
Intraperitoneal Chemotherapy as Adjuvant or Perioperative Chemotherapy for Patients with Type 4 Scirrhous Gastric Cancer: PHOENIX-GC2 Trial

 , ,
, ,  ,
,
Abstract
:1. Introduction
1.1. Characteristics of Type 4 Gastric Cancer
1.2. Treatment of Locally Advanced Gastric Cancer
1.3. Treatment of Gastric Cancer with Positive Peritoneal Lavage Cytology
1.4. Intraperitoneal Chemotherapy for Gastric Cancer
1.4.1. S-1/PTX+IP PTX Regimen
1.4.2. SOX+IP PTX Regimen
1.5. Intraperitoneal Chemotherapy Combined with Gastrectomy
2. Methods
2.1. Objective
2.2. Eligibility Criteria
2.3. Endpoints
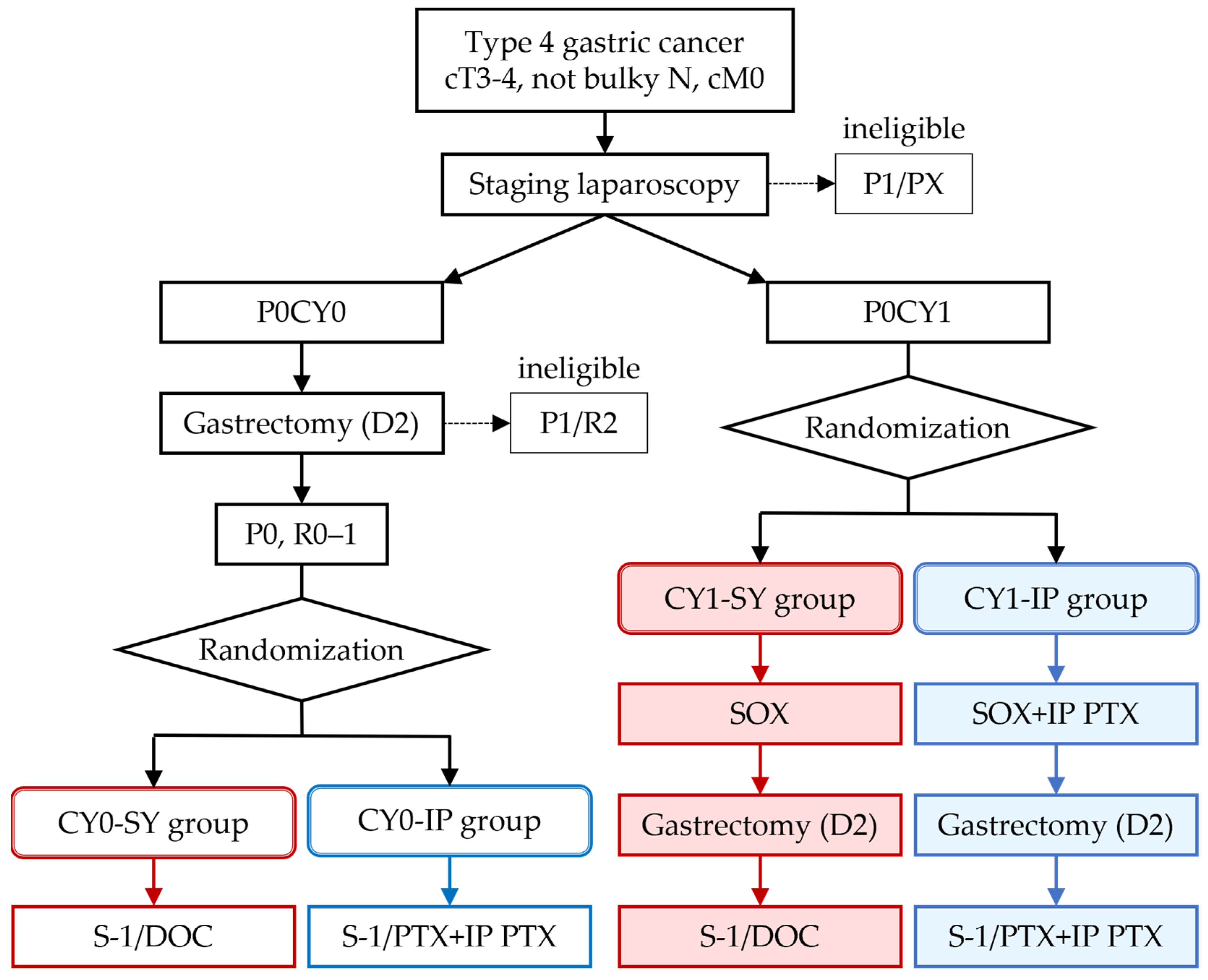
2.4. Study Design and Procudure
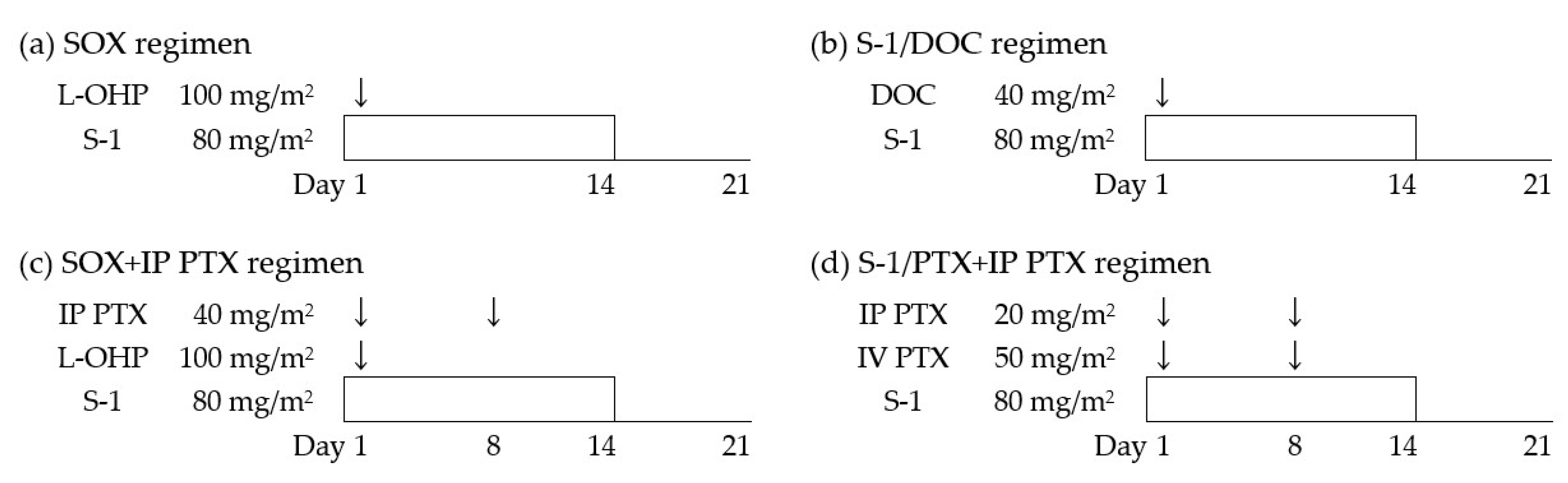
2.5. Chemotherapy Regimens
2.6. Sample Size Calculation and Statistical Considerations
3. Future Perspective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer 2011, 14, 101–112. [Google Scholar] [CrossRef] [Green Version]
- Katai, H.; Ishikawa, T.; Akazawa, K.; Isobe, Y.; Miyashiro, I.; Oda, I.; Tsujitani, S.; Ono, H.; Tanabe, S.; Fukagawa, T.; et al. Five-year survival analysis of surgically resected gastric cancer cases in Japan: A retrospective analysis of more than 100,000 patients from the nationwide registry of the Japanese Gastric Cancer Association (2001–2007). Gastric Cancer 2018, 21, 144–154. [Google Scholar] [CrossRef]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer 2021, 24, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Sakuramoto, S.; Sasako, M.; Yamaguchi, T.; Kinoshita, T.; Fujii, M.; Nashimoto, A.; Furukawa, H.; Nakajima, T.; Ohashi, Y.; Imamura, H.; et al. Adjuvant chemotherapy for gastric cancer with S-1, an oral fluoropyrimidine. N. Engl. J. Med. 2007, 357, 1810–1820. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Kodera, Y.; Kochi, M.; Ichikawa, W.; Kakeji, Y.; Sano, T.; Nagao, N.; Takahashi, M.; Takagane, A.; Watanabe, T.; et al. Addition of Docetaxel to Oral Fluoropyrimidine Improves Efficacy in Patients With Stage III Gastric Cancer: Interim Analysis of JACCRO GC-07, a Randomized Controlled Trial. J. Clin. Oncol. 2019, 37, 1296–1304. [Google Scholar] [CrossRef]
- Bang, Y.J.; Kim, Y.W.; Yang, H.K.; Chung, H.C.; Park, Y.K.; Lee, K.H.; Lee, K.W.; Kim, Y.H.; Noh, S.I.; Cho, J.Y.; et al. Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): A phase 3 open-label, randomised controlled trial. Lancet 2012, 379, 315–321. [Google Scholar] [CrossRef]
