
Specific versus Non-Specific Exercises for Chronic Neck or Shoulder Pain: A Systematic Review

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction and Analysis
2.4. Quality Assessment and Data Synthesis
3. Results
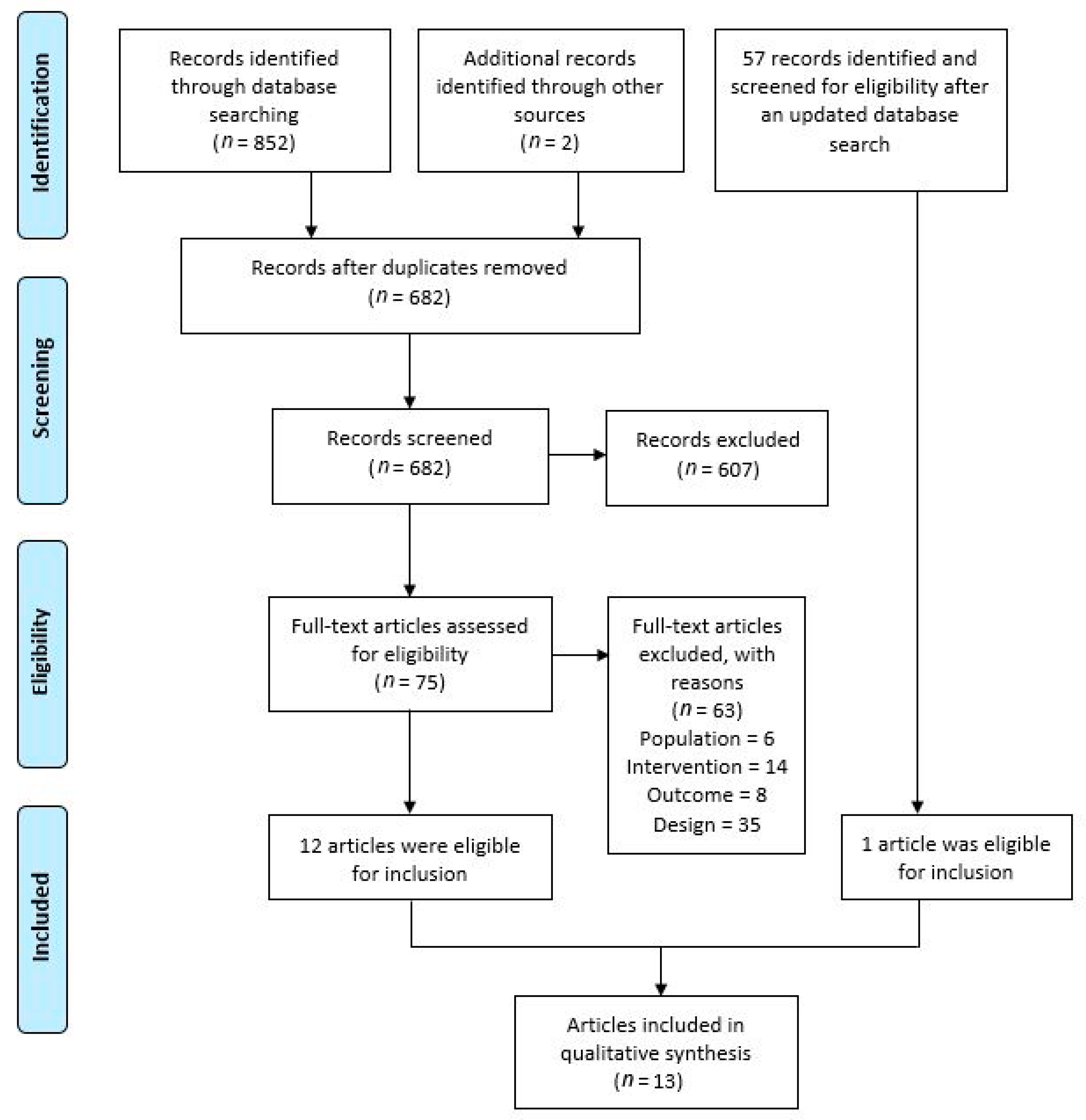
3.1. Search Results
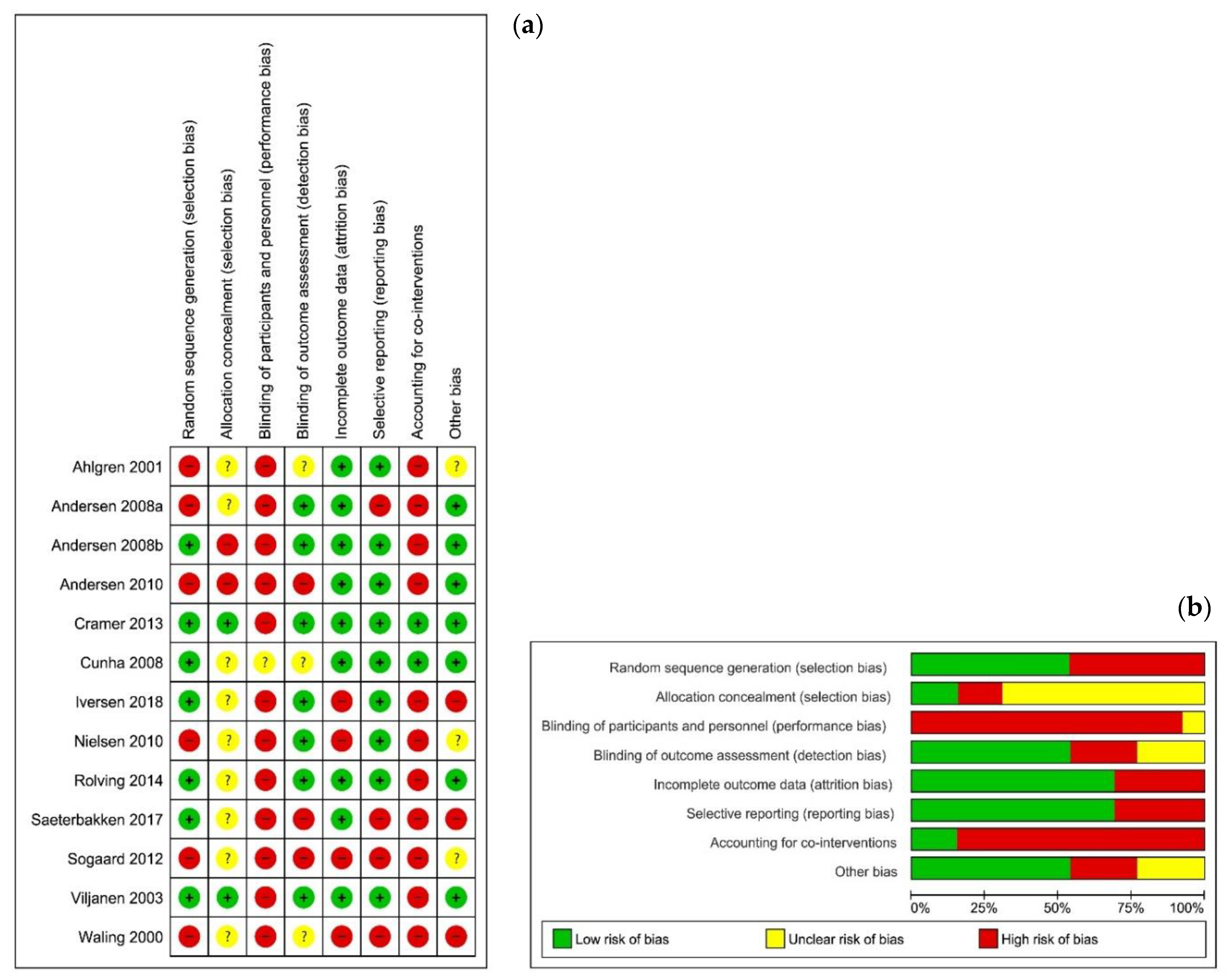
3.2. Risk of Bias and Quality of Evidence
3.3. Study Characteristics
3.4. Data Synthesis
3.4.1. Specific Strength vs. Non-Specific Aerobic Exercises
- Acute effects
- Short-term effects
- Long-term effects
3.4.2. Specific Strength vs. Body Mind Exercises
- Short-term effects
- Long-term effects
3.4.3. Specific Stretch vs. General Stretch Exercises
- Short and long-term effects
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hakala, P.; Rimpelä, A.; Salminen, J.J.; Virtanen, S.M.; Rimpelä, M. Back, Neck, and Shoulder Pain in Finnish Adolescents: National Cross Sectional Surveys. BMJ 2002, 325, 743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ihlebaek, C.; Brage, S.; Eriksen, H.R. Health Complaints and Sickness Absence in Norway, 1996–2003. Occup. Med. Oxf. Engl. 2007, 57, 43–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrari, R.; Russell, A.S. Regional Musculoskeletal Conditions: Neck Pain. Best Pract. Res. Clin. Rheumatol. 2003, 17, 57–70. [Google Scholar] [CrossRef]
- Urwin, M.; Symmons, D.; Allison, T.; Brammah, T.; Busby, H.; Roxby, M.; Simmons, A.; Williams, G. Estimating the Burden of Musculoskeletal Disorders in the Community: The Comparative Prevalence of Symptoms at Different Anatomical Sites, and the Relation to Social Deprivation. Ann. Rheum. Dis. 1998, 57, 649–655. [Google Scholar] [CrossRef] [PubMed]
- van der Windt, D.A.; Koes, B.W.; de Jong, B.A.; Bouter, L.M. Shoulder Disorders in General Practice: Incidence, Patient Characteristics, and Management. Ann. Rheum. Dis. 1995, 54, 959–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winters, J.C.; Sobel, J.S.; Groenier, K.H.; Arendzen, J.H.; Meyboom-de Jong, B. The Long-Term Course of Shoulder Complaints: A Prospective Study in General Practice. Rheumatol. Oxf. Engl. 1999, 38, 160–163. [Google Scholar] [CrossRef] [Green Version]
- Linsell, L.; Dawson, J.; Zondervan, K.; Rose, P.; Randall, T.; Fitzpatrick, R.; Carr, A. Prevalence and Incidence of Adults Consulting for Shoulder Conditions in UK Primary Care; Patterns of Diagnosis and Referral. Rheumatol. Oxf. Engl. 2006, 45, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Gross, A.R.; Paquin, J.P.; Dupont, G.; Blanchette, S.; Lalonde, P.; Cristie, T.; Graham, N.; Kay, T.M.; Burnie, S.J.; Gelley, G.; et al. Exercises for Mechanical Neck Disorders: A Cochrane Review Update. Man. Ther. 2016, 24, 25–45. [Google Scholar] [CrossRef]
- Teasell, R.W.; McClure, J.A.; Walton, D.; Pretty, J.; Salter, K.; Meyer, M.; Sequeira, K.; Death, B. A Research Synthesis of Therapeutic Interventions for Whiplash-Associated Disorder (WAD): Part 4-Noninvasive Interventions for Chronic WAD. Pain Res. Manag. 2010, 15, 313–322. [Google Scholar] [CrossRef]
