Using Salivary MMP-9 to Successfully Quantify Periodontal Inflammation during Orthodontic Treatment

 ,
,  ,
, 

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Saliva Sample Collection and Analysis
2.3. Statistical Analyses
3. Results
3.1. Clinical Parameters
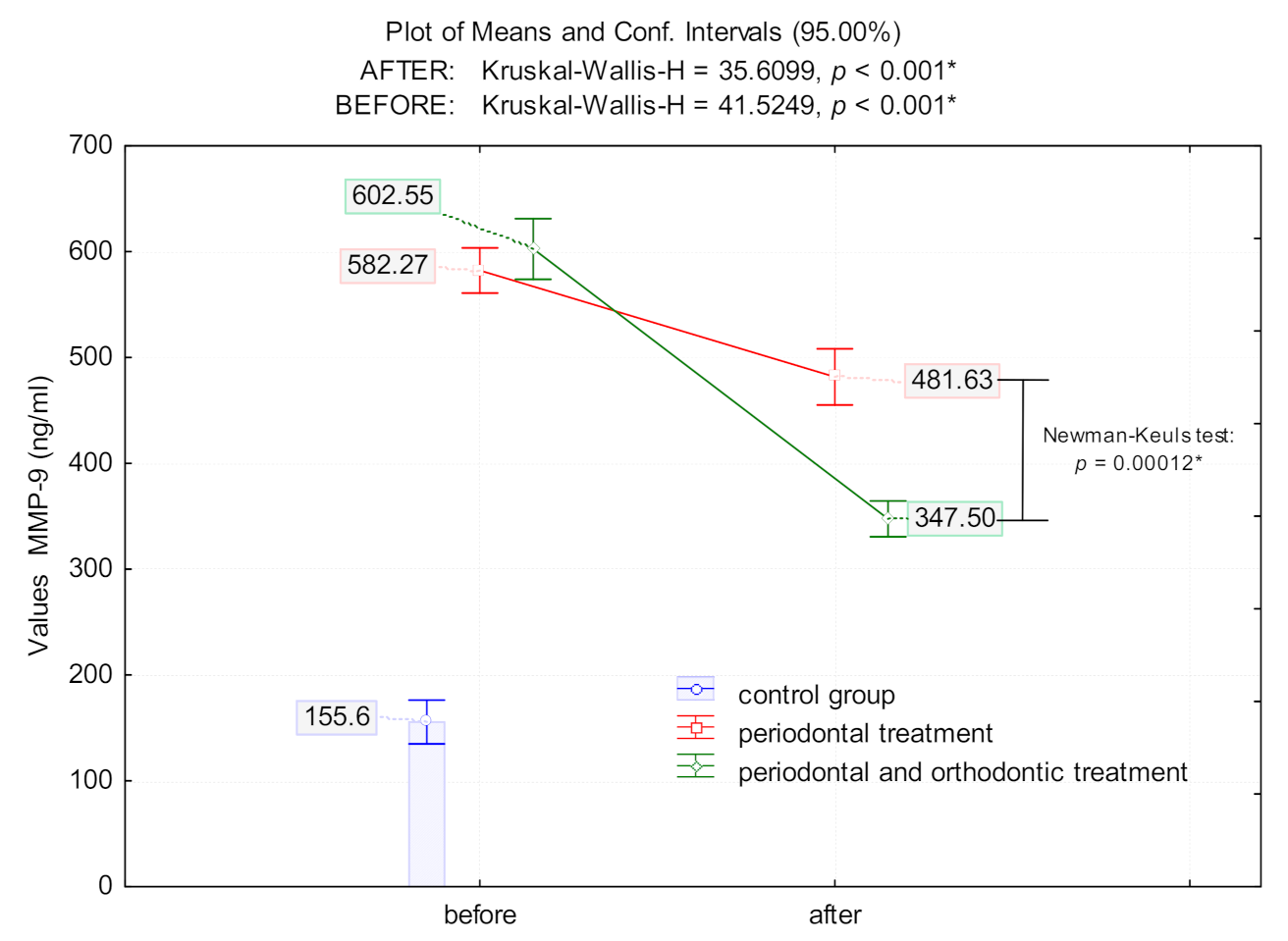
3.2. Effects of Periodontal and Combined Periodontal with Orthodontic Treatment on MMP-9 Levels
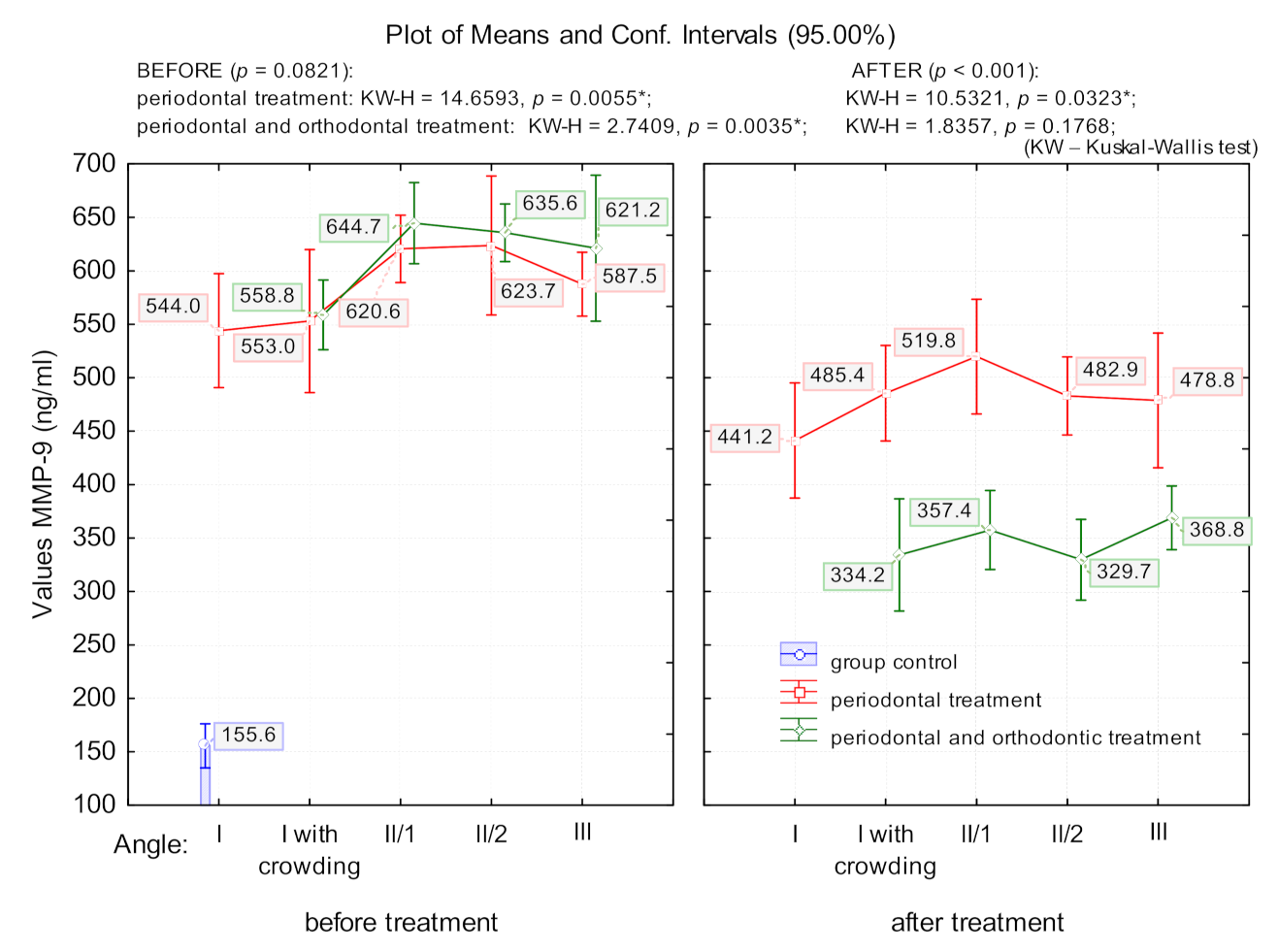
3.3. The Effect of Malocclusion on MMP-9 Levels
3.4. Correlation Between Clinical Parameters and MMP-9 Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Könönen, E.; Gursoy, M.; Gursoy, U.K. Periodontitis: A Multifaceted Disease of Tooth-Supporting Tissues. J. Clin. Med. 2019, 8, 1135. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.Y.; Kim, H.N. Changes in Inflammatory Cytokines in Saliva after Non-Surgical Periodontal Therapy: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 18, 194. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Susin, C. Periodontitis epidemiology: Is periodontitis under-recognized, over-diagnosed, or both? Periodontol. 2000 2017, 75, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, R.M. Oral health: The silent epidemic. Public Health Rep. 2010, 125, 158–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uitto, V.J.; Overall, C.M.; McCulloch, C. Proteolytic host cell enzymes in gingival crevice fluid. Periodontology 2000 2003, 31, 77–104. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Nucci, L.; Lanza, A.; Femiano, F.; Contaldo, M.; Grassia, V. Temporomandibular disc displacement with reduction treated with anterior repositioning splint: A 2-year clinical and magnetic resonance imaging (MRI) follow-up. J. Biol. Regul. Homeost. Agents 2020, 34, 151–160. [Google Scholar] [PubMed]
- Boelen, G.J.; Boute, L.; d’Hoop, J.; EzEldeen, M.; Lambrichts, I.; Opdenakker, G. Matrix metalloproteinases and inhibitors in dentistry. Clin. Oral. Investig. 2019, 23, 2823–2835. [Google Scholar] [CrossRef]
- Moccia, S.; Nucci, L.; Spagnuolo, C.; d’Apuzzo, F.; Piancino, M.G.; Minervini, G. Polyphenols as Potential Agents in the Management of Temporomandibular Disorders. Appl. Sci. 2020, 10, 5305. [Google Scholar] [CrossRef]
