
Decreased Left Atrial Reservoir Strain Is Associated with Adverse Outcomes in Restrictive Cardiomyopathy

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
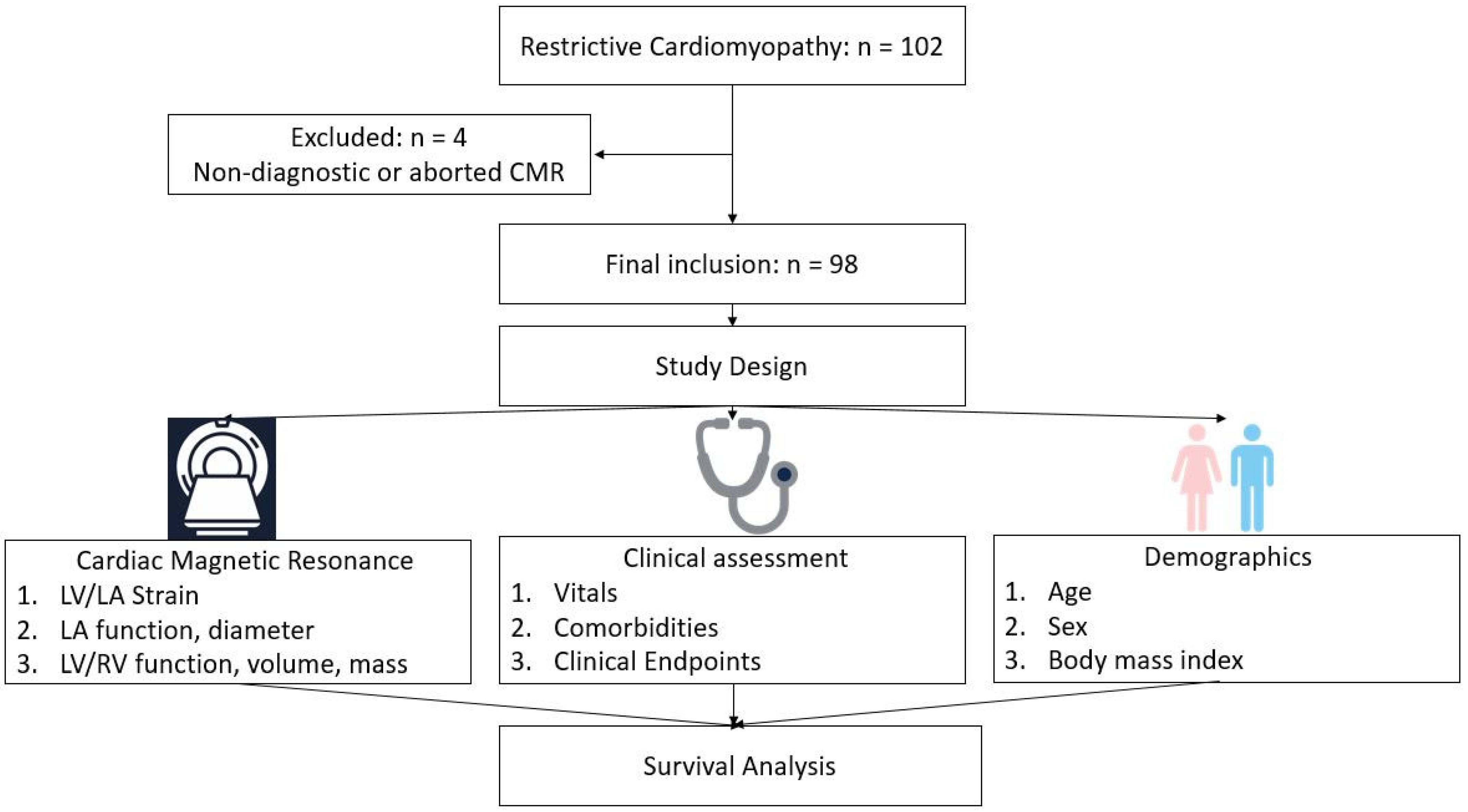
2.1. Study Population
2.2. Clinical Variables and Follow up
2.3. Clinical Endpoints
2.4. Cardiac Magnetic Resonance Imaging—Acquisition
2.5. Cardiac Magnetic Resonance Imaging—Post-Processing
2.6. Statistical Analysis
3. Results
3.1. Study Population
3.2. Imaging Characteristics
3.3. Time to All-Cause Mortality
3.4. Time to Composite Events (All-Cause Mortality and Cardiovascular Hospitalizations)
4. Discussion
4.1. Main Findings
4.2. All-Cause Mortality and Left Atrial Function
4.3. Time to Composite Events and Left Atrial Function
4.4. LGE and Endpoints
4.5. Prior Studies
4.6. Study Limitation
4.7. Future Direction
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DePascale, E.C.; Nasir, K.; Jacoby, D.L. Outcomes of adults with restrictive cardiomyopathy after heart transplantation. J. Heart Lung Transplant. 2012, 13, 1269–1275. [Google Scholar] [CrossRef] [PubMed]
- Muchtar, E.; Blauwet, L.A.; Gertz, M.A. Restrictive cardiomyopathy: Genetics, pathogenesis, clinical manifestations, diagnosis, and therapy. Circ. Res. 2017, 121, 819–837. [Google Scholar] [CrossRef]
- Locatelli, C.; Pradelli, D.; Campo, G.; Spalla, I.; Savarese, A.; Brambilla, P.G.; Bussadori, C. Survival and prognostic factors in cats with restrictive cardiomyopathy: A review of 90 cats. J. Feline Med. Surg. 2018, 20, 1138–1143. [Google Scholar] [CrossRef]
- Patel, A.R.; Kramer, C.M. Role of cardiac magnetic resonance in the diagnosis and prognosis of nonischemic cardiomyopathy. JACC Cardiovasc. Imaging 2017, 10 Pt A, 1180–1193. [Google Scholar] [CrossRef]
- Bisbal, F.; Baranchuk, A.; Braunwald, E.; Bayes de Luna, A.; Bayes-Genis, A. Atrial Failure as a clinical entity: JACC review topic of the week. JACC 2020, 75, 222–232. [Google Scholar] [CrossRef]
- Habibi, M.; Zareian, M.; Venkatesh, B.A.; Samiei, S.; Imai, M.; Wu, C.; Launer, L.J.; Shea, S.; Gottesman, R.F.; Heckbert, S.R.; et al. Left atrial mechanical function and incident ischemic evens independent of AF: Insights from the MESA study. JACC Cardiovasc. Imaging 2019, 12, 2417–2427. [Google Scholar] [CrossRef]
- Avitall, B.; Bi, J.; Mykytsey, A.; Chicos, A. Atrial and ventricular fibrosis induced by atrial fibrillation: Evidence to support early rhythm control. Heart Rhythm 2008, 5, 839–845. [Google Scholar] [CrossRef]
