
Guilt Feelings in Obsessive Compulsive Disorder: An Investigation between Diagnostic Groups

 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Participants
3. Measures
3.1. Obsessive-Compulsive Inventory Revised (OCI-R)
3.2. The Beck Depression Inventory II
3.3. Statistical Analysis
4. Results
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Item | Subscale |
|---|---|
| 5. I feel guilty if do not respect the figures that, to me, represent authority | MNV |
| 6. “First comes duty and then pleasure” | MNV |
| 7. When I disrespect the authority, I try to get back in line | MNV |
| 9. If I do not conform to society rules, I feel guilty | MNV |
| 14. I feel guilty if I act against nature | MNV |
| 15. I am careful not to violate moral norms | MNV |
| 2. When I see a beggar, I feel guilty because my condition is better than his/her | Empathy |
| 10. When I see someone suffering, I feel pain for him/her | Empathy |
| 13. I tend to feel guilty if I do not help who is suffering | Empathy |
| 16. I feel discomfort if I think there is someone who is worse off than me | Empathy |
| 17. I feel guilty if I do not treat others equitably | Empathy |
| 1. When I feel guilty, I feel dirty inside | MODI |
| 8. When I think about my mistakes, I feel myself a bad person | MODI |
| 12. When I have a dirty conscience, I feel the need to wash myself | MODI |
| 3. If I hurt someone, I try to soothe her suffering | Harm |
| 4. I feel guilty if I hurt someone who is dear to me | Harm |
| 11. If I hurt someone, I feel guilty for the harm I caused | Harm |
References
- Mancini, F.; Gangemi, A. Deontological and Altruistic Guilt Feelings: A Dualistic Thesis. Front. Psychol. 2021, 12, 2118. [Google Scholar] [CrossRef] [PubMed]
- Mancini, A.; Granziol, U.; Migliorati, D.; Gragnani, A.; Femia, G.; Cosentino, T.; Saliani, A.M.; Tenore, K.; Luppino, O.I.; Perdighe, C.; et al. Moral Orientation Guilt Scale (MOGS): Development and Validation of a Novel Guilt Measurement. Pers. Individ. Dif. 2022, 189, 111495. [Google Scholar] [CrossRef]
- Prinz, J.J.; Nichols, S. Moral Emotions. In The Moral Psychology Handbook; Doris, J.M., Ed.; Oxford University Press: Oxford, UK, 2010. [Google Scholar]
