Electromyographic Response of the Abdominal Muscles and Stabilizers of the Trunk to Reflex Locomotion Therapy (RLT). A Preliminary Study

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
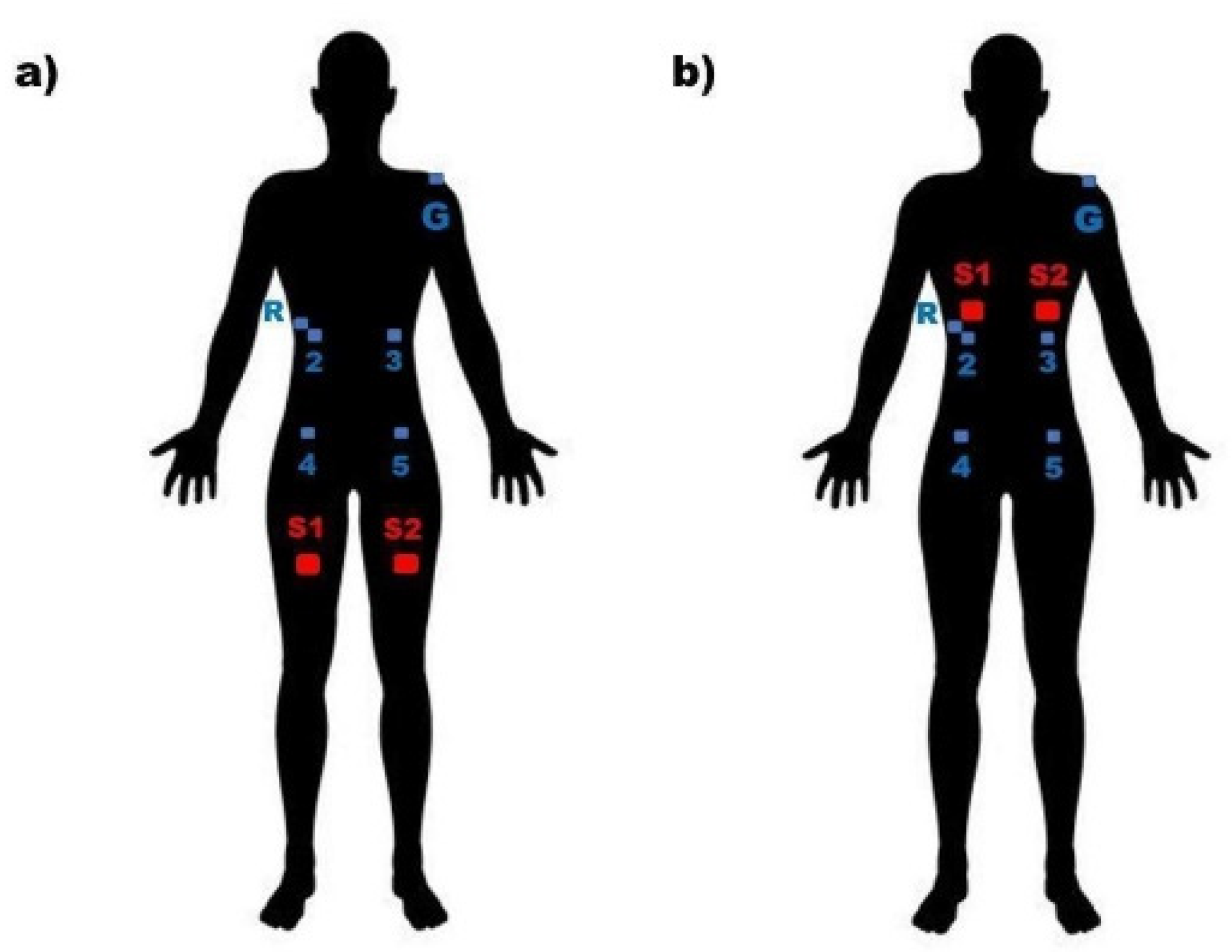
2.3. Tactile Stimuli Location
2.4. Electromyographic Recording (rEMG) Stimuli
- 10 min of absolute rest without EMG logging;
- 1 min of pre-stimulation rest with EMG registration (R1) non-STI condition;
- 2 min of non-STI right side styling condition with EMG (S1) registration;
- 1 min break with EMG (R2) non-STI condition.;
- 2 min of left side non-STI condition stimulation with EMG (S2) logging;
- 1 min of rest with EMG registration (R3) non-STI condition;
- 10 min of absolute rest without EMG logging;
- 1 min of pre-stimulation rest with EMG (R1) VSTI condition record;
- 2 min of right-side stimulation VSTI condition with EMG recording (S1);
- 1 min of rest with EMG registration (R2) VSTI condition;
- 2 min of left side stimulation VSTI condition with EMG recording (S2);
- 1 min standby with EMG (R3) VSTI condition.
