
Intravenous Iron Supplementation for the Treatment of Chemotherapy-Induced Anemia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 and
and
Abstract
:1. Background
2. Materials and Methods
2.1. Data Sources
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Definition of Outcomes
2.5. Data Synthesis and Analysis
3. Results
3.1. Description of Included Studies
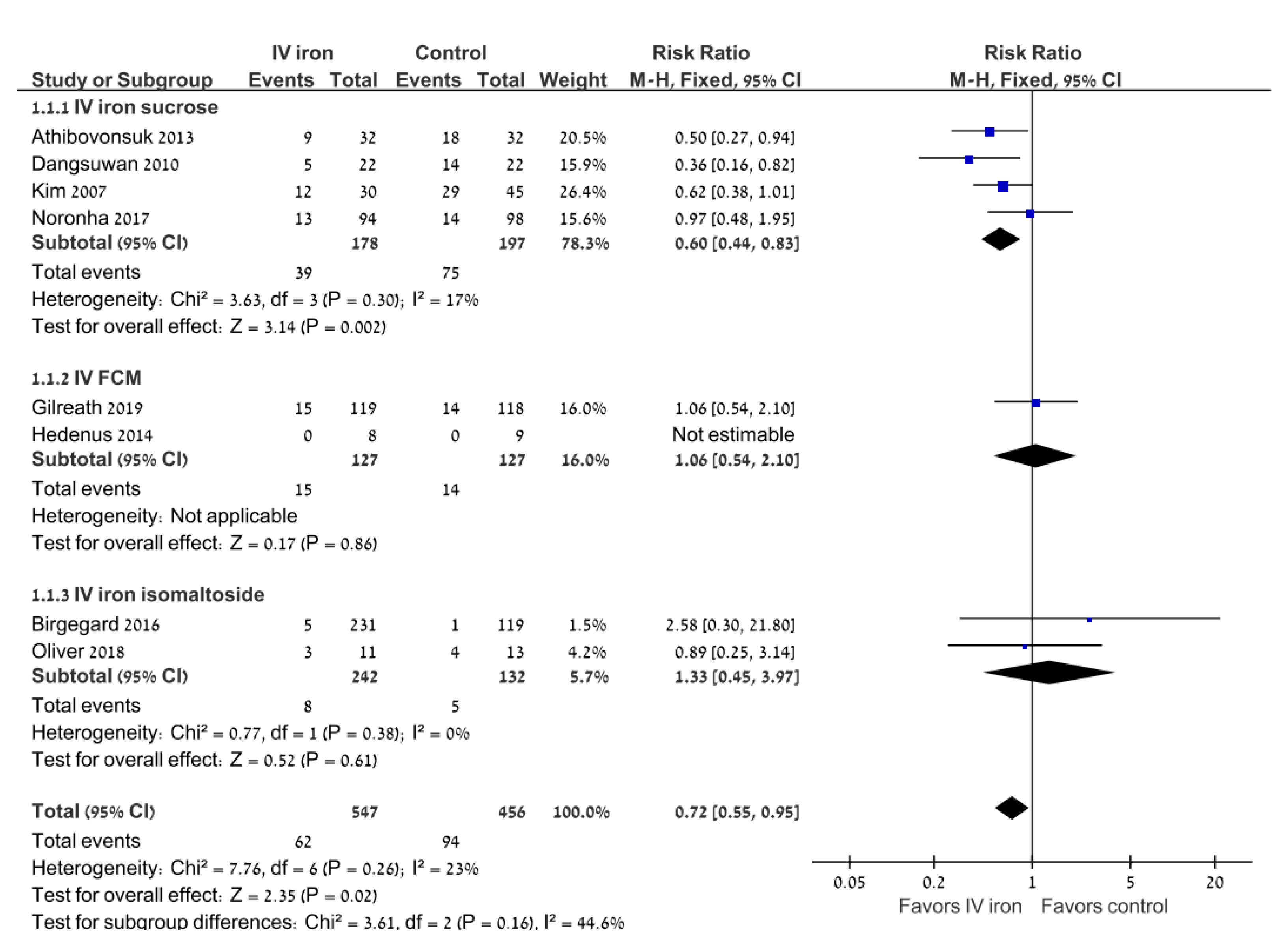
3.2. Primary Outcome: Transfusion Requirements
3.3. Secondary Outcomes
3.4. Safety
4. Discussion
Implications for Practice and Research
Funding
Conflicts of Interest
References
- Ludwig, H.; Van Belle, S.; Barrett-Lee, P.; Birgegård, G.; Bokemeyer, C.; Gascón, P.; Kosmidis, P.; Krzakowski, M.; Nortier, J.; Olmi, P.; et al. The European cancer anaemia survey (ECAS): A large, multinational, prospective survey defining the prevalence, incidence, and treatment of anaemia in cancer patients. Eur. J. Cancer 2004, 40, 2293–2306. [Google Scholar] [CrossRef] [PubMed]
- Gilreath, J.A.; Stenehjem, D.; Rodgers, G.M. Diagnosis and treatment of cancer-related anemia. Am. J. Hematol. 2014, 89, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Harper, P.; Littlewood, T. Anaemia of cancer: Impact on patient fatigue and long-term outcome. Oncology 2005, 69, 2–7. [Google Scholar] [CrossRef]
- Carson, J.L.; Guyatt, G.; Heddle, N.M.; Grossman, B.J.; Cohn, C.S.; Fung, M.K.; Gernsheimer, T.; Holcomb, J.B.; Kaplan, L.J.; Katz, L.M.; et al. Clinical practice guidelines from the AABB: Red blood cell transfusion thresholds and storage. JAMA 2016, 316, 2025–2035. [Google Scholar] [CrossRef] [PubMed]
- Gilreath, J.A.; Rodgers, G.M. How I treat cancer-associated anemia. Blood 2020, 136, 801–813. [Google Scholar] [CrossRef]
- Gabrilove, J.L.; Cleeland, C.S.; Livingston, R.B.; Sarokhan, B.; Winer, E.; Einhorn, L.H. Clinical evaluation of once-weekly dosing of epoetin alfa in chemotherapy patients: Improvements in hemoglobin and quality of life are similar to three-times-weekly dosing. J. Clin. Oncol. 2001, 19, 2875–2882. [Google Scholar] [CrossRef]
- Österborg, A.; Brandberg, Y.; Molostova, V.; Iosava, G.; Abdulkadyrov, K.; Hedenus, M.; Messinger, D. Randomized, double-blind, placebo-controlled trial of recombinant human erythropoietin, epoetin beta, in hematologic malignancies. J. Clin. Oncol. 2002, 20, 2486–2494. [Google Scholar] [CrossRef]
- Boogaerts, M.; Coiffier, B.; Kainz, C. Epoetin beta QOL working group. Impact of epoetin beta on quality of life in patients with malignant disease. Br. J. Cancer 2003, 88, 98895. [Google Scholar] [CrossRef] [Green Version]
- Bokemeyer, C.F.; Aapro, M.S.; Courdi, A.; Foubert, J.; Link, H.; Österborg, A.; Repetto, L.; Soubeyran, P. EORTC guidelines for the use of erythropoietic proteins in anaemic patients with cancer: 2006 update. Eur. J. Cancer 2007, 43, 258–270. [Google Scholar] [CrossRef]