- Childs, J.D.; Cleland, J.A.; Elliott, J.M.; Teyhen, D.S.; Wainner, R.S.; Whitman, J.M.; Sopky, B.J.; Godges, J.J.; Flynn, T.W. American Physical Therapy Association Neck Pain: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health from the Orthopedic Section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2008, 38, A1–A34. [Google Scholar] [CrossRef] [Green Version]
- Stewart, M.J.; Maher, C.G.; Refshauge, K.M.; Herbert, R.D.; Bogduk, N.; Nicholas, M. Randomized Controlled Trial of Exercise for Chronic Whiplash-Associated Disorders. Pain 2007, 128, 59–68. [Google Scholar] [CrossRef]
- Littlewood, C.; Bateman, M.; Brown, K.; Bury, J.; Mawson, S.; May, S.; Walters, S.J. A Self-Managed Single Exercise Programme versus Usual Physiotherapy Treatment for Rotator Cuff Tendinopathy: A Randomised Controlled Trial (the SELF Study). Clin. Rehabil. 2016, 30, 686–696. [Google Scholar] [CrossRef] [Green Version]
- Lannersten, L.; Kosek, E. Dysfunction of Endogenous Pain Inhibition during Exercise with Painful Muscles in Patients with Shoulder Myalgia and Fibromyalgia. Pain 2010, 151, 77–86. [Google Scholar] [CrossRef]
- Kroll, H.R. Exercise Therapy for Chronic Pain. Phys. Med. Rehabil. Clin. N. Am. 2015, 26, 263–281. [Google Scholar] [CrossRef]
- Naugle, K.M.; Fillingim, R.B.; Riley, J.L. A Meta-Analytic Review of the Hypoalgesic Effects of Exercise. J. Pain Off. J. Am. Pain Soc. 2012, 13, 1139–1150. [Google Scholar] [CrossRef] [Green Version]
- Nijs, J.; Kosek, E.; Van Oosterwijck, J.; Meeus, M. Dysfunctional Endogenous Analgesia during Exercise in Patients with Chronic Pain: To Exercise or Not to Exercise? Pain Physician 2012, 15, ES205–ES213. [Google Scholar] [CrossRef] [PubMed]
- Meeus, M.; Nijs, J.; Van Wilgen, P.; Noten, S.; Goubert, D.; Huijnen, I. Moving on to Movement in Patients with Chronic Joint Pain. Pain 2016, 1, 23–35. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Coghlan, J.A.; Buchbinder, R.; Green, S.; Johnston, R.V.; Bell, S.N. Surgery for Rotator Cuff Disease. Cochrane Database Syst. Rev. 2008, 1, CD005619. [Google Scholar] [CrossRef] [PubMed]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE Guidelines: 3. Rating the Quality of Evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Iversen, V.M.; Vasseljen, O.; Mork, P.J.; Fimland, M.S. Resistance Training vs General Physical Exercise in Multidisciplinary Rehabilitation of Chronic Neck Pain: A Randomized Controlled Trial. J. Rehabil. Med. 2018, 50, 743–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeterbakken, A.H.; Nordengen, S.; Andersen, V.; Fimland, M.S. Nordic Walking and Specific Strength Training for Neck- and Shoulder Pain in Office Workers: A Pilot-Study. Eur. J. Phys. Rehabil. Med. 2017, 53, 928–935. [Google Scholar] [CrossRef] [PubMed]
- Rolving, N.; Christiansen, D.H.; Andersen, L.L.; Skotte, J.; Ylinen, J.; Jensen, O.K.; Nielsen, C.V.; Jensen, C. Effect of Strength Training in Addition to General Exercise in the Rehabilitation of Patients with Non-Specific Neck Pain. A Randomized Clinical Trial. Eur. J. Phys. Rehabil. Med. 2014, 50, 617–626. [Google Scholar]
