
Fourteen-Year Temporal Trends in Patients Hospitalized for Mitral Regurgitation: The Increasing Burden of Mitral Valve Prolapse in Men

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Population
2.2. Statistical Analysis
3. Results
3.1. Characteristics of Patients Hospitalized for MR in 2019, According to Etiology
3.1.1. Primary MR
3.1.2. Secondary MR
3.2. Temporal Trends
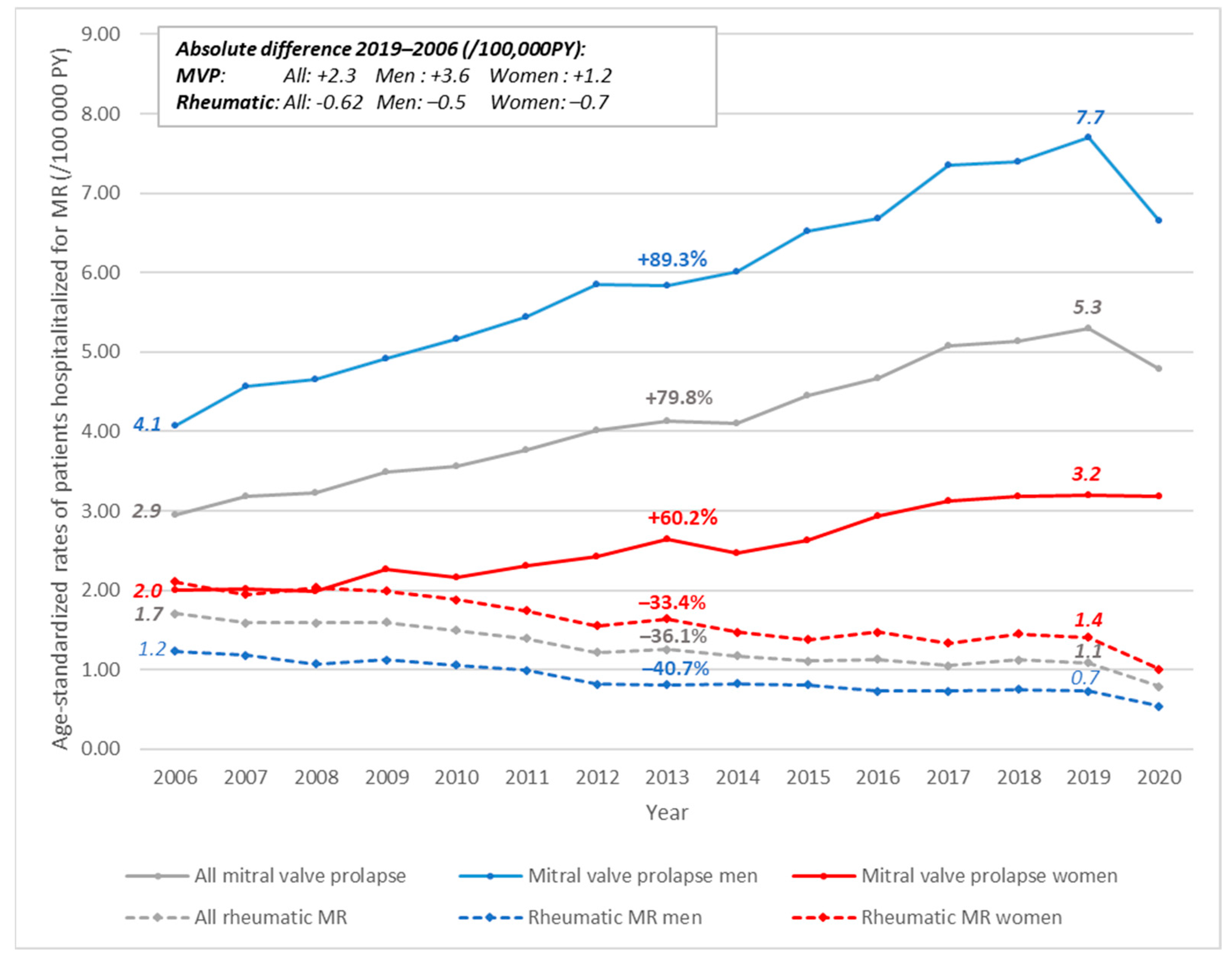
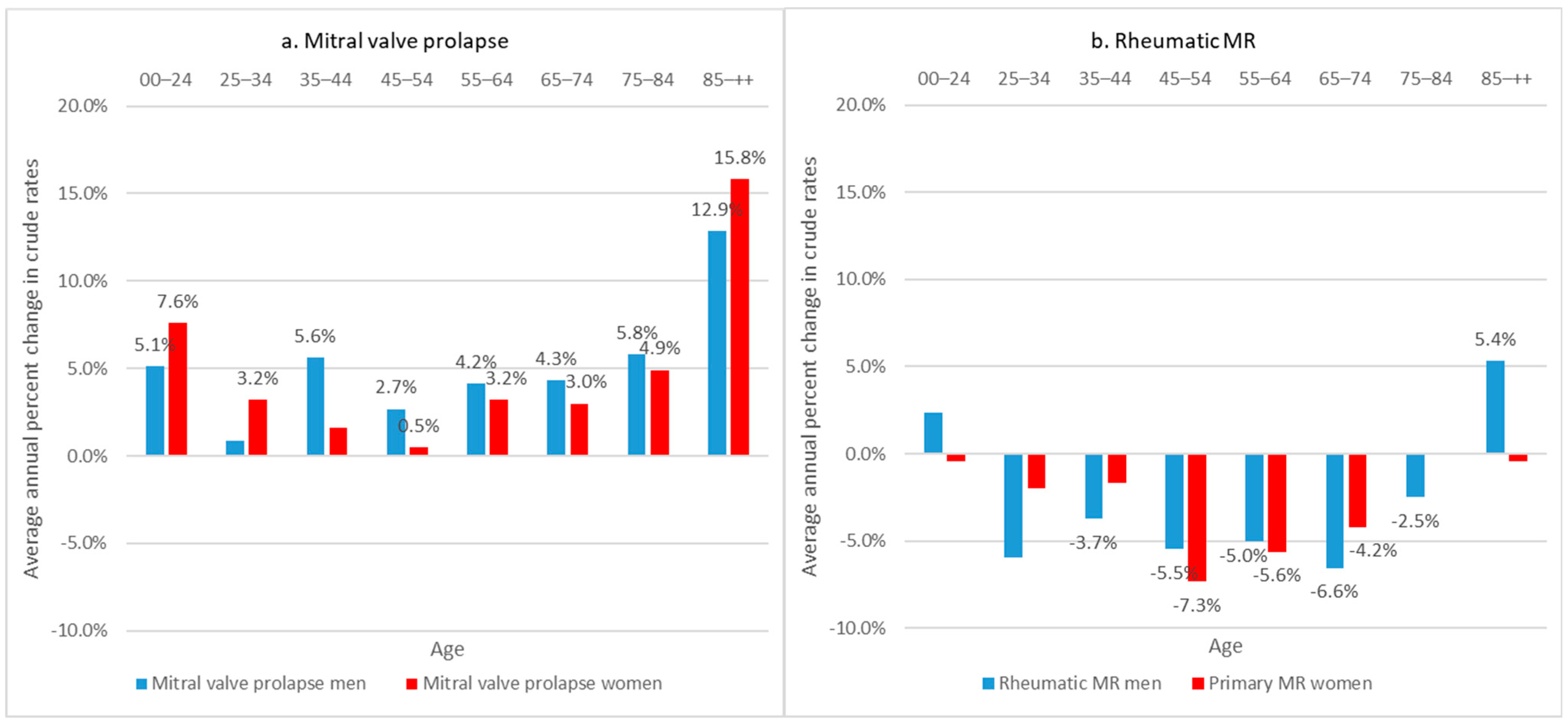
3.2.1. Primary MR
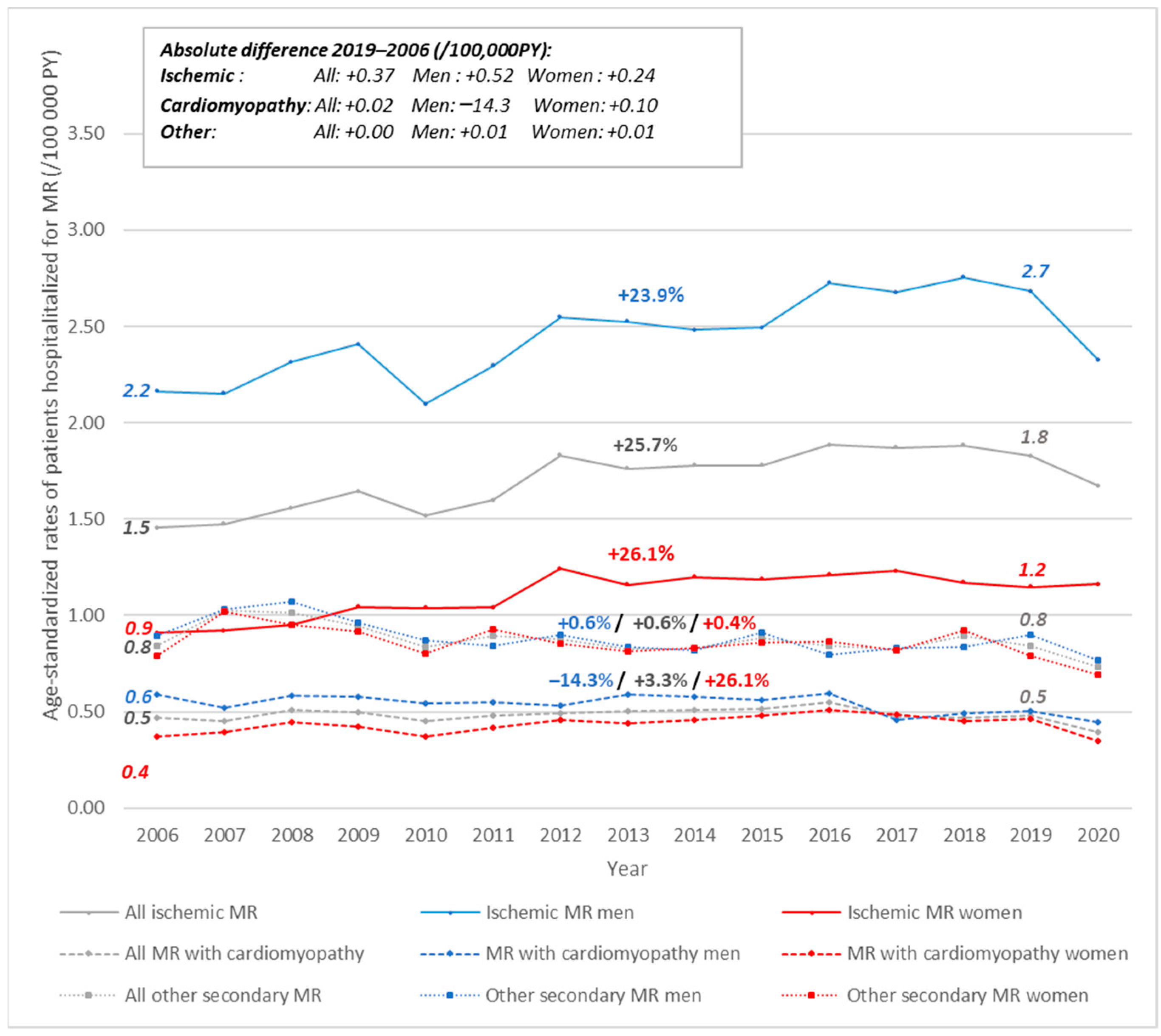
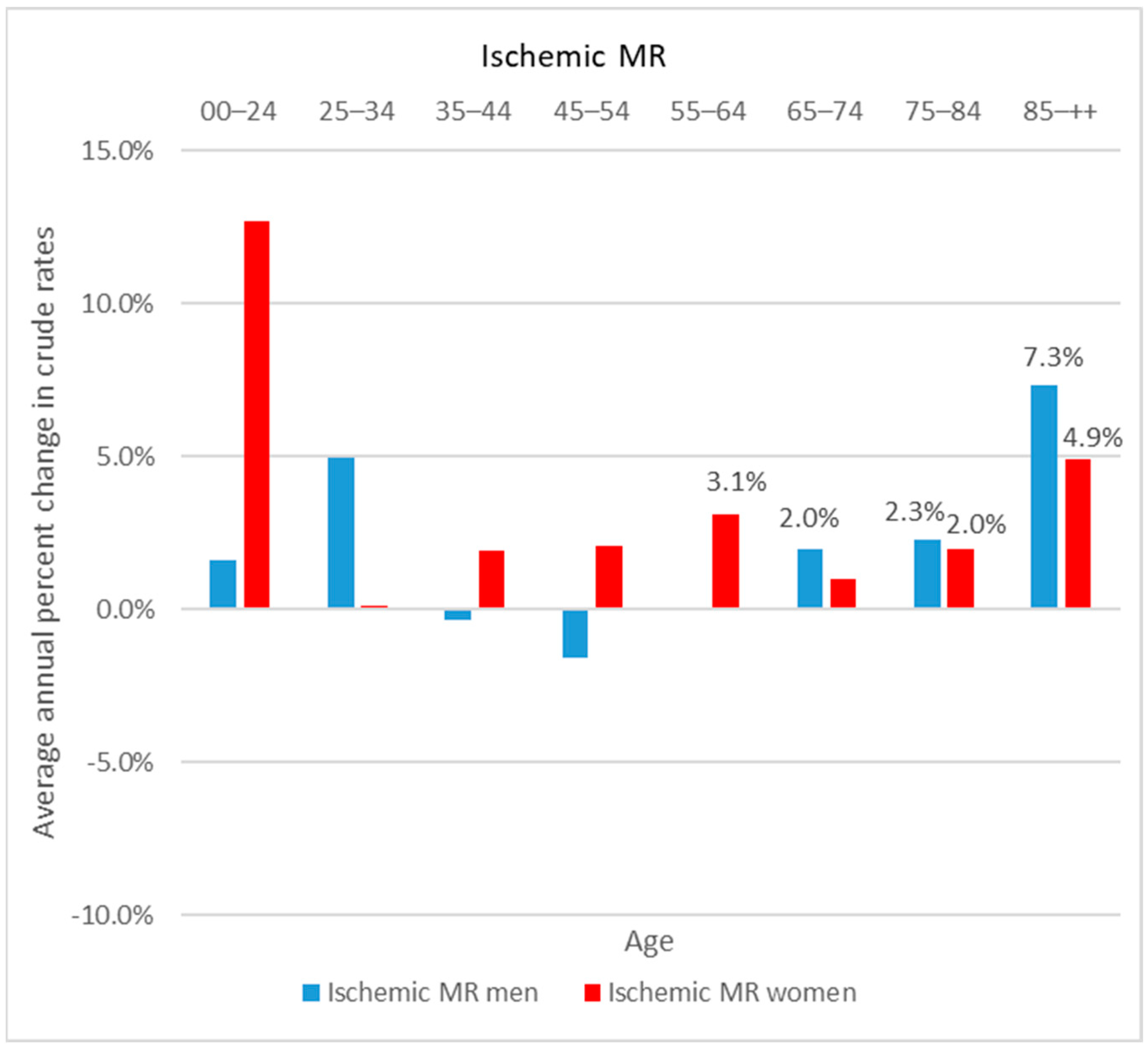
3.2.2. Secondary MR
3.3. Figures, Tables and Schemes
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nkomo, V.T.; Gardin, J.M.; Skelton, T.N.; Gottdiener, J.S.; Scott, C.G.; Enriquez-Sarano, M. Burden of valvular heart diseases: A population-based study. Lancet 2006, 368, 1005–1011. [Google Scholar] [CrossRef]
- Crousillat, D.R.; Wood, M.J. Valvular Heart Disease and Heart Failure in Women. Heart Fail. Clin. 2019, 15, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Iung, B.; Baron, G.; Butchart, E.G.; Delahaye, F.; Gohlke-Barwolf, C.; Levang, O.W.; Tornos, P.; Vanoverschelde, J.L.; Vermeer, F.; Boersma, E.; et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur. Heart J. 2003, 24, 1231–1243. [Google Scholar] [CrossRef] [Green Version]
- Iung, B.; Delgado, V.; Rosenhek, R.; Price, S.; Prendergast, B.; Wendler, O.; De Bonis, M.; Tribouilloy, C.; Evangelista, A.; Bogachev-Prokophiev, A.; et al. Contemporary Presentation and Management of Valvular Heart Disease: The EURObservational Research Programme Valvular Heart Disease II Survey. Circulation 2019, 140, 1156–1169. [Google Scholar] [CrossRef]
- Dziadzko, V.; Clavel, M.A.; Dziadzko, M.; Medina-Inojosa, J.R.; Michelena, H.; Maalouf, J.; Nkomo, V.; Thapa, P.; Enriquez-Sarano, M. Outcome and undertreatment of mitral regurgitation: A community cohort study. Lancet 2018, 391, 960–969. [Google Scholar] [CrossRef]
- Enriquez-Sarano, M.; Akins, C.W.; Vahanian, A. Mitral regurgitation. Lancet 2009, 373, 1382–1394. [Google Scholar] [CrossRef]
- Avierinos, J.F.; Gersh, B.J.; Melton, L.J.; Bailey, K.R.; Shub, C.; Nishimura, R.A.; Tajik, J.; Enriquez-Sarano, M. Natural history of asymptomatic mitral valve prolapse in the community. Circulation 2002, 106, 1355–1361. [Google Scholar] [CrossRef] [Green Version]
- Iung, B.; Vahanian, A. Epidemiology of acquired valvular heart disease. Can. J. Cardiol. 2014, 30, 962–970. [Google Scholar] [CrossRef]
- Yadgir, S.; Johnson, C.O.; Aboyans, V.; Adebayo, O.M.; Adedoyin, R.A.; Afarideh, M.; Alahdab, F.; Alashi, A.; Alipour, V.; Arabloo, J.; et al. Global, Regional, and National Burden of Calcific Aortic Valve and Degenerative Mitral Valve Diseases, 1990–2017. Circulation 2020, 141, 1670–1680. [Google Scholar] [CrossRef] [Green Version]
