
Predictive Value of HAS-BLED Score Regarding Bleeding Events and Graft Survival following Renal Transplantation

 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Study Population
2.2. Study Groups/Antithrombotic Strategy
2.3. Definition of Bleeding Episodes
2.4. Outcome Measures and Analysis
2.5. Surgical Techniques/Intraoperative Antithrombotic Protocol
2.6. Immunosuppression
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Incidence of Bleeding
3.3. Intra- and Postoperative Outcome
3.4. Risk Factors for Bleeding
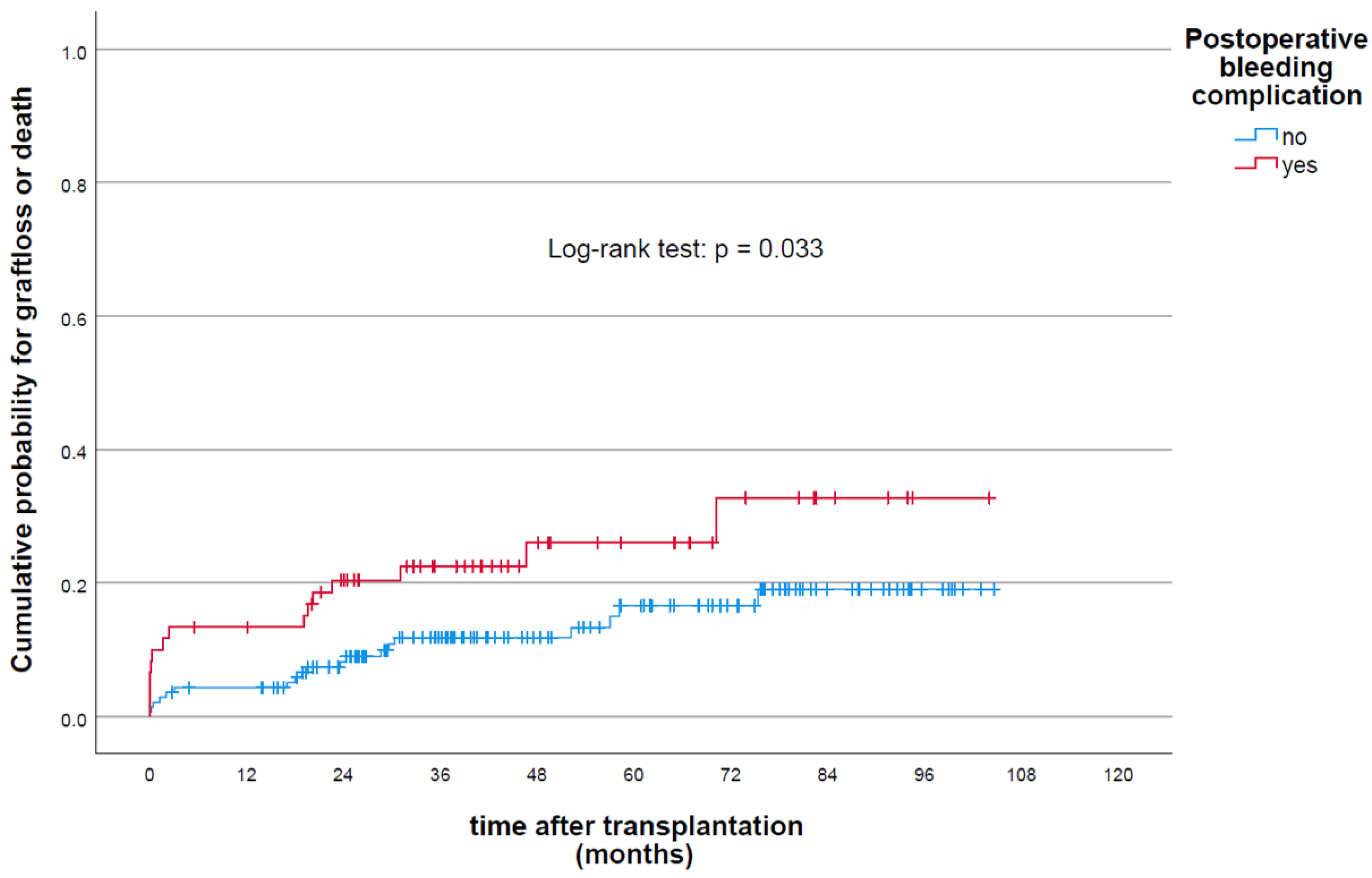
Graft Outcome and Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AF | atrial fibrillation |
| ANOVA | analysis of variance |
| APT | antiplatelet therapy |
| ARE | acute rejection episode |
| ASA | American Society of Anesthesiologists |
| ATG | Antithymoctye globulin |
| AUC | area under the curve |
| APT | antiplatelet therapy |
| BMI | body mass index |
| CDC | Clavien–Dindo classification |
| CI | confidence interval |
| CKD | chronic kidney disease |
| CMV | cytomegalovirus |
| CT | computed tomography |
| CVD | cerebrovascular disease |
| DGF | delayed graft function |
| DOAC | direct oral anticoagulants |
| EC | erythrocyte concentration |
| ERSD | end-stage renal disease |
| FFP | fresh frozen plasma |
| GFR | glomerular filtration rate |
| HLA | human leukocyte antigen |
| HLT | Hosmer–Lemshow test |
| HR | hazard Ratio |
| INR | international normalized ratio |
| KT | kidney transplantation |
| OR | odds ratio |
| PAD | peripheral arterial disease |
| PTT | partial thromboplastin time |
| ROC | receiver operating characteristics |
| TEC | thromboembolic complications |
| UFH | unfractionated heparin |
| VKA | vitamin K antagonists |
| VTE | venous thromboemolism |
References
- Vlachopanos, G.; Ghalli, F.G. Antithrombotic medications in dialysis patients: A double-edged sword. J. Evid. Based Med. 2017, 10, 53–60. [Google Scholar] [CrossRef]
- Casserly, L.F.; Dember, L.M. Thrombosis in end-stage renal disease. Semin. Dial. 2003, 16, 245–256. [Google Scholar] [CrossRef]
- Holden, R.M.; Harman, G.J.; Wang, M.; Holland, D.; Day, A.G. Major bleeding in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2008, 3, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Hachem, L.D.; Ghanekar, A.; Selzner, M.; Famure, O.; Li, Y.; Kim, S.J. Postoperative surgical-site hemorrhage after kidney transplantation: Incidence, risk factors, and outcomes. Transpl. Int. 2017, 30, 474–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berg, T.A.J.; Minnee, R.C.; Lisman, T.; Nieuwenhuijs-Moeke, G.J.; Wetering, J.; Bakker, S.J.L.; Pol, R.A. Perioperative antithrombotic therapy does not increase the incidence of early postoperative thromboembolic complications and bleeding in kidney transplantation—A retrospective study. Transpl. Int. 2019, 32, 418–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, J.C.Y.; Leung, M.; Landsberg, D. Evaluation of Heparin Anticoagulation Protocols in Post–Renal Transplant Recipients (EHAP-PoRT Study). Can. J. Hosp. Pharm. 2016, 69, 114. [Google Scholar] [CrossRef] [Green Version]
- Pawlicki, J.; Cierpka, L.; Król, R.; Ziaja, J. Risk Factors for Early Hemorrhagic and Thrombotic Complications After Kidney Transplantation. Transplant. Proc. 2011, 43, 3013–3017. [Google Scholar] [CrossRef]
- Mathis, A.S.; Davé, N.; Shah, N.K.; Friedman, G.S. Bleeding and Thrombosis in High-Risk Renal Transplantation Candidates Using Heparin. Ann. Pharmacother. 2004, 38, 537–543. [Google Scholar] [CrossRef]
- Parks, A.; Fang, M. Scoring Systems for Estimating the Risk of Anticoagulant-Associated Bleeding. Semin. Thromb. Hemost. 2017, 43, 514–524. [Google Scholar] [CrossRef]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; de Vos, C.B.; Crijns, H.J.G.M.; Lip, G.Y.H. A Novel User-Friendly Score (HAS-BLED) To Assess 1-Year Risk of Major Bleeding in Patients With Atrial Fibrillation. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef] [Green Version]