- Kohlberg, L. The Philosophy of Moral Development: Moral Stages and the Idea of Justice; Harper & Row: Manhattan, NY, USA, 1981. [Google Scholar]
- Gilligan, C. In a Different Voice: Psychological Theory and Women’s Development; Harvard University Press: Cambridge, MA, USA, 1982. [Google Scholar]
- Tangney, J.P.; Burggraf, S.A.; Wagner, P.E. Shame-Proneness, Guilt-Proneness, and Psychological Symptoms. In Self-Conscious Emotions: The Psychology of Shame, Guilt, Embarrassment, and Pride; Tangney, J.P., Fischer, K.W., Eds.; Guilford Press: New York, NY, USA, 1995; pp. 343–367. [Google Scholar]
- Jung, C.G. Adaptation, Individuation, Collectivity. In West Kirby School and College; West Kirby School and College: West Kirby, UK, 1916. [Google Scholar]
- Brooke, R. Jung and the Phenomenology of Guilt. J. Anal. Psychol. 1985, 30, 165–184. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.G. Aion; Researches into the Phenomenology of the Self; Princeton University Press: Princeton, NJ, USA, 1959. [Google Scholar]
- Barcaccia, B.; Mancini, F. Teoria e Clinica Del Perdono; Raffaello Cortina Editore: Milano, Italy, 2013. [Google Scholar]
- Freud, S. Hysterie Und Angst. Hemmung, Symp- Tom Und Angst. Studienausgabe. Volume VI; Fischer: Frankfurt am Main, Germany, 1992. [Google Scholar]
- Geissner, E.; Knechtl, L.M.; Baumert, A.; Rothmund, T.; Schmitt, M. Schulderleben bei Zwangspatienten. Verhaltenstherapie 2020, 30, 246–255. [Google Scholar] [CrossRef]
- Gangemi, A.; Mancini, F. Obsessive Patients and Deontological Guilt: A Review. Psychopathol. Rev. 2017, a4, 155–168. [Google Scholar] [CrossRef]
- Kang, L.L.; Rowatt, W.C.; Fergus, T.A. Moral Foundations and Obsessive-Compulsive Symptoms: A Preliminary Examination. J. Obsessive. Compuls. Relat. Disord. 2016, 11, 22–30. [Google Scholar] [CrossRef]
- Sunstein, C.R. Moral Heuristics. Behav. Brain Sci. 2005, 28, 531–541. [Google Scholar] [CrossRef]
- Mancini, F.; Gangemi, A. Deontological Guilt and Obsessive Compulsive Disorder. J. Behav. Ther. Exp. Psychiatry 2015, 49, 157–163. [Google Scholar] [CrossRef]
