
Diagnostic Delay in Paediatric Inflammatory Bowel Disease—A Systematic Investigation

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Study Questionnaries
2.3. Healthcare Data
2.4. Data Extraction
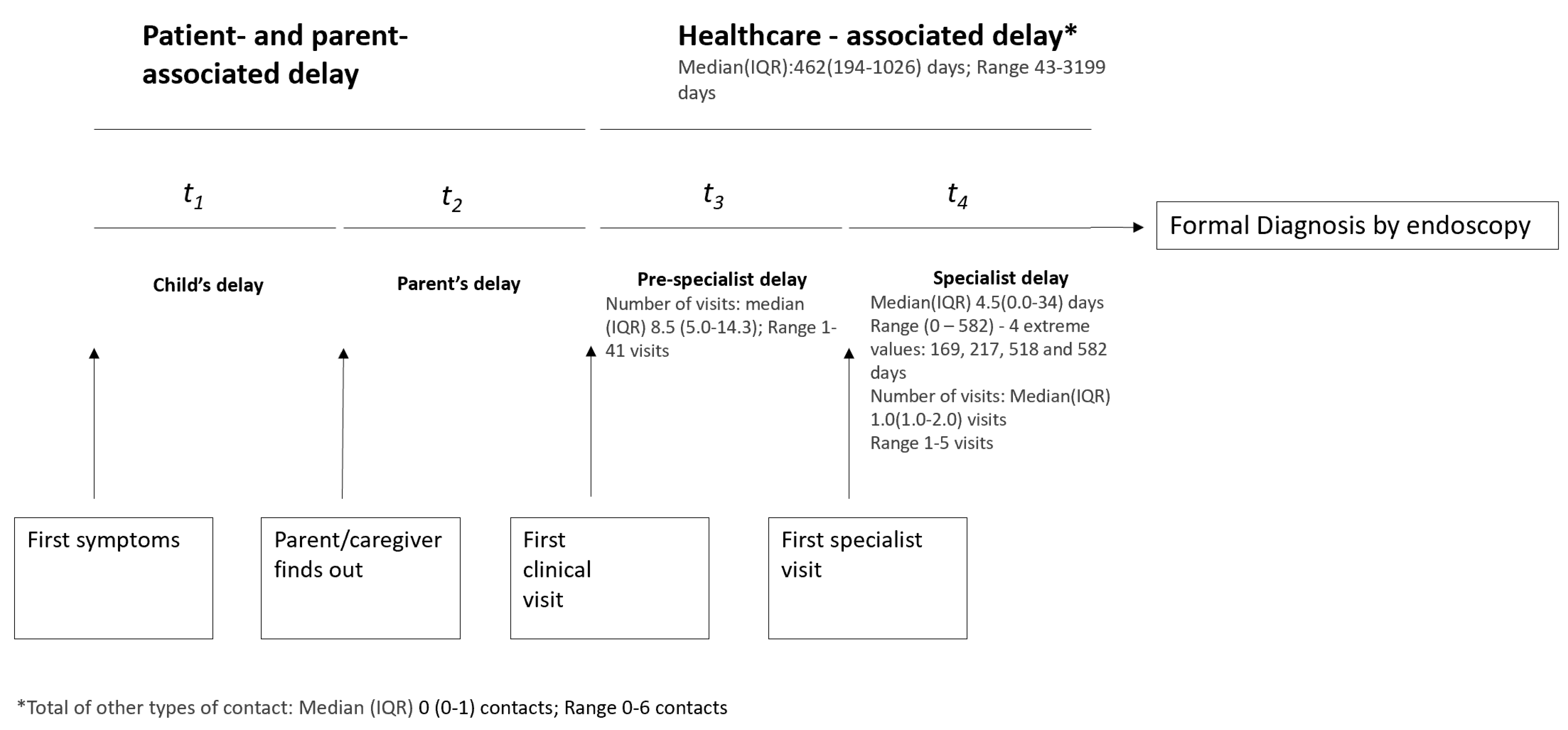
- Patient-associated delay: Time from the first symptoms to notifying parent/caregiver.
- Parent-associated delay: Time from parents noticing the symptoms to seeking healthcare.
- Healthcare delay: From the first clinical visit to formal diagnosis.
- a.
- Pre-specialist delay: First healthcare visit to specialist visit/formal diagnosis.
- b.
- Specialist delay: Time from the first specialist visit to formal diagnosis.
- Total DD: From first symptoms (as reported by the patient/parent) to formal diagnosis of disease.
