
Sex Disparities in Outcome of Patients with Alcohol-Related Liver Cirrhosis within the Eurotransplant Network—A Competing Risk Analysis

 , , , , , , ,
, , , , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Overview
3.2. Sex Differences in Registration and Outcomes
3.2.1. Successful Liver Transplantation
3.2.2. Removal from Waiting List
3.2.3. Died on Waiting List
3.2.4. Age Differences between the Sexes
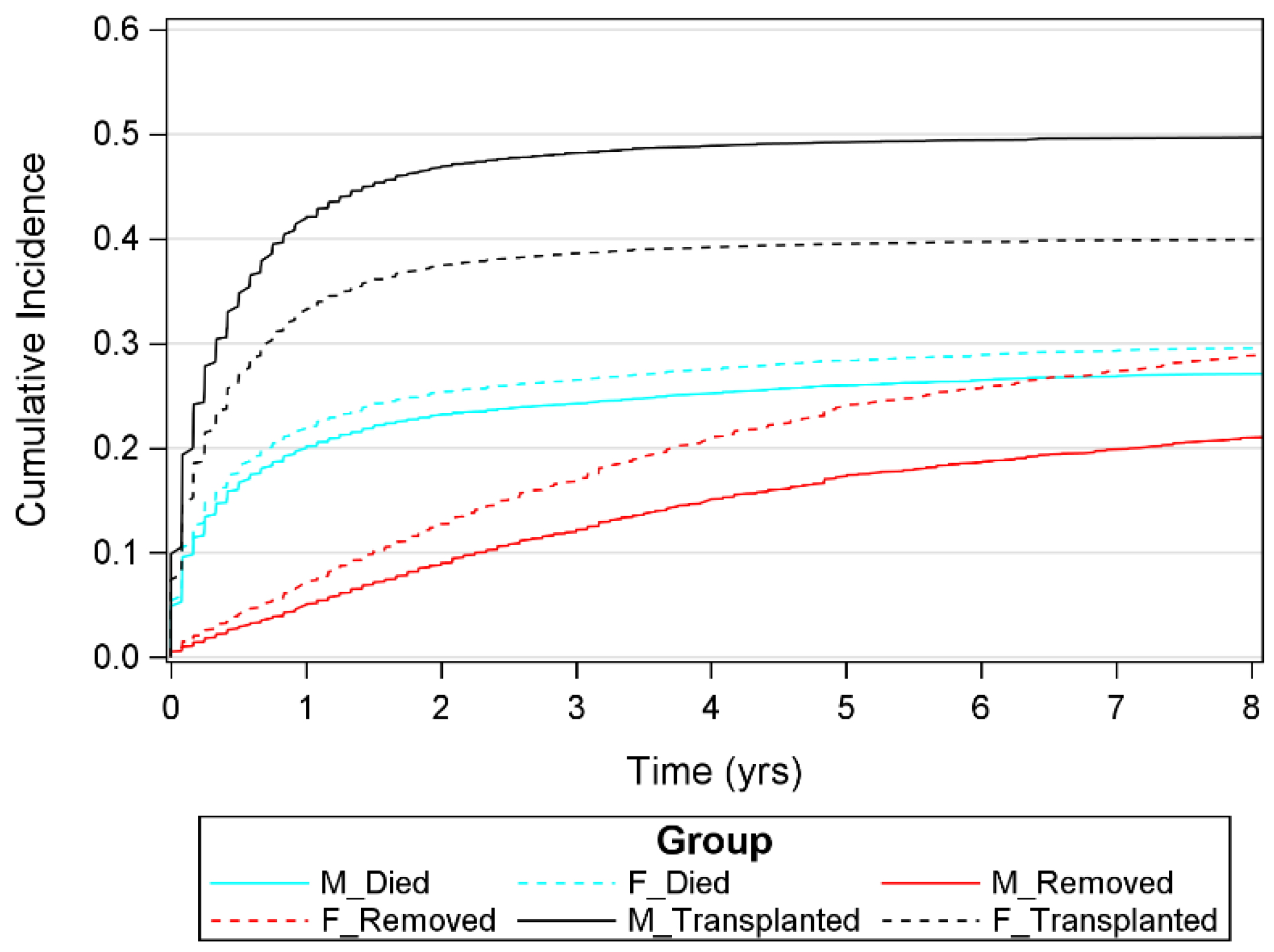
3.3. Cumulative Incidences
4. Discussion
4.1. Sex Disparities in LT Registrations
4.2. Sex Differences in LT Outcomes
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Status Report on Alcohol and Health 2018; World Health Organization: Geneva, Switzerland, 2018; Volume 65, pp. 74–85.