- Mancini, A.; Mancini, F. Do Not Play God: Contrasting Effects of Deontological Guilt and Pride on Decision-Making. Front. Psychol. 2015, 6, 1251. [Google Scholar] [CrossRef]
- Franklin, S.A.; McNally, R.J.; Riemann, B.C. Moral Reasoning in Obsessive-Compulsive Disorder. J. Anxiety Disord. 2009, 23, 575–577. [Google Scholar] [CrossRef]
- Basile, B.; Mancini, F.; Macaluso, E.; Caltagirone, C.; Bozzali, M. Abnormal Processing of Deontological Guilt in Obsessive-Compulsive Disorder. Brain Struct. Funct. 2014, 219, 1321–1331. [Google Scholar] [CrossRef] [PubMed]
- Rauch, S.L.; Dougherty, D.D.; Shin, L.M.; Alpert, N.M.; Manzo, P.; Leahy, L.; Fischman, A.J.; Jenike, M.A.; Baer, L. Neural Correlates of Factor-Analyzed OCD Symptom Dimensions: A PET Study. CNS Spectr. 1998, 3, 37–43. [Google Scholar] [CrossRef]
- Mataix-Cols, D.; do Rosario-Campos, M.C.; Leckman, J.F. A Multidimensional Model of Obsessive-Compulsive Disorder. Am. J. Psychiatry 2005, 162, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Basile, B.; Mancini, F.; Macaluso, E.; Caltagirone, C.; Frackowiak, R.S.J.; Bozzali, M. Deontological and Altruistic Guilt: Evidence for Distinct Neurobiological Substrates. Hum. Brain Mapp. 2011, 32, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Rozin, P.; Haidt, J.; McCauley, C.R. Disgust. In Handbook of Emotions; Lewis, M., Haviland-Jones, J., Eds.; Guilford Press: New York, NY, USA, 2000; pp. 637–653. [Google Scholar]
- Moll, J.; De Oliveira-Souza, R.; Garrido, G.J.; Bramati, I.E.; Caparelli-Daquer, E.; Paiva, M.L.M.F.; Zahn, R.; Grafman, J.H. The Self as a Moral Agent: Linking the Neural Bases of Social Agency and Moral Sensitivity. Soc. Neurosci. 2007, 2, 336–352. [Google Scholar] [CrossRef]
- Zahn-Waxler, C.; Van Hulle, C. Empathy, Guilt, and Depression: When Caring for Others Becomes Costly to Children. In Pathological Altruism; Oakley, B., Knafo, A., Madhavan, G., Wilson, D.S., Eds.; Oxford University Press: Oxford, UK, 2012; pp. 321–344. [Google Scholar]
- Tone, E.B.; Tully, E.C. Empathy as a “Risky Strength”: A Multilevel Examination of Empathy and Risk for Internalizing Disorders. Dev. Psychopathol. 2014, 26 4 Pt 2, 1547–1565. [Google Scholar] [CrossRef]
