
Alexithymia, Phosphorus Levels, and Sleep Disorders in Patients on Hemodialysis
Abstract
:1. Introduction
2. Materials and Methods
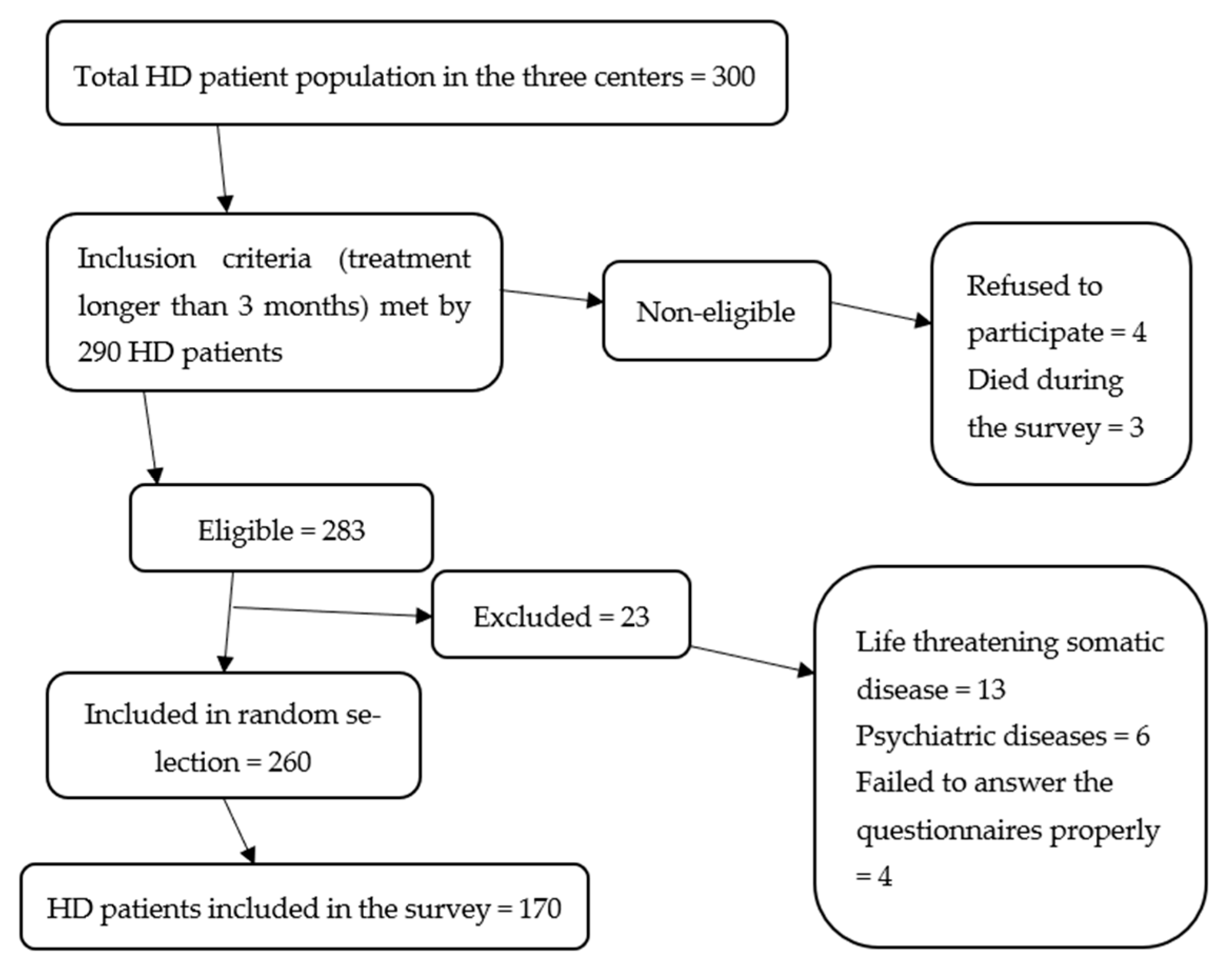
2.1. Participants
2.2. Selection Criteria for Participants in the Study
2.3. Evaluated Variables and Methods
2.4. Statistical Methods
3. Results
3.1. Basic Characteristics of the Participants
3.2. Alexithymia (TAS 26 Scale)
3.3. Sleep Quality (PSQI Questionnaire)
3.4. Epworth’s Daytime Sleepiness Scale
3.5. Levels of Depression (Hamilton Depression Rating Scale)
3.6. Correlation of Interdialytic Weight Gain, Blood Pressure, and Biochemical Indicators with Daytime Sleepiness
3.7. Correlation of Pittsburgh Sleep Quality Index (PSQI) with Biochemical Indicators and Depression
3.8. Correlation of Alexithymia with Factors of Inflammation, Sleep Quality, Daytime Sleepiness, and Depression
3.9. Influence of Individual Factors (Predictors) on Serum Phosphorus Levels and Daytime Sleepiness (Regression Analysis)
4. Discussion
5. Limitations and Lack of Studies
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ammirati, A.L. Chronic kidney disease. Rev. Assoc. Med. Bras. 2020, 66, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Khou, V.; De La Mata, N.L.; Morton, R.L.; Kelly, P.J.; Webster, A.C. Cause of death for people with end-stage kidney disease withdrawing from treatment in Australia and New Zealand. Nephrol. Dial. Transplant. 2020, 105, 1527–1537. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.K.; Ahmad, S.; Allon, M. Handbook of Dialysis; Wolters Kluwer Health: Philadelphia, PA, USA, 2015; ISBN 9781451144291. [Google Scholar]
- Arbor, A.; Oaks, T. Health-related quality of life among dialysis patients on three continents: The dialysis outcomes and practice patterns study. Kidney Int. 2003, 64, 1903–1910. [Google Scholar]
- Chen, S.S.; Al Mawed, S.; Unruh, M. Health-Related Quality of Life in End-Stage Renal Disease Patients: How Often Should We Ask and What Do We Do with the Answer? Blood Purif. 2016, 41, 218–224. [Google Scholar] [CrossRef]
- Shen, Q.; Huang, X.; Luo, Z.; Xu, X.; Zhao, X.; He, Q. Sleep quality, daytime sleepiness and health-related quality-of-life in maintenance haemodialysis patients. J. Int. Med. Res. 2016, 44, 698–709. [Google Scholar] [CrossRef] [Green Version]
- Sinatra, M.; Curci, A.; de Palo, V.; Monacis, L.; Tanucci, G. How Dialysis Patients Live: A Study on Their Depression and Associated Factors in Southern Italy. Psychology 2011, 02, 969–977. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- De Santo, R.M.; Livrea, A.; De Santo, N.G.; Conzo, G.; Bilancio, G.; Celsi, S.; Cirillo, M. The High Prevalence of Alexithymia in Hemodialyzed Patients with Secondary Hyperparathyroidism Unsuppressed by Medical Therapy Is Cured by Parathyroidectomy. J. Ren. Nutr. 2010, 20, 64–70. [Google Scholar] [CrossRef]
