
Evaluating the Medication Regimen Complexity Score as a Predictor of Clinical Outcomes in the Critically Ill

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Inclusion and Exclusion Criteria
2.4. Variables
2.5. Data Sources
MRC Scoring Tools
2.6. Definitions
2.7. Statistical Analysis
2.8. Prediction Model Development
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Clinical Characteristics between MRC Cohorts
3.2.1. Low- and High-MRC Cohorts
3.2.2. Survivor and Non-Survivor Cohorts
3.3. Medication Use
3.4. Associations between MRC Scores and Clinical Outcomes
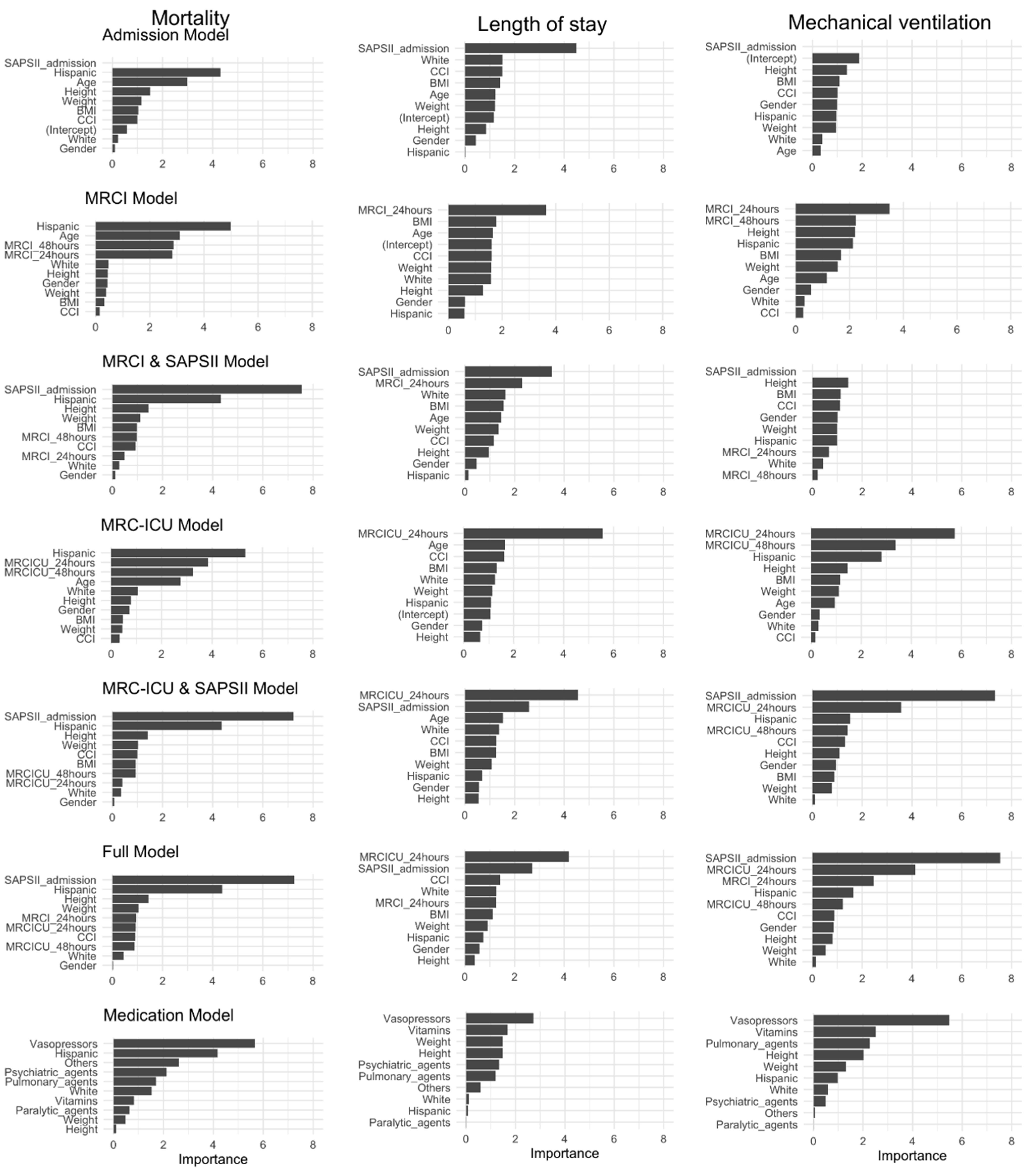
3.5. Role of MRC Scores in the Prediction of Clinical Outcomes
4. Discussion
4.1. Clinical Characteristics between MRC and Survivor Cohorts
4.2. Associations between MRC Scores and Clinical Outcomes
4.3. Medication Use as Predictor of Clinical Outcomes
4.4. Implications of These Findings
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- George, J.; Phun, Y.-T.; Bailey, M.J.; Kong, D.C.; Stewart, K. Development and Validation of the Medication Regimen Complexity Index. Ann. Pharmacother. 2004, 38, 1369–1376. [Google Scholar] [CrossRef]
- Masnoon, N.; Shakib, S.; Kalisch-Ellett, L.; Caughey, G.E. What is polypharmacy? A systematic review of definitions. BMC Geriatrics 2017, 17, 230. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, S.S.; Shati, M.; Keshtkar, A.; Malakouti, S.K.; Bazargan, M.; Assari, S. Defining polypharmacy in the elderly: A systematic review protocol. BMJ Open 2016, 6, e010989. [Google Scholar] [CrossRef]
- Pazan, F.; Wehling, M. Polypharmacy in older adults: A narrative review of definitions, epidemiology and consequences. Eur. Geriatr. Med. 2021, 12, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Paquin, A.M.; Zimmerman, K.M.; Kostas, T.R.; Pelletier, L.; Hwang, A.; Simone, M.; Skarf, L.M.; Rudolph, J.L. Complexity perplexity: A systematic review to describe the measurement of medication regimen complexity. Expert Opin. Drug Saf. 2013, 12, 829–840. [Google Scholar] [CrossRef]
