
The Usefulness of [18F]F-Fluorodeoxyglucose and [18F]F-Sodium Fluoride Positron Emission Tomography Imaging in the Assessment of Early-Stage Aortic Valve Degeneration after Transcatheter Aortic Valve Implantation (TAVI)—Protocol Description and Preliminary Results


 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Echocardiography
- Normal leaflets without thickening or calcification;
- Evidence of thickening but without calcification;
- Calcification: small calcium spot not exceeding one-third of the leaflet area;
- Moderate calcification: calcium not exceeding two-thirds of the leaflet area;
- Heavily calcified: calcification covering more than two-thirds of the leaflet area.
2.2. Positron Emission Tomography/Computed Tomography (PET/CT)
2.3. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Echocardiography
3.3. [18. F]F-FDG and [18F]F-NaF PET/CT
3.3.1. Differences in [18F]F-FDG and [18F]F-NaF Uptake between Inner and Outer Areas of Particular Levels of TAVI Valves
3.3.2. Differences between Particular Levels for [18F]F-FDG and [18F]F-NaF Uptake Regarding the Averaged Inner and Outer Analyzed Areas of TAVI Valves
3.4. Correlations
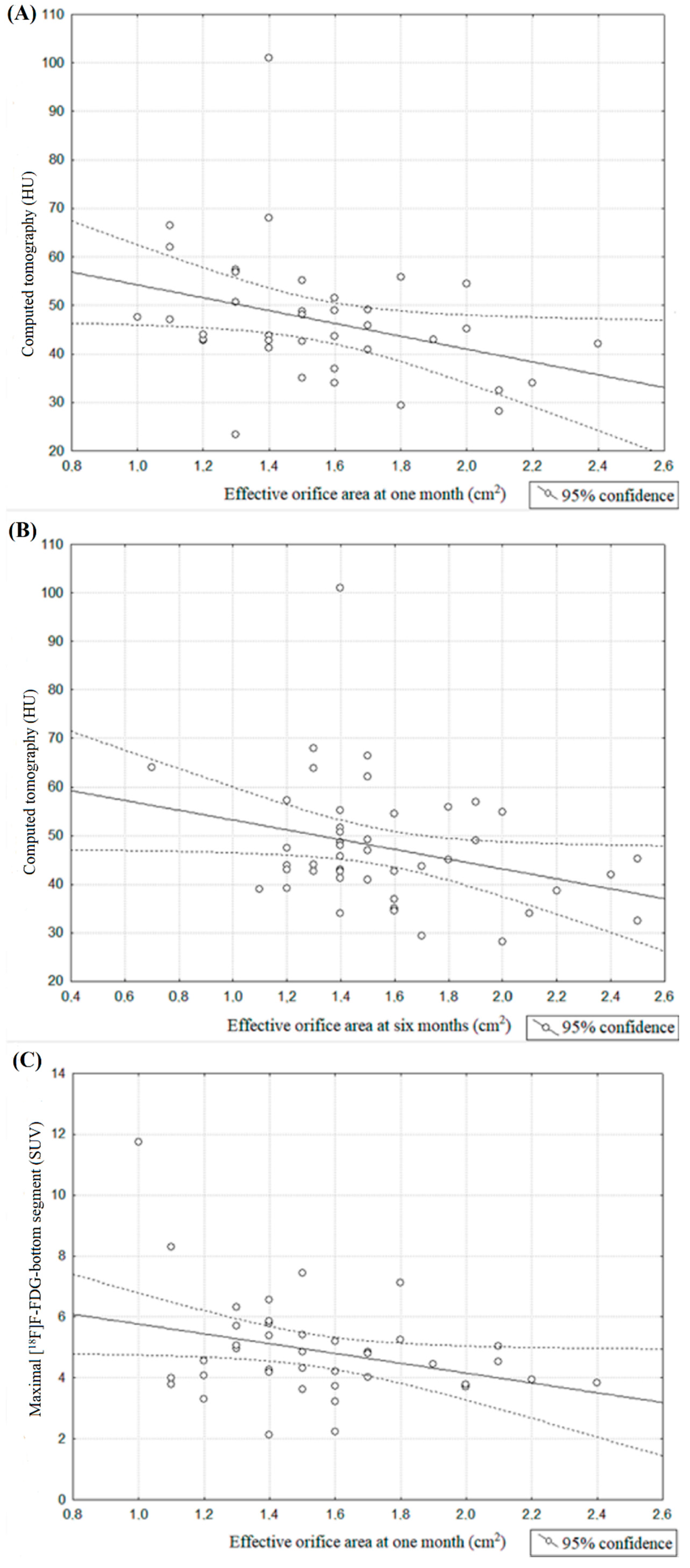
3.4.1. Effective Orifice Area
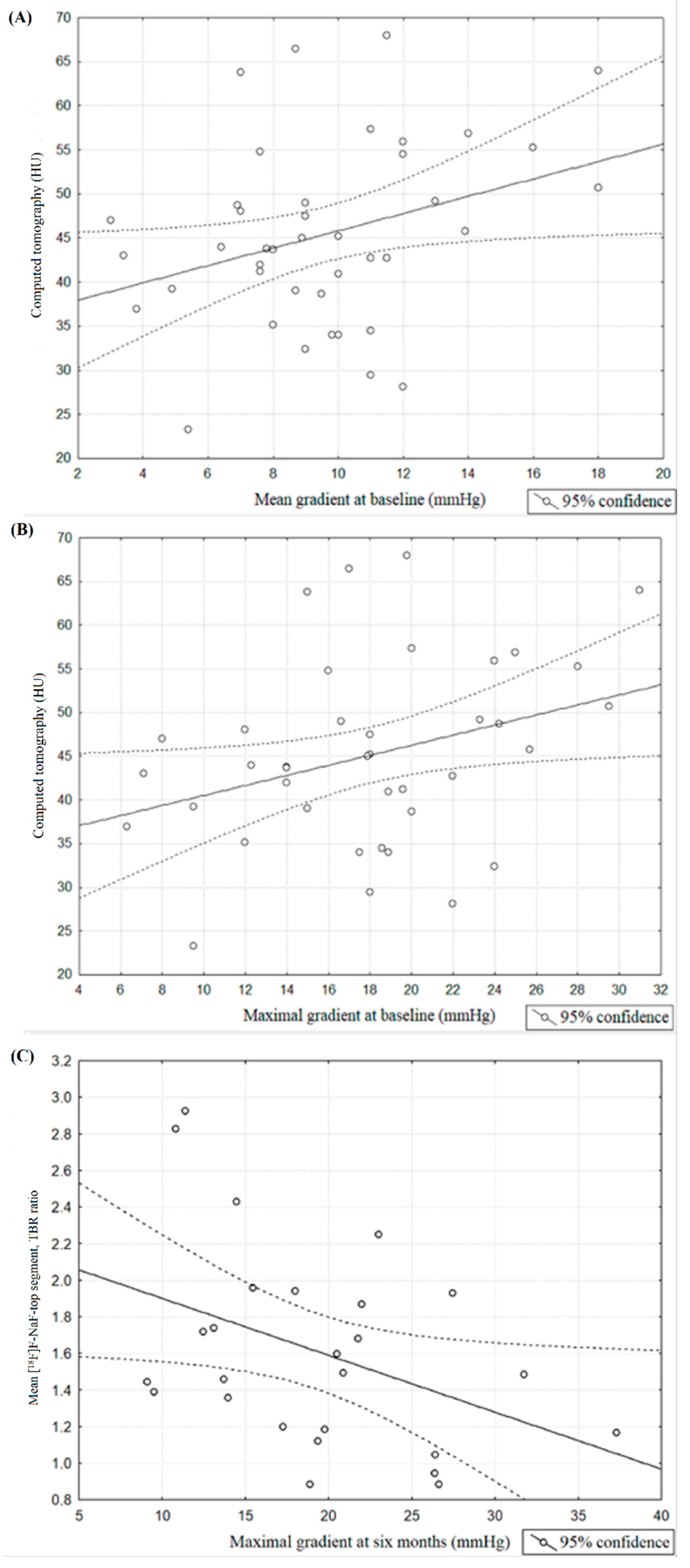
3.4.2. Aortic Valve Gradients
3.4.3. Valve Type
3.4.4. TAVI Valve Insufficiency
4. Discussion
Limitations
5. Conclusions
Impact on Daily Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eggebrecht, H.; Mehta, R.H. Transcatheter aortic valve implantation (TAVI) in Germany: More than 100,000 procedures and now the standard of care for the elderly. EuroIntervention 2019, 14, e1549–e1552. [Google Scholar] [CrossRef] [PubMed]
- Cartlidge, T.R.G.; Doris, M.K.; Sellers, S.L.; Pawade, T.A.; White, A.C.; Pessotto, R.; Kwiecinski, J.; Fletcher, A.; Alcaide, C.; Lucatelli, C.; et al. Detection and prediction of bioprosthetic aortic valve degeneration. J. Am. Coll. Cardiol. 2019, 73, 1107–1119. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Hung, J.; Bermejo, J.; Chambers, J.B.; Edvardsen, T.; Goldstein, S.; Lancellotti, P.; LeFevre, M.; Miller, F., Jr.; Otto, C.M. Recommendations on the echocardiographic assessment of aortic valve stenosis: A focused update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 254–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hahn, R.T.; Leipsic, J.; Douglas, P.S.; Jaber, W.A.; Weissman, N.J.; Pibarot, P.; Blanke, P.; Oh, J.K. Comprehensive Echocardiographic Assessment of Normal Transcatheter Valve Function. JACC Cardiovasc. Imaging 2019, 12, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Yousry, M.; Rickenlund, A.; Petrini, J.; Gustavsson, T.; Prahl, U.; Liska, J.; Eriksson, P.; Franco-Cereceda, A.; Eriksson, M.J.; Caidahl, K. Real-time imaging required for optimal echocardiographic assessment of aortic valve calcification. Clin. Physiol. Funct. Imaging 2012, 32, 470–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, W.S.; Vesey, A.T.; Shah, A.S.; Pawade, T.A.; Chin, C.W.; White, A.C.; Fletcher, A.; Cartlidge, T.R.; Mitchell, A.J.; Pringle, M.A.; et al. Valvular (18)F-Fluoride and (18)F-Fluorodeoxyglucose Uptake Predict Disease Progression and Clinical Outcome in Patients with Aortic Stenosis. J. Am. Coll. Cardiol. 2015, 66, 1200–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritman, E.L. Small-animal CT—Its difference from, and impact on, clinical CT. Nucl. Instrum. Methods Phys. Res. A 2007, 580, 968–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creager, M.D.; Hohl, T.; Hutcheson, J.D.; Moss, A.J.; Schlotter, F.; Blaser, M.C.; Park, M.A.; Lee, L.H.; Singh, S.A.; Alcaide-Corral, C.J.; et al. [18F]F-fluoride signal amplification identifies microcalcifications associated with atherosclerotic plaque instability in positron emission tomography/computed tomography images. Circ. Cardiovasc. 2019, 12, e007835. [Google Scholar] [CrossRef] [Green Version]
- Cocker, M.S.; Spence, J.D.; Hammond, R.; deKemp, R.A.; Lum, C.; Wells, G.; Bernick, J.; Hill, A.; Nagpal, S.; Stotts, G.; et al. Canadian Atherosclerosis Imaging Network (CAIN)—Project II. [[18F]F]-Fluorodeoxyglucose PET/CT imaging as a marker of carotid plaque inflammation: Comparison to immunohistology and relationship to acuity of events. Int. J. Cardiol. 2018, 271, 378–386. [Google Scholar] [CrossRef] [PubMed]