- Watkins, D.A.; Johnson, C.O.; Colquhoun, S.M.; Karthikeyan, G.; Beaton, A.; Bukhman, G.; Forouzanfar, M.; Longenecker, C.; Mayosi, B.; Mensah, G.; et al. Global, Regional, and National Burden of Rheumatic Heart Disease, 1990–2015. N. Engl. J. Med. 2017, 377, 713–722. [Google Scholar] [CrossRef]
- Gabet, A.; Danchin, N.; Juilliere, Y.; Olie, V. Acute coronary syndrome in women: Rising hospitalizations in middle-aged French women, 2004–14. Eur. Heart J. 2017, 38, 1060–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puymirat, E.; Simon, T.; Cayla, G.; Cottin, Y.; Elbaz, M.; Coste, P.; Lemesle, G.; Motreff, P.; Popovic, B.; Khalife, K.; et al. Acute Myocardial Infarction: Changes in Patient Characteristics, Management, and 6-Month Outcomes Over a Period of 20 Years in the FAST-MI Program (French Registry of Acute ST-Elevation or Non-ST-Elevation Myocardial Infarction) 1995 to 2015. Circulation 2017, 136, 1908–1919. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Muñoz, D.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef] [PubMed]
- Tuppin, P.; de Roquefeuil, L.; Weill, A.; Ricordeau, P.; Merliere, Y. French national health insurance information system and the permanent beneficiaries sample. Rev. Epidemiol. Sante Publique 2010, 58, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Tuppin, P.; Rudant, J.; Constantinou, P.; Gastaldi-Menager, C.; Rachas, A.; de Roquefeuil, L.; Maura, G.; Caillol, H.; Tajahmady, A.; Coste, J.; et al. Value of a national administrative database to guide public decisions: From the systeme national d’information interregimes de l’Assurance Maladie (SNIIRAM) to the systeme national des donnees de sante (SNDS) in France. Rev. Epidemiol. Sante Publique 2017, 65 (Suppl. S4), S149–S167. [Google Scholar] [CrossRef] [PubMed]
- Moulis, G.; Lapeyre-Mestre, M.; Palmaro, A.; Pugnet, G.; Montastruc, J.L.; Sailler, L. French health insurance databases: What interest for medical research? Rev. Med. Interne 2015, 36, 411–417. [Google Scholar] [CrossRef] [Green Version]
- ATIH. Guide Méthodologique de Production des Informations Relatives à L’activité Médicale et à sa Facturation en Médecine, Chirurgie, Obstétrique et Odontologie; ATIH: Lyon, France, 2017. [Google Scholar]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Rey, G.; Jougla, E.; Fouillet, A.; Hemon, D. Ecological association between a deprivation index and mortality in France over the period 1997–2001: Variations with spatial scale, degree of urbanicity, age, gender and cause of death. BMC Public Health 2009, 9, 33. [Google Scholar] [CrossRef] [Green Version]
- Messika-Zeitoun, D.; Candolfi, P.; Enriquez-Sarano, M.; Burwash, I.G.; Chan, V.; Philippon, J.F.; Toussaint, J.M.; Verta, P.; Feldman, T.E.; Iung, B.; et al. Presentation and outcomes of mitral valve surgery in France in the recent era: A nationwide perspective. Open Heart 2020, 7, e001339. [Google Scholar] [CrossRef]
