
Evaluation of QOL in Patients with Dyspeptic Symptoms Who Meet or Do Not Meet Rome IV Criteria


 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Assessment
2.4. Questionnaires (Digestive Symptoms, Psychological, HR-QOL)
2.5. Stastical Analysis
3. Results
3.1. Enrolment of the Patients
3.2. Baseline Characteristics and Symptoms
3.3. Subdivision of Non-FD Patients
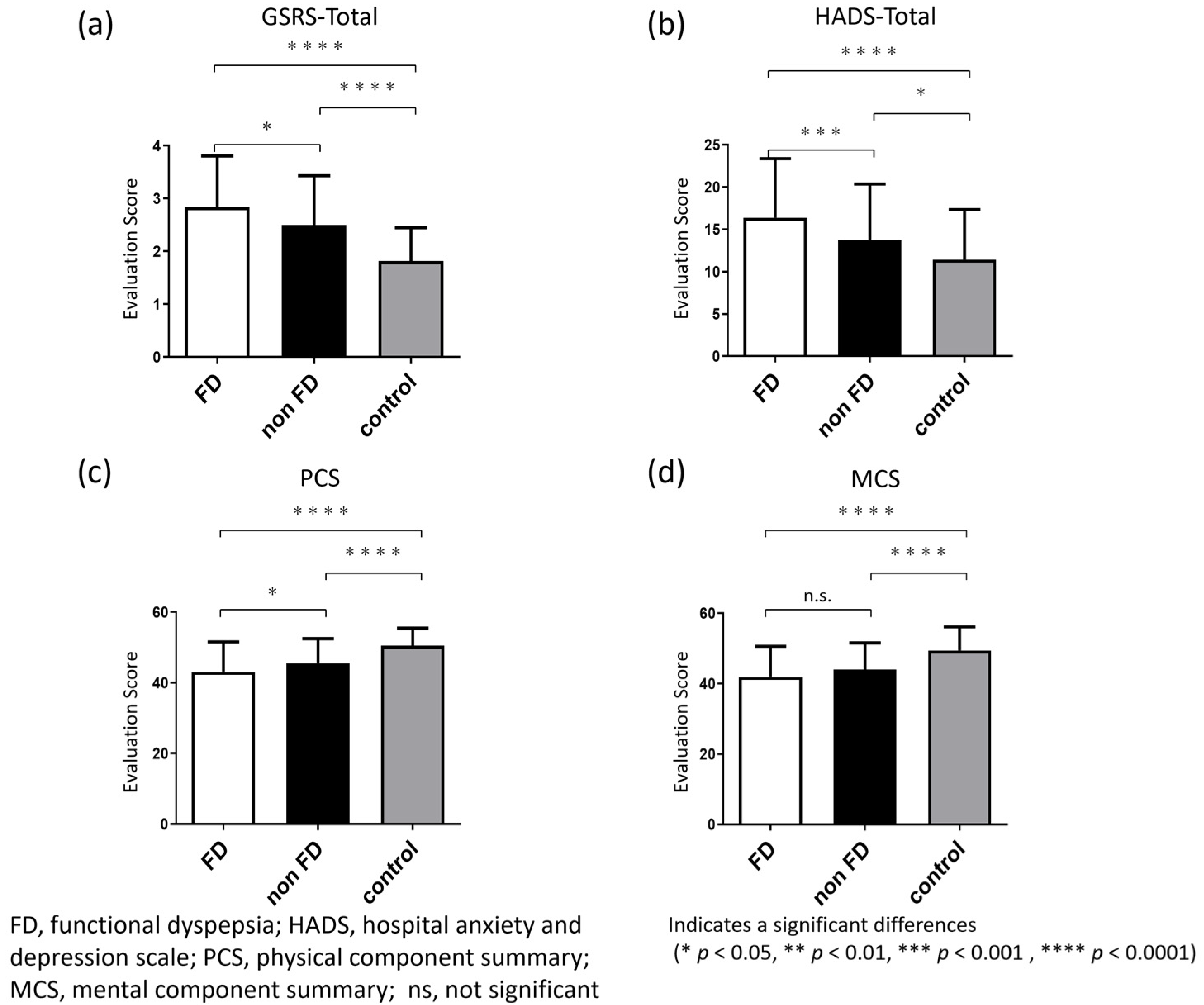
3.4. GSRS Score of the Three Groups (FD, Non-FD and Control)
3.5. HADS Score of the Three Groups (FD, Non-FD and Control)
3.6. SF-8 Score of the Three Groups (FD, Non-FD and Control)
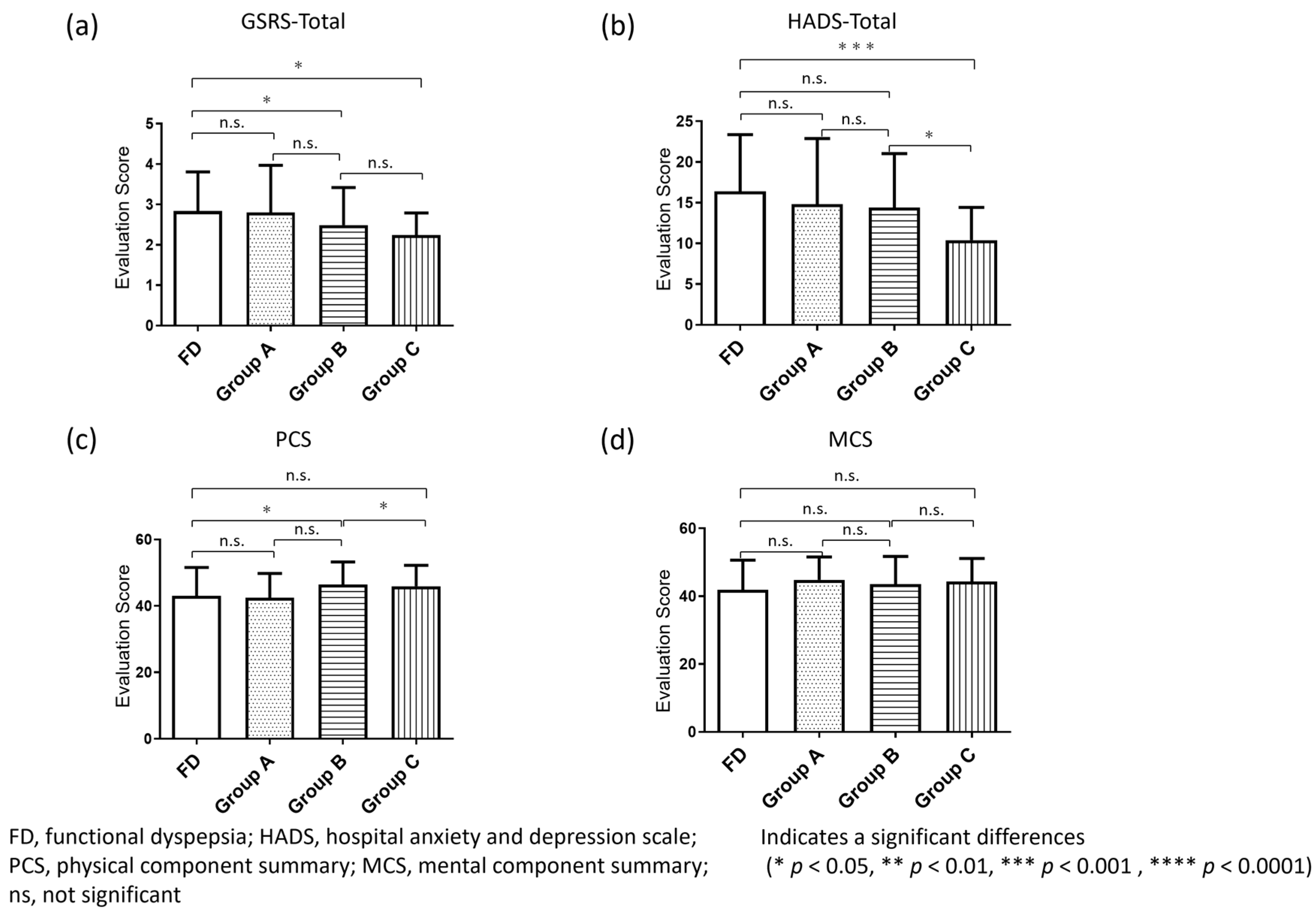
3.7. Comparison of Clinical Characteristics among the Four Groups (FD Group, Group A, Group B and Group C)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

References
- Drossman, D.A. Functional gastrointestinal disorders: History, pathophysiology, clinical features and Rome IV. Gastroenterology 2016, 150, 1262–1279. [Google Scholar] [CrossRef] [Green Version]
- Tomita, T.; Oshima, T.; Miwa, H. New approaches to diagnosis and treatment of functional dyspepsia. Curr. Gastroenterol. Rep. 2018, 20, 55. [Google Scholar] [CrossRef]
- Miwa, H.; Kusano, M.; Arisawa, T.; Oshima, T.; Kato, M.; Joh, T.; Suzuki, H.; Tominaga, K.; Nakada, K.; Nagahara, A.; et al. Japanese Society of Gastroenterology. Evidence-based clinical practice guidelines for functional dyspepsia. J. Gastroenterol. 2015, 50, 125–139. [Google Scholar] [CrossRef] [Green Version]
- Moayyedi, P.M.; Lacy, B.E.; Andrews, C.N.; Enns, R.A.; Howden, C.W.; Vakil, N. ACG and CAG Clinical Guideline: Management of Dyspepsia. Am. J. Gastroenterol. 2017, 112, 988–1013. [Google Scholar] [CrossRef] [PubMed]
- Stanghellini, V.; Chan, F.K.; Hasler, W.L.; Malagelada, J.R.; Suzuki, H.; Tack, J.; Talley, N.J. Gastroduodenal disorders. Gastroenterology 2016, 150, 1380–1392. [Google Scholar] [CrossRef]
- Tack, J.; Talley, N.J.; Camilleri, M.; Holtmann, G.; Hu, P.; Malagelada, J.-R.; Stanghellini, V. Functional gastroduodenal disorders. Gastroenterology 2006, 130, 1466–1479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Houte, K.; Carbone, F.; Goelen, N.; Schol, J.; Masuy, I.; Arts, J.; Caenepeel, P.; Staessen, D.; Vergauwe, P.; Van Roey, G.; et al. Effects of Rome IV definitions of functional dyspepsia subgroups in secondary care. Clin. Gastroenterol. Hepatol. 2020, 18, 838–846. [Google Scholar] [CrossRef]
