
Impact of Chronic Bronchial Infection by Staphylococcus aureus on Bronchiectasis

 , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
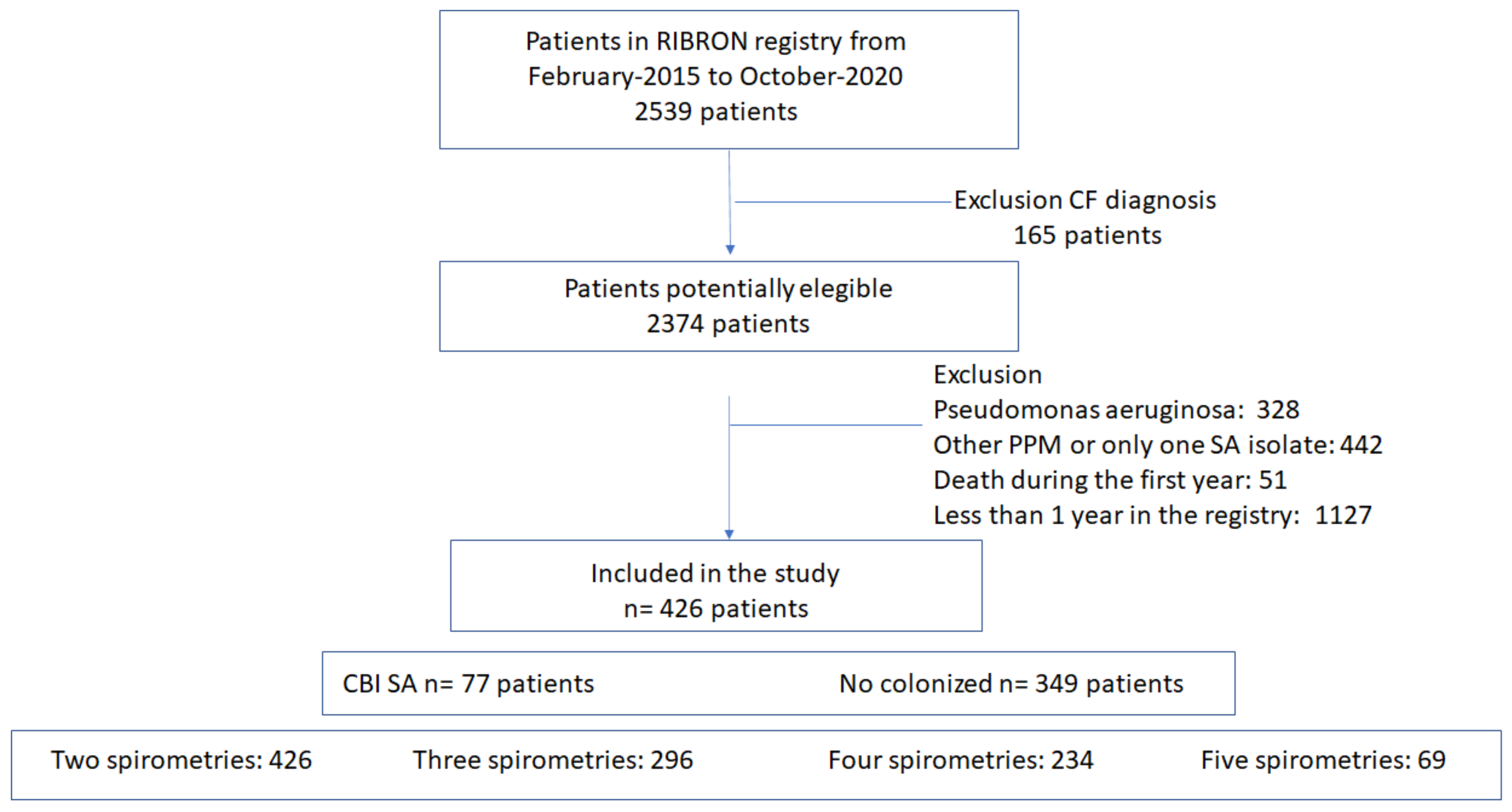
2.1. Design
2.2. Population
2.3. Variables
2.4. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Factors Associated with CBI by SA
Univariate Analysis
3.3. Multivariate Analysis
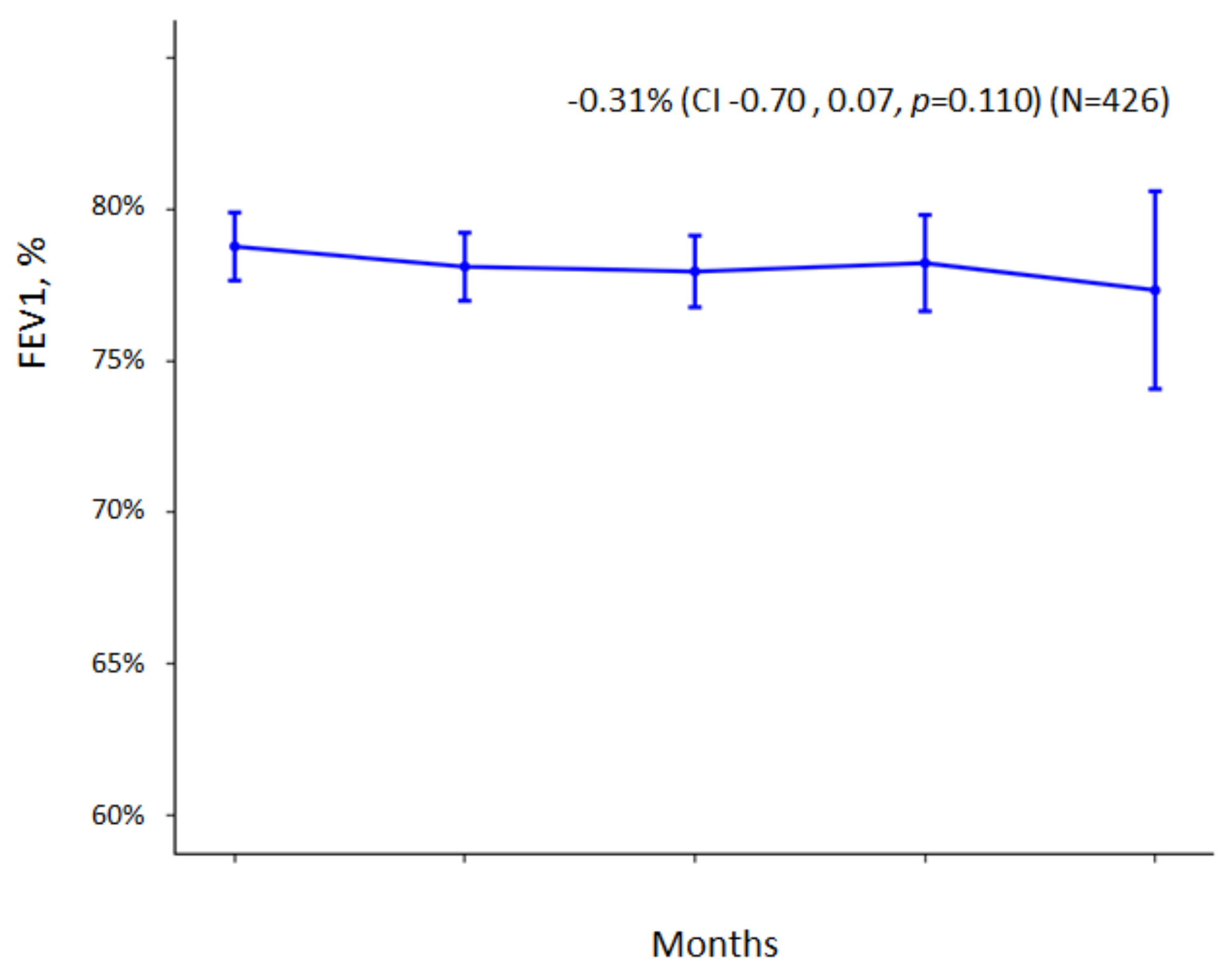
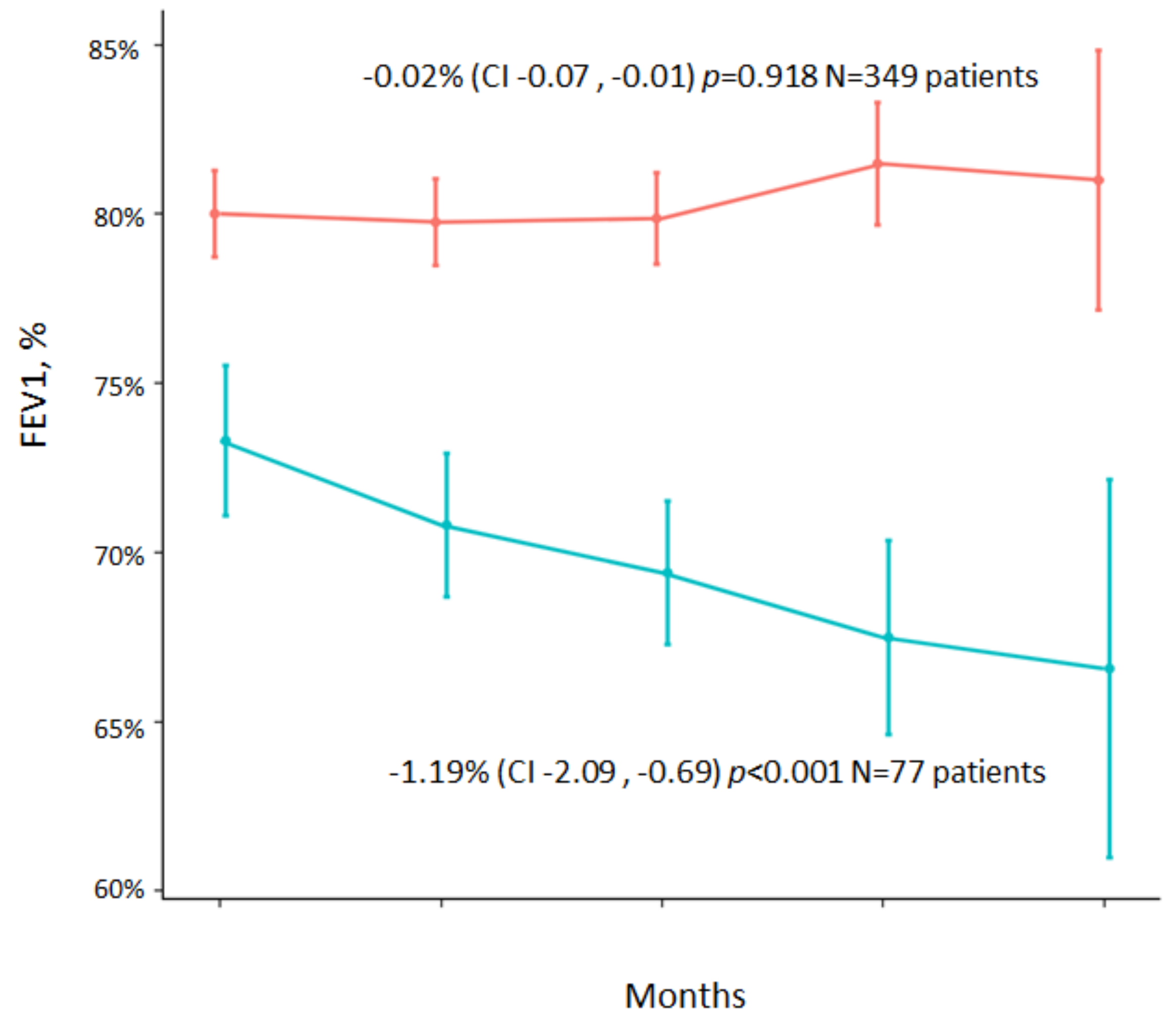
Impact of CBI Caused by SA on Lung Function
4. Discussion
Limitations of the Current Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flume, P.A.; Chalmers, J.D.; Olivier, K.N. Advances in bronchiectasis: Endotyping, genetics, microbiome, and disease heterogeneity. Lancet 2018, 392, 880–890. [Google Scholar] [CrossRef] [Green Version]
- Martínez-García, M.; Máiz, L.; Olveira, C.; Girón, R.M.; De La Rosa, D.; Blanco, M.; Cantón, R.; Vendrell, M.; Polverino, E.; De Gracia, J.; et al. Spanish guidelines on the evaluation and diagnosis of bronchiectasis in adults. Arch. Bronconeumol. 2018, 54, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.T.; Sullivan, A.L.; Chalmers, J.D.; De Soyza, A.; Elborn, J.S.; Floto, R.A.; Grillo, L.; Gruffydd-Jones, K.; Harvey, A.; Haworth, C.S.; et al. British Thoracic Society Guideline for bronchiectasis in adults. Thorax 2018, 74, 1–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monsó, E. Look at the wood and not at the tree: The Microbiome in Chronic Obstructive Lung Disease and Cystic Fibrosis. Arch. Bronconeumol. 2020, 56, 5–6. [Google Scholar] [CrossRef]
- Chen, C.L.; Huang, Y.; Yuan, J.J.; Li, H.M.; Han, X.R.; Martinez-Garcia, M.A.; de la Rosa-Carrillo, D.; Chen, R.C.; Guan, W.J.; Zhong, N.S. The roles of the bacteria and viruses in bronchiectasis exacerbation: A prospective Study. Arch. Bronconeumol. 2020, 56, 621–629. [Google Scholar] [CrossRef]
- Martinez-Garcia, M.A.; Posadas, T.; Sotgiu, G.; Blasi, F.; Saderi, L.; Aliberti, S. Repeteability of Circulating Eosinophil Measures and Inhaled Corticosteroids Effect in Bronchiectasis. A Post Hoc Analysis of a Randomized Clinical Trial. Arch. Bronconeumol. 2020, 56, 681–683. [Google Scholar] [CrossRef]
