
Early Intensive Physical Rehabilitation Combined with a Protocolized Decannulation Process in Tracheostomized Survivors from Severe COVID-19 Pneumonia with Chronic Critical Illness


 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Ethical Considerations
2.2. Intervention
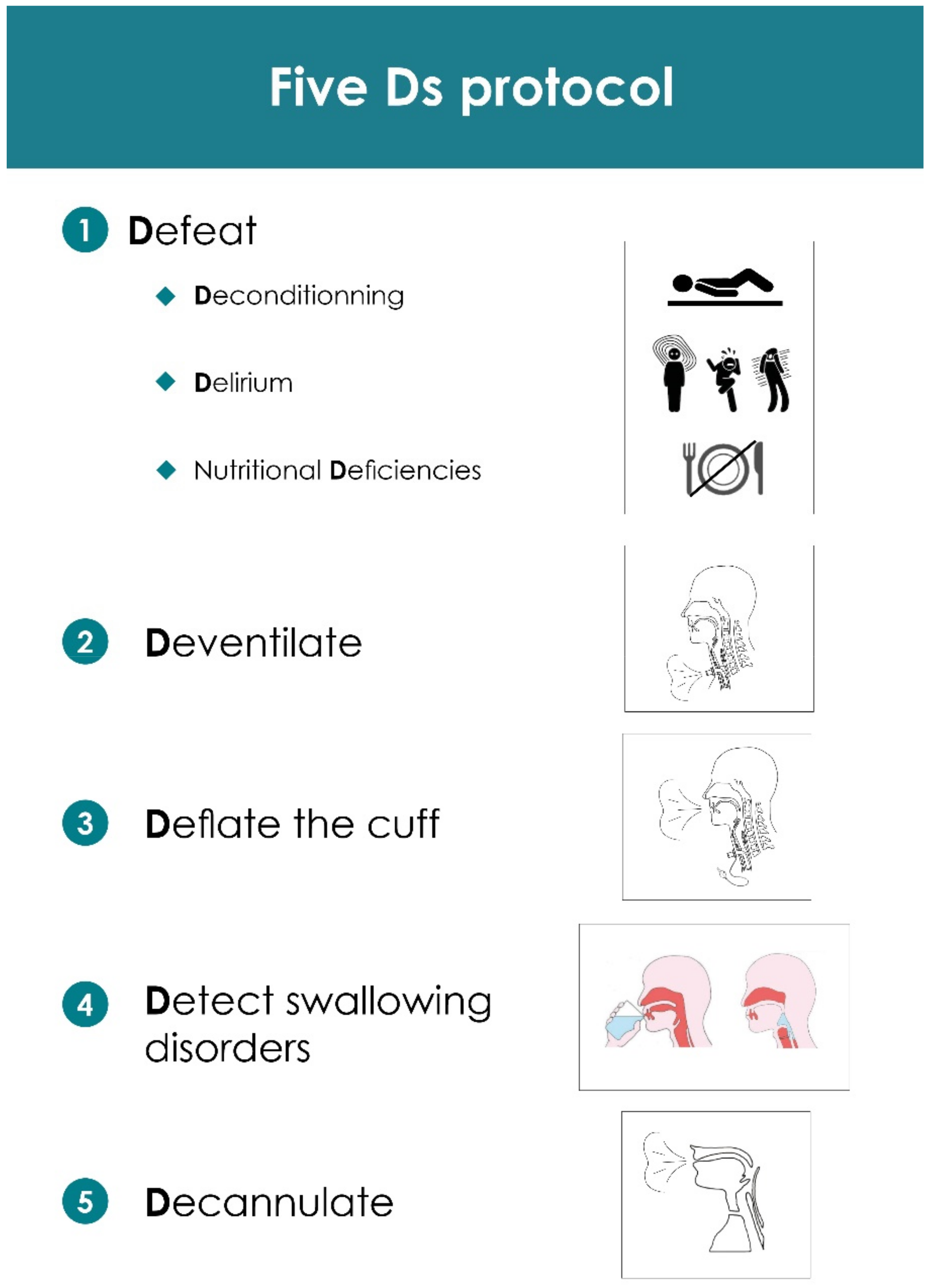
- Tracheostomy was performed early (beyond 10 days of mechanical ventilation) to facilitate the sedation withdrawal, to improve patient’s comfort and to secure the airway access, especially when the patient was moved [7]. Patients were mobilized, taken out of bed and put in a chair as soon as possible. Anything that interfered with the patient’s mobilization was removed, which included useless catheters, central venous access and continuous infusion syringe pumps. A percutaneous gastrostomy was also performed to more actively provide the prolonged nutritional support and protein intake required for such a long-lasting resuscitation process [8].