- Brewer, J.; Owens, M.Y.; Wallace, K.; Reeves, A.A.; Morris, R.; Khan, M.; LaMarca, B.; Martin, J.N. Posterior reversible encephalopathy syndrome in 46 of 47 patients with eclampsia. Am. J. Obstet. Gynecol. 2013, 208, 468.e1–468.e6. [Google Scholar] [CrossRef] [PubMed]
- Tack, J.; Van den Houte, K.; Carbone, F. The unfulfilled promise of prokinetics for functional dyspepsia/postprandial distress syndrome. Am. J. Gastroenterol. 2019, 114, 204–206. [Google Scholar] [CrossRef]
- Nakajima, S.; Takahashi, K.; Sato, J.; Fukuda, M.; Yamamoto, K.; Inoue, T.; Okumura, Y.; Fujiyama, Y. Spectra of functional gastrointestinal disorders diagnosed by Rome III integrative questionnaire in a Japanese outpatient office and the impact of overlapping. J. Gastroenterol. Hepatol. 2010, 25 (Suppl. 1), S138–S143. [Google Scholar] [CrossRef]
- Wei, Z.; Yang, Q.; Yang, Q.; Yang, J.; Tantai, X.; Xing, X.; Xiao, C.; Pan, Y.; Liu, N.; Wang, J. Rome III, Rome IV, and potential Asia symptom criteria for functional dyspepsia do not reliably distinguish functional from organic disease. Clin. Transl. Gastroenterol. 2020, 11, e00278. [Google Scholar] [CrossRef] [PubMed]
- Park, J.M.; Choi, M.-G.; Cho, Y.K.; Lee, I.S.; Kim, J.I.; Kim, S.W.; Chung, I.-S. Functional gastrointestinal disorders diagnosed by Rome III questionnaire in Korea. J. Neurogastroenterol. Motil. 2011, 17, 279–286. [Google Scholar] [CrossRef]
- Ghoshal, U.C.; Singh, R. Frequency and risk factors of functional gastro-intestinal disorders in a rural Indian population. J. Gastroenterol. Hepatol. 2017, 32, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Yang, Y.S.; Cui, L.H.; Sun, G.; Peng, L.H.; Wang, W.F.; Hyder, Q.; Zhang, X.L. The overlap of upper functional gastrointestinal disorders with irritable bowel syndrome in Chinese outpatients: A multicenter study. J. Gastroenterol. Hepatol. 2016, 31, 1584–1593. [Google Scholar] [CrossRef]
- Ohara, S.; Kawano, T.; Kusano, M.; Kouzu, T. Survey on the prevalence of GERD and FD based on the Montreal definition and the Rome III criteria among patients presenting with epigastric symptoms in Japan. J. Gastroenterol. 2011, 46, 603–611. [Google Scholar] [CrossRef]
