0.01 |
| HFrEF | ||||
| Age | 1.191(1.091 to 3.001) | 0.04 | 1.701 (0.913 to 3.119) | 0.11 |
| Female gender | 1.135 (0.937 to 2.095) | 0.10 | ||
| NYHA class > II | 1.830 (1.237 to 3.005) | 0.007 | 2.091 (1.613 to 4.009) | 0.01 |
| AH | 1.098 (0.811 to 3.211) | 0.22 | ||
| CHD | 1.109 (0.709 to 2.898) | 0.31 | ||
| BMI | 1.009 (0.801 to 3.701) | 0.18 | ||
| BMI ≥ 30kg/m2 | 1.890 (1.331 to 3.908) | 0.01 | 1.911 (1.401 to 4.018) | 0.03 |
| Diabetes | 1.205 (0.801 to 3.406) | 0.21 | ||
| Glycemic level ≥ 8.5 mmol/L | 1.961 (1.519 to 3.676) | 0.02 | 2.013 (1.519 to 4.101) | 0.01 |
| HFpEF | ||||
| Age | 1.161(1.007 to 1.399) | 0.02 | 1.301(0.977 to 3.019) | 0.08 |
| Female gender | 1.511 (1.193 to 3.121) | 0.04 | 1.591(1.110 to 3.029) | 0.04 |
| NYHA class > II | 1.311 (1.107 to 2.901) | 0.08 | ||
| AH | 1.011 (0.307 to 2.101) | 0.22 | ||
| CHD | 1.122 (0.530 to 2.537) | 0.61 | ||
| BMI | 1.129 (0.817 to 3.160) | 0.11 | ||
| BMI ≥ 30kg/m2 | 2.047 (1.108 to 3.397) | 0.02 | 1.926 (1.502 to 4.011) | 0.02 |
| Diabetes | 1.118 (0.909 to 2.915) | 0.17 | ||
| Glycemic level ≥ 8.5 mmol/L | 1.808 (1.015 to 3.541) | 0.03 | 1.703 (1.311 to 3101) | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fetahu, A.; Rrustemi, K.; Henein, M.Y.; Bytyçi, B.; Mehmeti, F.; Bytyçi, I.; Kamberi, L. Obesity and Uncontrolled Diabetes Predict Depression in HF Patients. J. Clin. Med. 2021, 10, 5663. https://doi.org/10.3390/jcm10235663
Fetahu A, Rrustemi K, Henein MY, Bytyçi B, Mehmeti F, Bytyçi I, Kamberi L. Obesity and Uncontrolled Diabetes Predict Depression in HF Patients. Journal of Clinical Medicine. 2021; 10(23):5663. https://doi.org/10.3390/jcm10235663
Chicago/Turabian StyleFetahu, Albenita, Kaltrinë Rrustemi, Michael Y. Henein, Besim Bytyçi, Flamure Mehmeti, Ibadete Bytyçi, and Lulzim Kamberi. 2021. "Obesity and Uncontrolled Diabetes Predict Depression in HF Patients" Journal of Clinical Medicine 10, no. 23: 5663. https://doi.org/10.3390/jcm10235663
APA StyleFetahu, A., Rrustemi, K., Henein, M. Y., Bytyçi, B., Mehmeti, F., Bytyçi, I., & Kamberi, L. (2021). Obesity and Uncontrolled Diabetes Predict Depression in HF Patients. Journal of Clinical Medicine, 10(23), 5663. https://doi.org/10.3390/jcm10235663