- Elliott, P.; Andersson, B.; Arbustini, E.; Bilinska, Z.; Cecchi, F.; Charron, P.; Dubourg, O.; Kühl, U.; Maisch, B.; McKenna, W.J.; et al. Classification of the cardiomyopathies: A position statement from the European society of cardiology working group on myocardial and pericardial diseases. Eur. Heart J. 2008, 29, 270–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habib, G.; Bucciarelli-Ducci, C.; Caforio, A.L.; Cardim, N.; Charron, P.; Cosyns, B.; Dehaene, A.; Derumeaux, G.; Donal, E.; Dweck, M.R.; et al. Multimodality imaging in restrictive cardiomyopathies: EACVI expert consensus document in collaboration with the “working group on myocardial and pericardial diseases” of the European society of cardiology endorsed by the Indian academy of echocardiography. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1090–1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egan, B.M.; Zhao, Y.; Axon, R.N. US trends in prevalence, awareness, treatment, and control of hypertension, 1988–2008. JAMA 2010, 303, 2043–2050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults. Executive summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2009, 32, S62–S67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosteller, R.D. Simplified calculation of body surface area. N. Engl. J. Med. 1987, 317, 1098. [Google Scholar] [PubMed]
- Stojanovska, J.; Cronin, P.; Gross, B.H.; Kazerooni, E.A.; Tsodikov, A.; Frank, L.; Oral, H. Left atrial function and maximum volume as determined by MDCT are independently associated with atrial fibrillation. Acad. Radiol. 2014, 2, 1162–1171. [Google Scholar] [CrossRef]
- Rossi, A.; Dini, F.L.; Agricola, E.; Faggiano, P.; Benfari, G.; Temporelli, P.L.; Cucco, C.; Scelsi, L.; Vassanelli, C.; Ghio, S. Left atrial dilation in systolic heart function: A marker of poor prognosis, not just a buffer between the left ventricle and pulmonary circulation. J. Echocardiogr. 2018, 16, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Cuspidi, C.; Negri, T.; Tadic, M.V.; Sala, C.; Parati, G. Left atrial enlargement and right ventricular hypertrophy in essential hypertension. Blood Press 2014, 23, 89–95. [Google Scholar] [CrossRef]
- Cioffi, G.; Gerts, E.; Cramauric, D.; Tarantini, L.; Di Lenarda, A.; Pulignano, G.; Del Sindaco, D.; Stefenelli, C.; de Simone, G. Left atrial size and force in patients with systolic chronic heart failure: Comparison with healthy controls and different cardiac diseases. Exp. Clin. Cardiol. 2010, 15, e45–e51. [Google Scholar] [PubMed]
- Khan, M.A.; Yang, E.Y.; Zhan, Y.; Judd, R.M.; Chan, W.; Nabi, F.; Heitner, J.F.; Kim, R.J.; Klem, I.; Nagueh, S.F.; et al. Association of left atrial volume index and all-cause mortality in patients referred for route cardiovascular magnetic resonance: A multicenter study. J. Cardiovasc. Magn. Reson. 2019, 21, 4. [Google Scholar] [CrossRef] [Green Version]
- Rossi, A.; Cicoira, M.; Zanolla, L.; Sandrini, R.; Golia, G.; Zardini, P.; Enriquez-Sarano, M. Determinants and prognostic value of left atrial volume in patients with dilated cardiomyopathy. JACC 2002, 40, 1425–1430. [Google Scholar] [CrossRef] [Green Version]