- Dweck, M.R.; Jenkins, W.S.; Vesey, A.T.; Pringle, M.A.; Chin, C.W.; Malley, T.S.; Cowie, W.J.; Tsampasian, V.; Richardson, H.; Fletcher, A.; et al. [18F]F-sodium fluoride uptake is a marker of active calcification and disease progression in patients with aortic stenosis. Circ. Cardiovasc. Imaging 2014, 7, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Tzolos, E.; Dweck, M.R. [18F]F-Sodium Fluoride ([18F]F-NaF) for Imaging Microcalcification Activity in the Cardiovascular System. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1620–1626. [Google Scholar] [CrossRef] [PubMed]
- Dweck, M.R.; Jones, C.; Joshi, N.V.; Fletcher, A.M.; Richardson, H.; White, A.; Marsden, M.; Pessotto, R.; Clark, J.C.; Wallace, W.A.; et al. Assessment of valvular calcification and inflammation by positron emission tomography in patients with aortic stenosis. Circulation 2012, 125, 76–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dweck, M.R.; Khaw, H.J.; Sng, G.K.; Luo, E.L.; Baird, A.; Williams, M.C.; Makiello, P.; Mirsadraee, S.; Joshi, N.V.; van Beek, E.J.; et al. Aortic stenosis, atherosclerosis, and skeletal bone: Is there a common link with calcification and inflammation? Eur. Heart J. 2013, 34, 1567–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clavel, M.A.; Burwash, I.G.; Pibarot, P. Cardiac imaging for assessing low-gradient severe aortic stenosis. JACC Cardiovasc. Imaging 2017, 10, 185–202. [Google Scholar] [CrossRef] [PubMed]
- Arani, L.S.; Gharavi, M.H.; Zadeh, M.Z.; Raynor, W.Y.; Seraj, S.M.; Constantinescu, C.M.; Gerke, O.; Werner, T.J.; Hoilund-Carlsen, P.F.; Alavi, A. Association between age, uptake of [18F]F-fluorodeoxyglucose and of [18F]F-sodium fluoride, as cardiovascular risk factors in the abdominal aorta. Hell. J. Nucl. Med. 2019, 22, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Pawade, T.A.; Cartlidge, T.R.; Jenkins, W.S.; Adamson, P.D.; Robson, P.; Lucatelli, C.; Van Beek, E.J.; Prendergast, B.; Denison, A.R.; Forsyth, L.; et al. Optimization and Reproducibility of Aortic Valve [18F]F-Fluoride Positron Emission Tomography in Patients With Aortic Stenosis. Circ. Cardiovasc. Imaging 2016, 9, e005131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joshi, N.V.; Vesey, A.T.; Williams, M.C.; Shah, A.S.; Calvert, P.A.; Craighead, F.H.; Yeoh, S.E.; Wallace, W.; Salter, D.; Fletcher, A.M.; et al. [18F]F-fluoride positron emission tomography for identification of ruptured and high-risk coronary atherosclerotic plaques: A prospective clinical trial. Lancet 2014, 383, 705–713. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Selected Indices | (n = 73) |