- Søgaard, K.; Blangsted, A.K.; Nielsen, P.K.; Hansen, L.; Andersen, L.L.; Vedsted, P.; Sjøgaard, G. Changed Activation, Oxygenation, and Pain Response of Chronically Painful Muscles to Repetitive Work after Training Interventions: A Randomized Controlled Trial. Eur. J. Appl. Physiol. 2012, 112, 173–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, P.K.; Andersen, L.L.; Olsen, H.B.; Rosendal, L.; Sjøgaard, G.; Søgaard, K. Effect of Physical Training on Pain Sensitivity and Trapezius Muscle Morphology. Muscle Nerve 2010, 41, 836–844. [Google Scholar] [CrossRef]
- Andersen, L.L.; Kjaer, M.; Søgaard, K.; Hansen, L.; Kryger, A.I.; Sjøgaard, G. Effect of Two Contrasting Types of Physical Exercise on Chronic Neck Muscle Pain. Arthritis Rheum. 2008, 59, 84–91. [Google Scholar] [CrossRef]
- Cunha, A.C.V.; Burke, T.N.; França, F.J.R.; Marques, A.P. Effect of Global Posture Reeducation and of Static Stretching on Pain, Range of Motion, and Quality of Life in Women with Chronic Neck Pain: A Randomized Clinical Trial. Clin. Sao Paulo Braz. 2008, 63, 763–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahlgren, C.; Waling, K.; Kadi, F.; Djupsjöbacka, M.; Thornell, L.E.; Sundelin, G. Effects on Physical Performance and Pain from Three Dynamic Training Programs for Women with Work-Related Trapezius Myalgia. J. Rehabil. Med. 2001, 33, 162–169. [Google Scholar] [CrossRef]
- Waling, K.; Sundelin, G.; Ahlgren, C.; Järvholm, B. Perceived Pain before and after Three Exercise Programs--a Controlled Clinical Trial of Women with Work-Related Trapezius Myalgia. Pain 2000, 85, 201–207. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Hohmann, C.; Lüdtke, R.; Haller, H.; Michalsen, A.; Langhorst, J.; Dobos, G. Randomized-Controlled Trial Comparing Yoga and Home-Based Exercise for Chronic Neck Pain. Clin. J. Pain 2013, 29, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Viljanen, M.; Malmivaara, A.; Uitti, J.; Rinne, M.; Palmroos, P.; Laippala, P. Effectiveness of Dynamic Muscle Training, Relaxation Training, or Ordinary Activity for Chronic Neck Pain: Randomised Controlled Trial. BMJ 2003, 327, 475. [Google Scholar] [CrossRef] [Green Version]
- Andersen, L.L.; Jørgensen, M.B.; Blangsted, A.K.; Pedersen, M.T.; Hansen, E.A.; Sjøgaard, G. A Randomized Controlled Intervention Trial to Relieve and Prevent Neck/Shoulder Pain. Med. Sci. Sports Exerc. 2008, 40, 983–990. [Google Scholar] [CrossRef]
- Andersen, L.L.; Christensen, K.B.; Holtermann, A.; Poulsen, O.M.; Sjøgaard, G.; Pedersen, M.T.; Hansen, E.A. Effect of Physical Exercise Interventions on Musculoskeletal Pain in All Body Regions among Office Workers: A One-Year Randomized Controlled Trial. Man. Ther. 2010, 15, 100–104. [Google Scholar] [CrossRef]
- Review Manager (RevMan) The Cochrane Collaboration; The Nordic Cochrane Centre: Copenhagen, Denmark, 2014.