- Number of clinical contacts: Number of in-person visits to health professional with complaints related to the IBD diagnosis were counted. Additional forms of contact, such as phone calls, emails and others were counted separately. The number of hospitalisations was also counted for each participant.
2.5. Statistical Analysis
3. Results
3.1. Data Summary
3.2. Study Sample
3.3. Healthcare-Associated Diagnostic Delays
3.4. Patient-Associated Delays
3.5. Parent-Associated Delays
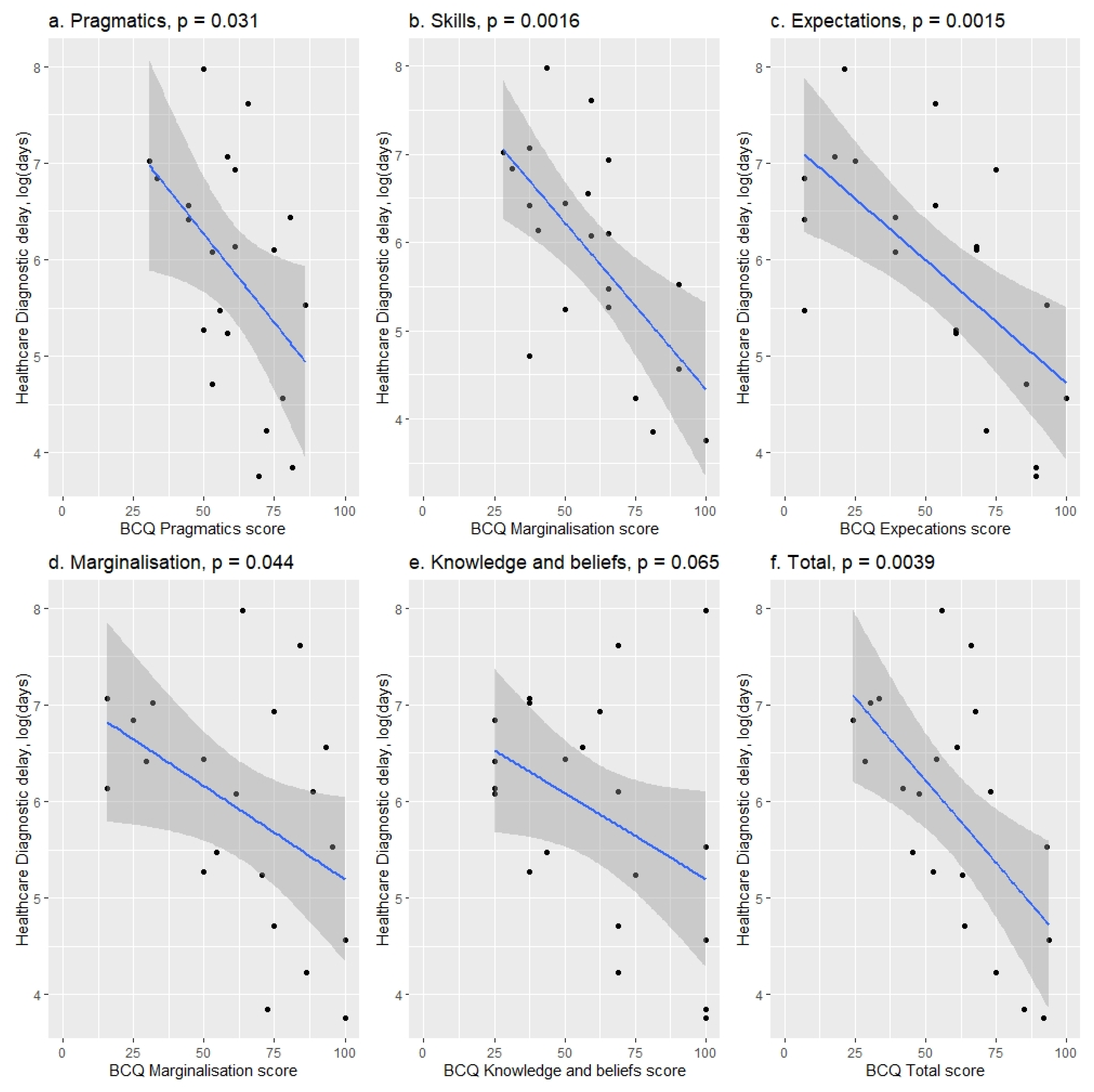
3.6. Healthcare Diagnostic Delays: Simple Linear Regression Analysis
3.7. Patient and Parent-Associated Delay: Logistic Ordinal Regression Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Event of Interest (Dates) | Definition and Specification |
|---|---|
| First symptoms 1 | First IBD symptoms, as reported by the patient or their parent/caregiver. |
| First contact with parents/caregivers/other 1 | Defined as the first person the child presented the symptoms to, such as parent, caregiver, other family member. In case the patient went directly to a doctor this would be their first contact. |
| First healthcare contact 2 | First visit to a healthcare professional due to potential IBD symptoms. All obtained healthcare data were reviewed for the first presentation with the following symptoms as defined in [1,2] and Community Health pathways *:
|
| First relevant specialist visit 2 | First specialist that would make final diagnosis/start of treatment; in this study gastroenterologist. |
| Formal diagnosis 2 | IBD diagnosis confirmed by endoscopy |
| Patient-associated delay | Time from the first symptoms to notifying parent/caregiver |
| Parent-associated delay | Time from parents noticing the symptoms to seeking healthcare |
| Healthcare delay | From the first clinical visit to formal diagnosis |
| Total DD ** | From first symptoms (as reported by the patient/parent) to formal diagnosis of disease |
| Number of clinical contacts | Number of in-person visits to healthcare professional with complains related to the IBD diagnosis were counted. Additional forms of contact, such as phone calls, emails and other were counted separately. The number of hospitalisations was also counted for each participant. |
| Other types of contact | Contacts with healthcare professional not made in-person e.g., e-mail, phone call, text message. |
| Predictors | Outcome Variables | |||||
|---|---|---|---|---|---|---|
| Patient Delayb, n = 29 | Parent Delayb, n = 27 | |||||
| Coefficient Estimate (SD) | p-Value | AIC Value | Coefficient Estimate (SD) | p-Value | AIC Value | |
| Age at first symptomsa | OR: 0.96 (1.10) | 0.72 | 91.8 | OR: 0.97 (1.07) | 0.63 | 80.8 |
| Patient Sex b, baseline—Male | OR: 5.1 (2.1) | 0.032 * | 87.0 | OR: 0.74 (2.08) | 0.68 | 80.9 |
| Patient diagnosisb, base—Crohn’s | OR: 1.16 (2.1) | 0.84 | 91.9 | OR: 1.57 (2.63) | 0.64 | 80.8 |
| Highest level of education in the household at diagnosisb, baseline—no qualification | OR: 0.30 (1.74) | 0.030 * | 62.1 | OR: 0.48 (1.61) | 0.12 | 78.6 |
| Complete log | ||||||
| Apprenticeship or advanced training (level 4–6) | ||||||