- Laronha, H.; Caldeira, J. Structure and Function of Human Matrix Metalloproteinases. Cells 2020, 9, 1076. [Google Scholar] [CrossRef]
- Birkedal-Hansen, H. Role of matrix metalloproteinases in human periodontal diseases. J. Periodontol. 1993, 64 (Suppl. 5), 474–484. [Google Scholar]
- Sorsa, T.; Tjaderhane, L.; Salo, T. Matrix metalloproteinases (MMPs) in oral diseases. Oral. Dis. 2004, 10, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Rathnayake, N.; Gustafsson, A.; Norhammar, A.; Kjellstrom, B.; Klinge, B.; Ryden, L.; Tervahartiala, T.; Sorsa, T.; Group, P.S. Salivary Matrix Metalloproteinase-8 and -9 and Myeloperoxidase in Relation to Coronary Heart and Periodontal Diseases: A Subgroup Report from the PAROKRANK Study (Periodontitis and Its Relation to Coronary Artery Disease). PLoS ONE 2015, 10, e0126370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narayanan, A.S.; Page, R.C. Connective tissues of the periodontium: A summary of current work. Coll. Relat. Res. 1983, 3, 33–64. [Google Scholar] [CrossRef]
- Aiba, T.; Akeno, N.; Kawane, T.; Okamoto, H.; Horiuchi, N. Matrix metalloproteinases-1 and -8 and TIMP-1 mRNA levels in normal and diseased human gingivae. Eur. J. Oral. Sci. 1996, 104, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Escalona, L.A.; Mastromatteo-Alberga, P.; Correnti, M. Cytokine and metalloproteinases in gingival fluid from patients with chronic periodontitis. Investig. Clin. 2016, 57, 131–142. [Google Scholar] [PubMed]
- Sorsa, T.; Tjaderhane, L.; Konttinen, Y.T.; Lauhio, A.; Salo, T.; Lee, H.M.; Golub, L.M.; Brown, D.L.; Mantyla, P. Matrix metalloproteinases: Contribution to pathogenesis, diagnosis and treatment of periodontal inflammation. Ann. Med. 2006, 38, 306–321. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.; Wilson, J.; Rock, P.; Chapple, I. Induction of cytokines, MMP9, TIMPs, RANKL and OPG during orthodontic tooth movement. Eur. J. Orthod. 2013, 35, 644–651. [Google Scholar] [CrossRef] [Green Version]
- Lahdentausta, L.S.J.; Paju, S.; Mantyla, P.; Buhlin, K.; Tervahartiala, T.; Pietiainen, M.; Alfthan, H.; Nieminen, M.S.; Sinisalo, J.; Sorsa, T.; et al. Saliva and serum biomarkers in periodontitis and coronary artery disease. J. Clin. Periodontol. 2018, 45, 1045–1055. [Google Scholar] [CrossRef]
