
Distal Radial Artery Access for Coronary and Peripheral Procedures: A Multicenter Experience

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Materials and Technique
2.2. Study Outcome, Definitions, Patient’s Selection
- (1)
- Ultrasound evidence of arterial occlusion, severe calcification, and a lumen of less than 1 mm;
- (2)
- Established cardiogenic shock;
- (3)
- Raynaud’s disease in the medical history.
- (1)
- Technical success;
- (2)
- Access site complications (determined at the end of the procedure and at 1 day);
- (3)
- The rate of crossover to another puncture site.
- (1)
- Baseline patient characteristics (age, gender, height, weight, cardiovascular risk factors);
- (2)
- Time to find the artery by Doppler USG;
- (3)
- The total number of puncture attempts;
- (4)
- Total access time, cannulation time, and puncture time (in seconds);
- (5)
- Total procedure time (including fluoroscopy time);
- (6)
- Indication for intervention, sheath size, catheter size;
- (7)
- Postoperative compression time, compression type;
- (8)
- Pain score (0–5);
- (9)
- Radiation dose, contrast amount;
- (10)
- Hospitalization time;
- (11)
- Postoperative complications (listed below);
- (12)
- Ultrasound measurement of arrtery diameters: distal radial artery in the anatomical snuffbox and proximal radial artery (2–3 cm of the styloid);
- (13)
- USG-measured radial artery peak systolic velocity (PSV) (cm/s) and distal radial PSV (cm/s) by USG.
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Ultrasonography Data
3.3. Procedural Data
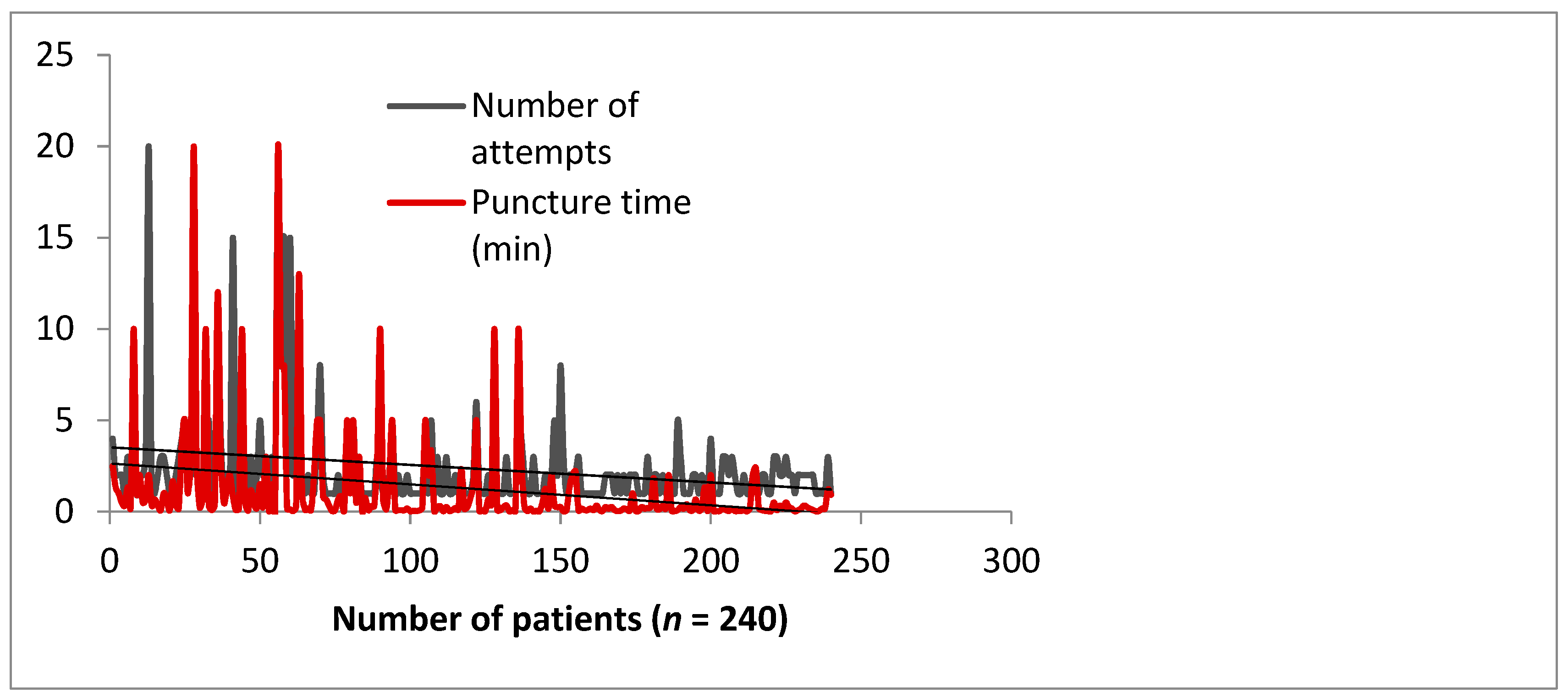
3.4. The Impact of the Learning Curve
3.5. Vascular Complications
3.6. Noncoronary Interventions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| dRA | distal radial access |
| pRA | proximal radial access |
| RA | radial artery |
| USG | ultrasonography |
| IV | intravenous |
| NTG | nitroglycerine |
| RAO | radial artery occlusion |
| PCI | percutaneous coronary intervention |
| CTO | chronic total occlusion |
| BAV | balloon aortic valvuloplasty |
| TAVI | transcatheter aortic valve implantation |
References
- Sgueglia, G.A.; Di Giorgio, A.; Gaspardone, A.; Babunashvili, A. Anatomic basis and physiological rationale of distal radial artery access for percutaneous coronary and endovascular procedures. JACC Cardiovasc. Interv. 2018, 11, 2113–2119. [Google Scholar] [CrossRef] [PubMed]
