
Efficacy of Low-Intensity Extracorporeal Shock Wave Treatment in Erectile Dysfunction Following Radical Prostatectomy: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria and Study Eligibility
- (1)
- Participants: Patients who underwent RP or radical cystoprostatectomy and had normal sexual function before surgery.
- (2)
- Interventions: Patients who underwent LI-ESWT for penile rehabilitation after the operation.
- (3)
- Comparators: Patients who did not receive LI-ESWT for penile rehabilitation after the operation.
- (4)
- Outcomes: Follow-up result of questionnaires that can evaluate erectile function (for example: International Index of Erectile Function (IIEF-5), Expanded Prostate Cancer Index Composite (EPIC), and Erection Hardness Score (EHS)).
- (5)
- Study design: No restriction on the study design so that both randomized controlled trials (RCTs) and observational studies could be included in the analysis.
2.3. Study Quality Assessments
2.4. Statistical Analysis
3. Results
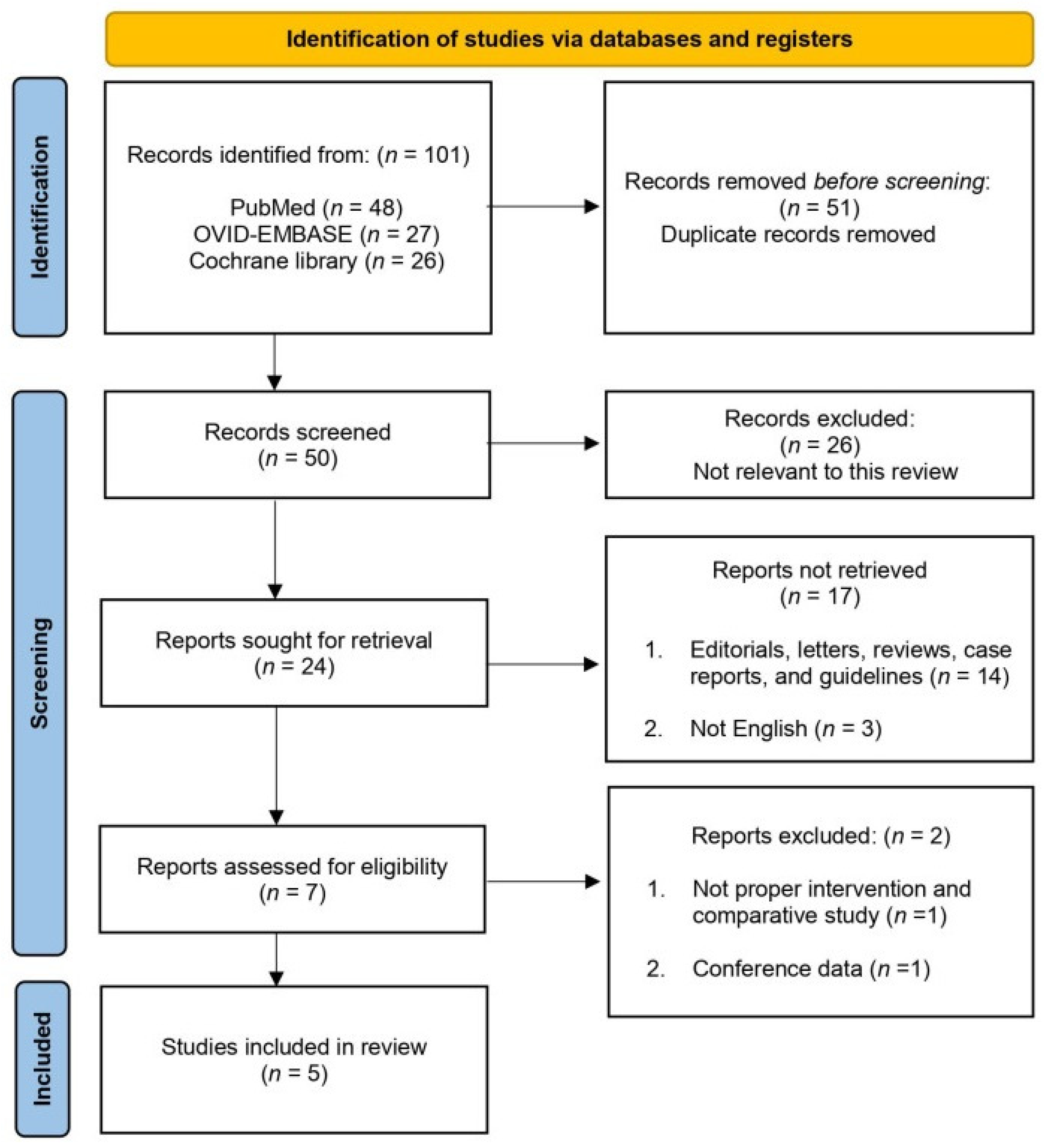
3.1. Systematic Review Process
3.2. Quality Assessment
3.3. IIEF-5 Questionnaire
3.3.1. A. RCT Studies
3.3.2. B. RCT and Non-RCT Studies
3.4. The Quality of Evidence Using the GRADE Approach
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
Abbreviations
| CI | Confidence intervals |
| EHS | Erection Hardness Score |
| ED | Erectile dysfunction |
| EPIC | Expanded Prostate Cancer Index Composite |
| IIEF | International Index of Erectile Function |
| LI-ESWT | Low-intensity extracorporeal shock wave treatment |
| NGF | Nerve growth factor |
| PDE5Is | Oral 5-phosphodiesterase inhibitors |
| RP | Radical prostatectomy |
| RCT | Randomized controlled trials |
| WMD | Weighted mean differences |
References
- Karakiewicz, P.I.; Tanguay, S.; Kattan, M.W.; Elhilali, M.M.; Aprikian, A.G. Erectile and urinary dysfunction after radical prostatectomy for prostate cancer in Quebec: A population-based study of 2415 men. Eur. Urol. 2004, 46, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Tal, R.; Alphs, H.H.; Krebs, P.; Nelson, C.J.; Mulhall, J.P. Erectile function recovery rate after radical prostatectomy: A meta-analysis. J. Sex. Med. 2009, 6, 2538–2546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, D.Y.; Song, K.M.; Choi, M.J.; Limanjaya, A.; Ghatak, K.; Ock, J.; Yin, G.N.; Hong, C.H.; Hong, S.S.; Suh, J.K.; et al. Neutralizing antibody to proNGF rescues erectile function by regulating the expression of neurotrophic and angiogenic factors in a mouse model of cavernous nerve injury. Andrology 2021, 9, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Salonia, A.; Burnett, A.L.; Graefen, M.; Hatzimouratidis, K.; Montorsi, F.; Mulhall, J.P.; Stief, C. Prevention and management of postprostatectomy sexual dysfunctions part 2: Recovery and preservation of erectile function, sexual desire, and orgasmic function. Eur. Urol. 2012, 62, 273–286. [Google Scholar] [CrossRef]
- Sharifi, N.; Gulley, J.L.; Dahut, W.L. Androgen deprivation therapy for prostate cancer. JAMA 2005, 294, 238–244. [Google Scholar] [CrossRef]