- O’Connor, L.E.; Berry, J.W.; Weiss, J.; Gilbert, P. Guilt, Fear, Submission, and Empathy in Depression. J. Affect. Disord. 2002, 71, 19–27. [Google Scholar] [CrossRef]
- O’Connor, L.E.; Berry, J.W.; Lewis, T.B.; Stiver, D.J. Empathy-Based Pathogenic Guilt, Pathological Altruism, and Psychopathology. Pathol. Altruism 2012, 10, 10–30. [Google Scholar]
- Pulcu, E.; Lythe, K.; Elliott, R.; Green, S.; Moll, J.; Deakin, J.F.W.; Zahn, R. Increased Amygdala Response to Shame in Remitted Major Depressive Disorder. PLoS ONE 2014, 9, e86900. [Google Scholar] [CrossRef]
- Sica, C.; Ghisi, M.; Altoè, G.; Chiri, L.R.; Franceschini, S.; Coradeschi, D.; Melli, G. The Italian Version of the Obsessive Compulsive Inventory: Its Psychometric Properties on Community and Clinical Samples. J. Anxiety Disord. 2009, 23, 204–211. [Google Scholar] [CrossRef]
- Marchetti, I.; Chiri, L.R.; Ghisi, M.; Sica, C. Obsessive-Compulsive Inventory-Revised (OCI-R): Presentazione e Indicazioni Di Utilizzo Nel Contesto Italiano. Psicoter. Cogn. Comport. 2010, 16, 69–84. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Beck Depression Inventory (BDI-II); Pearson: London, UK, 1996; Volume 10. [Google Scholar]
- Sica, C.; Ghisi, M. The Italian Versions of the Beck Anxiety Inventory and the Beck Depression Inventory-II: Psychometric Properties and Discriminant Power. In Leading-Edge Psychological Tests and Testing Research; Nova Science Publishers: Hauppauge, NY, USA, 2007. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Zhang, Z. Multiple Imputation with Multivariate Imputation by Chained Equation (MICE) Package. Ann. Transl. Med. 2016, 4, 30. [Google Scholar] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Erlbaum: Hillsdale, NJ, USA, 1998. [Google Scholar]
- Ben-Shachar, M.; Lüdecke, D.; Makowski, D. Effectsize: Estimation of Effect Size Indices and Standardized Parameters. J. Open Source Softw. 2020, 5, 2815. [Google Scholar] [CrossRef]
- Funder, D.C.; Ozer, D.J. Evaluating Effect Size in Psychological Research: Sense and Nonsense. Adv. Methods Pract. Psychol. Sci. 2019, 2, 156–168. [Google Scholar] [CrossRef]