- Degano, I.R.; Degano, I.R.; Salomaa, V.; Veronesi, G.; Ferrieres, J.; Kirchberger, I.; Laks, T.; Havulinna, A.; Ruidavets, J.; Ferrario, M.; et al. Twenty-five-year trends in myocardial infarction attack and mortality rates, and case-fatality, in six European populations. Heart 2015, 101, 1413–1421. [Google Scholar] [CrossRef]
- Gerber, Y.; Weston, S.A.; Jiang, R.; Roger, V.L. The changing epidemiology of myocardial infarction in Olmsted County, Minnesota, 1995–2012. Am. J. Med. 2015, 128, 144–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantovani, F.; Clavel, M.A.; Michelena, H.I.; Suri, R.M.; Schaff, H.V.; Enriquez-Sarano, M. Comprehensive Imaging in Women With Organic Mitral Regurgitation: Implications for Clinical Outcome. JACC Cardiovasc. Imaging 2016, 9, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Kislitsina, O.N.; Zareba, K.M.; Bonow, R.O.; Andrei, A.C.; Kruse, J.; Puthumana, J.; Akhter, N.; Malaisrie, C.; McCarthy, P.; Rigolin, V. Is mitral valve disease treated differently in men and women? Eur. J. Prev. Cardiol. 2020, 26, 1433–1443. [Google Scholar] [CrossRef] [PubMed]
- Michler, R.E.; Smith, P.K.; Parides, M.K.; Ailawadi, G.; Thourani, V.; Moskowitz, A.J.; Acker, M.; Hung, J.; Chang, H.; Perrault, L.; et al. Two-Year Outcomes of Surgical Treatment of Moderate Ischemic Mitral Regurgitation. N. Engl. J. Med. 2016, 374, 1932–1941. [Google Scholar] [CrossRef] [PubMed]
- Acker, M.A.; Parides, M.K.; Perrault, L.P.; Moskowitz, A.J.; Gelijns, A.C.; Voisine, P.; Smith, P.K.; Hung, J.W.; Blackstone, E.H.; Puskas, D.; et al. Mitral-valve repair versus replacement for severe ischemic mitral regurgitation. N. Engl. J. Med. 2014, 370, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Zhang, B.; Zhang, J.; Ying, Y.; Zhu, C.; Chen, B. Repair or replacement for severe ischemic mitral regurgitation: A meta-analysis. Medicine 2018, 97, e11546. [Google Scholar] [CrossRef]
- Obadia, J.F.; Messika-Zeitoun, D.; Leurent, G.; Iung, B.; Bonnet, G.; Piriou, N.; Lefèvre, T.; Piot, C.; Rouleau, F.; Carrié, D.; et al. Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation. N. Engl. J. Med. 2018, 379, 2297–2306. [Google Scholar] [CrossRef]
- Stone, G.W.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.; Grayburn, P.A.; Rinaldi, M.; Kapadia, S.R.; et al. Transcatheter Mitral-Valve Repair in Patients with Heart Failure. N. Engl. J. Med. 2018, 379, 2307–2318. [Google Scholar] [CrossRef]
- Feldman, T.; Kar, S.; Elmariah, S.; Smart, S.C.; Trento, A.; Siegel, R.J.; Apruzzese, P.; Fail, P.; Rinaldi, M.J.; Smalling, R.W.; et al. Randomized Comparison of Percutaneous Repair and Surgery for Mitral Regurgitation: 5-Year Results of EVEREST II. J. Am. Coll. Cardiol. 2015, 66, 2844–2854. [Google Scholar] [CrossRef] [Green Version]