- Bratu, O.; Oprea, I.; Marcu, D.; Spinu, D.; Niculae, A.; Geavlete, B.; Mischianu, D. Erectile dysfunction post-radical prostatectomy—A challenge for both patient and physician. J. Med. Life 2017, 10, 13–18. [Google Scholar]
- Martinez-Jabaloyas, J.M.; Gil-Salom, M.; Villamon-Fort, R.; Pastor-Hernandez, F.; Martinez-Garcia, R.; Garcia-Sisamon, F. Prognostic factors for response to sildenafil in patients with erectile dysfunction. Eur. Urol. 2001, 40, 641–646. [Google Scholar] [CrossRef]
- Manfredi, C.; Fortier, E.; Faix, A.; Martinez-Salamanca, J.I. Penile Implant Surgery Satisfaction Assessment. J. Sex. Med. 2021, 18, 868–874. [Google Scholar] [CrossRef]
- Otero, J.R.; Manfredi, C.; Wilson, S.K. The good, the bad, and the ugly about surgical approaches for inflatable penile prosthesis implantation. Int. J. Impot. Res. 2022, 34, 128–137. [Google Scholar] [CrossRef]
- Althof, S.E. Quality of life and erectile dysfunction. Urology 2002, 59, 803–810. [Google Scholar] [CrossRef]
- Boni, A.; Cochetti, G.; Del Zingaro, M.; Paladini, A.; Turco, M.; Rossi de Vermandois, J.A.; Mearini, E. Uroflow stop test with electromyography: A novel index of urinary continence recovery after RARP. Int. Urol. Nephrol. 2019, 51, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Gruenwald, I.; Appel, B.; Kitrey, N.D.; Vardi, Y. Shockwave treatment of erectile dysfunction. Ther. Adv. Urol. 2013, 5, 95–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porst, H. Review of the Current Status of Low Intensity Extracorporeal Shockwave Therapy (Li-ESWT) in Erectile Dysfunction (ED), Peyronie’s Disease (PD), and Sexual Rehabilitation After Radical Prostatectomy With Special Focus on Technical Aspects of the Different Marketed ESWT Devices Including Personal Experiences in 350 Patients. Sex. Med. Rev. 2021, 9, 93–122. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.Y.; Zhong, D.L.; Li, J.; Jin, R.J. The effectiveness and safety of extracorporeal shock wave therapy (ESWT) on spasticity after upper motor neuron injury: A protocol of systematic review and meta-analysis. Medicine 2020, 99, e18932. [Google Scholar] [CrossRef]
- Martinez-Sanchez, C.; Azar-Manzur, F.; Gonzalez-Pacheco, H.; Amezcua-Guerra, L.M.; Masso, F.; Marquez-Velasco, R.; Bojalil, R.; Carvajal-Juarez, I.; Alexanderson-Rosas, E.; Hernandez, S.; et al. Effectiveness and Safety of Extracorporeal Shockwave Myocardial Revascularization in Patients With Refractory Angina Pectoris and Heart Failure. Am. J. Cardiol. 2021, 144, 26–32. [Google Scholar] [CrossRef]
- Wang, C.J. Extracorporeal shockwave therapy in musculoskeletal disorders. J. Orthop. Surg. Res. 2012, 7, 11. [Google Scholar] [CrossRef] [Green Version]
- Lu, Z.; Lin, G.; Reed-Maldonado, A.; Wang, C.; Lee, Y.C.; Lue, T.F. Low-intensity Extracorporeal Shock Wave Treatment Improves Erectile Function: A Systematic Review and Meta-Analysis. Eur. Urol. 2017, 71, 223–233. [Google Scholar] [CrossRef]