- Booth, J.; Moseley, G.L.; Schiltenwolf, M.; Cashin, A.; Davies, M.; Hübscher, M. Exercise for Chronic Musculoskeletal Pain: A Biopsychosocial Approach. Musculoskelet. Care 2017, 15, 413–421. [Google Scholar] [CrossRef]
- Sluka, K.A.; Frey-Law, L.; Hoeger Bement, M. Exercise-Induced Pain and Analgesia? Underlying Mechanisms and Clinical Translation. Pain 2018, 159 (Suppl. S1), S91–S97. [Google Scholar] [CrossRef]
- Bialosky, J.E.; Beneciuk, J.M.; Bishop, M.D.; Coronado, R.A.; Penza, C.W.; Simon, C.B.; George, S.Z. Unraveling the Mechanisms of Manual Therapy: Modeling an Approach. J. Orthop. Sports Phys. Ther. 2018, 48, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Steiger, F.; Wirth, B.; de Bruin, E.D.; Mannion, A.F. Is a Positive Clinical Outcome after Exercise Therapy for Chronic Non-Specific Low Back Pain Contingent upon a Corresponding Improvement in the Targeted Aspect(s) of Performance? A Systematic Review. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2012, 21, 575–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lima, L.V.; Abner, T.S.S.; Sluka, K.A. Does Exercise Increase or Decrease Pain? Central Mechanisms Underlying These Two Phenomena. J. Physiol. 2017, 595, 4141–4150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falla, D.; Hodges, P.W. Individualized Exercise Interventions for Spinal Pain. Exerc. Sport Sci. Rev. 2017, 45, 105–115. [Google Scholar] [CrossRef]
- O’Riordan, C.; Clifford, A.; Van De Ven, P.; Nelson, J. Chronic Neck Pain and Exercise Interventions: Frequency, Intensity, Time, and Type Principle. Arch. Phys. Med. Rehabil. 2014, 95, 770–783. [Google Scholar] [CrossRef] [PubMed]
- Ferro Moura Franco, K.; Lenoir, D.; Dos Santos Franco, Y.R.; Jandre Reis, F.J.; Nunes Cabral, C.M.; Meeus, M. Prescription of Exercises for the Treatment of Chronic Pain along the Continuum of Nociplastic Pain: A Systematic Review with Meta-Analysis. Eur. J. Pain Lond. Engl. 2021, 25, 51–70. [Google Scholar] [CrossRef]
- Jordan, J.L.; Holden, M.A.; Mason, E.E.; Foster, N.E. Interventions to Improve Adherence to Exercise for Chronic Musculoskeletal Pain in Adults. Cochrane Database Syst. Rev. 2010, 1, CD005956. [Google Scholar] [CrossRef]
- Moseley, G.L. Do Training Diaries Affect and Reflect Adherence to Home Programs? Arthritis Rheum. 2006, 55, 662–664. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, M.L.; Ferreira, P.H.; Latimer, J.; Herbert, R.D.; Hodges, P.W.; Jennings, M.D.; Maher, C.G.; Refshauge, K.M. Comparison of General Exercise, Motor Control Exercise and Spinal Manipulative Therapy for Chronic Low Back Pain: A Randomized Trial. Pain 2007, 131, 31–37. [Google Scholar] [CrossRef]
- Holmgren, T.; Hallgren, H.B.; Öberg, B.; Adolfsson, L.; Johansson, K. Effect of Specific Exercise Strategy on Need for Surgery in Patients with Subacromial Impingement Syndrome: Randomised Controlled Study. BMJ 2012, 344, e787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Descarreaux, M.; Normand, M.C.; Laurencelle, L.; Dugas, C. Evaluation of a Specific Home Exercise Program for Low Back Pain. J. Manip. Physiol. Ther. 2002, 25, 497–503. [Google Scholar] [CrossRef]
- Marshall, P.W.; Murphy, B.A. Muscle Activation Changes after Exercise Rehabilitation for Chronic Low Back Pain. Arch. Phys. Med. Rehabil. 2008, 89, 1305–1313. [Google Scholar] [CrossRef]
- Hurwitz, E.L.; Morgenstern, H.; Chiao, C. Effects of Recreational Physical Activity and Back Exercises on Low Back Pain and Psychological Distress: Findings from the UCLA Low Back Pain Study. Am. J. Public Health 2005, 95, 1817–1824. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Keywords | |
|---|---|
| Group 1 (Population) | “Arthralgia”(MeSH) OR “Bursitis”(MeSH) OR “Cervical vertebrae”(MeSH) OR “Chronic pain”(MeSH) OR “Hernia”(MeSH) OR “Intervertebral Disc Displacement”(MeSH) OR “Musculoskeletal System”(MeSH) OR “Myalgia”(MeSH) OR “Myofascial Pain Syndromes”(MeSH) OR “Neck”(MeSH) OR “Neck Pain”(MeSH) OR “Osteoarthritis”(MeSH) OR “Pain, intractable”(MeSH) OR “Rotator cuff”(MeSH) OR “Shoulder Impingement Syndrome”(MeSH) OR “Shoulder Pain”(MeSH) OR “Shoulder”(MeSH) OR “Tendinopathy”(MeSH) OR “Whiplash Injuries”(MeSH) OR (Chronic pain OR Intractable pain OR Joint Pain OR Muscle Pain OR Musculoskeletal pain OR Myalgia OR Myofascial pain OR Osteoarthritis OR Persistent pain OR Severe pain OR Tendinopathy) AND (Neck OR Shoulder OR Cervical OR Adhesive capsulitis OR Frozen shoulder OR Impingement OR Rotator cuff OR Spinal disc herniation OR Spinal pain OR Whiplash) |