- Disconnection from the ventilator was obtained only after a gradual decrease in ventilatory assistance by decreasing the inspiratory support step by step or by lengthening the periods of spontaneous ventilation [9]. Inspiratory muscle training—through repetitive short inspiratory efforts against a resistive valve—was added to shorten the duration of the ventilatory support [10]. Considering that the night is a recovery period, nocturnal ventilatory assistance was maintained until the patient was able to hold out for 12 h without the help of the ventilator for at least 2 consecutive days [11]. This step was facilitated when a thinner tracheostomy tube was used (7 mm of internal diameter, for instance), providing that the cuff was deflated and a one-way speaking valve was connected to the proximal part of the cannula. This strategy enabled the patient to go through steps 2, 3 and 4 at once and drastically shortened the weaning process from mechanical ventilation.
- Using a one-way speaking Passy Muir valve not only accelerates the restoration of the aerodigestive tract functions of the larynx, such as speech, cough and swallow, but it also reduces the risk of aspiration and the need for suctioning [12]. We used this strategy as soon as the patient could be disconnected from the ventilator.
- Tracheostomized critically ill patients often exhibit clinically undetectable episodes of aspiration (called silent aspirations) [13]. That is why a fiberoptic examination of the upper airways with a blue dye swallowing test was part of the protocol, to control the anatomical and functional integrity of the larynx.
- The cannula was removed when the whole step-by-step process was completed.
2.3. Evaluation Criteria
2.4. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lemyze, M.; Courageux, N.; Maladobry, T.; Arumadura, C.; Pauquet, P.; Orfi, A.; Komorowski, M.; Mallat, J.; Granier, M. Implications of Obesity for the Management of Severe Coronavirus Disease 2019 Pneumonia. Crit. Care Med. 2020, 48, e761–e767. [Google Scholar] [CrossRef] [PubMed]
- Van Aerde, N.; Van den Berghe, G.; Wilmer, A.; Gosselink, R.; Hermans, G. Intensive care unit acquired muscle weakness in COVID-19 patients. Intensive Care Med. 2020, 46, 2083–2085. [Google Scholar] [CrossRef]