- Gage, B.F.; Yan, Y.; Milligan, P.E.; Waterman, A.D.; Culverhouse, R.; Rich, M.W.; Radford, M.J. Clinical classification schemes for predicting hemorrhage: Results from the National Registry of Atrial Fibrillation (NRAF). Am. Heart J. 2006, 151, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Beyth, R.J.; Quinn, L.M.; Landefeld, C.S. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. Am. J. Med. 1998, 105, 91–99. [Google Scholar] [CrossRef]
- Fang, M.C.; Go, A.S.; Chang, Y.; Borowsky, L.H.; Pomernacki, N.K.; Udaltsova, N.; Singer, D.E. A New Risk Scheme to Predict Warfarin-Associated Hemorrhage. J. Am. Coll. Cardiol. 2011, 58, 395–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruíz-Giménez, N.; Suárez, C.; González, R.; Nieto, J.; Todolí, J.; Samperiz, Á.; Monreal, M. Predictive variables for major bleeding events in patients presenting with documented acute venous thromboembolism. Findings from the RIETE Registry. Thromb. Haemost. 2008, 100, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Hippisley-Cox, J.; Coupland, C. Predicting risk of upper gastrointestinal bleed and intracranial bleed with anticoagulants: Cohort study to derive and validate the QBleed scores. BMJ 2014, 349, g4606. [Google Scholar] [CrossRef] [Green Version]
- Hijazi, Z.; Oldgren, J.; Lindbäck, J.; Alexander, J.H.; Connolly, S.J.; Eikelboom, J.W.; Ezekowitz, M.D.; Held, C.; Hylek, E.M.; Lopes, R.D.; et al. The novel biomarker-based ABC (age, biomarkers, clinical history)-bleeding risk score for patients with atrial fibrillation: A derivation and validation study. Lancet 2016, 387, 2302–2311. [Google Scholar] [CrossRef]
- Subherwal, S.; Bach, R.G.; Chen, A.Y.; Gage, B.F.; Rao, S.V.; Newby, L.K.; Wang, T.Y.; Gibler, W.B.; Ohman, E.M.; Roe, M.T.; et al. Baseline Risk of Major Bleeding in Non–ST-Segment–Elevation Myocardial Infarction. Circulation 2009, 119, 1873–1882. [Google Scholar] [CrossRef] [Green Version]
- Mehran, R.; Pocock, S.J.; Nikolsky, E.; Clayton, T.; Dangas, G.D.; Kirtane, A.J.; Parise, H.; Fahy, M.; Manoukian, S.V.; Feit, F.; et al. A Risk Score to Predict Bleeding in Patients With Acute Coronary Syndromes. J. Am. Coll. Cardiol. 2010, 55, 2556–2566. [Google Scholar] [CrossRef] [Green Version]
- Costa, F.; van Klaveren, D.; James, S.; Heg, D.; Räber, L.; Feres, F.; Pilgrim, T.; Hong, M.-K.; Kim, H.-S.; Colombo, A.; et al. Derivation and validation of the predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy (PRECISE-DAPT) score: A pooled analysis of individual-patient datasets from clinical trials. Lancet 2017, 389, 1025–1034. [Google Scholar] [CrossRef]
- Castini, D.; Persampieri, S.; Sabatelli, L.; Erba, M.; Ferrante, G.; Valli, F.; Centola, M.; Carugo, S. Utility of the HAS-BLED score for risk stratification of patients with acute coronary syndrome. Heart Vessels 2019, 34, 1621–1630. [Google Scholar] [CrossRef]
- Siedlecki, A.; Irish, W.; Brennan, D.C. Delayed graft function in the kidney transplant. Am. J. Transplant. 2011, 11, 2279–2296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Sollinger, H.W.; Odorico, J.S.; Knechtle, S.J.; D’Alessandro, A.M.; Kalayoglu, M.; Pirsch, J.D. Experience with 500 simultaneous pancreas-kidney transplants. Ann. Surg. 1998, 228, 284–296. [Google Scholar] [CrossRef] [PubMed]
- Sollinger, H.W.; Odorico, J.S.; Becker, Y.T.; D’Alessandro, A.M.; Pirsch, J.D. One thousand simultaneous pancreas-kidney transplants at a single center with 22-year follow-up. Ann. Surg. 2009, 250, 618–630. [Google Scholar] [CrossRef]
- Eurotranplant Chapter 9: The Donor. 2020. Available online: https://www.eurotransplant.org/wp-content/uploads/2020/01/H9-The-Donor-Februar-2020.pdf (accessed on 11 July 2021).