- Pighi, M.; Pighi, M.; Estevez-Loureiro, R.; Maisano, F.; Ussia, G.P.; Dall’Ara, G.; Franzen, O.; Laroche, C.; Settergren, M.; Winter, R.; et al. Immediate and 12-Month Outcomes of Ischemic Versus Nonischemic Functional Mitral Regurgitation in Patients Treated With MitraClip (from the 2011 to 2012 Pilot Sentinel Registry of Percutaneous Edge-To-Edge Mitral Valve Repair of the European Society of Cardiology). Am. J. Cardiol. 2017, 119, 630–637. [Google Scholar]
- Grayburn, A.; Sannino, A.; Packer, M. Proportionate and Disproportionate Functional Mitral Regurgitation: A New Conceptual Framework That Reconciles the Results of the MITRA-FR and COAPT Trials. JACC Cardiovasc. Imaging 2019, 12, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Juilliere, Y. Lessons from MITRA-FR and COAPT studies: Can we hope for an indication for severe functional mitral regurgitation in systolic heart failure? Arch. Cardiovasc. Dis. 2019, 112, 370–373. [Google Scholar] [CrossRef] [PubMed]
- Pibarot, P.; Delgado, V.; Bax, J.J. MITRA-FR vs. COAPT: Lessons from two trials with diametrically opposed results. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 620–624. [Google Scholar] [CrossRef]
- Ined. Espérance de vie—Evolution de L’espérance de vie à la Naissance et à 65 Ans. Available online: https://www.ined.fr/fr/tout-savoir-population/chiffres/france/mortalite-cause-deces/esperance-vie/ (accessed on 22 September 2020).
- GBD 2017 Mortality Collaborators. Global, regional, and national age-sex-specific mortality and life expectancy, 1950–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1684–1735. [Google Scholar] [CrossRef] [Green Version]
- Elmistekawy, E.; Mesana, T.; Chan, V. Ischemic mitral regurgitation: Current trends and treatment. Curr. Opin. Cardiol. 2013, 28, 661–665. [Google Scholar] [CrossRef] [PubMed]
- Bersano, A.; Kraemer, M.; Touzé, E.; Weber, R.; Alamowitch, S.; Sibon, I.; Pantoni, L. Stroke care during the COVID-19 pandemic: Experience from three large European countries. Eur. J. Neurol. 2020, 27, 1794–1800. [Google Scholar] [CrossRef] [PubMed]
- Mafham, M.M.; Spata, E.; Goldacre, R.; Gair, D.; Curnow, P.; Hollings, B.; Roebuck, C.; Gale, C.P.; Mamas, M.A. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England. Lancet 2020, 396, 381–389. [Google Scholar] [CrossRef]
- Mohamed, M.O.; Banerjee, A.; Clarke, S.; de Belder, M.; Patwala, A.; Kwok, G.C.S.; Rashid, M.; Gale, C.P.; Curzen, N. Impact of COVID-19 on cardiac procedure activity in England and associated 30-day mortality. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 247–256. [Google Scholar] [CrossRef]
- Khan, J.M.; Khan, J.M.; Khalid, N.; Shlofmitz, E.; Forrestal, B.J.; Yerasi, C.; Case, B.C.; Chezar-Azerrad, C.; Musallam, A.; Rogers, T.; et al. Guidelines for Balancing Priorities in Structural Heart Disease During the COVID-19 Pandemic. Cardiovasc. Revasc. Med. 2020, 21, 1030–1033. [Google Scholar] [CrossRef]