- Marcaccini, A.M.; Meschiari, C.A.; Zuardi, L.R.; de Sousa, T.S.; Taba, M., Jr.; Teofilo, J.M.; Jacob-Ferreira, A.L.; Tanus-Santos, J.E.; Novaes, A.B., Jr.; Gerlach, R.F. Gingival crevicular fluid levels of MMP-8, MMP-9, TIMP-2, and MPO decrease after periodontal therapy. J. Clin. Periodontol. 2010, 37, 180–190. [Google Scholar] [CrossRef]
- Grassia, V.; D’Apuzzo, F.; Ferrulli, V.E.; Matarese, G.; Femiano, F.; Perillo, L. Dento-skeletal effects of mixed palatal expansion evaluated by postero-anterior cephalometric analysis. Eur. J. Paediatr. Dent. 2014, 15, 59–62. [Google Scholar]
- Maspero, C.; Fama, A.; Cavagnetto, D.; Abate, A.; Farronato, M. Treatment of dental dilacerations. J. Biol. Regul. Homeost. Agents 2019, 33, 1623–1627. [Google Scholar] [PubMed]
- Maspero, C.; Abate, A.; Cavagnetto, D.; Fama, A.; Stabilini, A.; Farronato, G.; Farronato, M. Operculectomy and spontaneous eruption of impacted second molars: A retrospective study. J. Biol. Regul. Homeost. Agents 2019, 33, 1909–1912. [Google Scholar] [PubMed]
- Alikhani, M.; Chou, M.Y.; Khoo, E.; Alansari, S.; Kwal, R.; Elfersi, T.; Almansour, A.; Sangsuwon, C.; Al Jearah, M.; Nervina, J.M.; et al. Age-dependent biologic response to orthodontic forces. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 632–644. [Google Scholar] [CrossRef] [PubMed]
- Perinetti, G.; D’Apuzzo, F.; Contardo, L.; Primozic, J.; Rupel, K.; Perillo, L. Gingival crevicular fluid alkaline phosphate activity during the retention phase of maxillary expansion in prepubertal subjects: A split-mouth longitudinal study. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Di Domenico, M.; D’Apuzzo, F.; Feola, A.; Cito, L.; Monsurro, A.; Pierantoni, G.M.; Berrino, L.; De Rosa, A.; Polimeni, A.; Perillo, L. Cytokines and VEGF induction in orthodontic movement in animal models. J. Biomed. Biotechnol. 2012, 2012, 201689. [Google Scholar] [CrossRef]
- Balli, U.; Keles, G.C.; Cetinkaya, B.O.; Mercan, U.; Ayas, B.; Erdogan, D. Assessment of vascular endothelial growth factor and matrix metalloproteinase-9 in the periodontium of rats treated with atorvastatin. J. Periodontol. 2014, 85, 178–187. [Google Scholar] [CrossRef]