- Wang, A.; Liao, X.; Xiong, L.; Peng, S.; Xiao, Y.; Liu, S.; Hu, P.; Chen, M. The clinical overlap between functional dyspepsia and irritable bowel syndrome based on Rome III criteria. BMC Gastroenterol. 2008, 8, 43. [Google Scholar] [CrossRef] [Green Version]
- Okada, K.; Kawai, M.; Uesaka, K.; Kodera, Y.; Nagano, H.; Murakami, Y.; Morita, S.; Sakamoto, J.; Yamaue, H.; JAPAN-PD Investigators. Effect of Daikenchuto (TJ-100) on postoperative bowel motility and on prevention of paralytic ileus after pancreaticoduodenectomy: A multicenter, randomized, placebo-controlled phase II trial (the JAPAN-PD study). Jpn. J. Clin. Oncol. 2013, 43, 436–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svedlund, J.; Sjödin, I.; Dotevall, G. GSRS—A clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig. Dis. Sci. 1988, 33, 129–134. [Google Scholar] [CrossRef]
- Revicki, D.A.; Wood, M.; Wiklund, I.; Crawley, J. Reliability and validity of the Gastrointestinal Symptom Rating Scale in patients with gastroesophageal reflux disease. Qual. Life Res. 1998, 7, 75–83. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Higashi, A.; Yashiro, H.; Kiyota, K.; Inokuchi, H.; Hatta, H.; Fujita, K.; Watanabe, Y.; Kawai, K. Validation of the hospital anxiety and depression in a gastro-intestinal clinic. J. Jpn. Soc. Gastroenterol. 1996, 93, 884–892. [Google Scholar]
- Nam, K.; Kim, N.; Song, H.J.; Baik, G.H.; Choi, S.C.; Kim, H.J.; Lee, J.Y.; Park, K.S.; Park, S.-Y.; Park, S.J. Gender difference in the overlap of irritable bowel syndrome and functional dyspepsia: A prospective nationwide multicenter study in Korea. J. Gastroenterol. 2021, 56, 537–546. [Google Scholar] [CrossRef]
- Tokuda, Y.; Okubo, T.; Ohde, S.; Jacobs, J.; Takahashi, O.; Omata, F.; Yanai, H.; Hinohara, S.; Fukui, T. Assessing items on the SF-8 Japanese version for health-related quality of life: A psychometric analysis based on the nominal categories model of item response theory. Value Health 2009, 12, 568–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miwa, H.; Nagahara, A.; Tominaga, K.; Yokoyama, T.; Sawada, Y.; Inoue, K.; Ashida, K.; Fukuchi, T.; Hojo, M.; Yamashita, H.; et al. Efficacy of the 5-HT1A agonist tandospirone citrate in improving symptoms of patients with functional dyspepsia: A randomized controlled trial. Am. J. Gastroenterol. 2009, 104, 2779–2787. [Google Scholar] [CrossRef] [PubMed]