| University degree | ||||||
| Household income at diagnosisb, baseline—below average | OR: 0.38 (1.7) | 0.060 | 63.7 | OR: 0.59 (1.78) | 0.34 | 80.1 |
| Complete log | ||||||
| Average | ||||||
| Above average | ||||||
| Parents/caregivers had prior knowledge of IBD before diagnosisb, baseline—no | - | - | - | OR: 2.70 (2.13) | 0.19 | 79.2 |
| Barriers to care Questionnaire | ||||||
| Skillsa | - | - | - | OR: 1.0 (1.0) | 0.40 | 78.4 |
| Pragmaticsa | - | - | - | OR: 1.0 (1.0) | 0.73 | 79.0 |
| Expectationsa | - | - | - | OR: 1.0 (1.0) | 0.81 | 79.1 |
| Marginalizationa | - | - | - | OR: 1.0 (1.0) | 0.65 | 78.9 |
| Knowledge and Beliefsa | - | - | - | OR: 1.0 (1.0) | 0.67 | 78.9 |
| Totala | - | - | - | OR: 1.0 (1.0) | 0.60 | 78.9 |
| Reservations to share symptoms by the patientb, no | OR: 0.99 (1.01) | 0.40 | 91.2 | - | - | - |
| Question | % (n) |
|---|---|
| How old was your child when their symptoms first occurred? | |
| 0–4 years | 30 (8/27) |
| 5–9 years | 4 (1/27) |
| 10–14 years | 52 (14/27) |
| 15–18 years | 15 (4/27) |
| How did you become aware of their symptoms? (multiple choices possible) | |
| My child told me | 64 (18/28) |
| School teachers or school nurses told me | 14 (4/28) |
| I noticed them myself | 54 (15/28) |
| Who did you contact first about the symptoms? | |
| GP | 75 (21/28) |
| Paediatrician | 4 (1/28) |
| Other: | 21 (6/28) |
| Plunket nurse | 7 (2/28) |
| Surgeon | 4 (1/28) |
| GP and Gastroenterologist | 4 (1/28) |
| GP and Paediatrician | 4 (1/28) |
| GP and Emergency department | 4 (1/28) |
| How long did you initially wait before seeking help from a healthcare professional? | |
| Less than a week | 36 (10/28) |
| 1 week—less than a month | 25 (7/28) |
| 1 month—less than 2 months | 7 (2/28) |
| 2 months—less than 6 months | 14 (4/28) |
| 6 months | 4 (1/28) |
| More than 1 year | 4 (1/28) |
| I do not know/remember | 11 (3/28) |
| Did you have any prior knowledge about IBD and its symptoms BEFORE your child experienced them? | |
| Yes | 14 (4/28) |
| No | 64 (18/28) |
| Some | 21 (6/28) |
| Explanatory Variables | Outcome Variable—Total Healthcare Delay a, n = 26 | ||
|---|---|---|---|
| % Change (SD) | p-Value | Adj. R-Sq. Value | |
| Patient’s Age at first symptoms a | |||
| Complete log | −7 (4) % | 0.11 | 0.069 |
| Filtered log | −7 (4) % | 0.091 | 0.091 |
| Sex of the patient b, baseline male | |||
| Complete log | 17 (64) % | 0.75 | −0.039 |
| Filtered log | −17 (60) % | 0.70 | −0.040 |
| IBD diagnosis b, baseline Crohn’s disease | |||
| Complete log | 27 (70) % | 0.66 | −0.036 |
| Filtered log | −6 (71) % | 0.90 | −0.047 |
| Highest level of education in the household at diagnosis b, baseline—no qualification | |||
| Complete log | 0.0093 | ||
| Approximately average | 166 (123) % | 0.24 | |
| Above average | 16 (88) % | 1.0 | |
| Filtered log | 0.064 | ||
| Approximately average | 166 (109.4) % | 0.20 | |
| Above average | −17 (79.8) % | 0.76 | |
| Household income at diagnosis b, baseline—below average | |||
| Complete log | 0.31 | ||
| Average | −21 (65.6) % | 0.64 | |
| Above Average | −85 (82.5) % | 0.0059 ** | |
| Filtered log | 0.31 | ||