- Meschiari, C.A.; Marcaccini, A.M.; Santos Moura, B.C.; Zuardi, L.R.; Tanus-Santos, J.E.; Gerlach, R.F. Salivary MMPs, TIMPs, and MPO levels in periodontal disease patients and controls. Clin. Chim. Acta 2013, 421, 140–146. [Google Scholar] [CrossRef]
- Goncalves, P.F.; Huang, H.; McAninley, S.; Alfant, B.; Harrison, P.; Aukhil, I.; Walker, C.; Shaddox, L.M. Periodontal treatment reduces matrix metalloproteinase levels in localized aggressive periodontitis. J. Periodontol. 2013, 84, 1801–1808. [Google Scholar] [CrossRef] [Green Version]
- Greenwell, H.; Committee on Research, Science and Therapy; American Academy of Periodontology. Position paper: Guidelines for periodontal therapy. J. Periodontol. 2001, 72, 1624–1628. [Google Scholar]
- Rathnayake, N.; Gieselmann, D.R.; Heikkinen, A.M.; Tervahartiala, T.; Sorsa, T. Salivary Diagnostics-Point-of-Care diagnostics of MMP-8 in dentistry and medicine. Diagnostics (Basel) 2017, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Cobzeanu, B.M.; Costan, V.V.; Danciu, M.; Pasca, A.S.; Sulea, D.; Ungureanu, L.B.; Moscalu, M.; Cobzeanu, M.D.; Popescu, E. Environmental factors involved in genesis of retromolar—oropharynx junction cancer. Environ. Eng. Manag. J. 2017, 16, 1101–1106. [Google Scholar] [CrossRef]
- Marcaccini, A.M.; Novaes, A.B., Jr.; Meschiari, C.A.; Souza, S.L.; Palioto, D.B.; Sorgi, C.A.; Faccioli, L.H.; Tanus-Santos, J.E.; Gerlach, R.F. Circulating matrix metalloproteinase-8 (MMP-8) and MMP-9 are increased in chronic periodontal disease and decrease after non-surgical periodontal therapy. Clin. Chim. Acta 2009, 409, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Correa, F.O.B.; Goncalves, D.; Figueredo, C.M.S.; Gustafsson, A.; Orrico, S.R.P. The Short-Term Effectiveness of Non-Surgical Treatment in Reducing Levels of Interleukin-1beta and Proteases in Gingival Crevicular Fluid from Patients with Type 2 Diabetes Mellitus and Chronic Periodontitis. J. Periodontol. 2008, 79, 2143–2150. [Google Scholar] [CrossRef] [PubMed]
- Figueredo, C.M.; Areas, A.; Miranda, L.A.; Fischer, R.G.; Gustafsson, A. The short-term effectiveness of non-surgical treatment in reducing protease activity in gingival crevicular fluid from chronic periodontitis patients. J. Clin. Periodontol. 2004, 31, 615–619. [Google Scholar] [CrossRef]