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Human Resources for Health 1990–2019. Seattle, United States of America: Institute for Health Metrics and Evaluation (IHME). 2020. Available online: https://ghdx.healthdata.org/ (accessed on 1 November 2020).
- Griswold, M.G.; Fullman, N.; Hawley, C.; Arian, N.; Zimsen, S.R.M.; Tymeson, H.D.; Venkateswaran, V.; Tapp, A.D.; Forouzanfar, M.H.; Salama, J.S.; et al. Alcohol Use and Burden for 195 Countries and Territories, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet 2018, 392, 1015–1035. [Google Scholar] [CrossRef] [Green Version]
- Bellentani, S.; Saccoccio, G.; Costa, G.; Tiribelli, C.; Manenti, F.; Sodde, M.; Saveria Croce’, L.; Sasso, F.; Pozzato, G.; Cristianini, G.; et al. Drinking Habits as Cofactors of Risk for Alcohol Induced Liver Damage. Gut 1997, 41, 845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roerecke, M.; Vafaei, A.; Hasan, O.S.M.; Chrystoja, B.R.; Cruz, M.; Lee, R.; Neuman, M.G.; Rehm, J. Alcohol Consumption and Risk of Liver Cirrhosis: A Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2019, 114, 1574–1586. [Google Scholar] [CrossRef] [PubMed]
- Tsochatzis, E.A.; Bosch, J.; Burroughs, A.K. Liver Cirrhosis. Lancet 2014, 383, 1749–1761. [Google Scholar] [CrossRef]
- Buchanan, R.; Sinclair, J.M.A. Alcohol Use Disorder and the Liver. Addiction 2020, 116, 1270–1278. [Google Scholar] [CrossRef]
- Ginès, P.; Krag, A.; Abraldes, J.G.; Solà, E.; Fabrellas, N.; Kamath, P.S. Liver Cirrhosis. Lancet 2021, 398, 1359–1376. [Google Scholar] [CrossRef]
- Sepanlou, S.G.; Safiri, S.; Bisignano, C.; Ikuta, K.S.; Merat, S.; Saberifiroozi, M.; Poustchi, H.; Tsoi, D.; Colombara, D.; Abdoli, A.; et al. The Global, Regional, and National Burden of Cirrhosis by Cause in 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 245–266. [Google Scholar] [CrossRef] [Green Version]
- Trotter, J.F. Liver Transplantation around the World. Curr. Opin. Organ Transplant. 2017, 22, 123–127. [Google Scholar] [CrossRef]
- Ursic-Bedoya, J.; Faure, S.; Donnadieu-Rigole, H.; Pageaux, G.P. Liver Transplantation for Alcoholic Liver Disease: Lessons Learned and Unresolved Issues. World J. Gastroenterol. 2015, 21, 10994–11002. [Google Scholar] [CrossRef]
- Adam, R.; Karam, V.; Cailliez, V.; Grady, J.G.O.; Mirza, D.; Cherqui, D.; Klempnauer, J.; Salizzoni, M.; Pratschke, J.; Jamieson, N.; et al. 2018 Annual Report of the European Liver Transplant Registry (ELTR)—50-Year Evolution of Liver Transplantation. Transpl. Int. 2018, 31, 1293–1317. [Google Scholar] [CrossRef] [Green Version]
- Abouna, G.M. Ethical Issues in Organ Transplantation. Med. Princ. Pract. 2003, 12, 54–69. [Google Scholar] [CrossRef] [PubMed]
- Freeman, R.B.; Bernat, J.L. Ethical Issues in Organ Transplantation. Prog. Cardiovasc. Dis. 2012, 55, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.R.; Stock, P.G.; Smith, J.M.; Heimbach, J.K.; Skeans, M.A.; Edwards, E.B.; Harper, A.M.; Snyder, J.J.; Israni, A.K.; Kasiske, B.L. OPTN/SRTR 2011 Annual Data Report: Liver. Am. J. Transplant. 2013, 13, 73–102. [Google Scholar] [CrossRef] [PubMed]