- Martinez-Garcia, M.A. Bronchiectasis and eosinophils. Arch. Bronconeumol. 2021, 57, 671–672. [Google Scholar] [CrossRef]
- Posadas, T.; Oscullo, G.; Zaldivar, E.; Villa, C.; Dobarganes, Y.; Girón, R.; Olveira, C.; Maíz, L.; García-Clemente, M.; Sibila, O.; et al. C-Reactive Protein Concentration in Steady-State Bronchiectasis: Prognostic Value of Future Severe Exacerbations. Data From the Spanish Registry of Bronchiectasis (RIBRON). Arch. Bronconeumol. 2021, 57, 21–27. [Google Scholar] [CrossRef]
- Martinez-García, M.; Oscullo, G.; Posadas, T.; Zaldivar, E.; Villa, C.; Dobarganes, Y.; Girón, R.; Olveira, C.; Maíz, L.; García-Clemente, M.; et al. Pseudomonas aeruginosa and lung function decline in patients with bronchiectasis. Clin. Microbiol. Infect. 2021, 27, 428–434. [Google Scholar] [CrossRef]
- Vidaillac, C.; Chotirmall, S.H. Pseudomonas aeruginosa in bronchiectasis: Infection, inflammation, and therapies. Expert Rev. Respir. Med. 2021, 15, 649–662. [Google Scholar] [CrossRef]
- Araújo, D.; Shteinberg, M.; Aliberti, S.; Goeminne, P.C.; Hill, A.T.; Fardon, T.C.; Obradovic, D.; Stone, G.; Trautmann, M.; Davis, A.; et al. The independent contribution of Pseudomonas aeruginosa infection to long-term clinical outcomes in bronchiectasis. Eur. Respir. J. 2018, 51, 1701953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finch, S.; McDonnell, M.J.; Abo-Leyah, H.; Aliberti, S.; Chalmers, J.D. A comprehensive analysis of the impact of Pseudomonas aeruginosa colonization on prognosis in adult bronchiectasis. Ann. Am. Thorac. Soc. 2015, 12, 1602–1611. [Google Scholar] [PubMed] [Green Version]
- Martins, K.B.; Olmedo, D.W.V.; Paz, M.M.; Ramos, D.F. Staphylococcus aureus and its Effects on the Prognosis of Bronchiectasis. Microb. Drug Resist. 2021, 27, 823–834. [Google Scholar] [CrossRef] [PubMed]
- King, P.; Holdsworth, S.; Freezer, N.; Holmes, P. Bronchiectasis. Intern. Med. J. 2006, 36, 729–737. [Google Scholar] [CrossRef]