- Moller, J.E.; Hillis, G.S.; Oh, J.K.; Seward, J.B.; Reeder, G.S.; Wright, R.S.; Park, S.W.; Bailey, K.R.; Pellikka, P.A. Left atrial volume: A powerful predictor of survival after acute myocardial infarction. Circulation 2003, 107, 2207–2212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cameli, M.; Mandoli, G.E.; Mondillo, S. Left atrium: The last bulwark before overt heart failure. Heart Fail. Rev. 2017, 22, 123–131. [Google Scholar] [CrossRef]
- Singh, A.; Addetia, K.; Maffessanti, F.; Mor-Avi, V.; Lang, R.M. LA strain categorization of LV diastolic dysfunction. JACC Cardiovasc. Imaging 2017, 10, 735–743. [Google Scholar] [CrossRef]
- Nochioka, K.; Quarta, C.C.; Claggett, B.; Roca, G.Q.; Rapezzi, C.; Falk, R.H.; Solomon, S.D. Left atrial structure and function in cardiac amyloidosis. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1128–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modesto, K.M.; Dispenzieri, A.; Cauduro, S.A.; Lacy, M.; Khandheria, B.K.; Pellikka, P.A.; Belohlavek, M.; Seward, J.B.; Kyle, R.; Tajik, A.J.; et al. Left atrial myopathy in cardiac amyloidosis: Implications of novel echocardiographic techniques. Eur. Heart J. 2005, 26, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Di Bella, G.; Minutoli, F.; Madaffari, A.; Mazzeo, A.; Russo, M.; Donato, R.; Zito, C.; Aquaro, G.D.; Piccione, M.C.; Pedri, S.; et al. Left atrial function in cardiac amyloidosis. J. Cardiovasc. Med. 2016, 17, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, M.; Steel, K.; Jerosch-Herold, M.; Khin, M.; Tsang, S.; Hauser, T.; Kwong, R.Y. Strong cardiovascular implication of quantitative left atrial contractile function assessed by cardiac magnetic resonance imaging in patients with chronic hypertension. J. Cardiovasc. Magn. Reson. 2011, 13, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, D.A.; Blaschke, D.; Canaan-Kuhl, S.; Krebs, A.; Knobloch, G.; Walter, T.C.; Haverkamp, W. Global cardiac alteration detected by speckle-tracking echocardiography in Fabry disease: Left ventricular, right ventricular, and left atrial dysfunction are common and linked to worse symptomatic status. Int. J. Cardiovasc. Imaging 2015, 31, 301–313. [Google Scholar] [CrossRef]
- Assomull, R.G.; Prasad, S.K.; Lyne, J.; Smith, G.; Burman, E.D.; Khan, M.; Sheppard, M.N.; Poole-Wilson, A.; Pennell, D.J. Cardiovascular magnetic resonance, fibrosis, and prognosis in dilated cardiomyopathy. JACC 2006, 48, 1977–1985. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, E. Heart Mechanics: Magnetic Resonance Imaging; CRC Press: Boca Raton, FL, USA, 2017; 1507p. [Google Scholar]
- Halliday, B.P.; Baksi, J.A.; Gulati, A.; Ali, A.; Newsome, S.; Izgi, C.; Arzanauskaite, M.; Lota, A.; Tayal, U.; Vassiliou, V.S.; et al. Outcome in dilated cardiomyopathy related to the extent, location, and pattern of late gadolinium enhancement. JACC Cardiovasc. Imaging 2019, 12 Pt 2, 1645–1655. [Google Scholar] [CrossRef]