- Kollmann, D.; Sapisochin, G.; Goldaracena, N.; Hansen, B.E.; Rajakumar, R.; Selzner, N.; Bhat, M.; McCluskey, S.; Cattral, M.S.; Greig, P.D.; et al. Expanding the Donor Pool: Donation after Circulatory Death and Living Liver Donation Do Not Compromise the Results of Liver Transplantation. Liver Transplant. 2018, 24, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Marroni, C.A.; Fleck, A.M.; Fernandes, S.A.; Galant, L.H.; Mucenic, M.; de Mattos Meine, M.H.; Mariante-Neto, G.; de Mello Brandão, A.B. Liver Transplantation and Alcoholic Liver Disease: History, Controversies, and Considerations. World J. Gastroenterol. 2018, 24, 2785–2805. [Google Scholar] [CrossRef]
- Mellinger, J.L.; Volk, M.L. Transplantation for Alcohol-Related Liver Disease: Is It Fair? Alcohol Alcohol. 2018, 53, 173–177. [Google Scholar] [CrossRef]
- Tschuor, C.; Ferrarese, A.; Kuemmerli, C.; Dutkowski, P.; Burra, P.; Clavien, P.A.; Lendoire, J.; Imventarza, O.; Crawford, M.; Andraus, W.; et al. Allocation of Liver Grafts Worldwide—Is There a Best System? J. Hepatol. 2019, 71, 707–718. [Google Scholar] [CrossRef]
- Heilig, M.; MacKillop, J.; Martinez, D.; Rehm, J.; Leggio, L.; Vanderschuren, L.J.M.J. Addiction as a Brain Disease Revised: Why It Still Matters, and the Need for Consilience. Neuropsychopharmacology 2021, 46, 1715–1723. [Google Scholar] [CrossRef]
- Leggio, L.; Lee, M.R. Treatment of Alcohol Use Disorder in Patients with Alcoholic Liver Disease. Am. J. Med. 2017, 130, 124–134. [Google Scholar] [CrossRef] [Green Version]
- Addolorato, G.; Mirijello, A.; Barrio, P.; Gual, A. Treatment of Alcohol Use Disorders in Patients with Alcoholic Liver Disease. J. Hepatol. 2016, 65, 618–630. [Google Scholar] [CrossRef] [Green Version]
- Berlakovich, G.A. Challenges in Transplantation for Alcoholic Liver Disease. World J. Gastroenterol. 2014, 20, 8033–8039. [Google Scholar] [CrossRef] [PubMed]
- Rodrigue, J.R.; Hanto, D.W.; Curry, M.P. Substance Abuse Treatment and Its Association with Relapse to Alcohol Use after Liver Transplantation. Liver Transplant. 2013, 19, 1387–1395. [Google Scholar] [CrossRef] [PubMed]
- Nephew, L.D.; Serper, M. Racial, Gender, and Socioeconomic Disparities in Liver Transplantation. Liver Transplant. 2021, 27, 900–912. [Google Scholar] [CrossRef] [PubMed]
- Mathur, A.K.; Schaubel, D.E.; Gong, Q.; Guidinger, M.K.; Merion, R.M. Sex-Based Disparities in Liver Transplant Rates in the United States. Am. J. Transplant. 2011, 11, 1435–1443. [Google Scholar] [CrossRef] [Green Version]
- Moylan, C.A.; Brady, C.W.; Johnson, J.L.; Smith, A.D.; Tuttle-Newhall, J.E.; Muir, A.J. Disparities in Liver Transplantation before and after Introduction of the MELD Score. J. Am. Med. Assoc. 2008, 300, 2371–2378. [Google Scholar] [CrossRef] [Green Version]
- McElroy, L.M.; Likhitsup, A.; Winder, G.S.; Saeed, N.; Hassan, A.; Sonnenday, C.J.; Fontana, R.J.; Mellinger, J. Gender Disparities in Patients with Alcoholic Liver Disease Evaluated for Liver Transplantation. Transplantation 2020, 104, 293–298. [Google Scholar] [CrossRef]
- Verna, E.C.; Lai, J.C. Time for Action to Address the Persistent Sex-Based Disparity in Liver Transplant Access. JAMA Surg. 2020, 155, 546–547. [Google Scholar] [CrossRef]
- Moos, R.H.; Moos, B.S.; Timko, C. Gender, Treatment and Self-Help in Remission from Alcohol Use Disorders. Clin. Med. Res. 2006, 4, 163–174. [Google Scholar] [CrossRef] [Green Version]
- Holzhauer, C.G.; Cucciare, M.; Epstein, E.E. Sex and Gender Effects in Recovery from Alcohol Use Disorder. Alcohol Res. Curr. Rev. 2019, 40, 3. [Google Scholar] [CrossRef]