- Babunashvili, A.; Dundua, D. Recanalization and reuse of early occluded radial artery within 6 days after previous transradial diagnostic procedure. Catheter. Cardiovasc. Interv. 2011, 77, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Kiemeneij, F. Left distal transradial access in the anatomical snuffbox for coronary angiography (ldTRA) and interventions (ldTRI). EuroIntervention 2017, 13, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Davies, R.E.; Gilchrist, I.C. Back hand approach to radial access: The snuff box approach. Cardiovasc. Revasc. Med. 2018, 19, 324–326. [Google Scholar] [CrossRef] [PubMed]
- Achim, A.; Szűcsborus, T.; Sasi, V.; Nagy, F.; Jambrik, Z.; Nemes, A.; Varga, A.; Bertrand, O.F.; Ruzsa, Z. Distal radial secondary access for transcatheter aortic valve implantation: The minimalistic approach. Cardiovasc. Revasc. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- ldTRA. Twitter. Available online: https://twitter.com/hashtag/ldTRA?src=hash (accessed on 29 November 2018).
- Ruzsa, Z.; Csavajda, Á.; Nemes, B.; Deák, M.; Sótonyi, P.; Bertrand, O.F.; Merkely, B. Distal Radial Artery Access for Superficial Femoral Artery Interventions. J. Endovasc. Ther. 2021, 28, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Pirlet, C.; Ruzsa, Z.; Costerousse, O.; Nemes, B.; Merkely, B.; Poirier, P.; Bertrand, O.F. Transradial left gastric artery embolization to treat severe obesity: A pilot study. Catheter. Cardiovasc. Interv. 2019, 93, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Prasad, R.M.; Pandrangi, P.; Pandrangi, G.; Yoo, H.; Salazar, A.M.; Ukponmwan, E.; Kehdi, M.; Abela, G. Meta-Analysis Comparing Distal Radial Artery Approach Versus Traditional for Coronary Procedures. Am. J. Cardiol. 2021. [Google Scholar] [CrossRef]
- Roh, J.W.; Kim, Y.; Lee, O.H.; Im, E.; Cho, D.-K.; Choi, D.; Jeong, M.H. The learning curve of the distal radial access for coronary intervention. Sci. Rep. 2021, 11, 13217. [Google Scholar] [CrossRef] [PubMed]
- Flores, E.F. Incorporating Distal Radial Artery Access Into Clinical Practice. Diagnostic and Interventional Cardiology. 2019. Available online: https://www.dicardiology.com/article/incorporating-distal-radial-artery-access-clinical-practice (accessed on 20 February 2021).