| Average | 6 (66.6) % | 0.91 | |
| Above Average | −79 (82.0) % | 0.018 * | |
| Parents/caregivers had prior knowledge of IBD before diagnosis b, baseline—no | |||
| Complete log | −52 (71.5) % | 0.19 | 0.037 |
| Filtered log | −43 (68.8) % | 0.27 | −0.015 |
| Barriers to Care Questionnaire | |||
| Skills a Complete log Filtered log | |||
| −4 (1.0) % | 0.0016 ** | 0.39 | |
| −3 (0.99) % | 0.0023 ** | 0.38 | |
| Pragmatics a | |||
| Complete log | −4 (1.6) % | 0.031 * | 0.18 |
| Filtered log | −3 (1.5) % | 0.044 * | 0.16 |
| Expectations a | |||
| Complete log | −3 (0.69) % | 0.0015 ** | 0.39 |
| Filtered log | −2 (0.69) % | 0.0037 ** | 0.35 |
| Marginalisation a | |||
| Complete log | −2 (0.90) % | 0.044 * | 0.15 |
| Filtered log | −2 (0.91) % | 0.031 ** | 0.19 |
| Knowledge and Beliefs a | |||
| Complete log | −4 (2.1) % | 0.065 | 0.12 |
| Filtered log | −3 (0.78) % | 0.0035 *** | 0.35 |
| Total a | |||
| Complete log | −3 (1.0) % | 0.0039 *** | 0.33 |
| Filtered log | −3 (0.95) % | 0.0024 *** | 0.38 |
| Range and Median (IQR) for Individual BCQ Subscales, n = 27 | |
|---|---|
| Total Score | |
| Median (IQR) | 61 (48–74) |
| Range | 24–94 |
| Skills Score | |
| Median (IQR) | 59 (44–70) |
| Range | 28–100 |
| Pragmatics Score | |
| Median (IQR) | 61 (51–72) |
| Range | 31–86 |
| Expectations Score | |
| Median (IQR) | 61 (38–73) |
| Range | 7–100 |
| Marginalisation Score | |
| Median (IQR) | 66 (48–85) |
| Range | 16–100 |
| Knowledge & Beliefs Score | |
| Median (IQR) | 63 (41–72) |
| Range | 25–100 |
References
- Gomollón, F.; Dignass, A.; Annese, V.; Tilg, H.; Van Assche, G.; Lindsay, J.O.; Peyrin-Biroulet, L.; Cullen, G.J.; Daperno, M.; Kucharzik, T.; et al. 3rd European Evidence-based Consensus on the Diagnosis and Management of Crohn’s Disease 2016: Part 1: Diagnosis and Medical Management. J. Crohn’s Colitis 2017, 11, 3–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.B.; Hart, A.L.; Hindryckx, P.; et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders. J. Crohn’s Colitis 2017, 11, 649–670. [Google Scholar] [CrossRef] [PubMed]
- Austrian IBD Study Group (ATISG); Novacek, G.; Gröchenig, H.P.; Haas, T.; Wenzl, H.; Steiner, P.; Koch, R.; Feichtenschlager, T.; Eckhardt, G.; Mayer, A.; et al. Diagnostic delay in patients with inflammatory bowel disease in Austria. Wien. Klin. Wochenschr. 2019, 131, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.R.; Rodriguez, J.R. Clinical presentation of Crohn’s, ulcerative colitis, and indeterminate colitis: Symptoms, extraintestinal manifestations, and disease phenotypes. Semin. Pediatric Surg. 2017, 26, 349–355. [Google Scholar] [CrossRef]
- Mikocka-Walus, A.; Knowles, S.R.; Keefer, L.; Graff, L. Controversies Revisited: A Systematic Review of the Comorbidity of Depression and Anxiety with Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2016, 22, 752–762. [Google Scholar] [CrossRef]
- Rogala, L.; Miller, N.; Graff, L.A.; Rawsthorne, P.; Clara, I.; Walker, J.R.; Lix, L.; Ediger, J.P.; McPhail, C.; Bernstein, C.N. Population-based controlled study of social support, self-perceived stress, activity and work issues, and access to health care in inflammatory bowel disease. Inflamm. Bowel Dis. 2008, 14, 526–535. [Google Scholar] [CrossRef]