| Group 2 (Intervention) | “Exercise”(MeSH) OR “Exercise Therapy”(MeSH) OR “Cervical Vertebrae”(MeSH) OR “Functional Laterality”(MeSH) OR “Isometric Contraction”(MeSH) OR “Isotonic Contraction”(MeSH) OR “Muscle Strength”(MeSH) OR “Muscle Stretching Exercises”(MeSH) OR “Neck”(MeSH) OR “Plyometric Exercise”(MeSH) OR “Proprioception”(MeSH) OR “Resistance Training”(MeSH) OR “Shoulder”(MeSH) OR “Visual Motor Coordination”(MeSH) OR “Weight Lifting”(MeSH) OR “Weight-Bearing Exercise Program”(MeSH) OR Exercise AND (Shoulder OR Cervical OR Neck OR Abduction OR Adduction OR Balls OR Bands OR Concentric OR Coordination OR Dynamic OR Eccentric OR Extension OR External Rotation OR Flexibility OR Flexion OR Free weights OR Internal rotation OR Isometric OR Isotonic OR Kettlebell OR Motor control OR Plyometric OR Proprioception OR Red cord OR Resistance training OR Resisted OR Static OR Strength OR Strength training equipment OR Stretching OR Thera-band OR Weight-bearing exercise program OR Weights) |
| Group 3 (Comparison) | “Exercise”(MeSH) OR “Exercise Movement Techniques”(MeSH) OR “Exercise Therapy”(MeSH) OR “Bicycling”(MeSH) OR “Dancing”(MeSH) OR “Hydrotherapy”(MeSH) OR “Jogging”(MeSH) OR “Muscle Stretching Exercises”(MeSH) OR “Physical Fitness”(MeSH) OR “Physical Endurance”(MeSH) OR “Resistance Training”(MeSH) OR “Running”(MeSH) OR “Swimming”(MeSH) OR “Walking”(MeSH) OR “Yoga”(MeSH) OR Exercise AND (Non-specific exercise OR Non-specific training OR Aspecific OR Activity program OR Aerobic OR Alexander technique OR Aquatic exercise OR Bicycling OR Cycling OR Dancing OR Endurance OR Fitness OR General exercise OR Generic exercise OR Hydrotherapy OR Jogging OR Physical activity OR Resistance training OR Rowing OR Running OR Stretching OR Swimming OR Tai chi OR Training OR Walking OR Yoga) |
| Group 4 (Outcome) | “Pain”(MeSH) OR “Pain Measurement”(MeSH) OR “Analgesia”(MeSH) OR “Central Nervous System Sensitization”(MeSH) OR “Hyperalgesia”(MeSH) OR “Hypersensitivity”(MeSH) OR “Nociceptors”(MeSH) OR “Pain Management”(MeSH) OR “Pain Threshold”(MeSH) OR “Pain Perception”(MeSH) OR “Pain, Intractable”(MeSH) OR “Pain, Referred”(MeSH) OR “Somatosensory Disorders”(MeSH) OR “Visual Analogue Scale”(MeSH) OR Pain OR Pain measurement OR Algometry OR Analgesia OR Central nervous system sensitization OR Centrally mediated pain modulation OR Conditioned pain modulation OR Endogenous pain inhibition OR Endogenous pain-inhibitory mechanisms OR Exercise-induced hgperalgesia OR Hyperalgesia OR Hypersensitivity OR Hypoalgesia OR McGill OR Nociceptors OR Pain control OR Pain threshold OR Pain-relief OR Persistent pain OR Pressure pain thresholds OR Quantitative sensory testing OR Referred pain OR Sensitivity OR Somatosensory disorders OR Temporal summation OR Visual analogue scale OR Wind-up effect |
| Group 5 (Study design) | “Controlled Clinical Trials”(MeSH) OR Controlled clinical trials |
| 1-. SPECIFIC STRENGTH VS. NON-SPECIFIC AEROBIC | |||||
| 1.1. ACUTE EFFECTS | |||||
| Study | VAS/NRS | Risk of bias | GRADE | ||
| SI | NSI | REF | |||
| Andersen et al. [26] | ↑ VAS in untrained patients = VAS in trained patients | ↓ VAS | ø |  | ⊕⊖⊖⊖ |
| 1.2. SHORT-TERM EFFECTS | |||||
| Andersen et al. [32] | = pain (0–9 scale) in neck and shoulder pain patients | = pain (0–9 scale) in neck and shoulder pain patients |  | ⊕⊕⊖⊖ | |
| Andersen et al. [26] | VAS in general ↓ VAS at worst ↓ | VAS in general = VAS at worst = | |||
| Andersen et al. [33] | ↓ pain (0–9 scale) > than REF | ↓ pain (0–9 scale) | |||
| Iversen et al. [21] | NRS = | ø | |||
| Rolving et al. [23] | ↓ NRS | ø | |||
| Saeterbakken et al. [22] | VAS intensity ↓ | VAS intensity = | |||
| Søgaard et al. [24] | VAS at rest ↓ > than NSI and REF VAS during repetitive and stress tasks = | VAS at rest = VAS during repetitive tasks ↓ > than SI and REF | VAS at rest and during repetitive and stress tasks = | ||
| 1.3. LONG-TERM EFFECTS | |||||
| Andersen et al. [26] | VAS in general ↓ VAS at worst ↓ and keeps on, from short-term effects, stable and < than NSI and REF (therapy effects remained) | VAS in general = VAS at worst = ø |  | ⊕⊖⊖⊖ | |
| Saeterbakken et al. [22] | VAS intensity ↓ | VAS intensity = | |||
| 2-. SPECIFIC STRENGTH VS. BODY-MIND | |||||
| 2.1.ACUTE EFFECTS: no study | |||||
| 2.2.SHORT-TERM EFFECTS | |||||
| Ahlgren et al. [28] | Overall VAS ↓ ↓ VAS at worst > than REF | Overall VAS ↓ | Overall VAS = |  | ⊕⊕⊕⊖ |
| Cramer et al. [30] | VAS at motion ↓ VAS intensity = | VAS at motion ↓ VAS intensity ↓ > than SI | ø | ||
| Viljanen et al. [31] | = VAS | ||||
| Waling et al. [29] | Pain at present = Pain in general = VAS at worst ↓ > than REF | Overall pain = | Overall pain = | ||
| VAS at present and VAS at worst “exercisers” ↓ > than REF | |||||
| 2.3.LONG -TERM EFFECTS | |||||
| Viljanen et al. [31] | = VAS |  | ⊕⊖⊖⊖ | ||
| 3-. SPECIFIC STRETCH VS. GENERAL STRETCH | |||||
| 3.1.ACUTE EFFECTS: no study | |||||
| 3.2.SHORT-TERM EFFECTS | |||||
| Cunha et al. [27] | ↓ VAS | ø |  | ⊕⊖⊖⊖ | |
| 3.3. LONG -TERM EFFECTS | |||||