- Long, J.A. Interactions: Comprehensive, User-Friendly Toolkit for Probing Interactions; R Package Version 1.1.0; MIT: Cambridge, MA, USA, 2019. [Google Scholar]
- Neubauer, A.C.; Fink, A. Intelligence and Neural Efficiency. Neurosci. Biobehav. Rev. 2009, 33, 1004–1023. [Google Scholar] [CrossRef]
- Basile, B.; Luppino, O.I.; Mancini, F.; Tenore, K. A Theoretical Integration of Schema Therapy and Cognitive Therapy in OCD Treatment: Experiential Techniques and Cognitive-Based Interventions in Action (Part III). Psychology 2018, 9, 2296. [Google Scholar] [CrossRef][Green Version]
- Basile, B.; De Sanctis, B.; Fadda, S.; Luppino, O.I.; Perdighe, C.; Saliani, A.M.; Tenore, K.; Mancini, F. Early Life Experiences in OCD and Other Disorders: A Retrospective Observational Study Using Imagery with Re-Scripting. Clin. Neuropsychiatry J. Treat. Eval. 2018, 15, 299–305. [Google Scholar]
- Tenore, K.; Basile, B. Vulnerability in Obsessive-Compulsive Disorder. In The Obsessive Mind; Routledge: London, UK, 2018; pp. 133–148. [Google Scholar]
- Luppino, O.I.; Tenore, K.; Mancini, F.; Basile, B. A Theoretical Integration of Schema Therapy and Cognitive Therapy in OCD Treatment: Goals and Beliefs of the Obsessive Mind (Part I). Psychology 2018, 9, 2261. [Google Scholar] [CrossRef][Green Version]
- Tenore, K.; Basile, B.; Cosentino, T.; De Sanctis, B.; Fadda, S.; Femia, G.; Gragnani, A.; Luppino, O.I.; Pellegrini, V.; Perdighe, C.; et al. Imagery Rescripting on Guilt-Inducing Memories in OCD: A Single Case Series Study. Front. Psychiatry 2020, 11, 1018. [Google Scholar] [CrossRef]



| n = 68 | Frequency (%) | Missingness (%) |
|---|---|---|
| Gender | 0% | |
| Females Males | 45.59% 54.41% | |
| Diagnosis | ||
| OCD | 48.53% | |
| Non-OCD | ||
| Anxiety spectrum | 16.18% | |
| Mood spectrum | 35.29% | |
| Measures | M (SD) | |
| Moral Orientation Guilt Scale | ||
| Moral Norm Violation | 17.03 (5.73) | 0% |
| OCD | 19.30 (5.84) | 0% |
| Non-OCD | 14.89 (4.78) | 0% |
| Empathy | 14.07 (3.99) | 0% |
| OCD | 14.30 (4.21) | 0% |
| Non-OCD | 13.86 (3.82) | 0% |
| MOral DIrtiness | 8.23 (3.49) | 0% |
| OCD | 9.18 (2.88) | 0% |
| Non-OCD | 7.34 (3.82) | 0% |
| Harm | 12.78 (4.25) | 0% |
| OCD | 12.72 (2.33) | 0% |