- Salsgiver, E.L.; Fink, A.K.; Knapp, E.A.; LiPuma, J.J.; Olivier, K.N.; Marshall, B.C.; Saiman, L. Changing Epidemiology of the Respiratory Bacteriology of Patients With Cystic Fibrosis. Chest 2016, 149, 390–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-García, M.A.; Villa, C.; Dobarganes, Y.; Girón, R.; Maíz, L.; García-Clemente, M.; Sibila, O.; Golpe, R.; Rodríguez, J.; Barreiro, E.; et al. RIBRON: The Spanish online bronchiectasis registry. Characterization of the first 1912 patients. Arch. Bronconeumol. 2021, 57, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Shrestha, B.; Dunn, L. The Declaration of Helsinki on Medical Research involving Human Subjects: A Review of Seventh Revision. J. Nepal. Health Res. Counc. 2020, 17, 548–552. [Google Scholar] [CrossRef]
- Polverino, E.; Goeminne, P.C.; McDonnell, M.J.; Aliberti, S.; Marshall, S.E.; Loebinger, M.R.; Murris, M.; Cantón, R.; Torres, A.; Dimakou, K.; et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur. Respir. J. Off. J. Eur. Soc. Clin. Respir. Physiol. 2017, 50, 1700629. [Google Scholar] [CrossRef]
- Aliberti, S.; Masefield, S.; Polverino, E.; De Soyza, A.; Loebinger, M.R.; Menendez, R.; Ringshausen, F.C.; Vendrell, M.; Powell, P.; Chalmers, J.D. Research priorities in bronchiectasis: A consensus statement from the EMBARC Clinical Research Collaboration. Eur. Respir. J. 2016, 48, 632–647. [Google Scholar] [CrossRef] [Green Version]
- Aliberti, S.; Goeminne, P.C.; O’Donnell, A.E.; Aksamit, T.R.; Al-Jahdali, H.; Barker, A.F.; Blasi, F.; Boersma, W.G.; Crichton, M.L.; De Soyza, A.; et al. Criteria and definitions for the radiological and clinical diagnosis of bronchiectasis in adults for use in clinical trials: International consensus recommendations. Lancet Respir. Med. 2021, 10, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.T.; Haworth, C.S.; Aliberti, S.; Barker, A.; Blasi, F.; Boersma, W.; Chalmers, J.D.; De Soyza, A.; Dimakou, K.; Elborn, J.S.; et al. Pulmonary exacerbation in adults with bronchiectasis: A consensus definition for clinical research. Eur. Respir. J. 2017, 49, 1700051. [Google Scholar] [CrossRef] [PubMed]
- Martínez-García, M.A.; De Gracia, J.; Vendrell Relat, M.; Girón, R.M.; Maiz Carro, L.; de la Rosa Carrillo, D.; Olveira, C. Multidimensional approach to non-cystic fibrosis bronchiectasis: The FACED score. Eur. Respir. J. 2014, 43, 1357–1367. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Garcia, M.A.; Athanazio, R.A.; Girón, R.; Máiz-Carro, L.; de la Rosa, D.; Olveira, C.; De Gracia, J.; Vendrell, M.; Prados-Sánchez, C.; Gramblicka, G.; et al. Predicting high risk of exacerbations in bronchiectasis: The E-FACED score. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 275–284. [Google Scholar] [CrossRef] [Green Version]