| Cunha et al. [27] | ↓ VAS (from baseline to 6 w follow-up post-intervention) | ø |  | ⊕⊖⊖⊖ | |
| Reference | Characteristics of Participants | Specific Intervention (SI) | Non-Specific Intervention (NSI) + Reference Intervention (REF) | Outcome Measures / Follow-Up Period | Main Results |
|---|---|---|---|---|---|
| Andersen et al. [32] | Office workers with neck or shoulder pain > 3/9 and ≥3 m Neck: n = 182, ♀ (44 ± 0.9 y); ♂ (49 ± 1.4 y) Shoulder: n = 94, ♀ (44 ± 1.1 y); ♂ (48 ± 1.4 y) SI group Neck: n = 61 Shoulder: n = 41 NSI group Neck: n = 59 Shoulder: n = 46 REF group Neck: n = 62 Shoulder: n = 37 ITT analysis | Specific neck-shoulder dynamic and static strengthening ex with dumbbells and inelastic strap - 20′ × 3/w for 1 y - 2/3 supervised - during working hours - Load ↑ when they performed > 15 reps/ex - Last 15″: high-speed dynamic power ex (kayaking or ergometer rowing) | General fitness training - 1 h/w during working hours for 1 y - Filled in a “contract”, writing the ways to include + physical act in their lives - Swimming, fitness clubs, all-round strength and aerobic fitness lessons (1–4 visits/m), walking group sessions (step counters), group sessions of Nordic walking, aerobic fitness, etc. REF group - No physical act - Workplace ergonomics, stress management, etc. - =supervision as SI and NSI | Pain: - Pain intensity during last 3 m (0–9 scale) ̴ baseline ̴ post-intervention (1 y) | Short-term effects (post-intervention): PAIN INTENSITY: - = SI, NSI and REF |
| Andersen et al. [33] | Same characteristics as Andersen et al. [32] n (at baseline) = 616 397 ♀ (44.6 y); 219 ♂ (45.7 y) (67 excluded/withdrew = 549) SI group n = 180 NSI group n = 187 REF group n = 182 ITT analysis | Pain: - Pain intensity during last 3 m (0–9 scale) - Pain regions (n = 0–11), with a VAS ≥ 3/9 ̴ baseline ̴ post-intervention (1 y) | Short-term effects (post-intervention): PAIN INTENSITY: - ↓ SI, NSI and REF - ΔSI and ΔNSI > ΔREF Pain regions (n): - ↓ SI and NSI; =REF | ||
| Andersen et al. [26] | ♀ office workers (30–60 y), assembly line or office workers, with CNSP (≥30 d in the last y), reporting pain ≥ 1 episode/w + pain intensities at T0 ≥ 3 (0–9 scale) + diagnosed as trapezius myalgia. n = 48 ♀ (end 43 ♀) 44 ± 8 y SI group n = 18 ♀. 44 ± 8 y NSI group n = 16 ♀. 49 ± 7 y REF group n = 14 ♀ (end 9 ♀) 48 ± 11 y | 5 neck–shoulder specific strengthening ex with dumbbells - 20′ × 3/w supervised for 10 w - 3 sets (25–35″)/ex - High intensity (consecutive concentric and eccentric muscle contractions without pause or breaks) - Load progressively ↑ 12 → 8 RM; (~70 → 80% max intensity) | Bicycle ergometer training - 20′ × 3/w supervised for 10 w - High intensity - Intensity progressively ↑ 50 → 70% (Vo2max) REF group - 1 h/w for 10 w - No physical act - Health counseling on group + on individual level (workplace ergonomics, diet, relaxation, ...) - = supervision as SI and NSI | Pain (diary report): - General pain (VAS1) - Pain at worst (VAS2) - Pain immediately before the session (VAS3) - Pain immediately after the session (VAS4) ̴ baseline ̴ half of training period ̴ post-intervention (10 w) ̴ 10 w follow-up | Acute effects after 1 ex session • 1st half of training period: - VAS4-VAS3: ↑ SI; ↓ NSI. Effects lasted for 2 h - ΔNSI > ΔSI and REF • 2nd half of training period: VAS4-VAS3: - ↓ NSI; = SI. Effects lasted for 2 h - ΔNSI > ΔSI and REF Short-term effects (post-intervention): VAS1,2: - ↓ SI; = NSI and REF - ΔSI > ΔNSI and REF Long-term effects (follow-up): VAS1,2: - ↓ SI; = NSI and REF - ΔSI > ΔNSI and REF |
| Nielsen et al. [25] | PPTs: - Painful trapezius (PPT1) - Non-painful tibialis anterior (PPT2) ̴ baseline ̴ post-intervention (10 w) | Short-term effects (post-intervention): PPT1: - ↑ SI; = NSI and REF - Δmyalgia < Δcontrols PPT2: - ↑ SI and NSI; =REF - Δmyalgia < Δcontrols | |||
| Søgaard et al. [24] | ♀ performing monotonous & repetitive work tasks + trapezius myalgia (30–60 y) n = 47 ♀ (end 39 ♀) SI group n = 16 ♀ 44.6 ± 8.5 y NSI group n = 15 ♀ 45.5 ± 8.0 y REF group n = 16 ♀ (end 8 ♀) 42.5 ± 11.1 y | Pain: - At rest (VAS1): measured prior to the repetitive task - During repetitive task (VAS2): pegboard work (40′). VAS every 5′. Changes in VAS slope (time curve) (mm/min)- VAS after 120′ rest immediately before a stressful Stroop task (VAS3). - VAS immediately after the stressful Stroop task (VAS4) ̴ baseline (2 d before the intervention) ̴ post-intervention (10 w) | Short-term effects (post-intervention): VAS 1: - ↓ SI; = NSI and REF - ΔSI >ΔNSI = ΔREF VAS2: - ↓ NSI; = SI & REF - ΔNSI > ΔSI = ΔREF VAS3, 4: -ΔSI = ΔNSI = ΔREF | ||