- Sokolakis, I.; Hatzichristodoulou, G. Clinical studies on low intensity extracorporeal shockwave therapy for erectile dysfunction: A systematic review and meta-analysis of randomised controlled trials. Int. J. Impot. Res. 2019, 31, 177–194. [Google Scholar] [CrossRef]
- Baccaglini, W.; Pazeto, C.L.; Correa Barros, E.A.; Timoteo, F.; Monteiro, L.; Saad Rached, R.Y.; Navas, A.; Glina, S. The Role of the Low-Intensity Extracorporeal Shockwave Therapy on Penile Rehabilitation After Radical Prostatectomy: A Randomized Clinical Trial. J. Sex. Med. 2020, 17, 688–694. [Google Scholar] [CrossRef]
- Frey, A.; Sonksen, J.; Fode, M. Low-intensity extracorporeal shockwave therapy in the treatment of postprostatectomy erectile dysfunction: A pilot study. Scand. J. Urol. 2016, 50, 123–127. [Google Scholar] [CrossRef]
- Inoue, S.; Hayashi, T.; Teishima, J.; Matsubara, A. Effect of penile rehabilitation with low intensity extracorporeal shock wave therapy on erectile function recovery following robot-assisted laparoscopic prostatectomy. Transl. Androl. Urol. 2020, 9, 1559–1565. [Google Scholar] [CrossRef] [PubMed]
- Karakose, A.; Yitgin, Y. Penile rehabilitation with low-intensity extracorporeal shock wave therapy in patients after prostate cancer surgery. Early physiological changes and postoperative follow-up outcomes. Int. J. Clin. Pract. 2021, 75, e14804. [Google Scholar] [CrossRef] [PubMed]
- Ladegaard, P.B.J.; Mortensen, J.; Skov-Jeppesen, S.M.; Lund, L. Erectile Dysfunction A Prospective Randomized Placebo-Controlled Study Evaluating the Effect of Low-Intensity Extracorporeal Shockwave Therapy (LI-ESWT) in Men With Erectile Dysfunction Following Radical Prostatectomy. Sex. Med. 2021, 9, 100338. [Google Scholar] [CrossRef] [PubMed]
- Zewin, T.S.; El-Assmy, A.; Harraz, A.M.; Bazeed, M.; Shokeir, A.A.; Sheir, K.; Mosbah, A. Efficacy and safety of low-intensity shock wave therapy in penile rehabilitation post nerve-sparing radical cystoprostatectomy: A randomized controlled trial. Int. Urol. Nephrol. 2018, 50, 2007–2014. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schunemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Melsen, W.G.; Bootsma, M.C.; Rovers, M.M.; Bonten, M.J. The effects of clinical and statistical heterogeneity on the predictive values of results from meta-analyses. Clin. Microbiol. Infect. 2014, 20, 123–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenland, S.; Senn, S.J.; Rothman, K.J.; Carlin, J.B.; Poole, C.; Goodman, S.N.; Altman, D.G. Statistical tests, P values, confidence intervals, and power: A guide to misinterpretations. Eur. J. Epidemiol. 2016, 31, 337–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (Updated February 2021), 2021. Cochrane. Available online: https://training.cochrane.org/handbook/current (accessed on 31 May 2021).