- Yang, L.H.; Wong, L.Y.; Grivel, M.M.; Hasin, D.S. Stigma and Substance Use Disorders: An International Phenomenon. Curr. Opin. Psychiatry 2017, 30, 378–388. [Google Scholar] [CrossRef]
- Lale, R.; Sklar, M.; Wooldridge, J.; Sarkin, A. Gender Congruence Moderates Beliefs About the Causes of Alcohol Dependence and Major Depression. Int. J. Ment. Health Addict. 2014, 12, 395–405. [Google Scholar] [CrossRef]
- Thuluvath, P.J.; Amjad, W.; Zhang, T. Liver Transplant Waitlist Removal, Transplantation Rates and Post-Transplant Survival in Hispanics. PLoS ONE 2020, 15, e0244744. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y. Access to Liver Transplantation and Patient Survival among Asian Populations: Pre-Share 35 vs. Post-Share 35. Int. J. Organ Transplant. Med. 2017, 8, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Warren, C.; Carpenter, A.M.; Neal, D.; Andreoni, K.; Sarosi, G.; Zarrinpar, A. Racial Disparity in Liver Transplantation Listing. J. Am. Coll. Surg. 2021, 232, 526–534. [Google Scholar] [CrossRef]
- Bryce, C.L.; Angus, D.C.; Arnold, R.M.; Chang, C.-C.C.H.; Farrell, M.H.; Manzarbeitia, C.; Marino, I.R.; Roberts, M.S. Sociodemographic Differences in Early Access to Liver Transplantation Services. Am. J. Transplant. 2009, 9, 2092–2101. [Google Scholar] [CrossRef] [Green Version]
- Oloruntoba, O.O.; Moylan, C.A. Gender-Based Disparities in Access to and Outcomes of Liver Transplantation. World J. Hepatol. 2015, 7, 460–467. [Google Scholar] [CrossRef]
- Allen, A.M.; Heimbach, J.K.; Larson, J.J.; Mara, K.C.; Kim, W.R.; Kamath, P.S.; Therneau, T.M. Reduced Access to Liver Transplantation in Women: Role of Height, MELD Exception Scores, and Renal Function Underestimation. Transplantation 2018, 102, 1710–1716. [Google Scholar] [CrossRef]
- Locke, J.E.; Shelton, B.A.; Olthoff, K.M.; Pomfret, E.A.; Forde, K.A.; Sawinski, D.; Gray, M.; Ascher, N.L. Quantifying Sex-Based Disparities in Liver Allocation. JAMA Surg. 2020, 155, e201129. [Google Scholar] [CrossRef]
- Umgelter, A.; Hapfelmeier, A.; Kopp, W.; van Rosmalen, M.; Rogiers, X.; Guba, M. Disparities in Eurotransplant Liver Transplantation Wait-List Outcome between Patients with and without Model for End-Stage Liver Disease Exceptions. Liver Transplant. 2017, 23, 1256–1265. [Google Scholar] [CrossRef]
- Mazumder, N.R.; Mazumder, N.R.; Atiemo, K.; Daud, A.; Kho, A.; Abecassis, M.; Levitsky, J.; Ladner, A.D.P.; Ladner, A.D.P. Patients with Persistently Low MELD-Na Scores Continue to Be at Risk of Liver-Related Death. Transplantation 2020, 104, 1413–1418. [Google Scholar] [CrossRef]
- Jochmans, I.; van Rosmalen, M.; Pirenne, J.; Samuel, U. Adult Liver Allocation in Eurotransplant. Transplantation 2017, 101, 1542–1550. [Google Scholar] [CrossRef] [PubMed]
- Mindikoglu, A.L.; Regev, A.; Seliger, S.L.; Magder, L.S. Gender Disparity in Liver Transplant Waiting-List Mortality: The Importance of Kidney Function. Liver Transplant. 2010, 16, 1147–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cholongitas, E.; Marelli, L.; Kerry, A.; Goodier, D.W.; Nair, D.; Thomas, M.; Patch, D.; Burroughs, A.K. Female Liver Transplant Recipients with the Same GFR as Male Recipients Have Lower MELD Scores—A Systematic Bias. Am. J. Transplant. 2007, 7, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Nephew, L.D.; Zia, Z.; Ghabril, M.; Orman, E.; Lammert, C.; Kubal, C.; Chalasani, N. Sex Disparities in Waitlisting and Liver Transplant for Acute Liver Failure. JHEP Rep. 2021, 3, 100200. [Google Scholar] [CrossRef]