- Alves-Conceição, V.; Rocha, K.S.S.; Silva, F.V.N.; Silva, R.O.S.; Da Silva, D.T.; De Lyra, D.P., Jr. Medication Regimen Complexity Measured by MRCI: A Systematic Review to Identify Health Outcomes. Ann. Pharmacother. 2018, 52, 1117–1134. [Google Scholar] [CrossRef] [PubMed]
- Wimmer, B.C.; Cross, A.J.; Jokanovic, N.; Wiese, M.D.; George, J.; Johnell, K.; Diug, B.; Bell, J.S. Clinical Outcomes Associated with Medication Regimen Complexity in Older People: A Systematic Review. J. Am. Geriatr. Soc. 2017, 65, 747–753. [Google Scholar] [CrossRef] [PubMed]
- Brysch, E.G.; Cauthon, K.A.B.; Kalich, B.A.; Sarbacker, G.B. Medication Regimen Complexity Index in the Elderly in an Outpatient Setting: A Literature Review. Consult. Pharm. 2018, 33, 484–496. [Google Scholar] [CrossRef]
- Wurmbach, V.S.; Schmidt, S.J.; Lampert, A.; Bernard, S.; Meid, A.D.; Frick, E.; Metzner, M.; Wilm, S.; Mortsiefer, A.; Bücker, B.; et al. Prevalence and patient-rated relevance of complexity factors in medication regimens of community-dwelling patients with polypharmacy. Eur. J. Clin. Pharmacol. 2022, 78, 1127–1136. [Google Scholar] [CrossRef]
- Pichala, P.T.; Kumar, B.M.; Zachariah, S.; Thomas, D.; Saunchez, L.; Gerardo, A.-U. An interventional study on intensive care unit drug therapy assessment in a rural district hospital in India. J. Basic Clin. Pharm. 2013, 4, 64. [Google Scholar] [CrossRef]
- Moyen, E.; Camiré, E.; Stelfox, H.T. Clinical review: Medication errors in critical care. Crit. Care 2008, 12, 208. [Google Scholar] [CrossRef] [PubMed]
- SCCM. Standard Medication Concentrations: An Opportunity to Reduce Medication Errors. Available online: https://www.sccm.org/Communications/Critical-Connections/Archives/2019/Standard-Medication-Concentrations-An-Opportunity (accessed on 9 December 2021).