- Hedley, B.D.; Allan, A.L.; Xenocostas, A. The role of erythropoietin and erythropoiesis-stimulating agents in tumor progression. Clin. Cancer Res. 2011, 17, 6373–6380. [Google Scholar] [CrossRef] [Green Version]
- Todaro, M.; Turdo, A.; Bartucci, M.; Iovino, F.; Dattilo, R.; Biffoni, M.; Stassi, G.; Federici, G.; De Maria, R.; Zeuner, A. Erythropoietin activates cell survival pathways in breast cancer stem–like cells to protect them from chemotherapy. Cancer Res. 2013, 73, 6393–6400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, B.; Damrauer, J.S.; Bailey, S.T.; Hadzic, T.; Jeong, Y.; Clark, K.; Fan, C.; Murphy, L.; Lee, C.Y.; Troester, M.A.; et al. Erythropoietin promotes breast tumorigenesis through tumor-initiating cell self-renewal. J. Clin. Investig. 2014, 124, 553–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodnough, L.T. Erythropoietin and iron-restricted erythropoiesis. Exp. Hematol. 2007, 35 (Suppl. S1), 167–172. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, J.D.; Lichtin, A.E.; Woolf, S.H.; Seidenfeld, J.; Bennett, C.L.; Cella, D.; Djulbegovic, B.; Goode, M.J.; Jakubowski, A.A.; Lee, S.J.; et al. American society of clinical oncology/American society of hematology clinical practice guideline update on the use of epoetin and darbepoetin in adult patients with cancer. J. Clin. Oncol. 2010, 28, 4996–5010. [Google Scholar] [CrossRef] [Green Version]
- Bohlius, J.; Bohlke, K.; Castelli, R.; Djulbegovic, B.; Lustberg, M.B.; Martino, M.; Mountzios, G.; Peswani, N.; Porter, L.; Tanaka, T.N.; et al. Management of cancer-associated anemia with erythropoiesis-stimulating agents: ASCO/ASH clinical practice guideline update. Blood Adv. 2019, 3, 1197–1210. [Google Scholar] [CrossRef] [Green Version]
- Bohlius, J.; Schmidlin, K.; Brillant, C.; Schwarzer, G.; Trelle, S.; Seidenfeld, J.; Zwahlen, M.; Clarke, M.; Weingart, O.; Kluge, S.; et al. Recombinant human erythropoiesis-stimulating agents and mortality in patients with cancer: A meta-analysis of randomised trials. Lancet 2009, 373, 1532–1542. [Google Scholar] [CrossRef]
- Bennett, C.L.; Silver, S.M.; Djulbegovic, B.; Samaras, A.T.; Blau, C.A.; Gleason, K.J.; Barnato, S.E.; Elverman, K.M.; Courtney, D.M.; McKoy, J.M.; et al. Venous thromboembolism and mortality associated with recombinant erythropoietin and darbepoetin administration for the treatment of cancer-associated anemia. JAMA 2008, 299, 914–924. [Google Scholar] [CrossRef]
- Henry, D.H.; Dahl, N.V.; Auerbach, M.; Tchekmedyian, S.; Laufman, L.R. Intravenous ferric gluconate significantly improves response to epoetin alfa versus oral iron or no iron in anemic patients with cancer receiving chemotherapy. Oncologist 2007, 12, 231–242. [Google Scholar] [CrossRef] [Green Version]