- Miller, C.S.; Foley, J.D.; Bailey, A.L.; Campell, C.L.; Humphries, R.L.; Christodoulides, N.; Floriano, P.N.; Simmons, G.; Bhagwandin, B.; Jacobson, J.W.; et al. Current developments in salivary diagnostics. Biomark Med. 2010, 4, 171–189. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, P.; Kharbanda, O.P.; Monga, N.; Miglani, R.; Kapila, S. Effect of orthodontic forces on cytokine and receptor levels in gingival crevicular fluid: A systematic review. Prog. Orthod. 2014, 15, 65. [Google Scholar] [CrossRef] [Green Version]
- Saloom, H.F.; Carpenter, G.H.; Cobourne, M.T. A cross-sectional cohort study of gingival crevicular fluid biomarkers in normal-weight and obese subjects during orthodontic treatment with fixed appliances. Angle Orthod. 2019, 89, 930–935. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, I.; Onodera, K.; Nishimura, M.; Mitnai, H.; Sasano, Y.; Mitani, H. Expression of genes for gelatinases and tissue inhibitors of metalloproteinases in periodontal tissues during orthodontic tooth movement. J. Mol. Histol. 2006, 37, 333–342. [Google Scholar] [CrossRef]
- Kapoor, P.; Monga, N.; Kharbanda, O.P.; Kapila, S.; Miglani, R.; Moganty, R. Effect of orthodontic forces on levels of enzymes in gingival crevicular fluid (GCF): A systematic review. Dental. Press J. Orthod. 2019, 24, 40.e1–40.e22. [Google Scholar] [CrossRef]
- Kushlinskii, N.E.; Solovykh, E.A.; Karaoglanova, T.B.; Boyar, U.; Gershtein, E.S.; Troshin, A.A.; Maksimovskaya, L.N.; Yanushevich, O.O. Matrix metalloproteinases and inflammatory cytokines in oral fluid of patients with chronic generalized periodontitis and various construction materials. Bull. Exp. Biol. Med. 2012, 153, 72–76. [Google Scholar] [CrossRef]
- Capelli, J., Jr.; Kantarci, A.; Haffajee, A.; Teles, R.P.; Fidel, R., Jr.; Figueredo, C.M. Matrix metalloproteinases and chemokines in the gingival crevicular fluid during orthodontic tooth movement. Eur. J. Orthod. 2011, 33, 705–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boiculese, L.V.; Dimitriu, G.; Moscalu, M. Nearest neighbor classification with improved weighted dissimilarity measure. Proc. Rom. Acad. Ser. A 2009, 10, 205–213. [Google Scholar]