- Ricciuto, A.; Fish, J.R.; Tomalty, D.E.; Carman, N.; Crowley, E.; Popalis, C.; Muise, A.; Walters, T.D.; Griffiths, A.M.; Church, P.C. Diagnostic delay in Canadian children with inflammatory bowel disease is more common in Crohn’s disease and associated with decreased height. Arch. Dis. Child 2018, 103, 319–326. [Google Scholar] [CrossRef]
- De Greef, E.; Mahachie John, J.M.; Hoffman, I.; Smets, F.; Van Biervliet, S.; Scaillon, M.; Hauser, B.; Paquot, I.; Alliet, P.; Arts, W.; et al. Profile of pediatric Crohn’s disease in Belgium. J. Crohn’s Colitis 2013, 7, e588–e598. [Google Scholar] [CrossRef] [Green Version]
- Gower-Rousseau, C.; Dauchet, L.; Vernier-Massouille, G.; Tilloy, E.; Brazier, F.; Merle, V.; Dupas, J.-L.; Savoye, G.; Baldé, M.; Marti, R.; et al. The Natural History of Pediatric Ulcerative Colitis: A Population-Based Cohort Study. Am. J. Gastroenterol. 2009, 104, 2080–2088. [Google Scholar] [CrossRef]
- Jiménez Treviño, S.; Pujol Muncunill, G.; Martín-Masot, R.; Rodríguez Martínez, A.; Segarra Cantón, O.; Peña Quintana, L.; Armas Ramos, H.; Eizaguirre Arocena, F.J.; Barrio Torres, J.; García Burriel, J.I.; et al. Spanish Pediatric Inflammatory Bowel Disease Diagnostic Delay Registry: SPIDER Study from Sociedad Española de Gastroenterología, Hepatología y Nutrición Pediátrica. Front. Pediatr. 2020, 8, 584278. [Google Scholar] [CrossRef]
- Rinawi, F.; Assa, A.; Eliakim, R.; Mozer-Glassberg, Y.; Nachmias-Friedler, V.; Niv, Y.; Rosenbach, Y.; Silbermintz, A.; Zevit, N.; Shamir, R. Risk of Colectomy in Patients with Pediatric-onset Ulcerative Colitis. J. Pediatric Gastroenterol. Nutr. 2017, 65, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Savoye, G.; Salleron, J.; Gower-Rousseau, C.; Dupas, J.-L.; Vernier-Massouille, G.; Fumery, M.; Merle, V.; Lerebours, E.; Cortot, A.; Turck, D.; et al. Clinical predictors at diagnosis of disabling pediatric Crohn’s disease. Inflamm. Bowel Dis. 2012, 18, 2072–2078. [Google Scholar] [CrossRef] [PubMed]
- Schoepfer, A.; Santos, J.; Fournier, N.; Schibli, S.; Spalinger, J.; Vavricka, S.; Safroneeva, E.; Aslan, N.; Rogler, G.; Braegger, C.; et al. Systematic Analysis of the Impact of Diagnostic Delay on Bowel Damage in Paediatric Versus Adult Onset Crohn’s Disease. J. Crohn’s Colitis 2019, 13, 1334–1342. [Google Scholar] [CrossRef] [PubMed]
- Timmer, A.; Behrens, R.; Buderus, S.; Findeisen, A.; Hauer, A.; Keller, K.-M.; Kliemann, G.; Lang, T.; Lohr, W.; Rzehak, P.; et al. Childhood Onset Inflammatory Bowel Disease: Predictors of Delayed Diagnosis from the CEDATA German-Language Pediatric Inflammatory Bowel Disease Registry. J. Pediatrics 2011, 158, 467–473.e2. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Koo, J.S.; Choe, J.W.; Suh, S.J.; Kim, S.Y.; Hyun, J.J.; Jung, S.W.; Jung, Y.K.; Yim, H.J.; Lee, S.W. Diagnostic delay in inflammatory bowel disease increases the risk of intestinal surgery. World J. Gastroenterol. 2017, 23, 6474–6481. [Google Scholar] [CrossRef]