- Chalmers, J.D.; Goeminne, P.; Aliberti, S.; McDonnell, M.J.; Lonni, S.; Davidson, J.; Poppelwell, L.; Salih, W.; Pesci, A.; Dupont, L.J.; et al. The Bronchiectasis Severity Index. An International Derivation and Validation Study. Am. J. Respir. Crit. Care Med. 2014, 189, 576–585. [Google Scholar] [CrossRef] [Green Version]
- Sanchis, J.; Casan, P.; Castillo, J.; González, N.; Palenciano, L.; Roca, J. Normativas para la práctica de la espirometría forzada. Arch. Bronconeumol. 1989, 25, 132–142. [Google Scholar]
- De la Rosa Carrillo, D.; López-Campos, J.L.; Alcázar Navarrete, B.; Calle Rubio, M.; Cantón Moreno, R.; García-Rivero, J.L.; Máiz Carro, L.; Olveira Fuster, C.; Martínez-García, M.Á.; Comité Asesor del Documento; et al. Consensus Document on the Diagnosis and Treatment of Chronic Bronchial Infection in Chronic Obstructive Pulmonary Disease. Arch. Bronconeumol. 2020, 56, 651–664. [Google Scholar] [CrossRef]
- Angrill, J.; Agustí, C.; de Celis, R.; Rañó, A.; Gonzalez, J.; Solé, T.; Xaubet, A.; Rodriguez-Roisin, R.; Torres, A. Bacterial colonization in patients with bronchiectasis: Microbiological pattern and risk factors. Thorax 2002, 57, 15–19. [Google Scholar] [CrossRef] [Green Version]
- King, P.T.; Holdsworth, S.R.; Freezer, N.J.; Villanueva, E.; Holmes, P.W. Microbiologic follow-up study in adult bronchiectasis. Respir. Med. 2007, 101, 1633–1638. [Google Scholar] [CrossRef] [Green Version]
- Li, A.M.; Sonnappa, S.; Lex, C.; Wong, E.; Zacharasiewicz, A.; Bush, A.; Jaffe, A. Non-CF bronchiectasis: Does knowing the aetiology lead to changes in management? Eur. Respir. J. 2005, 26, 8–14. [Google Scholar] [CrossRef]