- Iwashyna, T.J.; Hodgson, C.L.; Pilcher, D.; Bailey, M.; van Lint, A.; Chavan, S.; Bellomo, R. Timing of onset and burden of persistent critical illness in Australia and New Zealand: A retrospective, population-based, observational study. Lancet Respir. Med. 2016, 4, 566–573. [Google Scholar] [CrossRef]
- Bigatello, L.M.; Stelfox, H.T.; Berra, L.; Schmidt, U.; Gettings, E.M. Outcome of patients undergoing prolonged mechanical ventilation after critical illness. Crit. Care Med. 2007, 35, 2491–2497. [Google Scholar] [CrossRef] [PubMed]
- Scheinhorn, D.J.; Hassenpflug, M.S.; Votto, J.J.; Chao, D.C.; Epstein, S.K.; Doig, G.S.; Knight, E.B.; Petrak, R.A. Ventilator-dependent survivors of catastrophic illness transferred to 23 long-term care hospitals for weaning from prolonged mechanical ventilation. Chest 2007, 131, 76–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unroe, M.; Kahn, J.M.; Carson, S.S.; Govert, J.A.; Martinu, T.; Sathy, S.J.; Clay, A.S.; Chia, J.; Gray, A.; Tulsky, J.A.; et al. One-year trajectories of care and resource utilization for recipients of prolonged mechanical ventilation: A cohort study. Ann. Intern. Med. 2010, 153, 167–175. [Google Scholar] [CrossRef]
- Nieszkowska, A.; Combes, A.; Luyt, C.E.; Ksibi, H.; Trouillet, J.L.; Gibert, C.; Chastre, J. Impact of tracheotomy on sedative administration, sedation level, and comfort of mechanically ventilated intensive care unit patients. Crit. Care Med. 2005, 33, 2527–2533. [Google Scholar] [CrossRef]
- Kiser, S.B.; Sciacca, K.; Jain, N.; Leiter, R.; Mazzola, E.; Gelfand, S.; Jehle, J.; Bernacki, R.; Lamas, D.; Cooper, Z.; et al. A Retrospective Observational Study Exploring 30- and 90-Day Outcomes for Patients with COVID-19 after Percutaneous Tracheostomy and Gastrostomy Placement. Crit. Care Med. 2022, 50, 819–824. [Google Scholar] [CrossRef]
- Vitacca, M.; Vianello, A.; Colombo, D.; Clini, E.; Porta, R.; Bianchi, L.; Arcaro, G.; Vitale, G.; Guffanti, E.; Coco, A.L.; et al. Comparison of two methods for weaning patients with chronic obstructive pulmonary disease requiring mechanical ventilation for more than 15 days. Am. J. Respir. Crit. Care Med. 2001, 164, 225–230. [Google Scholar] [CrossRef]
- Martin, A.D.; Smith, B.K.; Davenport, P.D.; Harman, E.; Gonzalez-Rothi, R.J.; Baz, M.; Layon, A.J.; Banner, M.J.; Caruso, L.J.; Deoghare, H.; et al. Inspiratory muscle strength training improves weaning outcome in failure to wean patients: A randomized trial. Crit. Care 2011, 15, R84. [Google Scholar] [CrossRef] [Green Version]