2.5. rEMG Acquisition
2.6. rEMG Data Analysis
2.7. Descriptive Data Analysis
3. Results
3.1. Descriptive Data
3.2. Muscular Electrical Activity
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Popper, K.; Eccles, J. El yo y su Cerebro; Thieme, L., Ed.; Labor Univ.: Leipzig, Germany, 1984. [Google Scholar]
- Eibel-Eibesfeldt, I. Die Biologie des Menschlichen Verhaltens; Piper Münc.: Zürich, Switzerland, 1984. [Google Scholar]
- Vojta, V.; Schweitzer, E. El Descubrimiento de la Motricidad Ideal; Educación infantil y primaria: Darmstadt, Germany, 2009; pp. 13–14. [Google Scholar]
- Vojta, V. Alteraciones Motoras Cerebrales Infantiles. Diagnóstico y Tratamiento Precoz; Ediciones Morata: Madrid, Spain, 2005; pp. 132–133. [Google Scholar]
- Vojta, V.; Peters, A. The Vojta Principle; Springer-v: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Orth, H. El Niño en la Terapia Vojta; Educación infantil y primaria: Madrid, Spain, 2019; pp. 71–81. [Google Scholar]
- Sanz-Esteban, I.; Calvo-Lobo, C.; Ríos-Lago, M.; Álvarez-Linera, J.; Muñoz-García, D.; Rodríguez-Sanz, D. Mapping the human brain during a specific Vojta’s tactile input: The ipsilateral putamen’s role. Medicine 2018, 97, e0253. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Esteban, I.; Cano-De-La-Cuerda, R.; San-Martín-Gómez, A.; Jiménez-Antona, C.; Monge-Pereira, E.; Estrada-Barranco, C.; Serrano, J.I. Cortical activity during sensorial tactile stimulation in healthy adults through Vojta therapy. A randomized pilot controlled trial. J. Neuroeng. Rehabil. 2021, 18, 13. [Google Scholar] [CrossRef] [PubMed]
- Martínek, M.; Pánek, D.; Nováková, T.; Pavlů, D. Analysis of Intracerebral Activity during Reflex Locomotion Stimulation According to Vojta’s Principle. Appl. Sci. 2022, 12, 2225. [Google Scholar] [CrossRef]
- Jung, M.W.; Landenberger, M.; Jung, T.; Lindenthal, T.; Philippi, H. Vojta therapy and neurodevelopmental treatment in children with infantile postural asymmetry: A randomised controlled trial. J. Phys. Ther. Sci. 2017, 29, 301–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, S.Y.; Sung, Y.H. Effects of Vojta approach on diaphragm movement in children with spastic cerebral palsy. J. Exerc. Rehabilitation 2018, 14, 1005–1009. [Google Scholar] [CrossRef] [PubMed]
- Sung, Y.H.; Ha, S.Y. The Vojta approach changes thicknesses of abdominal muscles and gait in children with spastic cerebral palsy: A randomized controlled trial, pilot study. Technol. Health Care 2020, 28, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.Y.; Sung, Y.H. Vojta Approach Affects Neck Stability and Static Balance in Sitting Position of Children With Hypotonia. Int. Neurourol. J. 2021, 25, S90–S95. [Google Scholar] [CrossRef] [PubMed]
- Kiebzak, W.; Żurawski, A.; Głuszek, S.; Kosztołowicz, M.; Białek, W.A. Cortisol Levels in Infants with Central Coordination Disorders during Vojta Therapy. Children 2021, 8, 1113. [Google Scholar] [CrossRef] [PubMed]
- Epple, C.; Maurer-Burkhard, B.; Lichti, M.-C.; Steiner, T. Vojta therapy improves postural control in very early stroke rehabilitation: A randomised controlled pilot trial. Neurol. Res. Pract. 2020, 2, 23. [Google Scholar] [CrossRef] [PubMed]