- Aicher, A.; Heeschen, C.; Sasaki, K.; Urbich, C.; Zeiher, A.M.; Dimmeler, S. Low-energy shock wave for enhancing recruitment of endothelial progenitor cells: A new modality to increase efficacy of cell therapy in chronic hind limb ischemia. Circulation 2006, 114, 2823–2830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, Y.; Ito, K.; Shiroto, T.; Tsuburaya, R.; Yi, G.J.; Takeda, M.; Fukumoto, Y.; Yasuda, S.; Shimokawa, H. Cardiac shock wave therapy ameliorates left ventricular remodeling after myocardial ischemia-reperfusion injury in pigs in vivo. Coron. Artery Dis. 2010, 21, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Guo, T.; Ma, T.K.; Cai, H.Y.; Tao, S.M.; Peng, Y.Z.; Yang, P.; Chen, M.Q.; Gu, Y. A modified regimen of extracorporeal cardiac shock wave therapy for treatment of coronary artery disease. Cardiovasc. Ultrasound 2012, 10, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vardi, Y.; Appel, B.; Jacob, G.; Massarwi, O.; Gruenwald, I. Can low-intensity extracorporeal shockwave therapy improve erectile function? A 6-month follow-up pilot study in patients with organic erectile dysfunction. Eur. Urol. 2010, 58, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Yee, C.H.; Chan, E.S.; Hou, S.S.; Ng, C.F. Extracorporeal shockwave therapy in the treatment of erectile dysfunction: A prospective, randomized, double-blinded, placebo controlled study. Int. J. Urol. 2014, 21, 1041–1045. [Google Scholar] [CrossRef]
- Campbell, J.D.; Trock, B.J.; Oppenheim, A.R.; Anusionwu, I.; Gor, R.A.; Burnett, A.L. Meta-analysis of randomized controlled trials that assess the efficacy of low-intensity shockwave therapy for the treatment of erectile dysfunction. Ther. Adv. Urol. 2019, 11, 1756287219838364. [Google Scholar] [CrossRef]
- Li, H.; Matheu, M.P.; Sun, F.; Wang, L.; Sanford, M.T.; Ning, H.; Banie, L.; Lee, Y.C.; Xin, Z.; Guo, Y.; et al. Low-Energy Shock Wave Therapy Ameliorates Erectile Dysfunction in a Pelvic Neurovascular Injuries Rat Model. J. Sex. Med. 2016, 13, 22–32. [Google Scholar] [CrossRef] [Green Version]
- Fode, M.; Hatzichristodoulou, G.; Serefoglu, E.C.; Verze, P.; Albersen, M.; Young Academic Urologists Men’s Health Group. Low-intensity shockwave therapy for erectile dysfunction: Is the evidence strong enough? Nat. Rev. Urol. 2017, 14, 593–606. [Google Scholar] [CrossRef]
- Fuchs, S.; Dohle, E.; Kolbe, M.; Kirkpatrick, C.J. Outgrowth endothelial cells: Sources, characteristics and potential applications in tissue engineering and regenerative medicine. Adv. Biochem. Eng. Biotechnol. 2010, 123, 201–217. [Google Scholar] [CrossRef] [PubMed]
- Qiu, X.; Lin, G.; Xin, Z.; Ferretti, L.; Zhang, H.; Lue, T.F.; Lin, C.S. Effects of low-energy shockwave therapy on the erectile function and tissue of a diabetic rat model. J. Sex. Med. 2013, 10, 738–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagoda, G.; Xie, Y.; Sezen, S.F.; Hurt, K.J.; Liu, L.M.; Musicki, B.; Burnett, A.L. FK506 Neuroprotection After Cavernous Nerve Injury is Mediated by Thioredoxin and Glutathione Redox Systems. J. Sex. Med. 2011, 8, 3325–3334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryu, J.K.; Suh, J.K.; Burnett, A.L. Research in pharmacotherapy for erectile