- Rittayamai, N.; Wilcox, E.; Drouot, X.; Mehta, S.; Goffi, A.; Brochard, L. Positive and negative effects of mechanical ventilation on sleep in the ICU: A review with clinical recommendations. Intensive Care Med. 2016, 42, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Dettelbach, M.A.; Gross, R.D.; Mahlmann, J.; Eibling, D.E. Effect of the Passy-Muir Valve on aspiration in patients with tracheostomy. Head Neck 1995, 17, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Elpern, E.H.; Scott, M.G.; Petro, L.; Ries, M.H. Pulmonary aspiration in mechanically ventilated patients with tracheostomies. Chest 1994, 105, 563–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Katz, S.; Downs, T.D.; Cash, H.R.; Grotz, R.C. Progress in development of the index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Herridge, M.S.; Chu, L.M.; Matte, A.; Tomlinson, G.; Chan, L.; Thomas, C.; Friedrich, J.O.; Mehta, S.; Lamontagne, F.; Levasseur, M.; et al. The RECOVER Program: Disability Risk Groups and 1-Year Outcome after 7 or More Days of Mechanical Ventilation. Am. J. Respir. Crit. Care Med. 2016, 194, 831–844. [Google Scholar] [CrossRef]
- Kinoshita, T.; Nishimura, Y.; Umemoto, Y.; Fujita, Y.; Kouda, K.; Yasuoka, Y.; Miyamoto, K.; Kato, S.; Tajima, F. The Effects of Early Rehabilitation in the Intensive Care Unit for Patients with Severe COVID-19 Pneumonia: A Retrospective Cohort Study. J. Clin. Med. 2022, 11, 357. [Google Scholar] [CrossRef]
- Stutz, M.R.; Leonhard, A.G.; Ward, C.M.; Pearson, S.D.; Osorio, P.L.; Herbst, P.R.; Wolfe, K.S.; Pohlman, A.S.; Hall, J.B.; Kress, J.P.; et al. Early Rehabilitation Feasibility in a COVID-19 ICU. Chest 2021, 160, 2146–2148. [Google Scholar] [CrossRef]
- Faure, M.; Decavèle, M.; Morawiec, E.; Dres, M.; Gatulle, N.; Mayaux, J.; Stefanescu, F.; Caliez, J.; Similowski, T.; Delemazure, J.; et al. Specialized Weaning Unit in the Trajectory of SARS-CoV-2 ARDS: Influence of Limb Muscle Strength on Decannulation and Rehabilitation. Respir. Care 2022, 67, respcare.09602. [Google Scholar] [CrossRef] [PubMed]