- Manabe, N.; Haruma, K.; Hata, J.; Imamura, H.; Kamada, T.; Kusunoki, H.; Sanuki, E.; Tsumaru, S.; Futagami, Y.; Sadamoto, Y.; et al. Clinical characteristics of Japanese dyspeptic patients: Is the Rome III classification applicable? Scand. J. Gastroenterol. 2010, 45, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Iacovou, M.; Tan, V.; Muir, J.G.; Gibson, P.R. The Low FODMAP Diet and its application in East and Southeast Asia. J. Neurogastroenterol. Motil. 2015, 21, 459–470. [Google Scholar] [CrossRef] [Green Version]
- Halmos, E.P.; Power, V.A.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology 2014, 146, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Talley, N.J. What Causes Functional Gastrointestinal Disorders? A Proposed Disease Model. Am. J. Gastroenterol. 2020, 115, 41–48. [Google Scholar] [CrossRef]
- Kinoshita, Y.; Chiba, T.; The FUTURE Study Group. Characteristics of Japanese patients with chronic gastritis and comparison with functional dyspepsia defined by ROME III criteria: Based on the large-scale survey, FUTURE study. Intern. Med. 2011, 50, 2269–2276. [Google Scholar] [CrossRef] [Green Version]
- Hori, M.; Matsuda, T.; Shibata, A.; Katanoda, K.; Sobue, T.; Nishimoto, H.; Japan Cancer Surveillance Research Group. Cancer incidence and incidence rates in Japan in 2009: A study of 32 population-based cancer registries for the Monitoring of Cancer Incidence in Japan (MCIJ) project. Jpn. J. Clin. Oncol. 2015, 45, 884–891. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics and Symptoms | Dyspepsia | Control | p Value | |||
|---|---|---|---|---|---|---|
| Meet the Rome Criteria (FD Group) | Do Not Meet the Rome Criteria (Non-FD Group) | |||||
| EPS | PDS | Overlap | ||||
| Patients (n) | 22 | 79 | 25 | 87 | 111 | |
| Age (years), mean ± SD | 54.0 ± 16.9 | 54.1 ± 14.6 | 55.3 ± 13.7 | 54.9 ± 12.1 | 54.4 ± 11.6 | 0.923 |
| Gender (n (% female)) | 14 (63.6) | 56 (70.9) | 16 (64.0) | 60 (68.8) | 74 (66.7) | 0.939 |
| BMI (kg/m2), mean ± SD | 21.5 ± 3.1 | 21.6 ± 4.2 | 21.1 ± 3.5 | 21.8 ± 3.2 | 22.8 ± 4.2 | 0.105 |
| Smoking (n (%)) | 4 (18.2) | 20 (25.3) | 5 (20.0) | 17 (19.5) | 32 (28.8) | 0.567 |
| Drinking (n (%)) | 7 (31.8) | 23 (29.1) | 6 (24.0) | 24 (28.6) | 43 (38.7) | 0.417 |
| After eradication of Helicobacter pylori (n (%)) | 5 (22.7) | 16 (20.3) | 7 (28.0) | 22 (26.0) | 29 (26.1) | 0.867 |