- Austin, B.A.; Tang, W.H.W.; Rodriguez, E.R.; Tan, C.; Flamm, S.D.; Taylor, D.O.; Starling, R.C.; Desai, M.Y. Delayed hyper-enhancement magnetic resonance imaging provides incremental diagnostic and prognostic utility in suspected cardiac amyloidosis. JACC Cardiovasc. Imaging 2009, 2, 1369–1377. [Google Scholar] [CrossRef] [Green Version]
- Pan, J.A.; Kerwin, M.J.; Salerno, M. Native T1 Mapping, Extracellular Volume Mapping, and Late Gadolinium Enhancement in Cardiac Amyloidosis: A Meta-Analysis. J. Am. Coll. Cardiol. Imaging 2020, 13, 1299–1310. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Composite Events | Survival | All | |||||
|---|---|---|---|---|---|---|---|
| Baseline Characteristics | Events (n = 55) | No Events (n = 43) | p-Value | Non-Survived (n = 35) | Survived (n = 63) | p-Value | |
| Age (years) | 65 ± 11 | 57 ± 13 | 0.002 * | 66 ± 11 | 59 ± 13 | 0.017 * | 61 ± 13 |
| Sex (female) | 19 (34%) | 11 (25%) | 0.383 | 13 (26%) | 17 (34%) | 0.369 | 30 (31%) |
| Diabetes n (%) | 22 (40%) | 28 (40%) | 0.285 | 14 (28%) | 20 (40%) | 0.507 | 50 (51%) |
| Hyperlipidemia n (%) | 17 (31%) | 19 (44%) | 0.208 | 10 (44%) | 26 (31) | 0.275 | 36 (37$) |
| Hypertension n (%) | 39 (71%) | 26 (60%) | 0.291 | 24 (60%) | 41 (71%) | 0.824 | 65 (66%) |
| Systemic Amyloid n (%) | 26 (47%) | 13 (30%) | 0.100 | 23 (30%) | 16 (47%) | 0.0002 * | 39 (40%) |
| Multiple Myeloma n (%) | 32 (58%) | 18 (42%) | 0.153 | 24 (42%) | 26 (58%) | 0.011 * | 50 (51%) |
| BMI (kg/m2) | 29 ± 7 | 30 ± 6 | 0.193 | 28 ± 7 | 30 ± 6 | 0.114 | 29 ± 7 |
| BSA (cm/m2) | 2.00 ± 0.3 | 2.07 ± 0.2 | 0.079 | 1.97 ± 0.3 | 2.07 ± 0.2 | 0.036 * | 2 ± 0.2 |
| Composite Outcome | Survival Outcome | All | |||||
|---|---|---|---|---|---|---|---|
| CMR Variables | Events (n = 55) | No Events (n = 43) | p-Value | Non-Survived (n = 35) | Survived (n = 63) | p-Value | |
| LGE | 29 (53%) | 17 (39%) | 0.224 | 19 (53%) | 27 (39%) | 0.298 | 48 (49) |
| LA reservoir strain (%) | 21 ± 11 | 30 ± 12 | 0.0008 * | 19 ± 11 | 28 ± 12 | 0.002 * | 25 ± 12 |
| LA contractile strain (%) | 11 ± 7 | 15 ± 6 | 0.002 * | 11 ± 8 | 14 ± 8 | 0.007 * | 13 ± 7 |
| LA EDV (mL) | 56 ± 36 | 40 ± 23 | 0.029 * | 56 ± 36 | 44 ± 25 | 0.184 | 49 ± 31 |
| LA EF (%) | 42 ± 21 | 53 ± 15 | 0.011 * | 41 ± 22 | 50 ± 17 | 0.054 | 47 ± 19 |
| LV EDV (indexed) | 92 ± 30 | 92 ± 39 | 0.529 | 88 ± 30 | 94 ± 36 | 0.479 | 95 ± 35 |
| LV EF (%) | 48 ± 16 | 50 ± 15 | 0.458 | 48 ± 17 | 49 ± 15 | 0.988 | 49 ± 15 |
| RV EF (%) | 48 ± 15 | 48 ± 13 | 0.924 | 45 ± 16 | 49 ± 12 | 0.449 | 49 ± 13 |
| RV EDV (indexed) | 89 ± 30 | 79 ± 23 | 0.147 | 90 ± 34 | 81 ± 22 | 0.323 | 82 ± 27 |
| LA diameter (mm) | 42 ± 7 | 39 ± 6 | 0.057 | 42 ± 7 | 41 ± 7 | 0.309 | 41 ± 7 |
| LA area (mm) | 25 ± 7 | 22 ± 4 | 0.045 * | 25 ± 7 | 23 ± 5 | 0.075 | 23 ± 6 |