- Aapro, M.; Österborg, A.; Gascón, P.; Ludwig, H.; Beguin, Y. Prevalence and management of cancer related anaemia, iron deficiency and the specific role of i.v. iron. Ann. Oncol. 2012, 23, 1954–1962. [Google Scholar] [CrossRef]
- Steinmetz, H.T. The role of intravenous iron in the treatment of anemia in cancer patients. Ther. Adv. Hematol. 2012, 3, 177–191. [Google Scholar] [CrossRef]
- Gafter-Gvili, A.; Rozen-Zvi, B.; Vidal, L.; Leibovici, L.; Vansteenkiste, J.; Gafter, U.; Shpilberg, O. Intravenous iron supplementation for the treatment of chemotherapy-induced anaemia—Systematic review and meta-analysis of randomised controlled trials. Acta Oncol. 2012, 52, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0. Available online: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf (accessed on 14 June 2010).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Kim, Y.T.; Kim, S.W.; Yoon, B.S.; Cho, H.J.; Nahm, E.J.; Kim, S.H.; Kim, J.H.; Kim, J.W. Effect of intravenously administered iron sucrose on the prevention of anemia in the cervical cancer patients treated with concurrent chemoradiotherapy. Gynecol. Oncol. 2007, 105, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Dangsuwan, P.; Manchana, T. Blood transfusion reduction with intravenous iron in gynecologic cancer patients receiving chemotherapy. Gynecol. Oncol. 2010, 116, 522–525. [Google Scholar] [CrossRef] [PubMed]
- Athibovonsuk, P.; Manchana, T.; Sirisabya, N. Prevention of blood transfusion with intravenous iron in gynecologic cancer patients receiving platinum-based chemotherapy. Gynecol. Oncol. 2013, 131, 679–682. [Google Scholar] [CrossRef]
- Hedenus, M.; Karlsson, T.; Ludwig, H.; Rzychon, B.; Felder, M.; Roubert, B.; Birgegård, G. Intravenous iron alone resolves anemia in patients with functional iron deficiency and lymphoid malignancies undergoing chemotherapy. Med. Oncol. 2014, 31, 302. [Google Scholar] [CrossRef] [Green Version]
- Birgegård, G.; Henry, D.; Glaspy, J.; Chopra, R.; Thomsen, L.L.; Auerbach, M. A Randomized Noninferiority Trial of Intravenous Iron Isomaltoside versus Oral Iron Sulfate in Patients with Nonmyeloid Malignancies and Anemia Receiving Chemotherapy: The PROFOUND Trial. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2016, 36, 402–414. [Google Scholar] [CrossRef]
- Noronha, V.; Joshi, A.; Patil, V.M.; Banavali, S.D.; Gupta, S.; Parikh, P.M.; Marfatia, S.; Punatar, S.; More, S.; Goud, S.; et al. Phase III randomized trial comparing intravenous to oral iron in patients with cancer-related iron deficiency anemia not on erythropoiesis stimulating agents. Asia-Pacific J. Clin. Oncol. 2017, 14, e129–e137. [Google Scholar] [CrossRef]