- Krska, J.; Corlett, S.A.; Katusiime, B. Complexity of Medicine Regimens and Patient Perception of Medicine Burden. Pharm. J. Pharm. Educ. Pract. 2019, 7, 18. [Google Scholar] [CrossRef] [PubMed]
- Abou-Karam, N.; Bradford, C.; Lor, K.B.; Barnett, M.; Ha, M.; Rizos, A. Medication regimen complexity and readmissions after hospitalization for heart failure, acute myocardial infarction, pneumonia, and chronic obstructive pulmonary disease. SAGE Open Med. 2016, 4, 205031211663242. [Google Scholar] [CrossRef] [PubMed]
- Colavecchia, A.C.; Putney, D.R.; Johnson, M.L.; Aparasu, R.R. Discharge medication complexity and 30-day heart failure readmissions. Res. Soc. Adm. Pharm. 2017, 13, 857–863. [Google Scholar] [CrossRef] [PubMed]
- Willson, M.N.; Greer, C.L.; Weeks, D.L. Medication regimen complexity and hospital readmission for an adverse drug event. Ann. Pharmacother. 2014, 48, 26–32. [Google Scholar] [CrossRef]
- Lee, S.; Jang, J.Y.; Yang, S.; Hahn, J.; Min, K.L.; Jung, E.H.; Oh, K.S.; Cho, R.; Chang, M.J. Development and validation of the Korean version of the medication regimen complexity index. PLoS ONE 2019, 14, e0216805. [Google Scholar] [CrossRef]
- Ghimire, S.; Castelino, R.L.; Lioufas, N.M.; Peterson, G.M.; Zaidi, S.T.R. Nonadherence to Medication Therapy in Haemodialysis Patients: A Systematic Review. PLoS ONE 2015, 10, e0144119. [Google Scholar] [CrossRef]
- Marienne, J.; Laville, S.M.; Caillard, P.; Batteux, B.; Gras-Champel, V.; Masmoudi, K.; Choukroun, G.; Liabeuf, S. Evaluation of Changes Over Time in the Drug Burden and Medication Regimen Complexity in ESRD Patients Before and After Renal Transplantation. Kidney Int. Rep. 2021, 6, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Tesfaye, W.H.; Peterson, G.M.; Castelino, R.L.; McKercher, C.; Jose, M.D.; Wimmer, B.C.; Zaidi, S.T.R. Medication Regimen Complexity and Hospital Readmission in Older Adults with Chronic Kidney Disease. Ann. Pharmacother. 2019, 53, 28–34. [Google Scholar] [CrossRef]
- Ayele, A.A.; Tegegn, H.G.; Ayele, T.A.; Ayalew, M.B. Medication regimen complexity and its impact on medication adherence and glycemic control among patients with type 2 diabetes mellitus in an Ethiopian general hospital. BMJ Open Diabetes Res. Care 2019, 7, e000685. [Google Scholar] [CrossRef]
- Wakai, E.; Ikemura, K.; Kato, C.; Okuda, M. Effect of number of medications and complexity of regimens on medication adherence and blood pressure management in hospitalized patients with hypertension. PLoS ONE 2021, 16, e0252944. [Google Scholar] [CrossRef] [PubMed]
- Ab Rahman, N.; Lim, M.T.; Thevendran, S.; Ahmad Hamdi, N.; Sivasampu, S. Medication Regimen Complexity and Medication Burden Among Patients with Type 2 Diabetes Mellitus: A Retrospective Analysis. Front. Pharmacol. 2022, 13, 808190. [Google Scholar] [CrossRef] [PubMed]
- Federman, A.D.; O’conor, R.; Wolf, M.S.; Wisnivesky, J.P. Associations of Medication Regimen Complexity with COPD Medication Adherence and Control. Int. J. Chron. Obstruct. Pulmon. Dis. 2021, 16, 2385–2392. [Google Scholar] [CrossRef]
- Newsome, A.S.; Anderson, D.; Gwynn, M.E.; Waller, J.L. Characterization of changes in medication complexity using a modified scoring tool. Am. J. Health-Syst. Pharm. 2019, 76, S92–S95. [Google Scholar] [CrossRef]
- Gwynn, M.E.; Poisson, M.O.; Waller, J.L.; Newsome, A.S. Development and validation of a medication regimen complexity scoring tool for critically ill patients. Am. J. Health Syst. Pharm. 2019, 76, S34–S40. [Google Scholar] [CrossRef] [PubMed]