- Nicotra, M.B.; Rivera, M.; Dale, A.M.; Shepherd, R.; Carter, R. Clinical, Pathophysiologic, and Microbiologic Characterization of Bronchiectasis in an Aging Cohort. Chest 1995, 108, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.; Mawdsley, S.; Nash, K.; Cullinan, P.; Cole, P.; Wilson, R. Determinants of chronic infection with Staphylococcus aureus in patients with bronchiectasis. Eur. Respir. J. 1999, 14, 1340–1345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somayaji, R.; Ramos, K.J.; Hoffman, L.R. Understanding the Role of Staphylococcus aureus in Non-Cystic Fibrosis Bronchiectasis: Where Are We Now? Ann. Am. Thorac. Soc. 2018, 15, 310–311. [Google Scholar] [CrossRef] [PubMed]
- Metersky, M.L.; Aksamit, T.R.; Barker, A.; Choate, R.; Daley, C.L.; Daniels, L.A.; DiMango, A.; Eden, E.; Griffith, D.; Johnson, M.; et al. The Prevalence and Significance of Staphylococcus aureus in Patients with Non–Cystic Fibrosis Bronchiectasis. Ann. Am. Thorac. Soc. 2018, 15, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Baindara, P. Host-directed therapies to combat tuberculosis and associated non-communicable diseases. Microb. Pathog. 2019, 130, 156–168. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, B.; Cox, M.J.; Cuthbertson, L.; James, P.; Cookson, W.O.C.; Davies, J.; Moffatt, M.F.; Bush, A. Longitudinal development of the airway microbiota in infants with cystic fibrosis. Sci. Rep. 2019, 9, 5143. [Google Scholar] [CrossRef]
- Caudri, D.; Turkovic, L.; Ng, J.; de Klerk, N.; Rosenow, T.; Hall, G.; Ranganathan, S.; Sly, P.; Stick, S. The association between Staphylococcus aureus and subsequent bronchiectasis in children with cystic fibrosis. J. Cyst. Fibros. 2018, 17, 462–469. [Google Scholar] [CrossRef]
- Goss, C.H.; Muhlebach, M.S. Review: Staphylococcus aureus and MRSA in cystic fibrosis. J. Cyst. Fibros. 2011, 10, 298–306. [Google Scholar] [CrossRef] [Green Version]
- LiPuma, J.J. The Changing Microbial Epidemiology in Cystic Fibrosis. Clin. Microbiol. Rev. 2010, 23, 299–323. [Google Scholar] [CrossRef] [Green Version]
- Lyczak, J.B.; Cannon, C.L.; Pier, G.B. Lung Infections Associated with Cystic Fibrosis. Clin. Microbiol. Rev. 2002, 15, 194–222. [Google Scholar] [CrossRef] [Green Version]