- Shah, B.N.; Schlosshan, D.; McConkey, H.Z.R.; Buch, M.H.; Marshall, A.J.; Cartwright, N.; Dobson, L.E.; Allen, C.; Campbell, B.; Khan, P.; et al. Outpatient management of heart valve disease following the COVID-19 pandemic: Implications for present and future care. Heart 2020, 106, 1549–1554. [Google Scholar] [CrossRef]
- Woolf, S.H.; Chapman, D.A.; Sabo, R.T.; Weinberger, D.M.; Hill, L. Excess Deaths From COVID-19 and Other Causes, March-April 2020. JAMA 2020, 324, 510–513. [Google Scholar] [CrossRef] [PubMed]
- Messika-Zeitoun, D.; Candolfi, P.; Vahanian, A.; Chan, V.; Burwash, I.G.; Philippon, J.F.; Toussaint, J.M.; Verta, P.; Feldman, T.E.; Iung, B.; et al. Dismal Outcomes and High Societal Burden of Mitral Valve Regurgitation in France in the Recent Era: A Nationwide Perspective. J. Am. Heart Assoc. 2020, 9, e016086. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2019 | Primary RM | Mitral Valve Prolapse | Rheumatic RM | ||||||
|---|---|---|---|---|---|---|---|---|---|
| All | Men | Women | p-Value | All | Men | Women | p-Value | ||
| Total number, n | 4277 | 3560 | 2338 | 1222 | 717 | 221 | 496 | ||
| Demographic characteristics | - | ||||||||
| Age (years), mean (SD) | 67.4 (14.0) | 67.8 (13.5) | 65.8 (13.0) | 71.8 (13.7) | <0.0001 | 65.1 (15.9) | 64.0 (16.8) | 65.5 (15.5) | 0.22 |
| Fdep *, n (%) | |||||||||
| Quintile 1 (the least disadvantaged) | 832 (20.2%) | 20.0% | 20.6% | 18.9% | 0.41 | 21.1% | 25.0% | 19.3% | 0.56 |
| Quintile 2 | 827 (20.1%) | 20.0% | 20.4% | 19.4% | 20.2% | 18.0% | 21.1% | ||
| Quintile 3 | 897 (21.8%) | 22.0% | 21.2% | 23.7% | 20.3% | 19.5% | 20.7% | ||
| Quintile 4 | 807 (19.6%) | 19.8% | 20.0% | 19.6% | 18.2% | 18.0% | 18.2% | ||
| Quintile 5 (the most disadvantaged) | 760 (18.4%) | 18.1% | 17.9% | 18.4% | 20.3% | 19.5% | 20.7% | ||
| Medical characteristics | |||||||||
| Charlson comorbidity index mean (SD) | 1.96 (2.11) | 1.9 (2.1) | 1.9 (2.1) | 1.9 (2.0) | 0.86 | 2.5 (2.2) | 2.7 (2.4) | 2.4 (2.1) | 0.05 |
| History of hospitalization for heart failure | 1447 (33.8%) | 30.8% | 28.1% | 36.0% | <0.001 | 48.7% | 47.5% | 49.2% | 0.68 |
| Length of index stay mean (SD) | 9.1 (10.8) | 9.0 (10.5) | 9.0 (8.6) | 8.9 (8.3) | 0.65 | 9.9 (11.9) | 10.2 (13.4) | 9.7 (11.2) | 0.61 |
| Management of mitral regurgitation in the year following the index hospital stay **, n (%) | |||||||||
| Surgical valve replacement | 1073 (25.1%) | 19.0% | 18.0% | 20.9% | 0.03 | 55.2% | 48.4% | 58.3% | 0.01 |
| Mean age | 67.1 | 69.4 | 68.4 | 71.1 | 63.2 | 60.3 | 64.3 | ||
| Surgical valve plasty | 2032 (47.5%) | 55.1% | 60.4% | 44.9% | <0.001 | 9.9% | 15.8% | 7.3% | <0.001 |
| Mean age | 62.8 | 63.0 | 61.5 | 66.8 | 58.1 | 62.8 | 53.6 | ||
| Percutaneous mitral valve repair | 555 (13.0) | 14.7% | 12.0% | 19.8% | <0.001 | 4.6% | 8.6% | 2.8% | <0.001 |