- Ladurner, R.; Steurer, W. Technik der Multiorganentnahme. Viszeralchirurgie 2004, 39, 439–442. [Google Scholar] [CrossRef]
- Hau, H.-M.; Jahn, N.; Brunotte, M.; Lederer, A.A.; Sucher, E.; Rasche, F.M.; Seehofer, D.; Sucher, R. Short and long-term metabolic outcomes in patients with type 1 and type 2 diabetes receiving a simultaneous pancreas kidney allograft. BMC Endocr. Disord. 2020, 20, 30. [Google Scholar] [CrossRef] [Green Version]
- Sucher, R.; Rademacher, S.; Jahn, N.; Brunotte, M.; Wagner, T.; Alvanos, A.; Sucher, E.; Seehofer, D.; Scheuermann, U.; Hau, H.-M. Effects of simultaneous pancreas-kidney transplantation and kidney transplantation alone on the outcome of peripheral vascular diseases. BMC Nephrol. 2019, 20, 453. [Google Scholar] [CrossRef]
- Scheuermann, U.; Rademacher, S.; Wagner, T.; Lederer, A.; Hau, H.-M.; Seehofer, D.; Sucher, R. Influence of Multiple Donor Renal Arteries on the Outcome and Graft Survival in Deceased Donor Kidney Transplantation. J. Clin. Med. 2021, 10, 4395. [Google Scholar] [CrossRef]
- Burlacu, A.; Genovesi, S.; Ortiz, A.; Combe, C.; Basile, C.; Schneditz, D.; van der Sande, F.; Popa, G.T.; Morosanu, C.; Covic, A. Pros and cons of antithrombotic therapy in end-stage kidney disease: A 2019 update. Nephrol. Dial. Transplant. 2019, 34, 923–933. [Google Scholar] [CrossRef]
- Burlacu, A.; Genovesi, S.; Goldsmith, D.; Rossignol, P.; Ortiz, A.; Kalra, P.A.; Małyszko, J.; Banach, M.; Kanbay, M.; Covic, A. Bleeding in advanced CKD patients on antithrombotic medication—A critical appraisal. Pharmacol. Res. 2018, 129, 535–543. [Google Scholar] [CrossRef]
- Mathews, R.; Peterson, E.D.; Chen, A.Y.; Wang, T.Y.; Chin, C.T.; Fonarow, G.C.; Cannon, C.P.; Rumsfeld, J.S.; Roe, M.T.; Alexander, K.P. In-Hospital Major Bleeding During ST-Elevation and Non–ST-Elevation Myocardial Infarction Care: Derivation and Validation of a Model from the ACTION Registry®-GWTGTM. Am. J. Cardiol. 2011, 107, 1136–1143. [Google Scholar] [CrossRef] [PubMed]
- Hernández, D.; Rufino, M.; Armas, S.; González, A.; Gutiérrez, P.; Barbero, P.; Vivancos, S.; Rodríguez, C.; de Vera, J.R.; Torres, A. Retrospective analysis of surgical complications following cadaveric kidney transplantation in the modern transplant era. Nephrol. Dial. Transplant. 2006, 21, 2908–2915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kusyk, T.; Verran, D.; Stewart, G.; Ryan, B.; Fisher, J.; Tsacalos, K.; Chadban, S.; Eris, J. Increased Risk of Hemorrhagic Complications in Renal Allograft Recipients Receiving Systemic Heparin Early Posttransplantation. Transplant. Proc. 2005, 37, 1026–1028. [Google Scholar] [CrossRef] [PubMed]
- Dimitroulis, D.; Bokos, J.; Zavos, G.; Nikiteas, N.; Karidis, N.P.; Katsaronis, P.; Kostakis, A. Vascular Complications in Renal Transplantation: A Single-Center Experience in 1367 Renal Transplantations and Review of the Literature. Transplant. Proc. 2009, 41, 1609–1614. [Google Scholar] [CrossRef] [PubMed]
- Fischereder, M.; Göhring, P.; Schneeberger, H.; Lohse, P.; Von Appen, K.; Samtleben, W.; Schlöndorff, D.; Land, W. Early loss of renal transplants in patients with thrombophilia. Transplantation 1998, 65, 936–939. [Google Scholar] [CrossRef]
- Friedman, G.S.; Meier-Kriesche, H.-U.; Kaplan, B.; Scott Mathis, A.; Bonomini, L.; Shah, N.; DeFranco, P.; Jacobs, M.; Mulgaonkar, S.; Geffner, S.; et al. Hypercoagulable states in renal transplant candidates: Impact of anticoagulation upon incidence of renal allograft thrombosis. Transplantation 2001, 72, 1073–1078. [Google Scholar] [CrossRef]
- Lock, J.F.; Ungeheuer, L.; Borst, P.; Swol, J.; Löb, S.; Brede, E.M.; Röder, D.; Lengenfelder, B.; Sauer, K.; Germer, C.-T. Markedly increased risk of postoperative bleeding complications during perioperative bridging anticoagulation in general and visceral surgery. Perioper. Med. 2020, 9, 39. [Google Scholar] [CrossRef]