| Non-OCD | 12.83 (5.52) | 0% |
| Obsessive-Compulsive Inventory Revised | ||
| Total score | 22.82 (14.98) | 27.94% |
| OCD | 29.82 (14.96) | 26.32% * |
| Non-OCD | 13.48 (8.70) | 73.68% |
| Beck Depression Inventory | ||
| Factor 1 (cognitive) | 10.90 (6.76) | 16.18% |
| OCD | 11.63 (7.50) | 60% |
| Non-OCD | 10.26 (6.09) | 40% |
| Factor 2 (affective and somatic) | 9.40) | 14.71% |
| OCD | 10.63 (7.01) | 54.54% |
| Non-OCD | 8.87 (11.18) | 45.46% |
| DV | Predictor | β | Std.Er | t Value | P | D | CI.L | CI.U |
|---|---|---|---|---|---|---|---|---|
| Moral Norm Violation | Group | 4.42 | 1.29 | 3.42 | <0.001 | 0.84 | 0.34 | 1.34 |
| Moral Dirtiness | Group | 1.84 | 0.82 | 2.23 | 0.03 | 0.55 | 0.06 | 1.04 |
| Empathy | Group | 0.45 | 0.97 | 0.46 | 0.65 | 0.11 | −0.37 | 0.6 |
| Harm | Group | 0.45 | 0.97 | 0.46 | 0.65 | 0.11 | −0.37 | 0.6 |
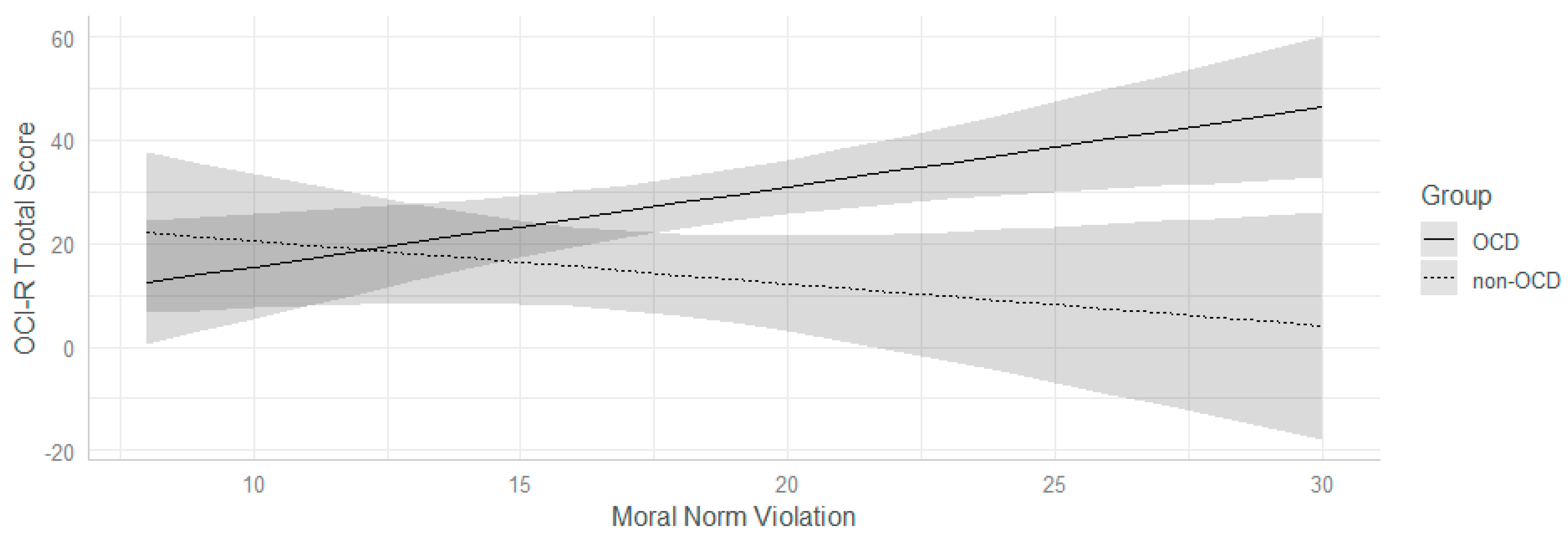
| OCI-R_Tot | Moral Norm Violation | −0.56 | 0.47 | −1.18 | 0.24 | −0.31 | −0.83 | 0.21 |
| Group | 7.58 | 15.02 | 0.5 | 0.62 | 0.13 | −0.38 | 0.65 | |
| Moral Dirtiness | 2.64 | 0.75 | 3.5 | <0.001 | 0.92 | 0.37 | 1.46 | |
| Empathy | 0.86 | 0.55 | 1.55 | 0.13 | 0.41 | −0.11 | 0.93 | |
| Harm | −1.13 | 0.56 | −2.04 | 0.06 | −0.54 | −1.06 | −0.01 | |
| Moral Norm Violation: Group | 1.94 | 0.66 | 2.94 | <0.01 | 0.77 | 0.24 | 1.3 | |
| Group: Moral Dirtiness | −1.11 | 1.11 | −1 | 0.32 | −0.26 | −0.78 | 0.26 | |
| Group: Empathy | −0.51 | 0.79 | −0.65 | 0.52 | −0.17 | −0.68 | 0.35 | |
| Group: Harm | −1.39 | 1.21 | −1.15 | 0.26 | −0.3 | −0.82 | 0.22 | |
| BDI_Factor 1 | Moral Norm Violation | 0.08 | 0.3 | 0.27 | 0.79 | 0.07 | −0.44 | 0.59 |
| Group | −8.32 | 9.64 | −0.86 | 0.39 | −0.23 | −0.74 | 0.29 | |
| Moral Dirtiness | 0.49 | 0.48 | 1.02 | 0.31 | 0.27 | −0.25 | 0.78 | |
| Empathy | −0.03 | 0.36 | −0.08 | 0.93 | −0.02 | −0.54 | 0.49 | |
| Harm | 0.15 | 0.36 | 0.42 | 0.68 | 0.11 | −0.41 | 0.62 | |
| Moral Norm Violation:Group | 0.3 | 0.42 | 0.71 | 0.48 | 0.19 | −0.33 | 0.7 | |
| Group: Moral Dirtiness | −0.02 | 0.72 | −0.02 | 0.98 | −0.01 | −0.52 | 0.51 | |
| Group: Empathy | 0.32 | 0.51 | 0.63 | 0.53 | 0.16 | −0.35 | 0.68 | |