|---|---|
| Age, years | 82.49 ± 7.11, 85 (80 ÷ 87) |
| Gender, males | 31 (42.4) |
| Body mass, kg | 72.05 ± 14.77, 71 (60 ÷ 80) |
| Body height, cm | 163.68 ± 9.58, 165 (158 ÷ 170) |
| Body-mass index, kg/m2 | 26.80 ± 4.51, 26.45 (23.05 ÷ 29.86) |
| Body Surface area, m2 | 1.78 ± 0.21, 1.77 (1.63 ÷ 1.95) |
| Glomerular filtration rate (GFR), mL/min./1.73 m2 | 62.69 ± 18.85, 64 (48 ÷ 78) |
| NYHA classification before TAVI:—I | 3 (4.1) |
| —II | 15 (20.5) |
| —III | 50 (68.5) |
| —IV | 5 (6.9) |
| Kidney failure (GFR < 60 mL/min./1.73 m2) | 31(42.3) |
| Arterial hypertension | 65(90.1) |
| Diabetes mellitus | 28(39.4) |
| Atrial fibrillation | 38 (52.1) |
| Prior myocardial infarction | 24(35.2) |
| Prior percutaneous coronary interventions | 29 (40.8) |
| Prior coronary artery by-pass surgery | 12 (16.9) |
| Prior balloon aortic valvuloplasty | 27 (38.0) |
| Carotid artery stenosis | 4 (5.6) |
| Chronic obstructive pulmonary disease | 10 (14.1) |
| Prior cerebral stroke/transient ischaemic attack | 10 (14.1) |
| Prior pacemaker implantation | 12 (16.9) |
| Selected Indices | Before TAVI (Initial) | After TAVI (Baseline) | Follow-Up | |
|---|---|---|---|---|
| 1 Month | 6 Months | |||
| Mean gradient before TAVI, mmHg | 52.93 ± 19.13 | 9.42 ± 3.81 | 9.95 ± 3.83 | 10.06 ± 3.89 |
| 50 (40 ÷ 66) | 9 (7.29 ÷ 11.07) * | 9.82 (7.44 ÷ 11.77) * | 9.46 (7.54 ÷ 12.11) * | |
| Peak gradient after TAVI, mmHg | 17.55 ± 7.10 | 17.97 ± 6.23 | 18.04 ± 6.41 | |
| 17.5 (13.9 ÷ 20.54) | 17.88 (13.47 ÷ 20.52) | 17.29 (13.75 ÷ 21.1) | ||
| Effective orifice area, cm2 | 0.63 ± 0.17 | 1.52 ± 0.32 | 1.74 ± 1.51 | |
| 0.6 (0.5 ÷ 0.7) | 1.5 (1.3 ÷ 1.7) | 1.5 (1.32 ÷ 1.77) | ||
| Left ventricle ejection fraction, % | 52.10 ± 15.34 | 54.74 ± 12.53 | 57.43 ± 12.54 | 56.79 ± 11.47 |
| 60 (40 ÷ 65) | 60 (45 ÷ 65)* | 60 (50 ÷ 66)* | 60 (48.75 ÷ 65)* | |
| Aortic regurgitation | ||||
| —none | 5 (7.1) | 42 (57.4) | 49 (92.4) | 51 (87.9) |
| —trace | 15 (20.5) | 19 (26.2) | 4 (7.6) | 6 (10.4) |
| —mild | 29 (39.5) | 12 (16.4) | 0 (0) | 1 (1.7) |
| —moderate | 16 (22.5) | 0 (0) | 0 (0) | 0 (0) |
| —severe | 8 (11.2) | 0 (0) | 0 (0) | 0 (0) |
| Paravalvular leak grade | 1.69 ± 1.32 | 1.62 ± 1.33 | ||