- Musetti, C.; Quaglia, M.; Cena, T.; Battista, M.; Fenoglio, R.; Lazzarich, E.; Stratta, P. Impact of pre-transplant antiaggregant and anticoagulant therapies on early hemorrhagic and cardiovascular events after kidney transplantation. J. Nephrol. 2015, 28, 757–764. [Google Scholar] [CrossRef]
- Eng, M.; Brock, G.; Li, X.; Chen, Y.; Ravindra, K.V.; Buell, J.F.; Marvin, M.R. Perioperative anticoagulation and antiplatelet therapy in renal transplant: Is there an increase in bleeding complication? Clin. Transplant. 2011, 25, 292–296. [Google Scholar] [CrossRef]
- Alonso-Escalante, J.C.; Machado, L.; Tabar, K.R.; Tindall, R.; Thai, N.; Uemura, T. Is Continuing Anticoagulation or Antiplatelet Therapy Safe Prior to Kidney Transplantation? Ann. Transplant. 2021, 26, e931648-1. [Google Scholar] [CrossRef]
- Merkow, R.P.; Bilimoria, K.Y.; McCarter, M.D.; Bentrem, D.J. Effect of Body Mass Index on Short-Term Outcomes after Colectomy for Cancer. J. Am. Coll. Surg. 2009, 208, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Hussan, H.; Gray, D.M.; Hinton, A.; Krishna, S.G.; Conwell, D.L.; Stanich, P.P. Morbid Obesity is Associated with Increased Mortality, Surgical Complications, and Incremental Health Care Utilization in the Peri-Operative Period of Colorectal Cancer Surgery. World J. Surg. 2016, 40, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Ghanta, R.K.; LaPar, D.J.; Zhang, Q.; Devarkonda, V.; Isbell, J.M.; Yarboro, L.T.; Kern, J.A.; Kron, I.L.; Speir, A.M.; Fonner, C.E.; et al. Obesity Increases Risk-Adjusted Morbidity, Mortality, and Cost Following Cardiac Surgery. J. Am. Heart Assoc. 2017, 6, e003831. [Google Scholar] [CrossRef] [Green Version]
- Kornblith, L.Z.; Howard, B.; Kunitake, R.; Redick, B.; Nelson, M.; Cohen, M.J.; Callcut, R. Obesity and clotting. J. Trauma Acute Care Surg. 2015, 78, 30–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilic, A.; George, T.J.; Beaty, C.A.; Merlo, C.A.; Conte, J.V.; Shah, A.S. The effect of center volume on the incidence of postoperative complications and their impact on survival after lung transplantation. J. Thorac. Cardiovasc. Surg. 2012, 144, 1502–1509. [Google Scholar] [CrossRef] [Green Version]
- Ozhathil, D.K.; Li, Y.F.; Smith, J.K.; Tseng, J.F.; Saidi, R.F.; Bozorgzadeh, A.; Shah, S.A. Impact of center volume on outcomes of increased-risk liver transplants. Liver Transplant. 2011, 17, 1191–1199. [Google Scholar] [CrossRef]
- Tsampalieros, A.; Knoll, G.A.; Fergusson, N.; Bennett, A.; Taljaard, M.; Fergusson, D. Center Variation and the Effect of Center and Provider Characteristics on Clinical Outcomes in Kidney Transplantation: A Systematic Review of the Evidence. Can. J. Kidney Health Dis. 2017, 4, 205435811773552. [Google Scholar] [CrossRef] [Green Version]
- Sonnenberg, E.M.; Cohen, J.B.; Hsu, J.Y.; Potluri, V.S.; Levine, M.H.; Abt, P.L.; Reese, P.P. Association of Kidney Transplant Center Volume With 3-Year Clinical Outcomes. Am. J. Kidney Dis. 2019, 74, 441–451. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Post-Surgical Anticoagulant Strategy | p-Value | |
|---|---|---|---|
| Prophylactic Anticoagulation (n = 108 Patients) | (Sub)therapeutic and/or Antiplatelet Therapy (n = 96 Patients) | ||
| Recipient characteristics | |||
| Gender (%) | |||
| male/female | 67 (62)/41 (38) | 61 (64)/35 (36) | 0.824 |
| Age (years) | 51.29 ± 13.13 | 55.88 ± 13.71 | <0.05 * |
| BMI (kg/m²) | 25.75 ± 4.18 | 25.68 ± 4.58 | 0.907 |
| ASA score | 2.99 ± 0.96 | 3.00 ± 0.145 | 0.501 |
| Prior transplant loss (%) | 8 (7) | 8 (8) | 0.806 |
| Pre-emptive KT (%) | 11 (10) | 3 (3) | <0.05 * |
| Type of dialysis (%) | |||
| Hemodialysis/CAPD | 91 (94)/6 (6) | 91 (98)/2 (2) | 0.166 |
| Time on dialysis (years) | 5.53 ± 3.29 | 5.72 ± 4.13 | 0.721 |
| Arterial hypertension (%) | 93 (86.1) | 88 (92) | 0.210 |