| Iversen et al. [21] | Patients (16–70 y) + non-specific neck pain ≥ 3 m or ≥ 2 times ≥ 4 w in the past y and worst neck pain in last 2 w NRS ≥ 4 n = 59 (39 ♀ & 20 ♂) (end 31) SI group n = 29 (end 15) 20 ♀ & 9 ♂ 44.6 ± 8.1 y NSI group n = 30 (end 16) 19 ♀ & 11 ♂ 48.2 ± 10.6 y | MDR + 8 neck-shoulder specific strengthening ex. with elastic bands - 3 w MDR: patient education, stress management, group discussions - 9 w SI program: 3 times/w. Supervised at 1st and 3rd w - +1 session NSI - +3 group booster sessions - Yellow–gold Theraband® - Reps/ex until muscular failure - Load progressively ↑: sets/reps/band color - Diary for daily registration | MDR + General fitness training - 3 w MDR: patient education, stress management, group discussions - 9 w NSI program: 1st and 3rd w, 4 and 3 supervised sessions - Introduction to group-based and individual act (circle-training, endurance, low-intensity resistance, stretching) - + 3 group booster sessions - Diary for daily registration | Pain: - Current neck pain (NRS1) - Pain at worst last 2 w (NRS2) - Pain at worst in last 4 w (NRS3) PD: Additional pain sites (n) PPTs: tibialis anterior muscle ̴ baseline ̴ post-intervention (12 w) | Short-term effects (post-intervention): NRS, pain sites and PPTs: - = SI and NSI - ΔSI = ΔNSI |
| Rolving et al. [23] | Patients on sick leave from work (4–16 w prior to study) due to non-specific neck pain (18–60 y) n = 83 (60 ♀ & 23 ♂) (end 71) SI group n = 43 (end 34) 27 ♀ & 16 ♂ 39.6 ± 9.2 y NSI group n = 40 (end 37) 33 ♀ & 7 ♂ 39.0 ± 11.0 y ITT analysis | General fitness training and 4 specific neck–shoulder-strengthening ex. With elastic band - 15–20′ supervised training ≥ 3 times/w for 12 w - Participants instructed to be physically active ≥ 30′/d, 3–4 h/w - 3 × 5 reps/ex - Load progressively ↑/2 w - Diary for daily registration | General fitness training - Participants instructed to be physically active ≥ 30′/d, 3–4 h/w for 12 w - Minimal supervision - Diary for daily registration | Pain: - Pain intensity during last w (0–10 scale) (NRS) ̴ baseline ̴ post-intervention (12 w) | Short-term effects (post-intervention): NRS: - ↓ SI and NSI - ΔSI = ΔNSI. |
| Saeterbakken et al. [22] | ♀ office workers with neck or shoulder pain ≥ 2 and ≥ 3 m n = 34 ♀ (end 31 ♀) SI group n = 13 (end 12) 47.6 ± 11.9 y NSI group n = 10 (end 9) 41.0 ± 15.3 y REF group n = 11 (end 10) 50.3 ± 14.8 y | 5 neck-shoulder specific strengthening ex with elastic bands - 30′ supervised training 2 times/w for 10 w - ≥2 d between sessions - 3 × 12 reps (3″/rep) - 1′ pause between ex. - Loads that allowed 12 reps, ending at or near to fatigue. When 17 reps, load progressively ↑ | Nordic walking - 30′ supervised training 2 times/w for 10 w - ≥ 2 d between sessions - Moderate intensity. Progressively ↑ (Borg 6–20 scale) - Nordic walking poles: individually adjusted REF group - No physical act | Pain: - Pain intensity (last 5 days’ mean) (VAS1) ̴ baseline ̴ post-intervention (10 w) ̴ 10 w follow-up | Short-term effects (post-intervention): VAS 1: - ↓ SI and NSI; = REF - ΔSI = ΔNSI = ΔREF Long-term effects (follow-up): VAS1: - ↓ SI? (p = 0.058) and NSI; =REF - ΔSI = ΔNSI = ΔREF |
| Reference | Characteristics of Participants | Specific Intervention (SI) | Non-Specific Intervention (NSI) + Reference Intervention (REF) | Outcome Measures / Follow-Up Period | Main Results |
|---|---|---|---|---|---|
| Ahlgren et al. [28] | ♀ < 45 y with trapezius myalgia for ≥1 y + sick leave ≤ 1 m last y n = 136 ♀ (−34 excluded/withdrew = 102 ♀) 38.2 y SI1 group n = 29 ♀ 38.0 ± 6.0 y SI2 group n = 28 ♀ 38.5 ± 5.6 y NSI group n = 25 ♀ 37.6 ± 6.1 y REF group n = 20 ♀ 38.9 ± 5.4 y | - 3 × 1 h/w supervised for 10 w - 15′ general warm-up - Last 10′: stretching SI1 group: 4 neck-shoulder specific strengthening concentric ex with air machines - Load individualized to 2 × 12 RM - Load ↑ when 3 sets = comfortable SI2 group: endurance training with arm ergometer alternated with specific arm ex. with rubber expanders - 4 × 3′ arm ergometer (110–120 bpm) - Specific arm ex: 3′ - Expanders individually loaded to allow 30–35 RM/ex/set (3 sets) | Body awareness - 3 × 1 h/w supervised for 10 w - 15′ general warm-up - Muscular tension awareness and relaxation - Attention focused on balance, posture and breathing REF group - 1 × 2 h/w supervised for 10 w - No physical act. Learn and discuss stress management | Pain: - Pain at present (VAS1) - Pain in general (VAS2) - Pain at worst (VAS3) ̴ baseline ̴ post-intervention (10 w) PPTs: 6 trigger points in the 3 portions of the trapezius (TP) muscle (TP2, TP4, TP5), 2 sides (R, L) PD: Pain distribution and pain character (% total body area) | Short-term effects (post-intervention): VAS1: - ↓ SI1, SI2 and NSI; = REFVAS2: - ↓ SI1, SI2 and NSI; = REFVAS3: - ↓ SI1, SI2 and NSI; = REF- ΔSI1 & ΔSI2 > ΔREF |