| Mean age | 81.2 | 81.4 | 79.3 | 83.9 | 77.0 | 77.3 | 76.6 | ||
| No mitral procedure mentioned | 617 (14.4%) | 11.2% | 9.6% | 14.3% | <0.001 | 30.3% | 27.1% | 31.7% | 0.23 |
| Mean age | 70.5 | 71.4 | 70.8 | 72.1 | 68.8 | 67.0 | 69.5 | ||
| Readmission in the year following | |||||||||
| After index stay, all causes, n (%) | 2600 (60.8%) | 59.9% | 59.5% | 60.9% | 0.41 | 65.0% | 70.1% | 62.7% | 0.05 |
| After index stay, for RM, n (%) | 1521 (35.6%) | 37.1% | 36.2% | 38.8% | 0.13 | 28.0% | 34.8% | 25.0% | 0.007 |
| After index stay, for heart failure, n (%) | 327 (7.6%) | 6.6% | 5.6% | 8.4% | 0.001 | 13.0% | 11.3% | 13.7% | 0.38 |
| After surgical or percutaneous act, all causes, n (%) | 1284 (35.1%) | 33.6% | 33.9% | 33.0% | 0.58 | 44.4% | 45.3% | 44.0% | 0.77 |
| After surgical or percutaneous act, for RM, n (%) | 80 (2.2%) | 2.3% | 1.9% | 3.2% | 0.03 | 1.0% | 3.1% | 0.6% | 0.04 |
| After surgical or percutaneous act, for heart failure, n (%) | 196 (5.4%) | 4.7% | 4.4% | 5.4% | 0.17 | 9.4% | 7.5% | 10.3% | 0.30 |
| After surgical or percutaneous act, MACCE, n (%) | 469 (12.8%) | 11.8% | 10.5% | 14.4% | 0.001 | 19.2% | 18.6% | 19.5% | 0.82 |
| All causes mortality, n (%) | |||||||||
| After index stay | |||||||||
| During the index hospital stay | 65 (1.5%) | 1.4% | 1.0% | 2.1% | 0.005 | 2.2% | 2.7% | 2.0% | 0.56 |
| Mean age | 74.2 | 76.4 | 73.7 | 78.8 | 67.4 | 67.2 | 67.6 | ||
| At 30 days | 109 (2.5%) | 2.4% | 1.8% | 3.5% | 0.002 | 3.2% | 2.7% | 3.4% | 0.62 |
| Mean age | 76.1 | 77.9 | 75.0 | 80.8 | 69.6 | 67.2 | 70.5 | ||
| At 1 year | 302 (7.1%) | 6.3% | 5.4% | 8.1% | 0.002 | 10.6% | 11.3% | 10.3% | 0.68 |
| Mean age | 77.6 | 78.5 | 76.3 | 81.4 | 74.7 | 76.3 | 73.9 | ||
| After surgical or percutaneous act | |||||||||
| At 30 days | 86 (2.3%) | 2.1% | 1.8% | 2.8% | 0.06 | 4.0% | 2.5% | 4.7% | 0.23 |
| Mean age | 74.5 | 75.6 | 72.7 | 79.4 | 70.7 | 69.8 | 70.9 | ||
| At 1 year | 197 (5.4%) | 4.8% | 4.0% | 6.4% | 0.003 | 9.0% | 9.3% | 8.8% | 0.86 |
| Mean age | 76.3 | 77.8 | 75.7 | 80.4 | 71.4 | 72.5 | 70.8 | ||
| 2019 | Secondary RM | Chronic Ischemic Heart Disease MR | MR with Cardiomyopathy | Other Secondary MR | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | Men | Women | p-Value | All | Men | Women | p-Value | All | Men | Women | p-Value | ||
| Total number, n | 2127 | 1235 | 790 | 445 | 319 | 150 | 169 | 573 | 267 | 306 | |||
| Demographic characteristics | |||||||||||||
| Age (years), mean (SD) | 72.1 (12.3) | 72.9 (10.7) | 71.9 (10.4) | 74.8 (10.9) | <0.001 | 68.5 (14.3) | 67.3 (14.2) | 69.5 (14.4) | 0.17 | 72.3 (13.8) | 69.8 (14.2) | 74.4 (13.0) | <0.001 |
| Fdep *, n (%) | |||||||||||||
| Quintile 1 (the least disadvantaged) | 358 (17.5%) | 17.5% | 18.7% | 15.5% | 0.54 | 17.4% | 20.8% | 14.4% | 0.07 | 17.6% | 16.5% | 18.5% | 0.19 |
| Quintile 2 | 406 (19.9%) | 19.3% | 18.5% | 20.7% | 22.4% | 23.6% | 21.3% | 19.8% | 20.1% | 19.5% | |||