| Diabetes mellitus (%) | 11 (10) | 16 (17) | 0.173 |
| Cardiovascular disease (%) | 22 (20) | 59 (62) | <0.01 ** |
| Pulmonary disease (%) | 5 (5) | 10 (10) | 0.114 |
| HAS-BLED score | 2.27 ± 0.69 | 3.29 ± 1.08 | <0.01 ** |
| Donor characteristics | |||
| Gender (%) | |||
| male/female | 50 (46)/58 (54) | 52 (54)/44 (46) | 0.216 |
| Donor age (years) | 49.8 ± 19.3 | 54.5 ± 16.0 | 0.069 |
| Donor BMI (kg/m2) | 29.9 ± 8.2 | 26.3 ± 5.8 | 0.245 |
| Donor type (%) | |||
| living/deceased | 28 (26)/80 (74) | 23 (24)/73 (76) | 0.746 |
| Cause of end-stage renal disease | |||
| Diabetic nephropathy (%) | 2 (2) | 9 (9) | 0.405 |
| Hypertensive kidney disease (%) | 16 (15) | 11 (12) | |
| Primary/secondary glomerulonephritis (%) | 47 (44) | 40 (42) | |
| Polycystic kidney disease (%) | 19 (18) | 16 (17) | |
| Tubulointerstitial nephritis (%) | 6 (6) | 8 (8) | |
| Cirrhosis of kidney (%) | 9 (8) | 5 (5) | |
| Reflux nephropathy (%) | 2 (2) | 3 (3) | |
| Alport syndrome (%) | 3 (3) | 1 (1) | |
| Unknown (%) | 4 (4) | 3 (3) | |
| Preoperative factors | |||
| Creatinine (mmol/L) | 0.64 ± 0.21 | 0.66 ± 0.23 | 0.520 |
| Urea (mmol/L) | 15.58 ± 7.21 | 15.84 ± 6.57 | 0.798 |
| Hemoglobin (mmol/dL) | 6.89 ± 0.88 | 6.83 ± 0.92 | 0.651 |
| Platelets (GPT/L) | 206 ± 70 | 201 ± 66 | 0.561 |
| Quick (%) | 102.39 ±12.80 | 96.53 ± 17.98 | <0.01 ** |
| INR | 0.97 ± 0.1 | 1.02 ± 0.24 | 0.054 |
| Immunosuppression | |||
| ABO incompatibility (%) | 11 (11) | 8 (9) | 0.638 |
| Prior induction therapy in case of HLA-mismatch (%) | 71 (66) | 74 (77) | 0.075 |
| Basiliximab (%) | 65 (60) | 68 (71) | 0.111 |
| ATG (%) | 7 (7) | 9 (9) | 0.443 |
| Rituximab (%) | 6 (6) | 5 (5) | 0.913 |
| HLA mismatch (%) | 71 (66) | 74 (77) | 0.075 |
| Variables | Postoperative Bleeding Complication | p-Value | |
|---|---|---|---|
| No (n = 143 Patients) | Yes (n = 61 Patients) | ||
| Recipient characteristics | |||
| Gender (%) | |||
| male/female | 93 (65)/50 (35) | 35 (57)/26 (43) | 0.300 |
| Age (years) | 53.12 ± 13.90 | 54.21 ± 13.09 | 0.600 |
| BMI (kg/m²) | 25.66 ± 4.45 | 25.84 ± 4.18 | 0.788 |
| ASA score | 2.99 ± 0.15 | 3.00 ± 0 | 0.708 |
| Prior transplant loss (%) | 11 (8) | 5 (8) | 0.902 |
| Pre-emptive KT (%) | 12 (8) | 2 (3) | 0.182 |
| Type of dialysis (%) | |||
| Hemodialysis/CAPD | 126 (88)/5 (4) | 56 (91.8)/3 (5) | 0.687 |
| Time on dialysis (years) | 5.47 ± 3.60 | 5.96 ± 3.98 | 0.399 |
| Dialysis prior to transplant/no dialysis prior to transplant | 22 (15)/121 (85) | 8 (13)/53 (87) | 0.674 |
| HAS-BLED score | 2.50 ± 0.92 | 3.44 ± 1.19 | <0.01 ** |
| Arterial hypertension (%) | 125 (87) | 56 (92) | 0.364 |
| Diabetes mellitus (%) | 19 (13) | 8 (13) | 0.971 |
| Cardiovascular disease (%) | 47 (33) | 34 (56) | <0.01 ** |
| Pulmonary disease (%) | 12 (8) | 3 (5) | 0.384 |
| Donor characteristics | |||
| Donor gender (%) | |||
| male/female | 67 (47)/76 (53) | 35 (87)/26 (13) | 0.162 |
| Donor BMI (kg/m²) | 25.3 ± 4.2 | 29.8 ± 7.2 | 0.533 |
| Donor age (years) | 54.6 ± 17.5 | 59.9 ± 18.2 | 0.193 |
| Donor type (%) | |||
| living/deceased | 42 (29)/101 (71) | 9 (15)/52 (85) | <0.05 * |
| Cause of end-stage renal disease | |||
| Diabetic nephropathy (%) | 7 (5) | 4 (7) | 0.498 |
| Hypertensive kidney disease (%) | 17 (12) | 10 (16) | |
| Primary/secondary glomerulonephritis (%) | 67 (47) | 20 (33) | |
| Polycystic kidney disease (%) | 23 (16) | 12 (20) | |
| Tubulointerstitial nephritis (%) | 7 (5) | 7 (12) | |
| Cirrhosis of kidney (%) | 11 (8) | 3 (5) | |
| Reflux nephropathy (%) | 4 (3) | 1 (2) | |
| Alport syndrome (%) | 2 (1) | 2 (3) | |
| Unknown (%) | 5 (4) | 2 (3) | |
| Preoperative factors | |||
| Prior anticoagulation (%) | |||
| Prior antiplatelet drug | 47 (33) | 26 (43) | 0.183 |
| Prior plasmatic anticoagulant/VKA therapy | 8 (6) | 10 (16) | <0.05 * |