- Flores-Bonilla, A.; Richardson, H.N. Sex Differences in the Neurobiology of Alcohol Use Disorder. Alcohol Res. Curr. Rev. 2019, 40, 1–19. [Google Scholar] [CrossRef]
- Guinle, M.I.B.; Sinha, R. The Role of Stress, Trauma, and Negative Affect in Alcohol Misuse and Alcohol Use Disorder in Women. Alcohol Res. Curr. Rev. 2019, 40, 5. [Google Scholar] [CrossRef]
- Melhem, N.M.; Porta, G.; Oquendo, M.A.; Zelazny, J.; Keilp, J.G.; Iyengar, S.; Burke, A.; Birmaher, B.; Stanley, B.; Mann, J.J.; et al. Severity and Variability of Depression Symptoms Predicting Suicide Attempt in High-Risk Individuals. JAMA Psychiatry 2019, 76, 603–612. [Google Scholar] [CrossRef]
- Ronzitti, S.; Loree, A.M.; Potenza, M.N.; Decker, S.E.; Wilson, S.M.; Abel, E.A.; Haskell, S.G.; Brandt, C.A.; Goulet, J.L. Gender Differences in Suicide and Self-Directed Violence Risk Among Veterans with Post-Traumatic Stress and Substance Use Disorders. Womens Health Issues 2019, 29, S94–S102. [Google Scholar] [CrossRef] [Green Version]
- Vandegrift, B.J.; You, C.; Satta, R.; Brodie, M.S.; Lasek, A.W. Estradiol Increases the Sensitivity of Ventral Tegmental Area Dopamine Neurons to Dopamine and Ethanol. PLoS ONE 2017, 12, e0187698. [Google Scholar] [CrossRef] [Green Version]
- Dazzi, L.; Serra, M.; Seu, E.; Cherchi, G.; Pisu, M.G.; Purdy, R.H.; Biggio, G. Progesterone Enhances Ethanol-Induced Modulation of Mesocortical Dopamine Neurons: Antagonism by Finasteride. J. Neurochem. 2002, 83, 1103–1109. [Google Scholar] [CrossRef] [Green Version]
- Morrow, A.L.; VanDoren, M.J.; Penland, S.N.; Matthews, D.B. The Role of GABAergic Neuroactive Steroids in Ethanol Action, Tolerance and Dependence. Brain Res. Rev. 2001, 37, 98–109. [Google Scholar] [CrossRef]
- Dozier, B.L.; Stull, C.A.; Baker, E.J.; Ford, M.M.; Jensen, J.P.; Finn, D.A.; Grant, K.A. Chronic Ethanol Drinking Increases during the Luteal Menstrual Cycle Phase in Rhesus Monkeys: Implication of Progesterone and Related Neurosteroids. Psychopharmacology 2019, 236, 1817–1828. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Listabarth, S.; König, D.; Berlakovich, G.; Munda, P.; Ferenci, P.; Kollmann, D.; Gyöeri, G.; Waldhoer, T.; Groemer, M.; van Enckevort, A.; et al. Sex Disparities in Outcome of Patients with Alcohol-Related Liver Cirrhosis within the Eurotransplant Network—A Competing Risk Analysis. J. Clin. Med. 2022, 11, 3646. https://doi.org/10.3390/jcm11133646
Listabarth S, König D, Berlakovich G, Munda P, Ferenci P, Kollmann D, Gyöeri G, Waldhoer T, Groemer M, van Enckevort A, et al. Sex Disparities in Outcome of Patients with Alcohol-Related Liver Cirrhosis within the Eurotransplant Network—A Competing Risk Analysis. Journal of Clinical Medicine. 2022; 11(13):3646. https://doi.org/10.3390/jcm11133646
Chicago/Turabian StyleListabarth, Stephan, Daniel König, Gabriela Berlakovich, Petra Munda, Peter Ferenci, Dagmar Kollmann, Georg Gyöeri, Thomas Waldhoer, Magdalena Groemer, Arjan van Enckevort, and et al. 2022. "Sex Disparities in Outcome of Patients with Alcohol-Related Liver Cirrhosis within the Eurotransplant Network—A Competing Risk Analysis" Journal of Clinical Medicine 11, no. 13: 3646. https://doi.org/10.3390/jcm11133646