- De-La-Barrera-Aranda, E.; Gonzalez-Gerez, J.J.; Saavedra-Hernandez, M.; Fernandez-Bueno, L.; Rodriguez-Blanco, C.; Bernal-Utrera, C. Vojta therapy in neuromotor development of pediatrics patients with periventricular leukomalacia: Case series. Medicina 2021, 57, 1149. [Google Scholar] [CrossRef] [PubMed]
- Lopez, L.P.; Palmero, N.V.; Ruano, L.G.; Pascual, C.S.L.; Orile, P.W.; Down, A.V.; Garcia-Fogeda, M.D.G.; Toré, S. The implementation of a reflex locomotion program according to Vojta produces short-term automatic postural control changes in patients with multiple sclerosis. J. Bodyw. Mov. Ther. 2021, 26, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Bauer, H.; Appaji, G.; Mundt, D. VOJTA neurophysiologic therapy. Indian J. Pediatrics 1992, 59, 37–51. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.; Kim, T. Effects of Vojta Therapy on Gait of Children with Spastic Diplegia. J. Phys. Ther. Sci. 2013, 25, 1605–1608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gajewska, E.; Huber, J.; Kulczyk, A.; Lipiec, J.; Sobieska, M. An attempt to explain the Vojta therapy mechanism of action using the surface polyelectromyography in healthy subjects: A pilot study. J. Bodyw. Mov. Ther. 2018, 22, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Esteban, I.; Cano-De-La-Cuerda, R.; San-Martin-Gomez, A.; Jimenez-Antona, C.; Monge-Pereira, E.; Estrada-Barranco, C.; Garcia-Sanchez, P.C.; Serrano, J.I. Innate Muscle Patterns Reproduction During Afferent Somatosensory Input With Vojta Therapy in Healthy Adults. A Randomized Controlled Trial. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 2232–2241. [Google Scholar] [CrossRef] [PubMed]
- Perales López, L.; Fernandez Aceñero, M. ¿Es transferible la terapia de locomoción refleja a una plataforma de teleneurorrehabilitación en el tratamiento del paciente adulto? Rehabilitación 2013, 47, 205–212. [Google Scholar] [CrossRef]
- Laufens, G.; Poltz, W.; Reimann, G.; Seitz, S. Alternating treadmill-Vojta-treadmill-therapy in patients with multiple sclerosis with severely affected gait. Phys. Med. Rehabil. Kurortmed. 2004, 14, 134–139. [Google Scholar]
- Laufens, G.; Poltz, W.; Reimann, G.; Seitz, S. Physiologische mechanismen bei der Vojta-physiotherapie an MS-patienten. Phys. Med. Rehabil. Kurortmed. 1994, 4, 1–4. [Google Scholar] [CrossRef]
- Hok, P.; Opavský, J.; Kutín, M.; Tüdös, Z.; Kaňovský, P.; Hluštík, P. Modulation of the sensorimotor system by sustained manual pressure stimulation. Neuroscience 2017, 348, 11–22. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Total Sample n = 27 | |
|---|---|
| Age (years) * | 20.58 (0.72) |
| Gender (female) ** | 23 (85.18) |
| Height (cm) * | 164.99 (6.18) |
| Weight (kg) * | 59.92 (9.38) |
| Body mass index (kg/m2) * | 21.94 (2.55) |
| Non-STI Condition n = 27 | VSTI Condition n = 27 | p * | Hedges’ g | ||
|---|---|---|---|---|---|
| REO | R1 | 1.003 (0.036) | 0.996 (0.026) | 0.562 | |
| S1 | 1.004 (0.054) | 1.123 (0.212) | 0.000 ** | 1.18 | |
| R2 | 0.997 (0.062) | 1.011 (0.065) | 0.050 | ||
| S2 | 0.991 (0.041) | 1.033 (0.097) | 0.006 ** | 0.62 | |
| R3 | 0.978 (0.076) | 1.004 (0.067) | 0.113 | ||
| LEO | R1 | 0.995 (0.033) | 1.007 (0.039) | 0.462 | |
| S1 | 1.004 (0.045) | 1.090 (0.144) | 0.000 ** | 1.01 | |
| R2 | 0.984 (0.056) | 1.015 (0.040) | 0.013 * | ||
| S2 | 0.991 (0.050) | 1.039 (0.102) | 0.001 ** | 0.51 | |