- Tsuburaya, A.; Mizusawa, J.; Tanaka, Y.; Fukushima, N.; Nashimoto, A.; Sasako, M.; Stomach Cancer Study Group of the Japan Clinical Oncology Group. Neoadjuvant chemotherapy with S-1 and cisplatin followed by D2 gastrectomy with para-aortic lymph node dissection for gastric cancer with extensive lymph node metastasis. Br. J. Surg. 2014, 101, 653–660. [Google Scholar] [CrossRef]
- Iwasaki, Y.; Terashima, M.; Mizusawa, J.; Katayama, H.; Nakamura, K.; Katai, H.; Yoshikawa, T.; Ito, S.; Kaji, M.; Kimura, Y.; et al. Gastrectomy with or without neoadjuvant S-1 plus cisplatin for type 4 or large type 3 gastric cancer (JCOG0501): An open-label, phase 3, randomized controlled trial. Gastric Cancer 2021, 24, 492–502. [Google Scholar] [CrossRef]
- Honma, Y.; Yamada, Y.; Terazawa, T.; Takashima, A.; Iwasa, S.; Kato, K.; Hamaguchi, T.; Shimada, Y.; Ohashi, M.; Morita, S.; et al. Feasibility of neoadjuvant S-1 and oxaliplatin followed by surgery for resectable advanced gastric adenocarcinoma. Surg. Today 2016, 46, 1076–1082. [Google Scholar] [CrossRef]
- Kang, Y.K.; Yook, J.H.; Park, Y.K.; Lee, J.S.; Kim, Y.W.; Kim, J.Y.; Ryu, M.H.; Rha, S.Y.; Chung, I.J.; Kim, I.H.; et al. PRODIGY: A Phase III Study of Neoadjuvant Docetaxel, Oxaliplatin, and S-1 Plus Surgery and Adjuvant S-1 Versus Surgery and Adjuvant S-1 for Resectable Advanced Gastric Cancer. J. Clin. Oncol. 2021, 39, 2903–2913. [Google Scholar] [CrossRef] [PubMed]
- Al-Batran, S.E.; Homann, N.; Pauligk, C.; Goetze, T.O.; Meiler, J.; Kasper, S.; Kopp, H.G.; Mayer, F.; Haag, G.M.; Luley, K.; et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet 2019, 393, 1948–1957. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, J.S.; Smalley, S.R.; Benedetti, J.; Hundahl, S.A.; Estes, N.C.; Stemmermann, G.N.; Haller, D.G.; Ajani, J.A.; Gunderson, L.L.; Jessup, J.M.; et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N. Engl. J. Med. 2001, 345, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, W.; Narahara, H.; Hara, T.; Takagane, A.; Akiya, T.; Takagi, M.; Miyashita, K.; Nishizaki, T.; Kobayashi, O.; Takiyama, W.; et al. S-1 plus cisplatin versus S-1 alone for first-line treatment of advanced gastric cancer (SPIRITS trial): A phase III trial. Lancet Oncol. 2008, 9, 215–221. [Google Scholar] [CrossRef]
- Yamada, Y.; Higuchi, K.; Nishikawa, K.; Gotoh, M.; Fuse, N.; Sugimoto, N.; Nishina, T.; Amagai, K.; Chin, K.; Niwa, Y.; et al. Phase III study comparing oxaliplatin plus S-1 with cisplatin plus S-1 in chemotherapy-naive patients with advanced gastric cancer. Ann. Oncol. 2015, 26, 141–148. [Google Scholar] [CrossRef]