| Quintile 3 | 431 (21.1%) | 22.1% | 22.7% | 20.9% | 18.8% | 13.2% | 23.8% | 20.3% | 23.6% | 17.5% | |||
| Quintile 4 | 421 (20.6%) | 21.1% | 20.5% | 22.1% | 18.4% | 21.5% | 15.6% | 20.9% | 22.0% | 19.9% | |||
| Quintile 5 (the most disadvantaged) | 425 (20.8%) | 20.0% | 19.6% | 20.7% | 23.0% | 20.8% | 25.0% | 21.4% | 17.7% | 24.6% | |||
| Medical characteristics | |||||||||||||
| Charlson comorbidity index mean (SD) | 3.1 (2.0) | 3.2 (2.2) | 3.1 (2.1) | 3.2 (2.2) | 0.51 | 2.9 (1.9) | 2.8 (1.9) | 2.9 (1.9) | 0.55 | 3.1 (1.7) | 3.0 (2.8) | 3.1 (2.9) | 0.65 |
| History of hospitalization for heart failure | 1371 (64.5%) | 63.4% | 61.8% | 66.3% | 0.11 | 68.3% | 64.0% | 72.2% | 0.12 | 64.6% | 60.3% | 68.3% | 0.05 |
| Length of index stay mean (SD) | 10.2 (12.4) | 10.5 (13.4) | 10.8 (13.7) | 10.0 (12.7) | 0.30 | 9.2 (11.0) | 9.0 (11.6) | 9.3 (10.5) | 0.80 | 9.9 (11.1) | 10.0 (9.6) | 9.9 (12.3) | 0.92 |
| Management of mitral regurgitation in the year following the index hospital stay **, n (%) | |||||||||||||
| Surgical valve replacement | 600 (28.2%) | 29.1% | 28.7% | 29.7% | 0.73 | 26.7% | 22.7% | 30.2% | 0.13 | 27.2% | 26.2% | 28.1% | 0.61 |
| Mean age (years) | 69.0 | 69.7 | 69.3 | 70.5 | 66.4 | 62.6 | 68.9 | 68.7 | 68.1 | 69.2 | |||
| Surgical valve plasty | 405 (19.0%) | 16.2% | 19.2% | 10.8% | <0.001 | 18.8% | 25.3% | 13.0% | <0.001 | 25.3% | 32.2% | 19.3% | <0.001 |
| Mean age (years) | 66.7 | 68.3 | 67.5 | 70.6 | 62.6 | 63.1 | 61.9 | 66.1 | 65.2 | 67.5 | |||
| Percutaneous mitral valve repair | 347 (16.3%) | 19.4% | 20.5% | 17.5% | 0.20 | 11.6% | 16.0% | 7.7% | 0.02 | 12.2% | 13.9% | 10.8% | 0.26 |
| Mean age (years) | 77.8 | 77.2 | 75.8 | 80.1 | 76.0 | 75.8 | 76.5 | 80.9 | 80.4 | 81.4 | |||
| No mitral procedure mentioned | 775 (36.4%) | 35.3% | 31.5% | 42.0% | <0.001 | 42.9% | 36.0% | 49.1% | 0.02 | 35.3% | 27.7% | 41.8% | <0.001 |
| Mean age (years) | 74.8 | 75.4 | 74.4 | 76.7 | 70.3 | 69.6 | 70.7 | 76.4 | 71.6 | 79.2 | |||
| Readmission in the year following | |||||||||||||
| After index stay, all causes, n (%) | 1277 (60.0%) | 62.1% | 60.5% | 64.9% | 0.12 | 62.4% | 68.0% | 57.4% | 0.05 | 54.3% | 55.1% | 53.6% | 0.73 |
| After index stay, for RM, n (%) | 426 (20.0%) | 18.9% | 18.5% | 19.8% | 0.58 | 20.1% | 22.7% | 17.8% | 0.27 | 22.3% | 24.7% | 20.3% | 0.20 |
| After index stay, for heart failure, n (%) | 318 (15.0%) | 16.6% | 15.1% | 19.3% | 0.05 | 12.2% | 10.7% | 13.6% | 0.42 | 12.9% | 14.6% | 11.4% | 0.26 |
| After surgical or percutaneous act, all causes, n (%) | 582 (43.0%) | 46.3% | 44.9% | 49.2% | 0.25 | 43.4% | 49.0% | 37.2% | 0.11 | 35.8% | 35.8% | 36.0% | 0.97 |
| After surgical or percutaneous act, for RM, n (%) | 24 (1.8%) | 1.6% | 1.5% | 1.9% | 0.77 | 1.6% | 1.0% | 2.3% | 0.60 | 2.2% | 2.1% | 2.2% | 0.91 |