- Pohlman, M.C.; Schweickert, W.D.; Pohlman, A.S.; Nigos, C.; Pawlik, A.J.; Esbrook, C.L.; Spears, L.; Miller, M.; Franczyk, M.; Deprizio, D.; et al. Feasibility of physical and occupational therapy beginning from initiation of mechanical ventilation. Crit. Care Med. 2010, 38, 2089–2094. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters | ICU Admission | Post ICU | Post Rehab | p |
|---|---|---|---|---|
| Age | 66 (62–68) | |||
| Male, n (%) | 36 (77%) | |||
| Weight (Kg) | 88.5 (80–102) | 80.5 (71–89) | <0.001 | |
| BMI (kg/m²) | 31.4 (26–34) | |||
| Frailty Score | 2 (2–3) | 7 (7–7) | 3 (2–3) | <0.001 |
| ADL | 6 (6–6) | 0 (0–0.25) | 6 (6–6) | <0.001 |
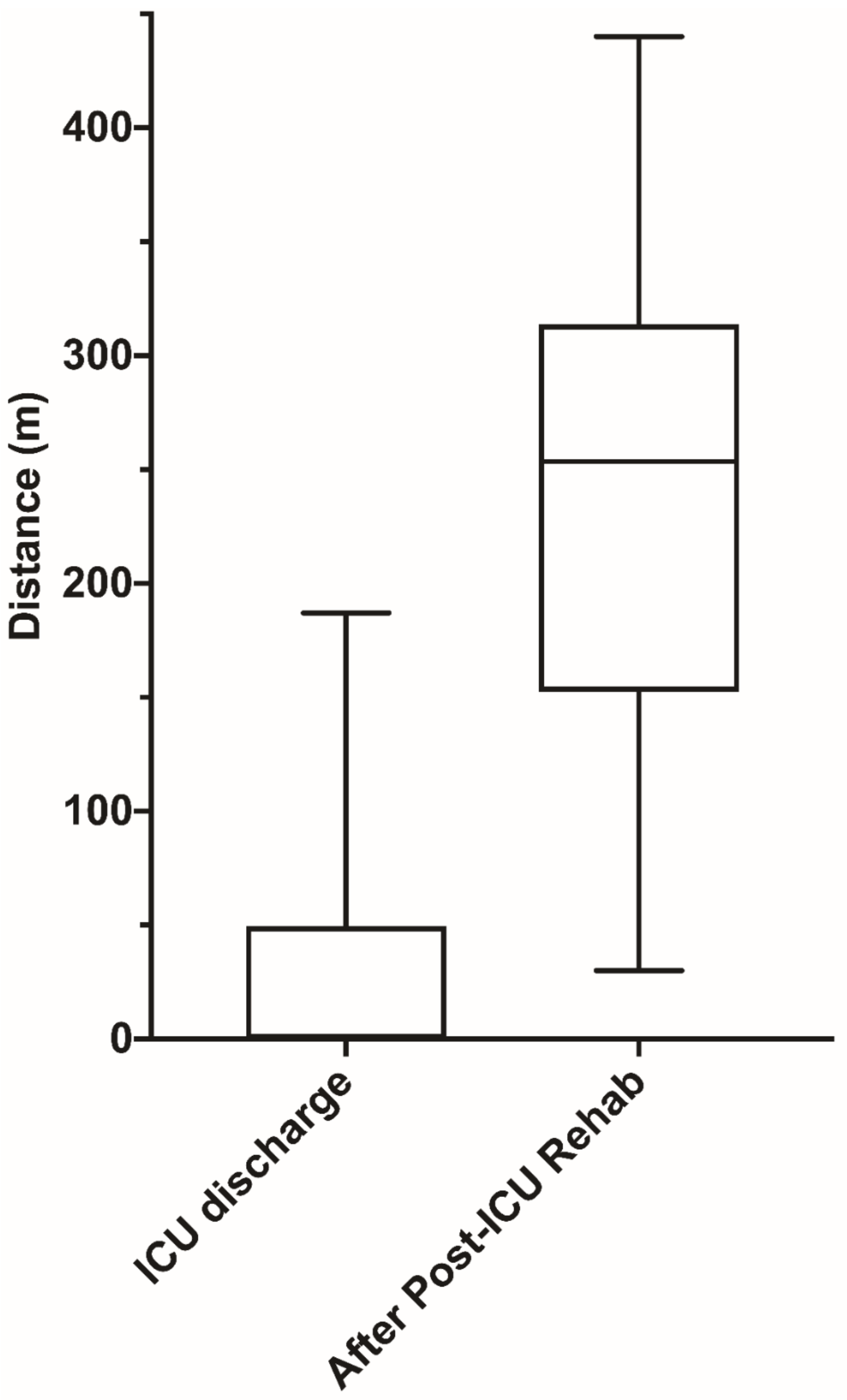
| 6′WT distance (m) | 0 (0–49) | 253 (155–312) | <0.001 | |
| HADS | 18 (14–22) | 10 (7–13) | <0.001 | |
| Anxiety | 12 (10–13) | 7 (4–10) | <0.001 | |
| Depression | 6 (5–10) | 2 (1–4) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lemyze, M.; Komorowski, M.; Mallat, J.; Arumadura, C.; Pauquet, P.; Kos, A.; Granier, M.; Grosbois, J.-M. Early Intensive Physical Rehabilitation Combined with a Protocolized Decannulation Process in Tracheostomized Survivors from Severe COVID-19 Pneumonia with Chronic Critical Illness. J. Clin. Med. 2022, 11, 3921. https://doi.org/10.3390/jcm11133921
Lemyze M, Komorowski M, Mallat J, Arumadura C, Pauquet P, Kos A, Granier M, Grosbois J-M. Early Intensive Physical Rehabilitation Combined with a Protocolized Decannulation Process in Tracheostomized Survivors from Severe COVID-19 Pneumonia with Chronic Critical Illness. Journal of Clinical Medicine. 2022; 11(13):3921. https://doi.org/10.3390/jcm11133921
Chicago/Turabian StyleLemyze, Malcolm, Matthieu Komorowski, Jihad Mallat, Clotilde Arumadura, Philippe Pauquet, Adrien Kos, Maxime Granier, and Jean-Marie Grosbois. 2022. "Early Intensive Physical Rehabilitation Combined with a Protocolized Decannulation Process in Tracheostomized Survivors from Severe COVID-19 Pneumonia with Chronic Critical Illness" Journal of Clinical Medicine 11, no. 13: 3921. https://doi.org/10.3390/jcm11133921
APA StyleLemyze, M., Komorowski, M., Mallat, J., Arumadura, C., Pauquet, P., Kos, A., Granier, M., & Grosbois, J.-M. (2022). Early Intensive Physical Rehabilitation Combined with a Protocolized Decannulation Process in Tracheostomized Survivors from Severe COVID-19 Pneumonia with Chronic Critical Illness. Journal of Clinical Medicine, 11(13), 3921. https://doi.org/10.3390/jcm11133921