- Moussa Pacha, H.; Alahdab, F.; Al-Khadra, Y.; Idris, A.; Rabbat, F.; Darmoch, F.; Soud, M.; Zaitoun, A.; Kaki, A.; Rao, S.V. Ultrasound-guided versus palpation-guided radial artery catheterization in adult population: A systematic review and meta-analysis of randomized controlled trials. Am. Heart J. 2018, 204, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Wang, F.; Li, Y. Ultrasound guidance for radial artery catheterization: An updated meta analysis of randomized controlled trials. PLoS ONE. 2014, 9, e111527. [Google Scholar] [CrossRef] [Green Version]
- Nikolakopoulos, I.; Patel, T.; Jefferson, B.K.; Sheikh, A.M.; Jaber, W.; Samady, H. Distal Radial Access in Chronic Total Occlusion Percutaneous Coronary Intervention: Insights From the PROGRESS-CTO Registry. J. Invasive Cardiol. 2021, 33, E717–E722. [Google Scholar] [PubMed]
- Nairoukh, Z.; Jahangir, S.; Adjepong, D.; Malik, B.H. Distal Radial Artery Access: The Future of Cardiovascular Intervention. Cureus 2020, 12, e7201. [Google Scholar] [CrossRef] [Green Version]
- Eid-Lidt, G.; Rodriguez, A.R.; Castellanos, J.J.; Pasos, J.I.F.; Lópetz, K.E.E.; Galspar, J. Distal radial artery approach to prevent radial artery occlusion trial. JACC Cardiovasc. Interv. 2021, 14, 378–385. [Google Scholar] [CrossRef]
- Mizuguchi, Y.; Izumikawa, T.; Hashimoto, S. Efficacy and safety of the distal transradial approach in coronary angiography and percutaneous coronary intervention: A Japanese multicenter experience. Cardiovasc. Interv. Ther. 2020, 35, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Aminian, A.; Sgueglia, G.A.; Wiemer, M.; Gasparini, G.L.; Kefer, J.; Ruzsa, Z.; van Leeuwen, M.A.; Vandeloo, B.; Ungureanu, C.; Kedev, S. Distal versus conventional radial access for coronary angiography and intervention: Design and rationale of DISCO RADIAL study. Am. Heart J. 2021, 244, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Hammami, R.; Zouari, F.; Ben Abdessalem, M.A.; Sassi, A.; Ellouze, T.; Bahloul, A. Distal radial approach versus conventional radial approach: A comparative study of feasibility and safety. Libyan J. Med. 2021, 16, 1830600. [Google Scholar] [CrossRef] [PubMed]
- Lee, O.H.; Kim, Y.; Son, N.H.; Roh, J.W.; Im, E.; Cho, D.K.; Choi, D. Comparison of Distal Radial, Proximal Radial, and Femoral Access in Patients with ST-Elevation Myocardial Infarction. J. Clin. Med. 2021, 10, 3438. [Google Scholar] [CrossRef] [PubMed]
- Chugh, Y.; Kanaparthy, N.S.; Piplani, S.; Chugh, S.; Shroff, A.; Vidovich, M.; Nolan, J.; Malmas, M.; Chugh, S.K. Comparison of distal radial access versus standard transradial access in patients with smaller diameter radial Arteries(The distal radial versus transradial access in small transradial ArteriesStudy: D.A.T.A—S.T.A.R study). Indian Heart J. 2021, 73, 26–34. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Demographic Features | Mean ± SD (Range)/n (%) |
|---|---|
| Age (years) | 66.4 ± 12 (25–92) |
| Gender: female/male, % (n) | 33.14% (411)/66.85% (829) |
| Height (cm) | 173 ± 8 |
| Weight (kg) | 78 ± 17 |
| Risk Factors | |
| Renal failure | 196 (15.8%) |
| Diabetes Mellitus | 463 (37.33%) |
| Hypertension | 1152 (92.9%) |
| Smoking | 311 (25.08%) |
| Family History | 255 (20.5%) |
| Dyslipidemia | 1035 (83.46%) |
| Previous MI | 295 (23.79%) |
| Previous CABG | 80 (6.45%) |
| Previous PCI | 199 (16.04%) |
| Indication for Catheterization | |
| Stable Angina Pectoris | 627 (50.56%) |
| Unstable Angina | 60 (4.83%) |
| NSTEMI | 82 (6.53%) |
| STEMI | 46 (3.7%) |
| Heart Failure | 16 (1.29%) |
| Severe Aortic Stenosis | 25 (2.01%) |
| Cardiac Arrest | 7 (0.56%) |
| Peripheral Interventions | 322 (25.72%) |