| Postoperative therapeutical heparin (%) | 20 (14) | 23 (37) | <0.01 ** |
| Intraoperative heparin (%) | 9 (6) | 8 (13) | 0.102 |
| Creatinine (mmol/L) | 0.64 ± 0.22 | 0.67 ± 0.24 | 0.457 |
| Urea (mmol/L) | 15.79 ± 7.15 | 15.49 ± 6.36 | 0.784 |
| GFR (ml/min) | 8.23 ± 3.34 | 7.79 ± 3.41 | 0.392 |
| Hemoglobin (mmol/L) | 7.51 ± 0.90 | 7.48 ± 0.91 | 0.812 |
| Platelets (GPT/L) | 230 ± 71 | 203 ± 58 | <0.05 * |
| INR | 0.98 ± 0.12 | 1.02 ± 0.24 | 0.125 |
| Quick (%) | 108 ± 16 | 105 ± 20 | 0.159 |
| PTT (s) | 31.6 ± 20.4 | 30.8 ± 5.3 | 0.776 |
| Immunological factors | |||
| ABO incompatibility (%) | 13 (9) | 6 (10) | 0.927 |
| Prior induction therapy in case of HLA-mismatch (%) | 100 (70) | 45 (74) | 0.156 |
| Basiliximab (%) | 92 (64) | 41 (67) | 0.693 |
| ATG (%) | 9 (6) | 7 (12) | 0.208 |
| Rituximab (%) | 6 (4) | 5 (8) | 0.247 |
| Postsurgical Anticoagulant Strategy | p-Value | ||
|---|---|---|---|
| Variables | Prophylactic Anticoagulation (n = 108) | (Sub)therapeutic and/or Antiplatelet Therapy (n = 96) | |
| Number of arteries | |||
| mean ± SD | 1.09 ± 0.32 | 1.17 ± 0.45 | 0.183 |
| 1/>1 (%) | 98 (92)/9 (8) | 82 (86)/13 (14) | 0.230 |
| Number of veins | |||
| mean ± SD | 1.06 ± 0.23 | 1.05 ± 0.22 | 0.918 |
| 1/>1 (%) | 101 (94)/6 (6) | 90 (95)/5 (5) | 0.914 |
| Cold ischemia time (min) | 532 ± 329 | 523 ± 299 | 0.859 |
| Warm ischemia time (min) | 46 ± 23 | 43 ± 17 | 0.519 |
| Surgery time (min) | 187 ± 41 | 200 ± 64 | 0.098 |
| Blood loss (mL) | 133 ± 212 | 192 ± 387 | 0.193 |
| Kidney right/left | 58 (54)/50 (46) | 46 (47)/50 (53) | 0.591 |
| Total transfusion during surgery (mL) | 2943.18 ± 1205.41 | 3385 ± 1554.64 | <0.05 * |
| Crystalloids (mL) | 2892.15 ± 1167.77 | 3162.19 ± 1288.93 | 0.119 |
| Crystalloids (mL/kg) | 38.89 ± 16.48 | 43.31 ± 19.38 | 0.820 |
| Crystalloids (mL/kg/h) | 12.93 ± 5.60 | 13.62 ± 6.97 | 0.446 |
| Red blood cells (mL) | 42.06 ± 167.13 | 159.38 ± 541.84 | <0.05 * |
| FFP (mL) | 46.17 ± 63.80 | 57.29 ± 325.91 | 0.134 |
| PLT (mL) | 2.80 ± 29.00 | 9.38 ± 52.47 | 0.264 |
| Postreperfusion urine output, 1 h (mL) | 162 ± 92 | 68 ± 101 | <0.05 * |
| Diuresis day 1 (mL) | 1961 ± 1290 | 1240 ± 1100 | <0.01 ** |
| Delayed graft function (%) | 17 (16) | 37 (39) | <0.01 ** |
| Rejection of transplant organ (%) | 29 (28) | 36 (38) | 0.098 |
| During hospitalization/≤12/>12 months | 14 (13)/7 (7)/8 (7) | 17 (18)/11 (12)/8 (8) | 0.806 |
| Thromboembolic complications (%) | 3 (3) | 8 (8) | 0.08 |
| Bleeding complication (%) | 21 (10) | 40 (20) | <0.01 ** |
| Complications according to Clavien–Dindo classification | |||
| minor/major (%) | 70 (65)/38 (35) | 38 (40)/58 (60) | <0.05 * |
| Platelets day 1 (GPT/L), mean ± SD | 195 ± 63 | 189 ± 68 | 0.531 |
| Quick day 1 (%), mean ± SD | 101 ± 15 | 94 ± 17 | <0.01 ** |
| PTT day 1 (s), mean ± SD | 27 ± 5.3 | 38 ± 21 | <0.01 ** |
| Platelets day 3 (GPT/L), mean ± SD | 187 ± 69 | 182 ± 66 | 0.571 |
| Quick day 3 (%), mean ± SD | 112 ± 15 | 101 ± 15 | 0.09 |
| PTT day 3 (s), mean ± SD | 26 ± 8 | 37 ±19 | <0.01 ** |
| Platelets day 5 (GPT/L), mean ± SD | 210 ± 88 | 193 ±71 | 0.216 |
| Quick day 5 (%), mean ± SD | 113 ± 15 | 105 ± 16 | <0.01 ** |
| PTT day 5 (s), mean ± SD | 26 ± 3.5 | 36 ± 19 | <0.01 ** |
| Variables | Postoperative Bleeding Complication | p-Value | |
|---|---|---|---|
| No (n = 143) | Yes (n = 61) | ||
| Number of arteries | |||
| mean ± SD | 1.15 ± 0.41 | 1.08 ± 0.33 | 0.245 |
| 1/>1 (%) | 124 (87)/18 (13) | 56 (92)/4 (7) | 0.210 |
| Number of veins | |||
| mean ± SD | 1.05 ± 0.22 | 1.07 ± 0.25 | 0.621 |
| 1/>1 (%) | 135 (94)/7 (5) | 56 (92)/4 (7) | 0.619 |
| Cold ischemia time (min), mean ± SD | 544 ± 325 | 492 ± 290 | 0.311 |
| Warm ischemia time (min), mean ± SD | 43 ± 21 | 49 ± 20 | 0.157 |
| Surgery time (min), mean ± SD | 186 ± 41 | 210 ± 72 | <0.05 * |
| Blood loss (mL), mean ± SD | 113 ± 164 | 274 ± 488 | <0.05 * |