| 1 (1 ÷ 2) | 1 (1 ÷ 2) | |||
| —none | 7 (13.2) | 10 (17.24) | ||
| —trace | 11 (20.75) | 11 (18.96) | ||
| —mild | 24 (45.28) | 25 (43.1) | ||
| —moderate | 11 (20.75) | 11 (18.96) | ||
| —severe | 0 (0) | 1 (1.72) | ||
| Assessment Area | Indicator Type | Marker Type | |||||
|---|---|---|---|---|---|---|---|
| [18F]F-Sodium Fluoride | [18F]F-Fluorodeoxyglucose | ||||||
| Mapping Level | |||||||
| Top | Middle | Bottom | Top | Middle | Bottom | ||
| SUV inner | Mean | 1.89 ± 0.48 | 1.89 ± 0.62 | 1.87 ± 0.53 | 2.16 ± 0.5 | 2.18 ± 0.43 | 2.17 ± 0.42 |
| 1.95 | 1.84 | 2.02 | 2.27 | 2.1 | 2.13 | ||
| (1.57 ÷ 2.2) | (1.44 ÷ 2.38) | (1.47 ÷ 2.35) | (1.84 ÷ 2.43) | (1.92 ÷ 2.54) | (2 ÷ 2.5) | ||
| Mean—TBR | 1.55 ± 0.52 | 1.57 ± 0.64 | 1.54 ± 0.56 | 1.59 ± 1.1 | 1.54 ± 0.58 | 1.57 ± 0.75 | |
| 1.47 | 1.55 | 1.47 | 1.34 | 1.43 | 1.5 | ||
| (1.11 ÷ 1.93) | (1.0 ÷ 1.86) | (1.25 ÷ 1.79) | (1.13 ÷ 1.6) | (1.13 ÷ 1.71) | (1.1 ÷ 1.85) | ||
| Max. | 4.15 ± 1.35 * | 4.39 ± 1.42 * | 4.24 ± 1.33 * | 4.41 ± 1.77 * | 4.4 ± 1.32 * | 4.35 ± 1.24 * | |
| 3.95 | 4.09 | 4.22 | 3.9 | 4.02 | 4.17 | ||
| (3.36 ÷ 5.18) | (3.55 ÷ 5.07) | (3.47 ÷ 5.03) | (3.46 ÷ 4.96) | (3.6 ÷ 4.98) | (3.61 ÷ 4.82) | ||
| Max. TBR | 3.02 ± 1.21 * | 3.23 ± 1.4 * | 3.14 ± 1.38 * | 2.98 ± 3.28 | 2.89 ± 2.38 | 2.85 ± 1.99 | |
| 2.66 | 2.98 | 3.06 | 2.44 | 2.56 | 2.39 | ||
| (2.05 ÷ 3.84) | (2.26 ÷ 3.84) | (2.18 ÷ 3.76) | (2.01 ÷ 2.99) | (2.06 ÷ 2.99) | (1.93 ÷ 3.26) | ||
| SUV outer | Mean | 1.95 ± 0.55 | 1.99 ± 0.63 | 1.88 ± 0.52 | 2.15 ± 0.42 | 2.25 ± 0.4 | 2.2 ± 0.42 |
| 1.92 | 2.05 | 1.86 | 2.04 | 2.22 | 2.29 | ||
| (1.58 ÷ 2.29) | (1.58 ÷ 2.62) | (1.52 ÷ 2.29) | (1.95 ÷ 2.43) | (1.98 ÷ 2.52) | (1.97 ÷ 2.43) | ||
| Mean—TBR | 1.61 ± 0.62 | 1.66 ± 0.74 | 1.56 ± 0.63 | 1.54 ± 0.65 | 1.63 ± 0.78 | 1.59 ± 0.73 | |
| 1.48 | 1.52 | 1.41 | 1.49 | 1.55 | 1.52 | ||
| (1.13 ÷ 1.86) | (1.15 ÷ 1.96) | (1.14 ÷ 1.85) | (1.1 ÷ 1.77) | (1.14 ÷ 1.84) | (1.09 ÷ 1.81) | ||
| Max. | 5.37 ± 1.71 | 5.33 ± 1.71 | 5.32 ± 1.96 | 4.82 ± 1.68 | 5.09 ± 2.06 | 5.36 ± 2.32 | |
| 4.99 | 5.19 | 5.09 | 4.41 | 4.59 | 4.84 | ||
| (4.16 ÷ 6.34) | (4.14 ÷ 6.02) | (3.92 ÷ 6.22) | (3.88 ÷ 5.31) | (3.99 ÷ 5.48) | (4.21 ÷ 5.74) | ||
| Max.—TBR | 3.92 ± 1.53 | 3.93 ± 1.76 | 3.91 ± 1.79 | 3.26 ± 3.31 | 3.54 ± 4.31 | 2.55 ± 1.02 | |