- Koizumi, W.; Kim, Y.H.; Fujii, M.; Kim, H.K.; Imamura, H.; Lee, K.H.; Hara, T.; Chung, H.C.; Satoh, T.; Cho, J.Y.; et al. Addition of docetaxel to S-1 without platinum prolongs survival of patients with advanced gastric cancer: A randomized study (START). J. Cancer Res. Clin. Oncol. 2014, 140, 319–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kodera, Y.; Ito, S.; Mochizuki, Y.; Kondo, K.; Koshikawa, K.; Suzuki, N.; Kojima, H.; Kojima, T.; Matsui, T.; Takase, T.; et al. A phase II study of radical surgery followed by postoperative chemotherapy with S-1 for gastric carcinoma with free cancer cells in the peritoneal cavity (CCOG0301 study). Eur. J. Surg. Oncol. 2009, 35, 1158–1163. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Takashima, A.; Nagashima, K.; Terashima, M.; Aizawa, M.; Ohashi, M.; Tanaka, R.; Yamada, T.; Kinoshita, T.; Matsushita, H.; et al. Impact of preoperative chemotherapy as initial treatment for advanced gastric cancer with peritoneal metastasis limited to positive peritoneal lavage cytology (CY1) or localized peritoneal metastasis (P1a): A multi-institutional retrospective study. Gastric Cancer 2021, 24, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Markman, M.; Rowinsky, E.; Hakes, T.; Reichman, B.; Jones, W.; Lewis, J.L., Jr.; Rubin, S.; Curtin, J.; Barakat, R.; Phillips, M.; et al. Phase I trial of intraperitoneal taxol: A Gynecoloic Oncology Group study. J. Clin. Oncol. 1992, 10, 1485–1491. [Google Scholar] [CrossRef]
- Armstrong, D.K.; Bundy, B.; Wenzel, L.; Huang, H.Q.; Baergen, R.; Lele, S.; Copeland, L.J.; Walker, J.L.; Burger, R.A.; Gynecologic Oncology, G. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N. Engl. J. Med. 2006, 354, 34–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fushida, S.; Fujita, H.; Kinami, S.; Ninomiya, I.; Fujimura, T.; Nishimura, G.; Ohta, T. Effectiveness of intraperitoneal chemotherapy using new-aged drugs for the peritoneal dissemination of gastric cancer. Gan To Kagaku Ryoho 2005, 32, 1691–1694. [Google Scholar]
- Ishigami, H.; Kitayama, J.; Otani, K.; Kamei, T.; Soma, D.; Miyato, H.; Yamashita, H.; Hidemura, A.; Kaisaki, S.; Nagawa, H. Phase I pharmacokinetic study of weekly intravenous and intraperitoneal paclitaxel combined with S-1 for advanced gastric cancer. Oncology 2009, 76, 311–314. [Google Scholar] [CrossRef]
- Ishigami, H.; Kitayama, J.; Kaisaki, S.; Hidemura, A.; Kato, M.; Otani, K.; Kamei, T.; Soma, D.; Miyato, H.; Yamashita, H.; et al. Phase II study of weekly intravenous and intraperitoneal paclitaxel combined with S-1 for advanced gastric cancer with peritoneal metastasis. Ann. Oncol. 2010, 21, 67–70. [Google Scholar] [CrossRef]