| Kidney right/left (%) | 71 (50)/72 (50) | 33 (54)/28 (66) | 0.564 |
| Total transfusion during surgery (mL), mean ± SD | 2936.06 ± 1085.08 | 3651.64 ± 1848.37 | <0.01 ** |
| Crystalloids (mL), mean ± SD | 2933.94 ± 1082.40 | 3219.84 ± 1513.19 | 0.130 |
| Crystalloids (mL/kg), mean ± SD | 39.76 ± 15.34 | 43.76 ± 22.90 | 0.148 |
| Crystalloids (mL/kg/h), mean ± SD | 13.23 ± 5.86 | 13.33 ± 7.62 | 0.915 |
| Red blood cells (mL), mean ± SD | 2.11 ± 25.18 | 319.67 ± 672.76 | <0.01 ** |
| FFP (mL), mean ± SD | 0.00 ± 0.00 | 100.98 ± 412.71 | 0.061 |
| PLT (mL), mean ± SD | 0.00 ± 0.00 | 19.67 ± 74.88 | <0.05 * |
| Postreperfusion urine output, 1 h (mL) | 101.17 ± 165.60 | 58.61 ± 126.18 | <0.05 * |
| Diuresis day 1 (mL) | 1791.05 ± 1730.84 | 1214.20 ± 1213.93 | <0.05 * |
| Delayed graft function (%) | 31 (22) | 23 (38) | <0.05 * |
| Rejection of transplant organ (%) | 37 (26) | 28 (46) | 0.426 |
| During hospitalization/≤12/>12 months | 17 (12)/11 (8)/9 (6) | 14 (23)/7 (12)/7 (12) | 0.911 |
| Thromboembolic complications (%) | 4 (3) | 7 (11) | <0.05 * |
| Complications according to Clavien–Dindo classification | |||
| minor/major (%) | 93 (6)/50 (35) | 15 (24)/46 (76) | <0.01 ** |
| Platelets day 1 (GPT/L), mean ± SD | 198 ± 63 | 178 ± 57 | <0.05 * |
| Quick day 1 (%), mean ± SD | 98 ± 16 | 96 ± 17 | 0.437 |
| PTT day 1 (s), mean ± SD | 29 ± 9 | 37 ± 22 | <0.01 ** |
| Platelets day 3 (GPT/L), mean ± SD | 192 ± 66 | 167 ± 68 | <0.05 * |
| Quick day 3 (%), mean ± SD | 110 ±13 | 109 ± 19 | 0.826 |
| PTT day 3 (s), mean ± SD | 28 ± 13 | 36 ± 19 | <0.05 * |
| Platelets day 5 (GPT/L), mean ± SD | 213 ± 80 | 176 ± 71 | <0.01 ** |
| Quick day 5 (%), mean ± SD | 109 ± 14 | 108 ± 17 | 0.908 |
| PTT day 5 (s), mean ± SD | 30 ± 15 | 35 ± 18 | 0.233 |
| Variables | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Recipient characteristics | ||
| Recipient BMI (per 5 kg/m2 increase) | 0.32 (0.12–0.91) | <0.05 * |
| Time on dialysis pretransplant (per 1-year increase) | 1.08 (0.92–1.18) | 0.165 |
| Recipient peripheral arterial disease (yes versus no) | 1.36 (0.42–3.25) | 0.235 |
| Recipient cardiovascular disease (yes versus no) | 2.89 (1.02–8.21) | <0.05 * |
| HAS-BLED score | 1.49 (1.08–2.07) | <0.05 * |
| HAS-BLED score > 2 | 5.41 (1.21–24.16) | <0.05 * |
| Donor characteristics | ||
| Donor age, >55 years | 1.02 (0.99–1.05) | 0.11 |
| Donor BMI (per 5 kg/m2 increase) | 1.049 (0.92–1.19) | 0.471 |
| Donor type (living versus deceased) | 0.43 (0.18–0.94) | <0.05 * |
| Transplant characteristics | ||
| Blood loss, mL | 1.03 (1.0–1.05) | <0.05 * |
| Delayed graft function (yes versus no) | 1.92 (0.98–3.77) | 0.056 |
| Clavien–Dindo classification > grade II | 3.34 (1.17–9.49) | <0.05 * |
| Cold ischemia time, hours | 0.99 (0.99–1.00) | 0.09 |
| Anastomosis time, min | 1.01 (0.98–1.05) | 0.256 |
| Duration of surgery, hours | 0.99 (0.98–1.06) | 0.474 |
| Pharmacological and laboratory characteristics | ||
| Preoperative VKA therapy | 5.89 (1.10–31.28) | <0.05 * |
| Preoperative antiplatelets (yes versus no) | 1.63 (0.85–3.15) | 0.144 |
| Intraoperative heparin | 1.35 (0.44–4.11) | 0.597 |
| Postoperative heparin | 2.5 (1.1–5.69) | <0.05 * |
| Postoperative antithrombotic regime ((sub)therapeutic versus prophylactic) | 2.14 (1.08–4.24) | <0.05 * |
| Prophylaxis | 1.0 | |
| Antiplatelet + prophylactic heparin | 0.998 (0.39–2.52) | 0.996 |
| Therapeutic heparin | 3.37 (1.37–8.23) | <0.01 ** |
| Antiplatelet + therapeutic heparin | 5.44 (1.31–22.31) | <0.05 * |
| Start antithrombotic therapy <6 h versus >6 h | 1.58 (0.85–2.98) | 0.151 |
| Starts platelets within 24 h versus after KT | 1.57 (0.71–3.49) | 0.268 |
| Variables | Univariate | Multivariate | ||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Recipient characteristics | ||||
| Recipient age, years | 1.06 (1.01–1.10) | <0.01 ** | NS | NS |