| Parameters | Mean ± SD |
|---|---|
| Radial artery diameter, mm | 2.45 ± 0.6 |
| Distal radial artery diameter, mm | 2.30 ± 0.5 |
| Radial artery PSV (cm/s) | 29.62 ± 10.5 |
| Distal radial artery PSV (cm/s) | 31.62 ± 17.2 |
| Procedural Characteristics | Values |
|---|---|
| Coronary angiography only | 272 (21.9%) |
| Coronary angiography and PCI | 966 (77.9%) |
| Right distal transradial access | 1108 (89.35%) |
| rdRA success rate | 1082 (97.65%) |
| Left distal transradial access | 172 (13.87%) |
| ldRA success rate | 166 (96.51%) |
| Number of puncture attempts | 2.28 ± 0.67 |
| Artery puncture time, min | 1.26 ± 1.1 |
| Tortuosity (loop) | 14 (5.9%) |
| Pain score (0–5) | 2.7 ± 0.8 |
| Sheath size (5F) | 852 (68.7%) |
| Sheath size (6F) | 269 (21.6%) |
| Sheath size (7F) | 11 (0.88%) |
| Sheath size (8.5F) | 4 (0.32%) |
| Procedural duration (min) | 42.12 ± 10.1 |
| Fluoroscopy time (min) | 14.6 ± 10.2 |
| Radiation dose (/mGy) | 733.99 ± 542.23 |
| Postoperative complications (total) | 13 (1.04%) |
| Major bleeding | 0 (0%) |
| Vasospasm | 6 (0.48%) |
| Hematomas | 4 (0.32%) |
| Artery occlusion | 5(0.4%) |
| Hemostasis time (min) | 225 ± 10 |
| Repeat hemostasis | 3 (0.24%) |
| Radial patency at discharge | 4 (0.32%) |
| 2019 (n = 550) | 2020 (n = 448) | 2021 (n = 242) | p Value | |
|---|---|---|---|---|
| Sheath Time | ||||
| Ultrasonography Time (s) | 23.9 | 20.5 | 11.82 c | 0.001 |
| Puncture Time (s) | 158 | 162 | 138 c | 0.001 |
| Number of attempts | 2.32 | 1.9 | 1.64 b | 0.02 |
| Wall puncture Anterior Wall | 261 | 223 | 148 c | 0.001 |
| Anterior & Posterior Wall | 202 | 214 | 92 c | 0.001 |
| Cannulation Time (s) | 16.65 | 15.3 | 15.9 | 0.14 |
| Procedure Time (min) | 38.1 | 45.2 | 41.48 | 0.13 |
| Impact of the Learning Curve | Impact of the Learning Curve after 15 Cases | Control Group | p Value |
|---|---|---|---|
| Ultrasonography | |||
| Finding time (s) | 10.9 (5.2–16.7) | 8.4 (4.8–12.2) | <0.0001 |
| Radial cannulation | |||
| Puncture time (s) | 114.0 (58.8–19.2) | 51.6 (40.7–62.6) | 0.0358 |
| Puncture attempts | 2.15 (1.6–2.7) | 1.6 (1.4–1.8) | 0.0001 |
| Procedural factors | |||
| Procedure time (min) | 41.3 (31.3–51.2) | 33.2 (30.4–36.1) | 0.0604 |
| Contrast volume (mL) | 106.4 (87.9–124.9) | 108.7 (98.3–119) | 0.8266 |
| Radiation (Dyn/cm2) | 457.1 (220–694.2) | 472.2 (404.6–539.9) | 0.0644 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Achim, A.; Kákonyi, K.; Jambrik, Z.; Nagy, F.; Tóth, J.; Sasi, V.; Hausinger, P.; Nemes, A.; Varga, A.; Bertrand, O.F.; et al. Distal Radial Artery Access for Coronary and Peripheral Procedures: A Multicenter Experience. J. Clin. Med. 2021, 10, 5974. https://doi.org/10.3390/jcm10245974
Achim A, Kákonyi K, Jambrik Z, Nagy F, Tóth J, Sasi V, Hausinger P, Nemes A, Varga A, Bertrand OF, et al. Distal Radial Artery Access for Coronary and Peripheral Procedures: A Multicenter Experience. Journal of Clinical Medicine. 2021; 10(24):5974. https://doi.org/10.3390/jcm10245974
Chicago/Turabian StyleAchim, Alexandru, Kornél Kákonyi, Zoltán Jambrik, Ferenc Nagy, Julia Tóth, Viktor Sasi, Péter Hausinger, Attila Nemes, Albert Varga, Olivier F. Bertrand, and et al. 2021. "Distal Radial Artery Access for Coronary and Peripheral Procedures: A Multicenter Experience" Journal of Clinical Medicine 10, no. 24: 5974. https://doi.org/10.3390/jcm10245974
APA StyleAchim, A., Kákonyi, K., Jambrik, Z., Nagy, F., Tóth, J., Sasi, V., Hausinger, P., Nemes, A., Varga, A., Bertrand, O. F., & Ruzsa, Z. (2021). Distal Radial Artery Access for Coronary and Peripheral Procedures: A Multicenter Experience. Journal of Clinical Medicine, 10(24), 5974. https://doi.org/10.3390/jcm10245974