- Schneider, M.; Mühlemann, K.; Droz, S.; Couzinet, S.; Casaulta, C.; Zimmerli, S. Clinical Characteristics Associated with Isolation of Small-Colony Variants of Staphylococcus aureus and Pseudomonas aeruginosa from Respiratory Secretions of Patients with Cystic Fibrosis. J. Clin. Microbiol. 2008, 46, 1832–1834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Einarsson, G.G.; Comer, D.M.; McIlreavey, L.; Parkhill, J.; Ennis, M.; Tunney, M.M.; Elborn, J.S. Community dynamics and the lower airway microbiota in stable chronic obstructive pulmonary disease, smokers and healthy non-smokers. Thorax 2016, 71, 795–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tantucci, C.; Modina, D. Lung function decline in COPD. Int. J. Chron. Obs. Pulmon Dis. 2012, 7, 95–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| All Sample (N = 426) | CBI SA (N = 77) | Not Colonized (N = 349) | p | |
|---|---|---|---|---|
| Age | 66. 9 ± 16.2 (19–96) | 60.2 ± 18.6 | 68.4 + 15.2 | 0.000 |
| Age < 50 years | 60 (14.1%) | 19 (24.7%) | 41 (11.7%) | 0.003 |
| Sex (male/female) | 129 (30.3%)/297 (69.7%) | 28 (36.4%)/49 (63.6%) | 101 (29%)/248 (71%) | 0.199 |
| BMI (kg/m2) | 25.1 ± 4.7 (14–44.1) | 23.9 ± 4.96 | 25.3 + 4.56 | 0.024 |
| Charlson index | 1.74 ± 1.33 (0–12) | 1.96 ± 1.97 | 1.70 ± 1.14 | 0.258 |
| Exacerbations in previous year | 1.44 ± 1.71 (0–12) | 1.86 ± 1.99 | 1.35 ± 1.64 | 0.019 |
| >2 exacerbations | 159 (37.3%) | 49.4% | 34.5% | 0.016 |
| Hospitalizations in previous year | 0.42 ± 1.11 (0–10) | 0.26 ± 0.68 | 0.46 ± 1.18 | 0.051 |
| >1 hospitalization | 94 (22.1%) | 16.9% | 23.2% | 0.226 |
| Hemoptysis in previous year | 0.49 ± 1.74 (0–21) | 1 ± 2.9 | 0.37 ± 1.34 | 0.067 |
| FACED score | 1.63 ± 1.41 (0–6) | 1.64 ± 1.31 | 1.63 ± 1.44 | 0.973 |
| EFACED score | 2.62 ± 2.07 | 1.97 ± 1.73 | 2.1 ± 1.8 | 0.594 |
| BSI score | 7.3 ± 4.5 | 7.1 ± 3.5 | 7.8 ± 3.9 | 0.630 |
| Exacerbations (first year) | 0.85 ± 1.20 (0–5) | 1.30 ± 1.46 | 0.79 ± 1.01 | 0.020 |
| Exacerbations (second year) | 1.15 ± 1.28 (0–6) | 1.60 ± 1.47 | 0.79 ± 1.08 | 0.001 |
| Exacerbations (third year) | 1.11 ± 1.56 (0–8) | 1.80 ± 1.32 | 0.85 ± 0.88 | 0.018 |
| Hospitalization (first year) | 0.02 ± 0.14 (0–1) | 0.12 ± 0.33 | 0.06 ± 0.37 | 0.320 |
| Hospitalization (second year) | 0.02 ± 0.14 (0–1) | 0.07 ± 0.26 | 0.08 ± 0.42 | 0.902 |