| LV mass (indexed) | 84 ± 36 | 62 ± 22 | 0.0006 * | 79 ± 31 | 71 ± 33 | 0.051 | 74 ± 32 |
| LV GLS (%) | −18 ± 9 | −20 ± 7 | 0.163 | −18 ± 10 | −20 ± 7 | 0.391 | −19 ± 8 |
| (A) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Univariate Regression Analysis | Adjusted Regression Analysis * | ||||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |||
| LA reservoir strain | 0.952 | 0.924 | 0.981 | 0.001 ** | 0.902 | 0.851 | 0.957 | 0.0006 ** |
| LA contractile strain | 0.936 | 0.887 | 0.987 | 0.015 ** | 0.903 | 0.821 | 0.993 | 0.035 |
| LA diameter | 1.030 | 0.982 | 1.081 | 0.220 | 1.022 | 0.961 | 1.088 | 0.482 |
| LA EF | 0.979 | 0.961 | 0.997 | 0.023 ** | 1.043 | 1.010 | 1.076 | 0.010 |
| LGE | 1.651 | 0.845 | 3.224 | 0.142 | 1.596 | 0.754 | 3.377 | 0.222 |
| LV GLS | 1.024 | 0.989 | 1.061 | 0.179 | 1.008 | 0.959 | 1.060 | 0.760 |
| LV EF | 0.996 | 0.975 | 1.017 | 0.684 | 1.030 | 0.995 | 1.065 | 0.091 |
| Systemic amyloidosis | 3.374 | 1.678 | 6.784 | 0.0006 ** | 2.122 | 0.896 | 5.025 | 0.087 |
| (B) | ||||||||
| Variable | Univariate Regression Analysis | Adjusted Regression Analysis * | ||||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |||
| LA reservoir strain | 0.960 | 0.938 | 0.982 | 0.0006 ** | 0.925 | 0.879 | 0.969 | 0.001 ** |
| LA contractile strain | 0.939 | 0.900 | 0.981 | 0.004 ** | 0.912 | 0.846 | 0.983 | 0.016 |
| LA diameter | 1.042 | 1.002 | 1.083 | 0.040 ** | 1.027 | 0.973 | 1.085 | 0.335 |
| LA EF | 0.980 | 0.965 | 0.995 | 0.009 ** | 1.037 | 1.006 | 1.068 | 0.017 |
| LGE | 1.684 | 0.984 | 2.881 | 0.057 ** | 1.549 | 0.870 | 2.756 | 0.224 |
| LV GLS | 1.021 | 0.992 | 1.052 | 0.155 | 1.013 | 0.968 | 1.060 | 0.580 |
| LV EF | 0.993 | 0.976 | 1.010 | 0.415 | 1.004 | 0.978 | 1.051 | 0.753 |
| Systemic amyloidosis | 1.652 | 0.968 | 2.818 | 0.065 | 1.113 | 0.570 | 1.031 | 2.174 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stojanovska, J.; Topaloglu, N.; Fujikura, K.; Khazai, B.; Ibrahim, E.-S.; Tsodikov, A.; Bhave, N.M.; Kolias, T.J. Decreased Left Atrial Reservoir Strain Is Associated with Adverse Outcomes in Restrictive Cardiomyopathy. J. Clin. Med. 2022, 11, 4116. https://doi.org/10.3390/jcm11144116
Stojanovska J, Topaloglu N, Fujikura K, Khazai B, Ibrahim E-S, Tsodikov A, Bhave NM, Kolias TJ. Decreased Left Atrial Reservoir Strain Is Associated with Adverse Outcomes in Restrictive Cardiomyopathy. Journal of Clinical Medicine. 2022; 11(14):4116. https://doi.org/10.3390/jcm11144116
Chicago/Turabian StyleStojanovska, Jadranka, Nevriye Topaloglu, Kana Fujikura, Behnaz Khazai, El-Sayed Ibrahim, Alex Tsodikov, Nicole M. Bhave, and Theodore J. Kolias. 2022. "Decreased Left Atrial Reservoir Strain Is Associated with Adverse Outcomes in Restrictive Cardiomyopathy" Journal of Clinical Medicine 11, no. 14: 4116. https://doi.org/10.3390/jcm11144116