dysfunction. Transl. Androl. Urol. 2017, 6, 207–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, E.; Cartmill, R. Evaluation of clinical efficacy, safety and patient satisfaction rate after low-intensity extracorporeal shockwave therapy for the treatment of male erectile dysfunction: An Australian first open-label single-arm prospective clinical trial. BJU Int. 2015, 115 (Suppl. S5), 46–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulakis, V.; Skriapas, K.; de Vries, R.; Dillenburg, W.; Ferakis, N.; Witzsch, U.; Melekos, M.; Becht, E. Extracorporeal shockwave therapy for Peyronie’s disease: An alternative treatment? Asian J. Androl. 2006, 8, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Goertz, O.; Lauer, H.; Hirsch, T.; Ring, A.; Lehnhardt, M.; Langer, S.; Steinau, H.U.; Hauser, J. Extracorporeal shock waves improve angiogenesis after full thickness burn. Burns 2012, 38, 1010–1018. [Google Scholar] [CrossRef]
- Ioppolo, F.; Rompe, J.D.; Furia, J.P.; Cacchio, A. Clinical application of shock wave therapy (SWT) in musculoskeletal disorders. Eur. J. Phys. Rehabil. Med. 2014, 50, 217–230. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Authors Year Country | Study Design | Study Summary | Total Patients | Setup of LI-ESWT | Protocol of LI-ESWT Treatment | Follow-Up (months) | Evaluation Tools for ED | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Higher Energy Flux Density (mJ/mm2) | Total Pulses /Each Treatment | Pulses /Each Region | No. of Treatments Each Week | No. of Sites | Total Course of Treatment (Weeks) | |||||||
| Zewin et al. 2018 Egypt | Randomized Clinical Trial | Comparison of penile rehabilitation with or without LI-ESWT after cystoprostatectomy (PDE5Is not used concurrently) | Control | 43 | 0.09 | 1500 | 300 | 2 | 5 | 6 | 1, 3, 6, 9 | IIEF EHS |
| LI-ESWT | 42 | |||||||||||
| Baccaglini et al. 2020 Brazil | Randomized Clinical Trial | Comparison of penile rehabilitation with or without LI-ESWT after prostatectomy (PDE5Is used concurrently) | Control | 41 | 0.09 | 2400 | 600 | 2 | 4 | 8 | 4 | IIEF-5 |
| LI-ESWT | 36 | |||||||||||
| Inoue et al. 2020 Japan | Non-Randomized Clinical Trial | Comparison of penile rehabilitation with or without LI-ESWT after prostatectomy (PDE5Is used concurrently) | Control | 16 | 0.09 | 1500 | 300 | 1 | 5 | 6 | 3, 6, 9, 12 | EPIC |
| LI-ESWT | 178 | |||||||||||
| Karakose et al. 2021 Turkey | Non-Randomized Clinical Trial | Comparison of penile rehabilitation with or without LI-ESWT after prostatectomy (PDE5Is used concurrently) | Control | 32 | 0.09 | 1500 | 300 | 2 | 5 | 6 | 3, 6, 12 | IIEF-5 |
| LI-ESWT | 34 | |||||||||||
| Ladegaard et al. 2021 Denmark | Randomized Clinical Trial | Comparison of penile rehabilitation with or without LI-ESWT after prostatectomy (PDE5Is used concurrently) | Control | 18 | 0.15 | 4000 | 500 | 1 | 6 (twice of each of the penile crurae) | 5 | 1, 3 | IIEF-5 EHS |
| LI-ESWT | 20 | |||||||||||