- Yamaguchi, H.; Kitayama, J.; Ishigami, H.; Emoto, S.; Yamashita, H.; Watanabe, T. A phase 2 trial of intravenous and intraperitoneal paclitaxel combined with S-1 for treatment of gastric cancer with macroscopic peritoneal metastasis. Cancer 2013, 119, 3354–3358. [Google Scholar] [CrossRef]
- Aizawa, M.; Ishigami, H.; Yabusaki, H.; Nashimoto, A.; Imamoto, H.; Imano, M.; Yamashita, H.; Kishi, K.; Kodera, Y.; Uenosono, Y.; et al. Phase II study of intraperitoneal paclitaxel plus S-1/paclitaxel for gastric cancer with positive peritoneal cytology: CY-PHOENIX trial. J. Clin. Oncol. 2017, 35, 96. [Google Scholar] [CrossRef]
- Ishigami, H.; Fujiwara, Y.; Fukushima, R.; Nashimoto, A.; Yabusaki, H.; Imano, M.; Imamoto, H.; Kodera, Y.; Uenosono, Y.; Amagai, K.; et al. Phase III Trial Comparing Intraperitoneal and Intravenous Paclitaxel Plus S-1 Versus Cisplatin Plus S-1 in Patients With Gastric Cancer With Peritoneal Metastasis: PHOENIX-GC Trial. J. Clin. Oncol. 2018, 36, 1922–1929. [Google Scholar] [CrossRef] [PubMed]
- Ishigami, H.; Kaisaki, S.; Yamaguchi, H.; Yamashita, H.; Emoto, S.; Kitayama, J. Phase I study of weekly intraperitoneal paclitaxel combined with S-1 and oxaliplatin for gastric cancer with peritoneal metastasis. J. Clin. Oncol. 2012, 30, 146. [Google Scholar] [CrossRef]
- Fujiwara, Y.; Ishigami, H.; Miwa, H.; Tanaka, T.; Kodera, Y.; Imamoto, H.; Imano, M.; Fukushima, R.; Hidemura, A.; Ueda, S.; et al. Phase II study of intraperitoneal paclitaxel plus S-1/oxaliplatin for gastric cancer with peritoneal metastasis: SOX+IP PTX trial. J. Clin. Oncol. 2016, 34, 4040. [Google Scholar] [CrossRef]
- Kitayama, J.; Ishigami, H.; Yamaguchi, H.; Emoto, S.; Watanabe, T. Intraperitoneal Paclitaxel is useful as adjuvant chemotherapy for advanced gastric cancer with serosal exposure. Case Rep. Oncol. 2014, 7, 58–64. [Google Scholar] [CrossRef]
- Ito, S.; Imano, M.; Uenosono, Y.; Arigami, T.; Yabusaki, H.; Hirono, Y.; Ueda, S.; Matsumura, T.; Fukushima, R.; Takeno, A.; et al. A phase II study of perioperative intraperitoneal paclitaxel plus S-1/paclitaxel for curatively resectable gastric cancer with serosal invasion: The GAPS study. J. Clin. Oncol. 2018, 36, 4033. [Google Scholar] [CrossRef]
- Takahashi, N.; Kanda, M.; Yoshikawa, T.; Takiguchi, N.; Fujitani, K.; Miyamoto, K.; Ito, Y.; Takayama, O.; Imano, M.; Mitsumori, N.; et al. A randomized phase II multicenter trial to explore efficacy of weekly intraperitoneal in comparison with intravenous paclitaxel administered immediately after gastrectomy to the patients with high risk of peritoneal recurrence: Final results of the INPACT trial. Gastric Cancer 2018, 21, 1014–1023. [Google Scholar] [CrossRef] [Green Version]