| Hospitalization (third year) | 0.04 ± 0.19 (0–1) | 0.19 ± 0.47 | 0.10 ± 0.39 | 0.272 |
| Oxygen saturation | 96.3 ± 2.3 (83–99) | 96.5 ± 2.3 | 96.3 ± 2.3 | 0.529 |
| Number of lobes | 2.73 ± 1.45 (0–6) | 3 ± 1.5 | 2.67 ± 1.45 | 0.063 |
| FVC | 2.8 ± 0.91 (0.56–5.92) | 2.7 ± 1.5 | 2.74 ± 0.92 | 0.229 |
| FVC% | 87 ± 20.9 (26.7–161.2) | 83.1 ± 17.4 | 85.8 ± 21.5 | 0.150 |
| FEV1 | 2 ± 0.76 (0.41–4.98) | 2.1 ± 0.74 | 1.98 ± 0.76 | 0.548 |
| FEV1% | 78.8 ± 23.1 (14.5–157.6) | 73.3 ± 19.5 | 80 ± 23.7 | 0.021 |
| FEV1/FVC | 71.2 ± 12.8 (22.4–97.4) | 68.5 ± 13.2 | 71.7 ± 12.7 | 0.047 |
| Bronchial obstruction (FEV1/FVC < 70) | 172 (40.4%) | 50.6% | 38.1% | 0.042 |
| Aetiology | 0.000 | |||
| Post-infectious | 158 (37.1%) | 28 (36.4%) | 130 (37.3%) | |
| COPD | 41 (9.6%) | 5 (6.5%) | 36 (10.3%) | |
| Asthma | 39 (9.2%) | 9 (11.7%) | 30 (8.9%) | |
| Ciliary dyskinesia | 16 (3.8%) | 6 (7.8%) | 10 (2.9%) | |
| Immunodeficiency | 27 (6.3%) | 6 (7.8%) | 21 (6%) | |
| Systemic diseases | 32 (7.5%) | 1 (1.3%) | 31 (8.9%) | |
| Inflammatory bowel disease | 4 (0.9%) | 3 (3.9%) | 1 (0.3%) | |
| Others | 40 (9.4%) | 7 (9.1%) | 33 (9.5%) | |
| Unknown | 69 (16.2%) | 12 (15.6%) | 57 (16.3%) | |
| Treatment | 0.003 | |||
| Inhaled antibiotics | 44 (10.3%) | 9 (11.7%) | 35 (10%) | |
| Macrolides | 13 (3.1%) | 7 (9.1%) | 6 (1.7%) | |
| Inhaled corticoids. | 76 (17.8%) | 15 (19.5%) | 61 (17.5%) | |
| Bronchodilators | 136 (31.9%) | 14 (18.2%) | 122 (34.9%) | |
| Mucolytics | 60 (14.1%) | 17 (22.1%) | 43 (12.3%) |
| OR | CI 95% | p | |
|---|---|---|---|
| Age | 0.97 | 0.94–0.99 | <0.001 |
| Initial FEV1% | 0.98 | 0.97–0.99 | 0.035 |
| Number of lobes | 1.53 | 1.2–1.95 | <0.001 |
| ≥2 exacerbations in the previous year | 2.33 | 1.15–4.69 | 0.018 |
| CBI SA (N = 77) | Not Colonized (N = 349) | p | |
|---|---|---|---|
| FVC (baseline) | 2.97 ±0.91 | 2.75 ± 0.91 | 0.06 |
| FVC (first year) | 2.91 ± 1.1 | 2.72 ± 0.89 | 0.188 |
| FVC (second year) | 2.94 ± 0.92 | 2.69 ± 0.89 | 0.087 |
| FVC (third year) | 2.98 ± 0.95 | 2.75 ± 0.90 | 0.175 |
| FVC% (baseline) | 83.9 ± 17.6 | 87.8 ± 21.5 | 0.157 |
| FVC% (first year) | 80.8 ± 18.1 | 88.5 ± 21.1 | 0.015 |
| FVC% (second year) | 82.3 ± 17.5 | 88.8 ± 22.7 | 0.073 |