| A. Results of Quality Assessment of Randomized Control Trial Study by the Cochrane Risk-of-Bias Tool | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Author(s) (Year) | Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personnel (Performance Bias) | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data Addressed (Attrition Bias) | Selective Reporting (Reporting Bias) | Other Bias | ||
| Zewin et al. (2018) [24] | Low risk | Low risk | High risk | High risk | Low risk | Low risk | Unclear | ||
| Baccaglini et al. (2020) [19] | Low risk | Low risk | High risk | High risk | Low risk | Low risk | Unclear | ||
| Ladegaard et al. (2020) [23] | Low risk | Low risk | High risk | High risk | Low risk | Low risk | Unclear | ||
| B. Results of Quality Assessment of Nonrandomized Studies by the Newcastle–Ottawa Scale | |||||||||
| Author(s) (Year) | Selection (4) | Comparability (2) | Exposure (3) | Total Score | |||||
| Adequate Definition of Cases | Representativeness of Cases | Selection of Controls | Definition of Controls | Control for Important Factor or Additional Factor | Ascertainment of Exposure | Same Method of Ascertainment for Cases and Controls | Non-Response Rate | ||
| Inoue et al. (2020) [21] | 1 | 1 | 0 | 1 | 2 | 1 | 1 | 0 | 7 |
| Karakose et al. (2021) [22] | 1 | 1 | 0 | 1 | 2 | 1 | 1 | 0 | 7 |
| Certainty Assessment | Number of Patients | Effect | Certainty | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Control | LI-ESWT | Mean Difference (95% CI) | |
| IIEF 3–4 Months after LI-ESWT | ||||||||||
| 3 | RCTs | not serious | serious a | not serious | serious b | none | 102 | 98 | −2.04 (−3.7, −0.35) | Low |
| IIEF 9–12 Months after LI-ESWT | ||||||||||
| 1 | RCT | Single study data | 43 | 42 | −1.80 (−2.54, −0.35) | |||||
| IIEF 3–4 Months after LI-ESWT | ||||||||||
| 4 | RCTs (3) + observational study (1) | not serious | serious a | not serious | serious b | none | 212 | 191 | −3.14 (−5.73, −0.55) | Very low |
| IIEF 9–12 Months after LI-ESWT | ||||||||||
| 2 | RCTs (3) + observational study (1) | not serious | serious a | not serious | serious b | none | 212 | 191 | −5.37 (−12.42, −1.69) | Very low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rho, B.Y.; Kim, S.H.; Ryu, J.-K.; Kang, D.H.; Kim, J.W.; Chung, D.Y. Efficacy of Low-Intensity Extracorporeal Shock Wave Treatment in Erectile Dysfunction Following Radical Prostatectomy: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 2775. https://doi.org/10.3390/jcm11102775
Rho BY, Kim SH, Ryu J-K, Kang DH, Kim JW, Chung DY. Efficacy of Low-Intensity Extracorporeal Shock Wave Treatment in Erectile Dysfunction Following Radical Prostatectomy: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(10):2775. https://doi.org/10.3390/jcm11102775
Chicago/Turabian StyleRho, Beom Yong, Si Hyeon Kim, Ji-Kan Ryu, Dong Hyuk Kang, Jong Won Kim, and Doo Yong Chung. 2022. "Efficacy of Low-Intensity Extracorporeal Shock Wave Treatment in Erectile Dysfunction Following Radical Prostatectomy: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 10: 2775. https://doi.org/10.3390/jcm11102775