| Postprandial fullness (n (%)) | 0 | 48 (60.8) | 20 (80.0) | 32 (36.8) | 0 | |
| Early satiation (n (%)) | 0 | 41 (51.9) | 19 (76.0) | 24 (27.6) | 0 | |
| Epigastric pain or burning (n (%)) | 22 (100) | 30 (38.0) | 25 (100) | 31 (35.6) | 0 | |
| Postprandial epigastric pain or burning (n (%)) | 0 | 34 (43.0) | 0 | 17 (19.5) | 0 | |
| Characteristics | Meet the Rome Criteria | Do Not Meet the Rome Criteria | Control | p Value | ||
|---|---|---|---|---|---|---|
| FD Group | Group A | Group B | Group C | |||
| Patients (n) | 126 | 17 | 53 | 17 | 111 | |
| Age (years), mean ± SD | 54.3 ± 14.9 | 59.2 ± 11.6 | 54.8 ± 11.8 | 52.8 ± 14.0 | 54.4 ± 11.6 | 0.931 |
| Gender (n (% female)) | 86 (68.5) | 11 (64.7) | 34 (64.2) | 13 (76.5) | 74 (66.7) | 0.909 |
| BMI (kg/m2), mean ± SD | 21.8 ± 3.5 | 21.9 ± 3.2 | 21.7 ± 3.5 | 22.2 ± 3.2 | 22.8 ± 4.2 | 0.257 |
| Smoking (n (%)) | 29 (23.4) | 3 (17.6) | 14 (26.4) | 2 (11.8) | 32 (28.8) | 0.516 |
| Drinking (n (%)) | 36 (28.8) | 7 (41.1) | 17 (32.1) | 3 (17.6) | 43 (38.7) | 0.277 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mieno, M.; Tomita, T.; Aono, S.; Tozawa, K.; Nakai, K.; Okugawa, T.; Fukushima, M.; Oshima, T.; Fukui, H.; Miwa, H. Evaluation of QOL in Patients with Dyspeptic Symptoms Who Meet or Do Not Meet Rome IV Criteria. J. Clin. Med. 2022, 11, 21. https://doi.org/10.3390/jcm11010021
Mieno M, Tomita T, Aono S, Tozawa K, Nakai K, Okugawa T, Fukushima M, Oshima T, Fukui H, Miwa H. Evaluation of QOL in Patients with Dyspeptic Symptoms Who Meet or Do Not Meet Rome IV Criteria. Journal of Clinical Medicine. 2022; 11(1):21. https://doi.org/10.3390/jcm11010021
Chicago/Turabian StyleMieno, Masatoshi, Toshihiko Tomita, Sota Aono, Katsuyuki Tozawa, Keisuke Nakai, Takuya Okugawa, Masashi Fukushima, Tadayuki Oshima, Hirokazu Fukui, and Hiroto Miwa. 2022. "Evaluation of QOL in Patients with Dyspeptic Symptoms Who Meet or Do Not Meet Rome IV Criteria" Journal of Clinical Medicine 11, no. 1: 21. https://doi.org/10.3390/jcm11010021
APA StyleMieno, M., Tomita, T., Aono, S., Tozawa, K., Nakai, K., Okugawa, T., Fukushima, M., Oshima, T., Fukui, H., & Miwa, H. (2022). Evaluation of QOL in Patients with Dyspeptic Symptoms Who Meet or Do Not Meet Rome IV Criteria. Journal of Clinical Medicine, 11(1), 21. https://doi.org/10.3390/jcm11010021