| FVC% (third year) | 80.6 ± 16.3 | 90.4 ± 20.4 | 0.012 |
| FEV1 (baseline) | 2.04 ± 0.74 | 1.98 ± 0.76 | 0.548 |
| FEV1 (first year) | 1.95 ± 0.71 | 1.93 ± 0.73 | 0.836 |
| FEV1 (second year) | 1.86 ± 0.67 | 1.91 ± 0.74 | 0.618 |
| FEV1 (third year) | 1.79 ± 0.69 | 1.96 ± 0.76 | 0.116 |
| FEV1% (baseline) | 73.3 ± 19.5 | 80 ± 23.7 | 0.021 |
| FEV1% (first year) | 70.8 ± 18.5 | 79.8 ± 23.6 | 0.002 |
| FEV1% (second year) | 69.4 ± 18.5 | 79.9 ± 24.9 | 0.001 |
| FEV1% (third year) | 67.5 ± 20.1 | 81.5 ± 23 | 0.000 |
| Variable | Coefficient β | 95% CI | p |
|---|---|---|---|
| Age | −2 | −3, −2 | <0.001 |
| Inhaled corticosteroids | −31 | −52, −10 | 0.004 |
| CBI caused by SA | −28 | −48, −8 | 0.007 |
| Gender | −42 | −59, −24 | <0.001 |
| FEV1 baseline | −90 | −93, −86 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García Clemente, M.; Olveira, C.; Girón, R.; Máiz, L.; Sibila, O.; Golpe, R.; Menéndez, R.; Rodríguez, J.; Barreiro, E.; Rodríguez Hermosa, J.L.; et al. Impact of Chronic Bronchial Infection by Staphylococcus aureus on Bronchiectasis. J. Clin. Med. 2022, 11, 3960. https://doi.org/10.3390/jcm11143960
García Clemente M, Olveira C, Girón R, Máiz L, Sibila O, Golpe R, Menéndez R, Rodríguez J, Barreiro E, Rodríguez Hermosa JL, et al. Impact of Chronic Bronchial Infection by Staphylococcus aureus on Bronchiectasis. Journal of Clinical Medicine. 2022; 11(14):3960. https://doi.org/10.3390/jcm11143960
Chicago/Turabian StyleGarcía Clemente, Marta, Casilda Olveira, Rosa Girón, Luis Máiz, Oriol Sibila, Rafael Golpe, Rosario Menéndez, Juan Rodríguez, Esther Barreiro, Juan Luis Rodríguez Hermosa, and et al. 2022. "Impact of Chronic Bronchial Infection by Staphylococcus aureus on Bronchiectasis" Journal of Clinical Medicine 11, no. 14: 3960. https://doi.org/10.3390/jcm11143960
APA StyleGarcía Clemente, M., Olveira, C., Girón, R., Máiz, L., Sibila, O., Golpe, R., Menéndez, R., Rodríguez, J., Barreiro, E., Rodríguez Hermosa, J. L., Prados, C., De la Rosa, D., Carbajal, C. M., Solís, M., & Martínez-García, M. Á. (2022). Impact of Chronic Bronchial Infection by Staphylococcus aureus on Bronchiectasis. Journal of Clinical Medicine, 11(14), 3960. https://doi.org/10.3390/jcm11143960