| 3.77 | 3.66 | 3.52 | 2.78 | 2.78 | 2.35 | ||
| (2.63 ÷ 4.91) | (2.62 ÷ 4.72) | (2.83 ÷ 4.72) | (2.21 ÷ 3.37) | (2.29 ÷ 3.38) | (2.01 ÷ 2.82) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sorysz, D.; Januszek, R.; Sowa-Staszczak, A.; Grochowska, A.; Opalińska, M.; Bagieński, M.; Zawiślak, B.; Dziewierz, A.; Tokarek, T.; Krawczyk-Ożóg, A.; et al. The Usefulness of [18F]F-Fluorodeoxyglucose and [18F]F-Sodium Fluoride Positron Emission Tomography Imaging in the Assessment of Early-Stage Aortic Valve Degeneration after Transcatheter Aortic Valve Implantation (TAVI)—Protocol Description and Preliminary Results. J. Clin. Med. 2021, 10, 431. https://doi.org/10.3390/jcm10030431
Sorysz D, Januszek R, Sowa-Staszczak A, Grochowska A, Opalińska M, Bagieński M, Zawiślak B, Dziewierz A, Tokarek T, Krawczyk-Ożóg A, et al. The Usefulness of [18F]F-Fluorodeoxyglucose and [18F]F-Sodium Fluoride Positron Emission Tomography Imaging in the Assessment of Early-Stage Aortic Valve Degeneration after Transcatheter Aortic Valve Implantation (TAVI)—Protocol Description and Preliminary Results. Journal of Clinical Medicine. 2021; 10(3):431. https://doi.org/10.3390/jcm10030431
Chicago/Turabian StyleSorysz, Danuta, Rafał Januszek, Anna Sowa-Staszczak, Anna Grochowska, Marta Opalińska, Maciej Bagieński, Barbara Zawiślak, Artur Dziewierz, Tomasz Tokarek, Agata Krawczyk-Ożóg, and et al. 2021. "The Usefulness of [18F]F-Fluorodeoxyglucose and [18F]F-Sodium Fluoride Positron Emission Tomography Imaging in the Assessment of Early-Stage Aortic Valve Degeneration after Transcatheter Aortic Valve Implantation (TAVI)—Protocol Description and Preliminary Results" Journal of Clinical Medicine 10, no. 3: 431. https://doi.org/10.3390/jcm10030431
APA StyleSorysz, D., Januszek, R., Sowa-Staszczak, A., Grochowska, A., Opalińska, M., Bagieński, M., Zawiślak, B., Dziewierz, A., Tokarek, T., Krawczyk-Ożóg, A., Bartuś, S., & Dudek, D. (2021). The Usefulness of [18F]F-Fluorodeoxyglucose and [18F]F-Sodium Fluoride Positron Emission Tomography Imaging in the Assessment of Early-Stage Aortic Valve Degeneration after Transcatheter Aortic Valve Implantation (TAVI)—Protocol Description and Preliminary Results. Journal of Clinical Medicine, 10(3), 431. https://doi.org/10.3390/jcm10030431