- Parker, K.P.; Bliwise, N.L.; Bailey, J.L.; Rye, D.B. Daytime sleepiness in stable hemodialysis patients. Am. J. Kidney Dis. 2003, 41, 394–402. [Google Scholar] [CrossRef]
- Fukunishi, I. Psychosomatic aspects of patients on hemodialysis. 2. Alexithymic trait of hemodialysis patients with diabetic nephropathy. Psychother. Psychosom. 1989, 52, 58–65. [Google Scholar] [CrossRef]
- Liakopoulos, V.; Roumeliotis, S.; Gorny, X.; Dounousi, E.; Mertens, P.R. Review article oxidative stress in hemodialysis patients: A review of the literature. Oxid. Med. Cell. Longev. 2017, 2017, 1–22. [Google Scholar]
- Hu, A.; Xue, Z.; Mwansisya, T.; Zhou, A.; Pu, W.; Chen, X.; Sun, M.; Wang, P.; Fan, H.; Wang, Z.; et al. Major depressive disorder in hemodialysis patients in China. Asia-Pacific Psychiatry 2015, 7, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Wittenborn, A.K.; Rahmandad, H.; Rick, J.; Hosseinichimeh, N. Depression as a systemic syndrome: Mapping the feedback loops of major depressive disorder. Psychol. Med. 2016, 46, 551–562. [Google Scholar] [CrossRef] [PubMed]
- Kojima, M.; Hayano, J.; Suzuki, S.; Seno, H.; Kasuga, H.; Takahashi, H.; Toriyama, T.; Kawahara, H.; Furukawa, T.A. Depression, Alexithymia and Long-Term Mortality in Chronic Hemodialysis Patients. Psychother. Psychosom. 2010, 79, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Firoz, M.N.; Shafipour, V.; Jafari, H.; Hosseini, S.H.; Charati, J.Y. Sleep Quality and Depression and Their Association with Other Factors in Hemodialysis Patients. Glob. J. Health Sci. 2016, 8, 121–127. [Google Scholar] [CrossRef]
- Parker, K.P.; Kutner, N.G.; Bliwise, D.L.; Bailey, J.L.; Rye, D.B. Nocturnal sleep, daytime sleepiness, and quality of life in stable patients on hemodialysis. Health Qual. Life Outcomes 2003, 1, 68. [Google Scholar] [CrossRef] [Green Version]
- Gencdal, Y. Subjective sleep quality and excessive daytime sleepiness in hemodialysis patients waitlisted for renal transplant. Cogn. Behav. Neurol. 2019, 32, 25–30. [Google Scholar] [CrossRef]
- Akyüz, O.; Parmaks, E. Ardahanl Investigation of the Relationship Between Biochemical Parameters, Alexithymia and Stress Levels in Hemodialysis Patients. South. Clin. Istanb. Eurasia 2021, 32, 13–18. [Google Scholar] [CrossRef]
- Tayaz, E.; Koç, A. Influence of Selected Biomarkers on Stress and Alexithymia in Patients Under Hemodialysis Treatment. Yonago Acta Med. 2019, 62, 285–292. [Google Scholar] [CrossRef] [Green Version]
- Cozzolino, M.; Mangano, M.; Stucchi, A.; Ciceri, P.; Conte, F.; Galassi, A. Cardiovascular disease in dialysis patients. Nephrol. Dial. Transplant. 2018, 33, iii28–iii34. [Google Scholar] [CrossRef]
- Helmers, K.F.; Mente, A. Alexithyimia and health behaviors in healthy male volunteers. J. Psychosom. Res. 1999, 47, 635–645. [Google Scholar] [CrossRef]