| Waling et al. [29] | Short-term effects (post-intervention): VAS 1: - ↓ SI1, SI2, NSI; = REF - ΔSI1 = ΔSI2 = ΔNSI = ΔREF - Δ“exercisers” (SI1 + SI2 + NSI) > ΔREF VAS 2: - ↓ SI1, SI2, NSI; = REF - ΔSI1 = Δ SI2 = ΔNSI = ΔREF VAS3: - ↓ SI1, SI2, NSI; = REF - ΔSI1 and ΔSI2 > ΔREF - Δ“exercisers” (SI1 + SI2 + NSI) > ΔREF PPTs: - ↑SI2 (in 2 trigger points); = SI1, NSI and REF - TP2L: ΔSI1 < ΔSI2 ΔSI2 > ΔREF - TP5L: ΔSI2 > ΔREF ΔNSI > ΔREF - TP2R, TP5R and TP5L: Δ“exercisers” (SI1 + SI2 + NSI) > ΔREF PD: - ΔSI1 = ΔSI2 = ΔNSI = ΔREF | ||||
| Cramer et al. [30] | Patients (18–60 y) + non-specific neck pain VAS ≥ 4 and ≥ 3 m n = 51 42 ♀ and 9 ♂ 47.8 ± 10.4 y VAS 4.5 ± 1.9 SI group n = 26 21 ♀ and 5 ♂ 49.5 ± 9.5 y NSI group n = 25 21 ♀ and 4 ♂ 46.2 ± 11.2 y | Specific neck–shoulder posture awareness, stretching and strengthening ex - 10′/d (home ex) for 9 w - Self-care manual - Sitting position - Use of a towel as an aid - Diary | Yoga - 90′ yoga session/w for 9 w: - 10–15 patients - 8–10 yoga postures/session - Last 15′ relaxation - Iyengar yoga type - 3 sitting + 3 standing postures - No previous experience in yoga - + 10′/d (home ex) - Diary | Pain: - Pain at rest (VAS1) - Pain at motion (VAS2) (after 6 reps of head flex, ext, lateral flex R/L, rotation R/L) (mean pain intensity of the 6 movements) SF36-BP (bodily pain items) PPTs: - Maximal pain site (PPT) ̴ baseline ̴ post-intervention (9 w) | Short-term effects (post-intervention): VAS1: - ↓NSI; = SI - ΔNSI > ΔSI VAS2: - ↓ SI & NSI - ΔSI = ΔNSI SF36-BP: - ↑ NSI; = SI - ΔNSI > ΔSI PPTs: - ↑ NSI; = SI - ΔNSI > ΔSI |
| Viljanen et al. [31] | ♀ office workers (30–60 y) with chronic non-specific neck pain ≥ 3 m n = 393 ♀ (end 340 ♀) SI group n = 135 ♀ (end 111 ♀) 45 ± 6.6 y NSI group n = 128 ♀ (end 110 ♀) 43 ± 7.3 y REF group n = 130 ♀ (end 119 ♀) 44 ± 7.4 y ITT analysis | Specific neck–shoulder dynamic strengthening ex with dumbbells - 3 times/w for 12 w + reinforcement training for 1 w - Supervised groups ≤ 10 people - 1–3 kg according to RM test with 7.5 kg - Intensity progressively ↑ - Stretching after each ex | Relaxation - 3 times/w for 12 w + reinforcement training for 1 w: - Supervised groups ≤ 10 people - Progressive relaxation method, autogenic training, functional relaxation and systematic desensitisation - ≠Techniques being incorporated through the 12 w REF group - Ordinary act - No supervision | Pain: - Pain intensity (VAS) ̴ Baseline ̴ post-intervention (13 w) ̴ 3 m follow-up ̴ 9 m follow-up | Short-term effects (post-intervention): VAS: - =SI, NSI and REF - ΔSI = ΔNSI = ΔREF Long-term effects (both follow-up moments): VAS: - =SI, NSI and REF - ΔSI = ΔNSI = ΔREF |
| Reference | Characteristics of Participants | Specific Intervention (SI) | Non-Specific Intervention (NSI) + Reference Intervention (REF) | Outcome Measures / Follow-Up Period | Main Results |
|---|---|---|---|---|---|
| Cunha et al. [27] | ♀ (35–60 y) with chronic neck pain lasting ≥ 3 m n = 33 ♀ (end 31 ♀) SI group n = 17 (end 16) 48.7 ± 7.3 y NSI group n = 16 (end 15) 44.4 ± 7.8 y | Static neck-shoulder stretching ex - 60′ × 2/w for 6 w - 30′ manual therapy and breathing ex + 30′ conventional auto-passive stretching - 2 × 30″/ex | Global posture reeducation stretching - 60′ × 2/w for 6 w - 30′ manual therapy and breathing ex + 30′ supervised muscle chain stretching - 2 postures: posterior and anterior chains (15′/posture) | Pain: - Pain intensity (VAS) SF36-BP (bodily pain items) ̴ baseline ̴ post-intervention (6 w) ̴ 6 w follow-up | Short-term effects (post-intervention): VAS: - ↓ SI and NSI - ΔSI = ΔNSI SF36-BP: - ↑ SI and NSI - ΔSI = ΔNSI Long-term effects (follow-up): VAS: - ↓ SI and NSI - ΔSI = ΔNSI SF36-BP: - ↑ SI and NSI - ΔSI = ΔNSI |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dueñas, L.; Aguilar-Rodríguez, M.; Voogt, L.; Lluch, E.; Struyf, F.; Mertens, M.G.C.A.M.; Meulemeester, K.D.; Meeus, M. Specific versus Non-Specific Exercises for Chronic Neck or Shoulder Pain: A Systematic Review. J. Clin. Med. 2021, 10, 5946. https://doi.org/10.3390/jcm10245946
Dueñas L, Aguilar-Rodríguez M, Voogt L, Lluch E, Struyf F, Mertens MGCAM, Meulemeester KD, Meeus M. Specific versus Non-Specific Exercises for Chronic Neck or Shoulder Pain: A Systematic Review. Journal of Clinical Medicine. 2021; 10(24):5946. https://doi.org/10.3390/jcm10245946
Chicago/Turabian StyleDueñas, Lirios, Marta Aguilar-Rodríguez, Lennard Voogt, Enrique Lluch, Filip Struyf, Michel G. C. A. M. Mertens, Kayleigh De Meulemeester, and Mira Meeus. 2021. "Specific versus Non-Specific Exercises for Chronic Neck or Shoulder Pain: A Systematic Review" Journal of Clinical Medicine 10, no. 24: 5946. https://doi.org/10.3390/jcm10245946
APA StyleDueñas, L., Aguilar-Rodríguez, M., Voogt, L., Lluch, E., Struyf, F., Mertens, M. G. C. A. M., Meulemeester, K. D., & Meeus, M. (2021). Specific versus Non-Specific Exercises for Chronic Neck or Shoulder Pain: A Systematic Review. Journal of Clinical Medicine, 10(24), 5946. https://doi.org/10.3390/jcm10245946