- Herr, A.E.; Hatch, A.V.; Throckmorton, D.J.; Tran, H.M.; Brennan, J.S.; Giannobile, W.V.; Singh, A.K. Microfluidic immunoassays as rapid saliva-based clinical diagnostics. Proc. Natl. Acad. Sci. USA 2007, 104, 5268–5273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinane, D.F.; Darby, I.B.; Said, S.; Luoto, H.; Sorsa, T.; Tikanoja, S.; Mantyla, P. Changes in gingival crevicular fluid matrix metalloproteinase-8 levels during periodontal treatment and maintenance. J. Periodontal. Res. 2003, 38, 400–404. [Google Scholar] [CrossRef]
- Prescher, N.; Maier, K.; Munjal, S.K.; Sorsa, T.; Bauermeister, C.D.; Struck, F.; Netuschil, L. Rapid quantitative chairside test for active MMP-8 in gingival crevicular fluid: First clinical data. Ann. N. Y. Acad. Sci. 2007, 1098, 493–495. [Google Scholar] [CrossRef]
- Sorsa, T.; Hernandez, M.; Leppilahti, J.; Munjal, S.; Netuschil, L.; Mantyla, P. Detection of gingival crevicular fluid MMP-8 levels with different laboratory and chair-side methods. Oral. Dis. 2010, 16, 39–45. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luchian, I.; Moscalu, M.; Goriuc, A.; Nucci, L.; Tatarciuc, M.; Martu, I.; Covasa, M. Using Salivary MMP-9 to Successfully Quantify Periodontal Inflammation during Orthodontic Treatment. J. Clin. Med. 2021, 10, 379. https://doi.org/10.3390/jcm10030379
Luchian I, Moscalu M, Goriuc A, Nucci L, Tatarciuc M, Martu I, Covasa M. Using Salivary MMP-9 to Successfully Quantify Periodontal Inflammation during Orthodontic Treatment. Journal of Clinical Medicine. 2021; 10(3):379. https://doi.org/10.3390/jcm10030379
Chicago/Turabian StyleLuchian, Ionut, Mihaela Moscalu, Ancuta Goriuc, Ludovica Nucci, Monica Tatarciuc, Ioana Martu, and Mihai Covasa. 2021. "Using Salivary MMP-9 to Successfully Quantify Periodontal Inflammation during Orthodontic Treatment" Journal of Clinical Medicine 10, no. 3: 379. https://doi.org/10.3390/jcm10030379
APA StyleLuchian, I., Moscalu, M., Goriuc, A., Nucci, L., Tatarciuc, M., Martu, I., & Covasa, M. (2021). Using Salivary MMP-9 to Successfully Quantify Periodontal Inflammation during Orthodontic Treatment. Journal of Clinical Medicine, 10(3), 379. https://doi.org/10.3390/jcm10030379