- Wasse, H.; Kutner, N.; Zhang, R.; Huang, Y. Association of Initial Hemodialysis Vascular Access with Patient-Reported Health Status and Quality of Life. Clin. J. Am. Soc. Nephrol. 2007, 2, 708–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khezri, H.D.; Baradari, A.G.; Espahbodi, F.; Jannati, Y.; Lesani, M.; Yaghoubi, T.; Zeydi, A.E. Sleep quality and its correlation with serum c-reactive protein level in hemodialysis patients. Saudi J. Kidney Dis. Transplant. 2014, 25, 750–755. [Google Scholar] [CrossRef] [PubMed]
- Gençöz, F.; Gencoz, T.; Soykan, A. Psychometric properties of the Hamilton Depression Rating Scale and other physician-rated psychiatric scales for the assessment of depression in ESRD patients undergoing hemodialysis in Turkey. Psychol. Health Med. 2007, 12, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Afsar, B.; Elsurer, R. The Relationship Between Sleep Quality and Daytime Sleepiness and Various Anthropometric Parameters in Stable Patients Undergoing Hemodialysis. J. Ren. Nutr. 2013, 23, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Lovko, S.K.; Gelo, J.; Karlović, D. Validation study of Toronto Alexithymia Scale (TAS-26) in Croatian population. Acta Clin. Croat. 2015, 54, 272–278. [Google Scholar]
- Taylor, G.J.; Bagby, R.M.; Ryan, D.P.; Parker, J.D.; Doody, K.F.; Keefe, P. Criterion validity of the Toronto Alexithymia Scale. Psychosom. Med. 1988, 50, 500–509. [Google Scholar] [CrossRef]
- Armitage, P.; Berry, G.; Matthews, J.N.S.; Methods, S. Statistical Methods in Medical Research; John Wiley & Sons: Hoboken, NJ, USA, 2003; ISBN 0632052570. [Google Scholar]
- Onor, M.; Trevisiol, M.; Spano, M.; Aguglia, E.; Paradiso, S. Alexithymia and aging: A neuropsychological perspective. J. Nerv. Ment. Dis. 2013, 198, 891–895. [Google Scholar] [CrossRef] [Green Version]
- Besharat, M.A.; Shahidi, S. What is the relationship between alexithymia and ego defense styles? A correlational study with Iranian students. Asian J. Psychiatry 2011, 4, 145–149. [Google Scholar] [CrossRef]
- Guilbaud, O.; Corcos, M.; Hjalmarsson, L.; Loas, G.; Jeammet, P. Is there a psychoneuroimmunological pathway between alexithymia and immunity? Immune and physiological correlates of alexithymia. Biomed. Pharmacother. 2003, 57, 292–295. [Google Scholar] [CrossRef]
- Chiu, Y.-L.; Chuang, Y.-F.; Fang, K.-C.; Liu, S.-K.; Chen, H.-Y.; Yang, J.-Y.; Pai, M.-F.; Peng, Y.-S.; Wu, K.-D.; Tsai, T.-J. Higher systemic inflammation is associated with poorer sleep quality in stable haemodialysis patients. Nephrol. Dial. Transplant. 2009, 24, 247–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taraz, M.; Khatami, M.-R.; Dashti-Khavidaki, S.; Akhonzadeh, S.; Noorbala, A.-A.; Ghaeli, P.; Taraz, S. Sertraline decreases serum level of interleukin-6 (IL-6) in hemodialysis patients with depression: Results of a randomized double-blind, placebo-controlled clinical trial. Int. Immunopharmacol. 