- Abraham, B.P.; Mehta, S.; El-Serag, H.B. Natural history of pediatric-onset inflammatory bowel disease: A systematic review. J. Clin. Gastroenterol. 2012, 46, 581–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubinsky, M. Special issues in pediatric inflammatory bowel disease. World J. Gastroenterol. 2008, 14, 413–420. [Google Scholar] [CrossRef] [Green Version]
- Coppell, K.J.; Galts, C.P.-C.; Huizing, F.Y.; Norton, J.K.; Gray, A.R.; Schultz, K.; Hobbs, C.E.; Aluzaite, K.; Schultz, M. Annual Incidence and Phenotypic Presentation of IBD in Southern New Zealand: An 18-Year Epidemiological Analysis. Inflamm. Intest. Dis. 2018, 3, 32–39. [Google Scholar] [CrossRef]
- Lopez, R.N.; Evans, H.M.; Appleton, L.; Bishop, J.; Chin, S.; Mouat, S.; Gearry, R.B.; Day, A.S. Prospective Incidence of Paediatric Inflammatory Bowel Disease in New Zealand in 2015: Results from the Paediatric Inflammatory Bowel Disease in New Zealand (PINZ) Study. J. Pediatr. Gastroenterol. Nutr. 2018, 66, e122–e126. [Google Scholar] [CrossRef]
- Lopez, R.N.; Appleton, L.; Gearry, R.B.; Day, A.S. Rising Incidence of Paediatric Inflammatory Bowel Disease in Canterbury, New Zealand, 1996–2015. J. Pediatr. Gastroenterol. Nutr. 2018, 66, e45–e50. [Google Scholar] [CrossRef]
- O’Neill, J. IBD Database. EpiSoft. Available online: https://episofthealth.com/solutions-other-specialties/other-specialties-ibd-emr-01-scheduling/ (accessed on 25 May 2021).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Seid, M.; Sobo, E.J.; Gelhard, L.R.; Varni, J.W. Parents’ reports of barriers to care for children with special health care needs: Development and validation of the barriers to care questionnaire. Ambul. Pediatr. 2004, 4, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Seid, M.; Opipari-Arrigan, L.; Gelhard, L.R.; Varni, J.W.; Driscoll, K. Barriers to care questionnaire: Reliability, validity, and responsiveness to change among parents of children with asthma. Acad. Pediatr. 2009, 9, 106–113. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Arcos-Machancoses, J.V.; Donat-Aliaga, E.; Polo-Miquel, B.; Masip-Simó, E.; Ribes-Koninckx, C.; Pereda-Pérez, A. Description and study of risk factors for the diagnostic delay of paediatric inflammatory bowel disease. Anales de Pediatría 2015, 82, 247–254. [Google Scholar] [CrossRef]
- Saadah, O.I.; El Mouzan, M.; Al Mofarreh, M.; Al Edreesi, M.; Hasosah, M.; Al-Hussaini, A.; AlSaleem, K. Characteristics of Pediatric Crohn’s Disease in Saudi Children: A Multicenter National Study. Gastroenterol. Res. Pract. 2016, 2016, 7403129. [Google Scholar] [CrossRef] [Green Version]
- Yap, J.; Wesley, A.; Mouat, S.; Chin, S. Paediatric inflammatory bowel disease in New Zealand. N. Z. Med. J. 2008, 121, 17. [Google Scholar]
- El Mouzan, M.; Al Saleem, B.; Hasosah, M.; Al-Hussaini, A.; Al Anazi, A.; Saadah, O.; Al Sarkhy, A.; Al Mofarreh, M.; Assiri, A. Diagnostic delay of pediatric inflammatory bowel disease in Saudi Arabia. Saudi J. Gastroenterol. 2019, 25, 257. [Google Scholar] [CrossRef]
- Stamm, R.; Aluzaite, K.; Arnold, M.; Caspritz, T.; White, C.; Schultz, M. Challenges for the future: The gastroenterology specialist workforce in New Zealand. N. Z. Med. J. 2020, 133, 9. [Google Scholar]