- Oliver, N.; Keeler, B.; Simpson, J.A.; Madhusudan, S.; Brookes, M.; Acheson, A. Feasibility of intravenous iron isomaltoside to improve anemia and quality of life during palliative chemotherapy for esophagogastric adenocarcinoma. Nutr. Cancer 2018, 70, 1106–1117. [Google Scholar] [CrossRef]
- Gilreath, J.A.; Makharadze, T.; Boccia, R.V.; Krupa, A.; Henry, D.H. Efficacy and Safety of Ferric Carboxymaltose Injection in Reducing Anemia in Patients Receiving Chemotherapy for Non-Myeloid Malignancies: A Phase 3, Placebo-Controlled Study (IRON CLAD). Blood 2019, 134, 3535. [Google Scholar] [CrossRef]
- Sahu, S.; Hemlata; Verma, A. Adverse events related to blood transfusion. Indian J. Anaesth. 2014, 58, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.; Tobian, A.A.R.; Shaz, B.H. Noninfectious transfusion-associated adverse events and their mitigation strategies. Blood 2019, 133, 1831–1839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.-L.; Tai, Y.-H.; Lin, S.-P.; Chan, M.-Y.; Chen, H.-H.; Chang, K.-Y. The impact of blood transfusion on recurrence and mortality following colorectal cancer resection: A propensity score analysis of 4030 patients. Sci. Rep. 2018, 8, 13345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estcourt, L.J.; Malouf, R.; Trivella, M.; Fergusson, D.A.; Hopewell, S.; Murphy, M.F. Restrictive versus liberal red blood cell transfusion strategies for people with haematological malignancies treated with intensive chemotherapy or radiotherapy, or both, with or without haematopoietic stem cell support. Cochrane Database Syst. Rev. 2017, 2017, CD011305. [Google Scholar] [CrossRef]
- Fortner, B.V.; Tauer, K.; Zhu, L.; Okon, T.A.; Moore, K.; Templeton, D.; Schwartzberg, L. Medical visits for chemotherapy and chemotherapy-induced neutropenia: A survey of the impact on patient time and activities. BMC Cancer 2004, 4, 22. [Google Scholar] [CrossRef] [Green Version]
- Tokunaga, R.; Nakagawa, S.; Miyamoto, Y.; Ohuchi, M.; Izumi, D.; Kosumi, K.; Taki, K.; Higashi, T.; Miyata, T.; Yoshida, N.; et al. The impact of preoperative anaemia and anaemic subtype on patient outcome in colorectal cancer. Color. Dis. 2018, 21, 100–109. [Google Scholar] [CrossRef] [Green Version]
- Clarke, H.; Pallister, C.J. The impact of anaemia on outcome in cancer. Int. J. Lab. Hematol. 2005, 27, 1–13. [Google Scholar] [CrossRef]
- Avni, T.; Bieber, A.; Grossman, A.; Green, H.; Leibovici, L.; Gafter-Gvili, A. The Safety of Intravenous Iron Preparations. Mayo Clin. Proc. 2015, 90, 12–23. [Google Scholar] [CrossRef] [Green Version]