2013, 17, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Afsar, B. The Relationship of Serum Cortisol Levels with Depression, Cognitive Function and Sleep Disorders in Chronic Kidney Disease and Hemodialysis Patients. Psychiatr. Q. 2014, 85, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Strüber, N.; Strüber, D.; Roth, G. Impact of early adversity on glucocorticoid regulation and later mental disorders. Neurosci. Biobehav. Rev. 2014, 38, 17–37. [Google Scholar] [CrossRef]
- Han, B.; Zhu, F.-X.; Shi, C.; Wu, H.-L.; Gu, X.-H. Association between Serum Vitamin D Levels and Sleep Disturbance in Hemodialysis Patients. Nutrients 2017, 9, 139. [Google Scholar] [CrossRef] [Green Version]
- Nguyen-Khoa, T.; Massy, Z.A.; De Bandt, J.P.; Kebede, M.; Salama, L.; Lambrey, G.; Witko-Sarsat, V.; Drueke, T.B.; Lacour, B.; Thévenin, M. Oxidative stress and haemodialysis: Role of inflammation and duration of dialysis treatment. Nephrol. Dial. Transplant. 2001, 16, 335–340. [Google Scholar] [CrossRef]
- Tenhouten, D.; Bogen, E.; Hoppe, D. Alexithymia- an experimental study of cerebral commissurotomy patients and normal control subjects. Am. J. Psychiatry 1986, 143, 312–316. [Google Scholar]
- Alessandro, C.D.; Piccoli, G.B.; Cupisti, A. The “phosphorus pyramid ”: A visual tool for dietary phosphate management in dialysis and CKD patients. BMC Nephrol. 2015, 16, 1–6. [Google Scholar]
- Oliver, G.; Wardle, J.; Gibson, E.L. Stress and Food Choice: A Laboratory Study. Psychosom. Med. 2000, 62, 853–865. [Google Scholar] [CrossRef]
- Lumley, M.A.; Norman, S. Alexithymia and Health Care Utilization. Psychosom. Med. 1996, 58, 197–202. [Google Scholar] [CrossRef]
- Carrozzino, D.; Porcelli, P. Alexithymia in Gastroenterology and Hepatology: A Systematic Review. Front. Psychol. 2018, 9, 470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukunishi, I. Alexithymic characteristics of bulimia nervosa in diabetes mellitus with end-stage renal disease. Psychol. Rep. 1997, 81, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, A.; Bhatt, N.; Rossetti, S.; Beto, J. Management of Hyperphosphatemia in End-Stage Renal Disease: A New Paradigm. J. Ren. Nutr. 2021, 31, 21–34. [Google Scholar] [CrossRef]
- Hanly, P. Sleep Apnea and Daytime Sleepiness in End-Stage Renal Disease. Semin. Dial. 2004, 17, 109–114. [Google Scholar] [CrossRef]
- Roumelioti, M.-E.; Brown, L.K.; Unruh, M.L. The Relationship Between Volume Overload in End-Stage Renal Disease and Obstructive Sleep Apnea. Semin. Dial. 2015, 28, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Fukunishi, I.; Yamasaki, Y.; Fukui, T.; Sei, H.; Morita, Y.; Tatemischi, T.; Horiguchi, E. Sleep characteristics of Japaneese working men who scores alexithymic on the Toronto Alexithymia Scale. Percept. Mot. Skills 1997, 84, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Bazydlo, R.; Lumley, M.A.; Roehrs, T. Alexithymia and Polysomnographic Measures of Sleep in Healthy Adults. Psychosom. Med. 2001, 63, 56–61. [Google Scholar] [CrossRef]