- Basu, A.; Ghosh, D.; Mandal, B.; Mukherjee, P.; Maji, A. Barriers and explanatory mechanisms in diagnostic delay in four cancers—A health-care disparity? South Asian J Cancer 2019, 8, 221–225. [Google Scholar] [CrossRef]
- Walton, L.; McNeill, R.; Stevens, W.; Murray, M.; Lewis, C.; Aitken, D.; Garrett, J. Patient perceptions of barriers to the early diagnosis of lung cancer and advice for health service improvement. Fam Pract. 2013, 30, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.Q.; Jiang, D.; Hoffman, S.N.; Guntaka, S.; Mays, J.L.; Wang, A.; Gomes, J.; Sorrentino, D. Impact of Diagnostic Delay and Associated Factors on Clinical Outcomes in a U.S. Inflammatory Bowel Disease Cohort: Inflamm. Bowel Dis. 2017, 23, 1825–1831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaharie, R.; Tantau, A.; Zaharie, F.; Tantau, M.; Gheorghe, L.; Gheorghe, C.; Gologan, S.; Cijevschi, C.; Trifan, A.; Dobru, D.; et al. Diagnostic Delay in Romanian Patients with Inflammatory Bowel Disease: Risk Factors and Impact on the Disease Course and Need for Surgery. J. Crohn’s Colitis 2016, 10, 306–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vavricka, S.R.; Spigaglia, S.M.; Rogler, G.; Pittet, V.; Michetti, P.; Felley, C.; Mottet, C.; Braegger, C.P.; Rogler, D.; Straumann, A.; et al. Systematic evaluation of risk factors for diagnostic delay in inflammatory bowel disease: Inflamm. Bowel Dis. 2012, 18, 496–505. [Google Scholar] [CrossRef]
- Nahon, S.; Lahmek, P.; Lesgourgues, B.; Poupardin, C.; Chaussade, S.; Peyrin-Biroulet, L.; Abitbol, V. Diagnostic delay in a French cohort of Crohn’s disease patients. J. Crohn’s Colitis 2014, 8, 964–969. [Google Scholar] [CrossRef] [Green Version]
- Maconi, G.; Orlandini, L.; Asthana, A.K.; Sciurti, R.; Furfaro, F.; Bezzio, C.; de Franchis, R. The impact of symptoms, irritable bowel syndrome pattern and diagnostic investigations on the diagnostic delay of Crohn’s disease: A prospective study. Dig. Liver Dis. 2015, 47, 646–651. [Google Scholar] [CrossRef]
- Li, Y.; Ren, J.; Wang, G.; Gu, G.; Wu, X.; Ren, H.; Hong, Z.; Hu, D.; Wu, Q.; Li, G.; et al. Diagnostic delay in Crohn’s disease is associated with increased rate of abdominal surgery: A retrospective study in Chinese patients. Dig. Liver Dis. 2015, 47, 544–548. [Google Scholar] [CrossRef]
- Cantoro, L.; Di Sabatino, A.; Papi, C.; Margagnoni, G.; Ardizzone, S.; Giuffrida, P.; Giannarelli, D.; Massari, A.; Monterubbianesi, R.; Lenti, M.V.; et al. The Time Course of Diagnostic Delay in Inflammatory Bowel Disease Over the Last Sixty Years: An Italian Multicentre Study. J. Crohn’s Colitis 2017, 11, 975–980. [Google Scholar] [CrossRef] [Green Version]
- Car, L.T.; Papachristou, N.; Bull, A.; Majeed, A.; Gallagher, J.; El-Khatib, M.; Aylin, P.; Rudan, I.; Atun, R.; Car, J.; et al. Clinician-identified problems and solutions for delayed diagnosis in primary care: A PRIORITIZE study. BMC Fam Pract. 2016, 17, 131. [Google Scholar] [CrossRef]
- HealthPathways. Available online: https://healthpathwaysglobal.org/ (accessed on 25 May 2021).