| Recipient gender (male versus female) | 2.08 (0.94–4.6) | 0.06 | ||
| Recipient BMI > 30 kg/m2 versus <18.5–24.9 kg/m2 | 1.96 (1.18–3.07) | <0.05 * | NS | NS |
| Type of transplantation (pre-emptive versus not) | 2.8 (1.3–5.2) | <0.05 * | NS | NS |
| Recipient history of diabetes (yes versus no) | 1.99 (1.02–3.12) | <0.05 * | 1.71 (1.07–2.73) | <0.05 * |
| Recipient cardiovascular disease (yes versus no) | 1.99 (1.01–3.91) | <0.05 * | NS | NS |
| HAS-BLED score, >3 versus <3 | 4.01 (1.87–8.90) | <0.01 ** | 3.2 (1.46–7.1) | <0.01 ** |
| Donor characteristics | ||||
| Donor age, <55 versus >55 years | 2.8 (1.3–5.9) | <0.01 ** | 3.2 (1.5–6.81) | <0.01 * |
| Donor type (living versus deceased) | 11.6 (1.55–83.1) | <0.01 ** | NS | NS |
| Transplant characteristics | ||||
| Cold ischemia time, hours | 1.01 (1.00–1.02) | <0.05 * | NS | NS |
| Duration of surgery, hours | 1.007 (1.003–1.011) | <0.01 ** | 1.006 (1.002–1.01) | <0.01 ** |
| Acute rejection | 3.2 (1.6–5.4) | <0.01 ** | 2.71 (1.83–4.1) | <0.01 ** |
| Delayed graft function (yes versus no) | 2.47 (1.25–4.87) | <0.01 ** | NS | NS |
| Clavien–Dindo score, <2 versus >2 | 4.2 (1.7–10.3) | <0.01 ** | 4.2 (1.7–9.4) | <0.01 ** |
| Pharmacological factors (preoperative, during hospital stay and follow-up) | ||||
| Preoperative anticoagulation (yes versus no, not stopped or INR not corrected) | 3.35 (1.01–10.93) | <0.05 * | 5.21 (1.4–18.9) | <0.05 |
| Preoperative antidiabetics (yes versus no) | 3.12 (1.05–9.21) | <0.05 * | NS | NS |
| Antithrombotic therapy postoperative ((sub) therapeutic versus prophylactic) | 3.32 (1.6–6.9) | <0.01 ** | 2.9 (1.41–6.23) | <0.01 ** |
| Transfusion blood products postop (yes versus not) | 2.57 (1.11–5.46) | <0.05 * | NS | NS |
| Postoperative catecholamine therapy (yes versus not) | 5.51 (2.67–11.3) | <0.01 ** | 3.79 (1.4–6.8) | <0.01 ** |
| Antibiotics postoperative (yes versus not) | 3.3 (1.64–6.67) | <0.01 ** | NS | NS |
| Platelet inhibitor postoperative | 2.91 (1.4–5.72) | <0.01 ** | NS | NS |
| CMV infection/CMV therapy (yes versus no) | 1.59 (1.13–2.2) | <0.05 * | NS | NS |
| Tranexamic acid | 1.01 (1.001–1.003) | <0.01 ** | NS | NS |
| Change in immunosuppression (yes versus no) | 4.32 (1.23–15.18) | <0.05 * | NS | NS |
| Treatment for poliomavirus (change IS, immunoglobulin) | 3.49 (1.62–7.2) | <0.01 ** | NS | NS |
| Fungal therapy | 4.2 (1.6–10.9) | <0.05 * | NS | NS |
| Postoperative antithrombotic regime | <0.01 ** | <0.05 * | ||
| Prophylaxis | 1.0 | 1.0 | ||
| Platelet + prophylactic heparin | 2.91 (1.03–8.18) | <0.05 * | 2.8 (1.1–7.4) | 0.123 |
| Platelet + therapeutical Heparin | 4.23 (1.82–9.81) | <0.01 ** | 3.3 (1.52–6.58) | <0.05 * |
| Postoperative heparin (therapeutically) | 6.76 (2.26–20.56) | <0.01 ** | 2.25 (0.82–6.13) | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hau, H.M.; Eckert, M.; Laudi, S.; Völker, M.T.; Stehr, S.; Rademacher, S.; Seehofer, D.; Sucher, R.; Piegeler, T.; Jahn, N. Predictive Value of HAS-BLED Score Regarding Bleeding Events and Graft Survival following Renal Transplantation. J. Clin. Med. 2022, 11, 4025. https://doi.org/10.3390/jcm11144025
Hau HM, Eckert M, Laudi S, Völker MT, Stehr S, Rademacher S, Seehofer D, Sucher R, Piegeler T, Jahn N. Predictive Value of HAS-BLED Score Regarding Bleeding Events and Graft Survival following Renal Transplantation. Journal of Clinical Medicine. 2022; 11(14):4025. https://doi.org/10.3390/jcm11144025
Chicago/Turabian StyleHau, Hans Michael, Markus Eckert, Sven Laudi, Maria Theresa Völker, Sebastian Stehr, Sebastian Rademacher, Daniel Seehofer, Robert Sucher, Tobias Piegeler, and Nora Jahn. 2022. "Predictive Value of HAS-BLED Score Regarding Bleeding Events and Graft Survival following Renal Transplantation" Journal of Clinical Medicine 11, no. 14: 4025. https://doi.org/10.3390/jcm11144025