- He, S.; Zhu, J.; Jiang, W.; Ma, J.; Li, G.; He, Y. Sleep disturbance, negative affect and health-related quality of life in patients with maintenance hemodialysis. Psychol. Health Med. 2019, 24, 294–304. [Google Scholar] [CrossRef]


{kind=link}
| Median (Interquartile Range) | Minimum–Maximum | |
|---|---|---|
| Difficulty describing feelings | 15 (11–18) | 5–34 |
| Difficulty identifying feelings | 28 (22–38) | 7–58 |
| Externally oriented thinking | 12 (10–16) | 3–32 |
| Reduced daydreaming | 15 (12–18.75) | 8–22 |
| Total Toronto Alexithymia Scale 26 | 68 (62–77) | 27–114 |
| Median (Interquartile Range) According to TAS 26 | Difference % | 95% Confidence Interval | p * | ||
|---|---|---|---|---|---|
| Up to 62 points | Above 63 points | ||||
| Age of participants | 54.5 (46–61) | 73 (66–80) | −2 | −7 to 2 | 0.318 |
| Arithmetic Mean (Standard Deviation) | Difference % | 95% Confidence Interval | p * | ||
|---|---|---|---|---|---|
| Men | Women | ||||
| Levels of alexithymia | 69.38 (14.87) | 68.04 (15.41) | 1.33 | −3.59 to 6.26 | 0.594 |
| Median (Interquartile Range) | Minimum–Maximum | |
|---|---|---|
| Total points on the sleep scale (PSQI) | 6 (4–10) | 0–21 |
| Sleep latency | 1 (1–2) | 0–3 |
| Duration of a sleep | 1 (0–2) | 0–3 |
| Number (%) of Participants | |
|---|---|
| Up to 10 | 124 (72.9) |
| 11 or more (high daytime sleepiness) | 35 (20.9) |
| Total | 159 (93.5) |
| Median (Interquartile Range) According to the Epworth Scale | Difference % | 95% Confidence Interval | p * | ||
|---|---|---|---|---|---|
| Up to 10 | Up to 10 | ||||
| Interdialytic weight gain | 0.0149 (0.0099–0.0196) | 0.0124 (0.0099–0.0158) | −0.003 | −0.005 to 0 | 0.05 |
| Systolic blood pressure (mmHg) | 137 (121–146) | 137 (127–146) | 3 | −5 to 10 | 0.49 |
| Diastolic blood pressure (mmHg) | 78 (70–81) | 77 (73–81) | 0 | −3.3 to 3.3 | 0.92 |
| Median (Interquartile Range) According to PSQI § | Difference % | 95% Confidence Interval | p * | ||
|---|---|---|---|---|---|
| Good Sleepers | Bad Sleepers | ||||
| CRP | 2.8 (1–5.8) | 5.6 (2.2–10.6) | 1.6 | 0.18 to 3.76 | 0.02 |
| Leukocytes | 6.3 (4.85–7.3) | 6.5 (5.2–8.33) | 0.6 | −0.1 to 1.3 | 0.11 |
| Depression (HDRS) | 4 (3–6.5) | 9 (5–14) | −5 | −7 to −2 | 0.00 |
| Median (Interquartile Range) Based on Alexithymia | Difference % | 95% Confidence Interval | p * | ||
|---|---|---|---|---|---|
| Without Alexithymia (n = 45) | With Alexithymia (n = 109) | ||||
| Age (years) | 66.5 (53–72) | 67 (59–75) | 2 | −2 to 7 | 0.32 |
| Interdialytic weight gain | 0.0128 (0.009–0.0185) | 0.0146 (0.01–0.0191) | 0.001 | −0.002 to 0.004 | 0.39 |
| CRP | 5.2 (1.5–10.8) | 4.05 (1.8–9.8) | −0.29 | −2.1 to 1.1 | 0.62 |