| After surgical or percutaneous act, for heart failure, n (%) | 135 (10.0%) | 11.3% | 10.0% | 14.0% | 0.10 | 9.3% | 9.4% | 9.3% | 0.99 | 7.6% | 8.8% | 6.2% | 0.34 |
| After surgical or percutaneous act, MACCE, n (%) | 316 (23.4%) | 24.4% | 21.4% | 30.6% | 0.005 | 24.7% | 20.8% | 29.1% | 0.20 | 20.5% | 17.1% | 24.2% | 0.09 |
| All causes mortality, n (%) | |||||||||||||
| After index stay | |||||||||||||
| During the index hospital stay | 89 (4.2%) | 4.5% | 3.7% | 5.8% | 0.08 | 4.1% | 2.7% | 5.3% | 0.23 | 3.7% | 3.0% | 4.2% | 0.43 |
| Mean age (years) | 75.2 | 75.1 | 74.5 | 75.7 | 75.5 | 67.3 | 79.1 | 75.4 | 71.6 | 77.7 | |||
| At 30 days | 127 (6.0%) | 6.4% | 5.6% | 7.9% | 0.11 | 5.0% | 4.0% | 5.9% | 0.43 | 5.6% | 3.4% | 7.5% | 0.03 |
| Mean age (years) | 75.2 | 75.2 | 74.5 | 76.1 | 76.9 | 72.3 | 79.6 | 0.7 | 74.2 | 71.1 | 75.4 | ||
| At 1 year | 308 (14.5%) | 15.4% | 14.2% | 17.5% | 0.12 | 15.0% | 16.0% | 14.2% | 0.65 | 12.2% | 9.0% | 15.0% | 0.03 |
| Mean age (years) | 75.4 | 75.3 | 74.0 | 77.1 | 74.4 | 73.4 | 75.4 | 76.5 | 74.8 | 77.3 | |||
| After surgical or percutaneous act | |||||||||||||
| At 30 days | 83 (6.1%) | 6.3% | 5.5% | 7.8% | 0.23 | 7.7% | 3.1% | 12.8% | 0.02 | 5.1% | 1.6% | 9.0% | 0.001 |
| Mean age (years) | 74.3 | 74.3 | 73.6 | 75.5 | 71.3 | 60.7 | 74.2 | 76.3 | 73.7 | 76.8 | |||
| At 1 year | 164 (12.1%) | 12.6% | 11.8% | 14.3% | 0.32 | 13.2% | 10.4% | 16.3% | 0.24 | 10.5% | 6.7% | 14.6% | 0.01 |
| Mean age (years) | 73.1 | 72.8 | 71.7 | 74.8 | 70.7 | 66.3 | 73.9 | 75.2 | 75.0 | 75.3 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grave, C.; Tribouilloy, C.; Tuppin, P.; Weill, A.; Gabet, A.; Juillière, Y.; Cinaud, A.; Olié, V. Fourteen-Year Temporal Trends in Patients Hospitalized for Mitral Regurgitation: The Increasing Burden of Mitral Valve Prolapse in Men. J. Clin. Med. 2022, 11, 3289. https://doi.org/10.3390/jcm11123289
Grave C, Tribouilloy C, Tuppin P, Weill A, Gabet A, Juillière Y, Cinaud A, Olié V. Fourteen-Year Temporal Trends in Patients Hospitalized for Mitral Regurgitation: The Increasing Burden of Mitral Valve Prolapse in Men. Journal of Clinical Medicine. 2022; 11(12):3289. https://doi.org/10.3390/jcm11123289
Chicago/Turabian StyleGrave, Clémence, Christophe Tribouilloy, Philippe Tuppin, Alain Weill, Amélie Gabet, Yves Juillière, Alexandre Cinaud, and Valérie Olié. 2022. "Fourteen-Year Temporal Trends in Patients Hospitalized for Mitral Regurgitation: The Increasing Burden of Mitral Valve Prolapse in Men" Journal of Clinical Medicine 11, no. 12: 3289. https://doi.org/10.3390/jcm11123289
APA StyleGrave, C., Tribouilloy, C., Tuppin, P., Weill, A., Gabet, A., Juillière, Y., Cinaud, A., & Olié, V. (2022). Fourteen-Year Temporal Trends in Patients Hospitalized for Mitral Regurgitation: The Increasing Burden of Mitral Valve Prolapse in Men. Journal of Clinical Medicine, 11(12), 3289. https://doi.org/10.3390/jcm11123289