- Ishigami, H.; Yamaguchi, H.; Yamashita, H.; Asakage, M.; Kitayama, J. Surgery after intraperitoneal and systemic chemotherapy for gastric cancer with peritoneal metastasis or positive peritoneal cytology findings. Gastric Cancer 2017, 20, 128–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oba, K.; Paoletti, X.; Alberts, S.; Bang, Y.J.; Benedetti, J.; Bleiberg, H.; Catalano, P.; Lordick, F.; Michiels, S.; Morita, S.; et al. Disease-free survival as a surrogate for overall survival in adjuvant trials of gastric cancer: A meta-analysis. J. Natl. Cancer Inst. 2013, 105, 1600–1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Japanese Gastric Cancer, A. Japanese Classification of Gastric Carcinoma—2nd English Edition. Gastric Cancer 1998, 1, 10–24. [Google Scholar] [CrossRef] [Green Version]
- Lakatos, E. Sample sizes based on the log-rank statistic in complex clinical trials. Biometrics 1988, 44, 229–241. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
Inclusion criteria
|
Exclusion criteria
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishigami, H.; Tsuji, Y.; Shinohara, H.; Kodera, Y.; Kanda, M.; Yabusaki, H.; Ito, S.; Imano, M.; Yamashita, H.; Hidemura, A.; et al. Intraperitoneal Chemotherapy as Adjuvant or Perioperative Chemotherapy for Patients with Type 4 Scirrhous Gastric Cancer: PHOENIX-GC2 Trial. J. Clin. Med. 2021, 10, 5666. https://doi.org/10.3390/jcm10235666
Ishigami H, Tsuji Y, Shinohara H, Kodera Y, Kanda M, Yabusaki H, Ito S, Imano M, Yamashita H, Hidemura A, et al. Intraperitoneal Chemotherapy as Adjuvant or Perioperative Chemotherapy for Patients with Type 4 Scirrhous Gastric Cancer: PHOENIX-GC2 Trial. Journal of Clinical Medicine. 2021; 10(23):5666. https://doi.org/10.3390/jcm10235666
Chicago/Turabian StyleIshigami, Hironori, Yasushi Tsuji, Hisashi Shinohara, Yasuhiro Kodera, Mitsuro Kanda, Hiroshi Yabusaki, Seiji Ito, Motohiro Imano, Hiroharu Yamashita, Akio Hidemura, and et al. 2021. "Intraperitoneal Chemotherapy as Adjuvant or Perioperative Chemotherapy for Patients with Type 4 Scirrhous Gastric Cancer: PHOENIX-GC2 Trial" Journal of Clinical Medicine 10, no. 23: 5666. https://doi.org/10.3390/jcm10235666
APA StyleIshigami, H., Tsuji, Y., Shinohara, H., Kodera, Y., Kanda, M., Yabusaki, H., Ito, S., Imano, M., Yamashita, H., Hidemura, A., Yamaguchi, H., Fukagawa, T., Oba, K., Kitayama, J., & Seto, Y. (2021). Intraperitoneal Chemotherapy as Adjuvant or Perioperative Chemotherapy for Patients with Type 4 Scirrhous Gastric Cancer: PHOENIX-GC2 Trial. Journal of Clinical Medicine, 10(23), 5666. https://doi.org/10.3390/jcm10235666