| Patient Characteristics | % (n) |
|---|---|
| Age at the time of the study, years | |
| Median (IQR) | 22 (15–28) |
| Range | 8–72 |
| Time since diagnosis *, years | |
| Median (IQR) | 9.5 (4–12) |
| Range | 0–59 |
| Age at diagnosis, years | |
| Median (IQR) | 12 (10–15) |
| Range | 0–17 years |
| Sex, male | 47 (17/36) |
| Ethnicity | |
| NZ European ** | 94 (33/35) |
| Asian | 3 (1/35) |
| MELAA (Middle Eastern/Latin American/African) | 3 (1/35) |
| Mixed Māori and European | 6 (2/33) |
| Diagnosis | |
| Crohn’s disease | 71 (25/35) |
| Ulcerative Colitis | 29 (10/35) |
| Parent/caregiver characteristics | % (n) |
| Ethnicity | |
| NZ European | 89 (25/28) |
| Other European | 7 (2/28) |
| MELAA (Middle Eastern/Latin American/African) | 4 (1/28) |
| Highest level of education in the household (at the time of diagnosis) | |
| High school or less | 18 (5/28) |
| Apprenticeship or advanced | 54 (15/28) |
| University degree | 29 (8/28) |
| Employment (at the time of diagnosis) | |
| Both employed | 3 (10/28) |
| One employed | 25 (7/28) |
| None employed | 0 (0/28) |
| At least one employed (only info from one parent) | 39 (11/28) |
| Income *** (at the time of diagnosis) | |
| Below average | 21 (6/28) |
| Middle | 54 (15/28) |
| Above average | 25 (7/28) |
| Question | % (n) |
|---|---|
| What were your initial symptoms? (multiple choices possible) | |
| Abdominal pain | 74 (26/35) |
| Diarrhoea | 69 (24/35) |
| Tiredness | 63 (22/35) |
| Blood in stool | 60 (21/35) |
| Weight loss | 54 (19/35) |
| Nausea | 26 (9/35) |
| Vomiting | 23 (8/35) |
| Pus in stool | 11 (4/35) |
| Constipation | 9 (3/35) |
| Fever | 6 (2/35) |
| How long after you first noticed symptoms did you tell someone? | |
| Less than a week | 18 (6/33) |
| 1 week to less than 1 month | 24 (8/33) |
| 1 month to less than 2 months | 15 (5/33) |
| 2 months to less than 1 years | 15 (5/33) |
| More than 1 year | 9 (3/33) |
| Do not know/ remember | 18 (6/33) |
| Who did you tell first about the symptoms? | |
| Parent/caregiver | 85 (28/33) |
| GP/family doctor | 6 (2/33) |
| Other—parents/caregivers noticed/the patient was an infant | 9 (3/33) |
| Which healthcare professional did you see first? | |
| GP/family doctor | 85 (28/33) |
| Multiple | 3 (1/33) |
| Emergency Department | 3 (1/33) |
| Do not know/remember | 9 (3/33) |
| Overall experience of the diagnostic process: | |
| Very good | 12 (4/33) |
| Good | 9 (3/33) |
| Neither good nor bad | 30 (10/33) |
| Bad | 24 (8/33) |
| Very bad | 9 (3/33) |
| Do not know/ remember | 15 (5/33) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khalilipour, B.S.; Day, A.S.; Kenrick, K.; Schultz, M.; Aluzaite, K. Diagnostic Delay in Paediatric Inflammatory Bowel Disease—A Systematic Investigation. J. Clin. Med. 2022, 11, 4161. https://doi.org/10.3390/jcm11144161
Khalilipour BS, Day AS, Kenrick K, Schultz M, Aluzaite K. Diagnostic Delay in Paediatric Inflammatory Bowel Disease—A Systematic Investigation. Journal of Clinical Medicine. 2022; 11(14):4161. https://doi.org/10.3390/jcm11144161
Chicago/Turabian StyleKhalilipour, Bahareh Sophia, Andrew S. Day, Kristin Kenrick, Michael Schultz, and Kristina Aluzaite. 2022. "Diagnostic Delay in Paediatric Inflammatory Bowel Disease—A Systematic Investigation" Journal of Clinical Medicine 11, no. 14: 4161. https://doi.org/10.3390/jcm11144161