| R3 | 0.0992 (0.050) | 0.999 (0.040) | 0.159 | ||
| RIO | R1 | 1.003 (0.044) | 1.011 (0.027) | 0.634 | |
| S1 | 1.005 (0.049) | 1.147 (0.247) | 0.000 ** | 1.17 | |
| R2 | 0.990 (0.052) | 1.018 (0.051) | 0.001 ** | ||
| S2 | 0.995 (0.047) | 1.047 (0.181) | 0.001 ** | 0.61 | |
| R3 | 0.993 (0.077) | 1.008 (0.035) | 0.192 | ||
| LIO | R1 | 0.999 (0.077) | 0.998 (0.024) | 0.337 | |
| S1 | 1.000 (0.018) | 1.031 (0.157) | 0.000 ** | 1.06 | |
| R2 | 0.999 (0.020) | 1.003 (0.019) | 0.473 | ||
| S2 | 1.000 (0.022) | 1.009 (0.022) | 0.065 | 0.32 | |
| R3 | 0.999 (0.027) | 0.995 (0.024) | 0.373 |
| Non-STI Condition n = 27 | VSTI Condition n = 27 | P++ Inter-condition | ||||
|---|---|---|---|---|---|---|
| % Difference | p * | % Difference | p * | |||
| REO | ||||||
| S1–R1 | 0.0 (2.9) | 0.361 | 11.7 (20.6) | 0.000 | 0.000 | |
| S2–R2 | 0.0 (2.5) | 0.923 | 18.3 (9.2) | 0.037 | 0.174 | |
| R3–R1 | −3.5 (10.8) | 0.008 | −0.2 (7.7) | 0.239 | 0.130 | |
| S2–S1 | −1.9 (5.4) | 0.034 | −9.5 (16.3) | 0.002 | 0.030 | |
| LEO | ||||||
| S1–R1 | 0.2 (2.5) | 0.414 | 7.2 (16.0) | 0.000 | 0.000 | |
| S2–R2 | −0.3 (1.7) | 0.701 | 0.9 (7.7) | 0.032 | 0.110 | |
| R3–R1 | −1.5 (2.6) | 0.021 | 0.1 (3.0) | 0.361 | 0.186 | |
| S2–S1 | −0.7 (2.0) | 0.022 | −5.3 (8.5) | 0.002 | 0.033 | |
| RIO | ||||||
| S1–R1 | 0.1 (3.3) | 0.792 | 13.1 (23.4) | 0.000 | 0.000 | |
| S2–R2 | 0.4 (3.1) | 0.755 | 1.2 (16.4) | 0.025 | 0.130 | |
| R3–R1 | −1.0 (6.1) | 0.118 | −0.1 (2.9) | 0.829 | 0.216 | |
| S2–S1 | −0.1 (2.8) | 0.212 | −4.8 (20.0) | 0.001 | 0.008 | |
| LIO | ||||||
| S1–R1 | 0.1 (1.2) | 0.719 | 2.6 (15.6) | 0.000 | 0.000 | |
| S2–R2 | −0.0 (1.5) | 0.866 | 1.3 (1.7) | 0.107 | 0.149 | |
| R3–R1 | 0.2 (2.5) | 0.981 | −0.00 (1.9) | 0.904 | 0.710 | |
| S2–S1 | −0.2 (1.2) | 0.866 | −1.9 (10.7) | 0.005 | 0.012 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Robledo, F.; Sánchez-González, J.L.; Bermejo-Gil, B.M.; Llamas-Ramos, R.; Llamas-Ramos, I.; de la Fuente, A.; Martín-Nogueras, A.M. Electromyographic Response of the Abdominal Muscles and Stabilizers of the Trunk to Reflex Locomotion Therapy (RLT). A Preliminary Study. J. Clin. Med. 2022, 11, 3866. https://doi.org/10.3390/jcm11133866
Pérez-Robledo F, Sánchez-González JL, Bermejo-Gil BM, Llamas-Ramos R, Llamas-Ramos I, de la Fuente A, Martín-Nogueras AM. Electromyographic Response of the Abdominal Muscles and Stabilizers of the Trunk to Reflex Locomotion Therapy (RLT). A Preliminary Study. Journal of Clinical Medicine. 2022; 11(13):3866. https://doi.org/10.3390/jcm11133866
Chicago/Turabian StylePérez-Robledo, Fátima, Juan Luis Sánchez-González, Beatriz María Bermejo-Gil, Rocío Llamas-Ramos, Inés Llamas-Ramos, Antonio de la Fuente, and Ana María Martín-Nogueras. 2022. "Electromyographic Response of the Abdominal Muscles and Stabilizers of the Trunk to Reflex Locomotion Therapy (RLT). A Preliminary Study" Journal of Clinical Medicine 11, no. 13: 3866. https://doi.org/10.3390/jcm11133866
APA StylePérez-Robledo, F., Sánchez-González, J. L., Bermejo-Gil, B. M., Llamas-Ramos, R., Llamas-Ramos, I., de la Fuente, A., & Martín-Nogueras, A. M. (2022). Electromyographic Response of the Abdominal Muscles and Stabilizers of the Trunk to Reflex Locomotion Therapy (RLT). A Preliminary Study. Journal of Clinical Medicine, 11(13), 3866. https://doi.org/10.3390/jcm11133866