| Group: Harm | −0.21 | 0.78 | −0.27 | 0.79 | −0.07 | −0.59 | 0.44 | |
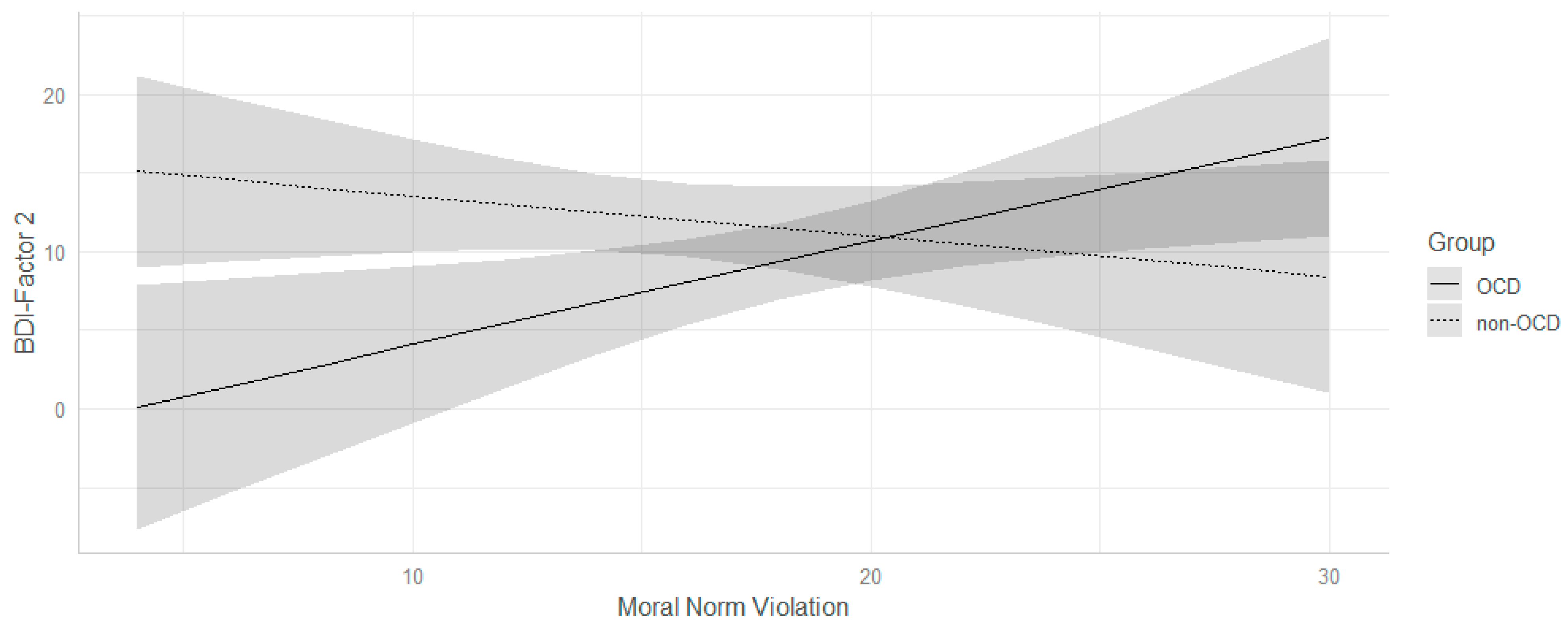
| BDI_Factor 2 | Moral Norm Violation | −0.46 | 0.28 | −1.6 | 0.11 | −0.42 | −0.94 | 0.1 |
| Group | 6.71 | 9.03 | 0.74 | 0.46 | 0.2 | −0.32 | 0.71 | |
| Moral Dirtiness | 1.86 | 0.45 | 4.09 | <0.001 | 1.07 | 0.52 | 1.62 | |
| Empathy | 0 | 0.33 | −0.01 | 0.99 | 0 | −0.52 | 0.51 | |
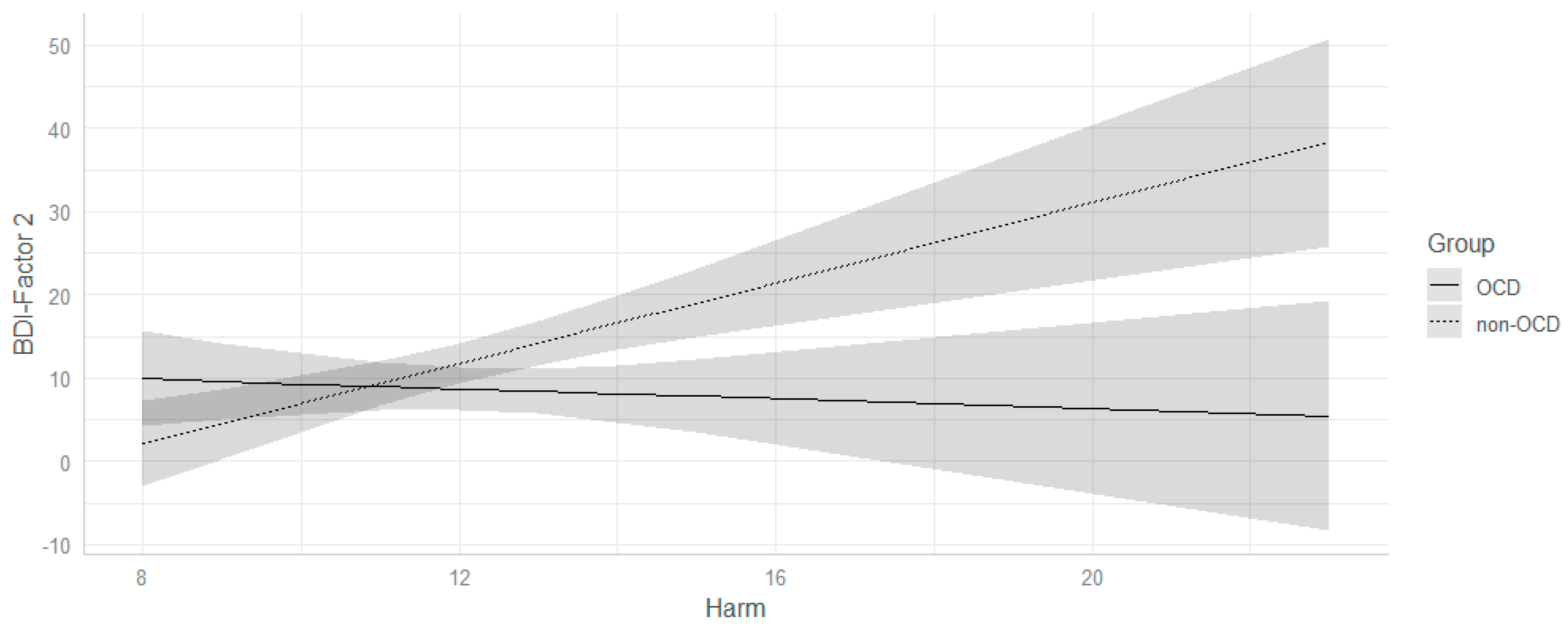
| Harm | 1.15 | 0.33 | 3.45 | <0.001 | 0.9 | 0.36 | 1.44 | |
| Moral Norm Violation: Group | 1.02 | 0.4 | 2.59 | 0.01 | 0.68 | 0.15 | 1.21 | |
| Group:Moral Dirtiness | −1.27 | 0.67 | −1.9 | 0.06 | −0.5 | −1.02 | 0.03 | |
| Group: Empathy | 0.44 | 0.47 | 0.92 | 0.36 | 0.24 | −0.28 | 0.76 | |
| Group: Harm | −1.87 | 0.73 | −2.56 | 0.01 | −0.67 | −1.2 | −0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mancini, A.; Granziol, U.; Gragnani, A.; Femia, G.; Migliorati, D.; Cosentino, T.; Luppino, O.I.; Perdighe, C.; Saliani, A.M.; Tenore, K.; et al. Guilt Feelings in Obsessive Compulsive Disorder: An Investigation between Diagnostic Groups. J. Clin. Med. 2022, 11, 4673. https://doi.org/10.3390/jcm11164673
Mancini A, Granziol U, Gragnani A, Femia G, Migliorati D, Cosentino T, Luppino OI, Perdighe C, Saliani AM, Tenore K, et al. Guilt Feelings in Obsessive Compulsive Disorder: An Investigation between Diagnostic Groups. Journal of Clinical Medicine. 2022; 11(16):4673. https://doi.org/10.3390/jcm11164673
Chicago/Turabian StyleMancini, Alessandra, Umberto Granziol, Andrea Gragnani, Giuseppe Femia, Daniele Migliorati, Teresa Cosentino, Olga Ines Luppino, Claudia Perdighe, Angelo Maria Saliani, Katia Tenore, and et al. 2022. "Guilt Feelings in Obsessive Compulsive Disorder: An Investigation between Diagnostic Groups" Journal of Clinical Medicine 11, no. 16: 4673. https://doi.org/10.3390/jcm11164673
APA StyleMancini, A., Granziol, U., Gragnani, A., Femia, G., Migliorati, D., Cosentino, T., Luppino, O. I., Perdighe, C., Saliani, A. M., Tenore, K., & Mancini, F. (2022). Guilt Feelings in Obsessive Compulsive Disorder: An Investigation between Diagnostic Groups. Journal of Clinical Medicine, 11(16), 4673. https://doi.org/10.3390/jcm11164673