| Leukocytes | 5.9 (4.1–7.4) | 6.5 (5.4–8.2) | 0.9 | 0.2 to 1.6 | 0.02 |
| Pre-HD phosphorus | 1.71 (1.38–2.09) | 1.45 (1.13–1.77) | −0.27 | −0.44 to −0.08 | 0.005 |
| Subjective sleep quality (PSQI §) | 1 (0.75–1) | 1 (1–2) | 0 | 0 to 0 | 0.10 |
| Sleep latency | 1 (1–2) | 1 (1–2) | 0 | 0 to 0 | 0.437 |
| Duration of a sleep | 1 (0–2) | 1 (0–2) | 0 | 0 to 1 | 0.316 |
| Epworth Sleepiness Scale | 4 (3–6) | 8 (4–11) | 3 | 1 to 4 | 0.001 |
| Depression (HDRS $) | 5 (3–10) | 8 (4–15) | −3 | −6 to −1 | 0.01 |
| Bivariate Linear Regression | ||||
|---|---|---|---|---|
| ß * | 95% CI % ß | p | R2 | |
| Pre-HD phosphorus | ||||
| Alexithymia | −0.01 | −0.01 to −0.004 | 0.001 | 0.079 |
| Predictive Factors | ß * | Standard Error | Wald | Odds Ratio (OR) | 95% Confidence Interval | p |
|---|---|---|---|---|---|---|
| Bivariate Regression | ||||||
| Age | 0.001 | 0.015 | 0.01 | 1.01 | 0.97 to 1.03 | 0.94 |
| Gender | 0.286 | 0.401 | 0.509 | 1.33 | 0.60 to 2.92 | 0.48 |
| Interdialytic weight gain | −65.74 | 29.75 | 4.82 | 0.00 | 0.00 to 0.001 | 0.03 |
| Systolic blood pressure | 0.01 | 0.011 | 0.42 | 1.01 | 0.98 to 1.03 | 0.52 |
| Diastolic blood pressure | −0.002 | 0.023 | 0.01 | 0.99 | 0.95 to 1.04 | 0.94 |
| Hemoglobin | −0.005 | 0.015 | 0.10 | 0.99 | 0.96 to 1.02 | 0.75 |
| Alexithymia (scale) | 0.49 | 0.014 | 11.6 | 1.05 | 1.02 to 1.08 | 0.001 |
| Depression (HDRS §) | 0.02 | 0.034 | 0.002 | 1.002 | 0.93 to 1.07 | 0.96 |
| Sleep quality (poor) (PSQI %) | 0.03 | 0.043 | 0.59 | 1.03 | 0.95 to 1.12 | 0.44 |
| Sleep latency | 0.28 | 0.225 | 1.530 | 1.321 | 0.85 to 2.05 | 0.21 |
| Duration of a sleep | −0.43 | 0.22 | 3.87 | 0.65 | 0.42 to 0.99 | 0.049 |
| Multivariate Regression (Stepwise Method) | ||||||
| Alexithymia | 0.049 | 0.018 | 7.336 | 1.051 | 1.014 to 1.089 | 0.007 |
| Constant | −4.015 | 1.47 | 7.46 | 0.006 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pojatić, Đ.; Nikić, D.; Tolj, I.; Pezerović, D.; Šantić, A.; Degmečić, D. Alexithymia, Phosphorus Levels, and Sleep Disorders in Patients on Hemodialysis. J. Clin. Med. 2022, 11, 3218. https://doi.org/10.3390/jcm11113218
Pojatić Đ, Nikić D, Tolj I, Pezerović D, Šantić A, Degmečić D. Alexithymia, Phosphorus Levels, and Sleep Disorders in Patients on Hemodialysis. Journal of Clinical Medicine. 2022; 11(11):3218. https://doi.org/10.3390/jcm11113218
Chicago/Turabian StylePojatić, Đorđe, Dajana Nikić, Ivana Tolj, Davorin Pezerović, Andrijana Šantić, and Dunja Degmečić. 2022. "Alexithymia, Phosphorus Levels, and Sleep Disorders in Patients on Hemodialysis" Journal of Clinical Medicine 11, no. 11: 3218. https://doi.org/10.3390/jcm11113218
APA StylePojatić, Đ., Nikić, D., Tolj, I., Pezerović, D., Šantić, A., & Degmečić, D. (2022). Alexithymia, Phosphorus Levels, and Sleep Disorders in Patients on Hemodialysis. Journal of Clinical Medicine, 11(11), 3218. https://doi.org/10.3390/jcm11113218