- Aapro, M.; Beguin, Y.; Bokemeyer, C.; Dicato, M.; Gascón, P.; Glaspy, J.; Hofmann, A.; Link, H.; Littlewood, T.; Ludwig, H.; et al. Management of anemia and iron deficiency in patients with cancer: ESMO clinical practice guidelines. Ann. Oncol. 2018, 29 (Suppl. S4), iv96–iv110. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Study | Treatment Arms | Number of Randomized Patients | IV Iron Type and Dosing Schedule | Type of Malignancy | Inclusion Criteria | Hb and Ferritin at Baseline | TSAT at Baseline | Ferritin at Baseline |
|---|---|---|---|---|---|---|---|---|
| Kim 2007 [24] | IV iron sucrose | 30 | Iron sucrose 200 mg, one single dose after chemotherapy infusion for a maximum of 6 weeks | All patients with cervical cancer treated with concurrent chemoradiotherapy | Hgb < 12 g/dL and Hgb > 10 g/dL | 11.27 ± 1.94 g/dL | Not reported | Not reported |
| No iron | 45 | 11.33 ± 2.14 g/dL | ||||||
| Dangsuwan 2010 [25] | IV iron sucrose | 22 | Iron sucrose 200 mg, one single dose after chemotherapy infusion | All patients with ovarian or endometrial cancer receiving platinum-based chemotherapy | Hgb < 10 g/dL | 8.9 ±0.6 g/dL | Not reported | Not reported |
| Oral iron | 22 | Ferrous fumarate 600 mg daily | 9 ±0.6 g/dL | |||||
| Athibovonsuk 2013 [26] | IV iron sucrose | 32 | Iron sucrose 200 mg, one single dose after chemotherapy infusion for 6 weeks | All patients with ovarian or endometrial cancer receiving platinum-based chemotherapy | Hgb < 12 g/dL (women) or Hgb < 13 g/dL (men) | 11.3 ± 0.8 g/dL | Not reported | Not reported |
| Oral iron | 32 | Ferrous fumarate 600 mg daily during the treatment period | 11.4 ± 1 g/dL | |||||
| Hedenus 2014 [27] | IV iron carboxymaltose | 8 | Ferric carboxymaltose 1000 mg weekly for 8 weeks | All patients with lymphoid malignancies | Hgb < 10.5 g/dL and FID TSAT < 20%, ferritin > 30 ng/mL (women) or > 40 ng/mL (men) | Hb 9.5 (9–10.5) g/dL Ferritin 216 (65–800) ng/mL | 16 (3–35) | 216 (65–800) mcg/L |
| No iron | 11 | Hb 9.8 (8.4–10.6) g/dL Ferritin 322 (8–707) ng/mL | 18 (0–31) | 322 (8–707) mcg/L | ||||
| Birgegård 2016 [28] | IV iron isomaltoside (infusion) | 114 | Iron isomaltoside up to 1000 mg for a maximum of 2 weeks | All types | Hgb < 12.0 g/dL, TSAT < 50%, serum ferritin < 800 ng/ml | Hb 10.6 ± 8.7 g/dL Ferritin 254.2 ± 290.3 ng/mL | 58.1 ± 13.5 | 254.2 ± 290.3 mcg/L |
| IV iron isomaltoside (bolus) | 117 | Iron isomaltoside 500 mg weekly for 4 weeks | Hb 14.1 ± 14.4 g/dL Ferritin 222.0 ± 207.9 ng/mL | 60.1 ± 14.6 | 222.0 ± 207.9 mcg/L | |||
| Oral iron | 119 | Iron sulfate 200 mg daily for 12 weeks | Hb 14.5 ±11.9 g/dL Ferritin 247.4 ± 254 ng/mL | 58.9 ± 13.3 | 247.4 ± 254 mcg/L | |||
| Noronha 2017 [29] | IV iron sucrose | 94 | Iron sucrose 760 mg after chemotherapy infusion for 2 weeks | All types | Hgb < 10 g/dL and TSAT < 20% | 10.2 (7,2–11.9) g/dL | Not reported | Not reported |
| Oral iron | 98 | 300 mg daily for 2 weeks | 10.1 (7.2–12.5) g/dL | |||||
| Oliver 2018 [30] | IV iron isomaltoside | 14 | Iron isomaltoside, single dose | All patients with esophageal adenocarcinoma | Hgb < 12 g/dL (women) or Hb < 13 g/dL (men) | Hb 9.96 g/dL Ferritin 105 (120) ng/mL | Not reported | Not reported |
| No iron | 13 | Hb 11.45 g/dL Ferritin 161 (123) ng/mL | ||||||
| Jeffrey A. Gilreath 2019 [31] | IV iron carboxymaltose | 122 | 15 mg/kg (750 mg max) for 2 weeks | All types | Hgb < 11 g/dL and FID, TSAT < 35%, ferritin 100–800 ng/mL | Not reported | Not reported | Not reported |
| No iron | 122 |
| Study | Sequence Generation | Allocation Concealment | Blinding | Incomplete Outcome Data | Selective Outcome Reporting |
|---|---|---|---|---|---|
| Kim 2007 [24] | Low risk | Unclear risk | None | Low risk | Low risk |
| Dangsuwan 2010 [25] | Unclear risk | Unclear risk | None | Low risk | Low risk |
| Athibovonsuk 2013 [26] | Low risk | Unclear risk | None | Low risk | Low risk |
| Hedenus 2014 [27] | Low risk | Unclear risk | None | Low risk | Low risk |
| Birgegård 2016 [28] | Low risk | Unclear risk | None | Low risk | Low risk |
| Noronha 2017 [29] | Low risk | Unclear risk | None | Low risk | Low risk |
| Oliver 2018 [30] | Unclear risk | Unclear risk | Only patient-blinded | Low risk | Low risk |
| Jeffrey A. Gilreath 2019 [31] | Low risk | Low risk | Double-blind | Low risk | Low risk |
| Relative Risk | 95% Confidence Interval | Number of Trials | ||
|---|---|---|---|---|
| Analysis according to type of IV iron preparation | Iron sucrose | 0.67 | 0.47–0.94 | 4 |
| Iron ferric carboxymaltose | 1.06 | 0.54–2.1 | 2 | |
| Iron isomaltoside | 2.58 | 0.3–21.8 | 2 | |
| Analysis according to type of malignancy | Solid tumors | 1.06 | 0.68–1.66 | 5 |
| Lymphoproliferative malignancy | 1 | |||
| Gynecologic malignancy | 0.51 | 0.36–0.73 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buchrits, S.; Itzhaki, O.; Avni, T.; Raanani, P.; Gafter-Gvili, A. Intravenous Iron Supplementation for the Treatment of Chemotherapy-Induced Anemia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2022, 11, 4156. https://doi.org/10.3390/jcm11144156
Buchrits S, Itzhaki O, Avni T, Raanani P, Gafter-Gvili A. Intravenous Iron Supplementation for the Treatment of Chemotherapy-Induced Anemia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2022; 11(14):4156. https://doi.org/10.3390/jcm11144156
Chicago/Turabian StyleBuchrits, Shira, Oranit Itzhaki, Tomer Avni, Pia Raanani, and Anat Gafter-Gvili. 2022. "Intravenous Iron Supplementation for the Treatment of Chemotherapy-Induced Anemia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 11, no. 14: 4156. https://doi.org/10.3390/jcm11144156