- Newsome, A.S.; Smith, S.E.; Jones, T.W.; Taylor, A.; van Berkel, M.A.; Rabinovich, M. A survey of critical care pharmacists to patient ratios and practice characteristics in intensive care units. J. Am. Coll. Clin. Pharm. 2020, 3, 68–74. [Google Scholar] [CrossRef]
- Newsome, A.S.; Smith, S.E.; Olney, W.J.; Jones, T.W. Multicenter validation of a novel medication-regimen complexity scoring tool. Am. J. Health-Syst. Pharm. 2020, 77, 474–478. [Google Scholar] [CrossRef]
- Al-Mamun, M.A.; Brothers, T.; Newsome, A.S. Development of Machine Learning Models to Validate a Medication Regimen Complexity Scoring Tool for Critically Ill Patients. Ann. Pharmacother. 2021, 55, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Newsome, A.S.; Smith, S.E.; Olney, W.J.; Jones, T.W.; Forehand, C.C.; Jun, A.H.; Coppiano, L. Medication regimen complexity is associated with pharmacist interventions and drug-drug interactions: A use of the novel MRC-ICU scoring tool. J. Am. Coll. Clin. Pharm. 2020, 3, 47–56. [Google Scholar] [CrossRef]
- Ripley, B.D. The R Project in Statistical Computing. Available online: http://www.ltsn.gla.ac.uk/rworkshop.asp (accessed on 14 December 2021).
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 25 April 2020).
- Villanueva, R.A.M.; Chen, Z.J.; Wickham, H. ggplot2, Elegant Graphics for Data Analysis Using the Grammar of Graphics; Springer: New York, NY, USA, 2016. [Google Scholar] [CrossRef]
- Schoonover, H.; Corbett, C.F.; Weeks, D.L.; Willson, M.N.; Setter, S.M. Predicting potential postdischarge adverse drug events and 30-day unplanned hospital readmissions from medication regimen complexity. J. Patient Saf. 2014, 10, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Wimmer, B.C.; Bell, J.S.; Fastbom, J.; Wiese, M.D.; Johnell, K. Medication Regimen Complexity and Number of Medications as Factors Associated with Unplanned Hospitalizations in Older People: A Population-based Cohort Study. J. Gerontol. Ser. A 2016, 71, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Gamble, J.M.; Hall, J.J.; Marrie, T.J.; Sadowski, C.A.; Majumdar, S.R.; Eurich, D.T. Medication transitions and polypharmacy in older adults following acute care. Ther. Clin. Risk Manag. 2014, 10, 189. [Google Scholar] [CrossRef] [PubMed]
- Moitra, V.K.; Guerra, C.; Linde-Zwirble, W.T.; Wunsch, H. Relationship Between ICU Length of Stay and Long-Term Mortality for Elderly ICU Survivors. Crit. Care Med. 2016, 44, 655–662. [Google Scholar] [CrossRef]
- De Corte, W.; Dhondt, A.; Vanholder, R.; de Waele, J.; Decruyenaere, J.; Sergoyne, V.; Vanhalst, J.; Claus, S.; Hoste, E.A.J. Long-term outcome in ICU patients with acute kidney injury treated with renal replacement therapy: A prospective cohort study. Crit. Care 2016, 20, 256. [Google Scholar] [CrossRef]
- Marshall, J.; Finn, C.A.; Theodore, A.C. Impact of a clinical pharmacist-enforced intensive care unit sedation protocol on duration of mechanical ventilation and hospital stay. Crit. Care Med. 2008, 36, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Chertoff, J. Racial disparities in critical care: Experience from the USA. Lancet Respir. Med. 2017, 5, e11–e12. [Google Scholar] [CrossRef]
- Velasco, F.; Yang, D.M.; Zhang, M.; Nelson, T.; Sheffield, T.; Keller, T.; Wang, Y.; Walker, C.; Katterapalli, C.; Zimmerman, K.; et al. Association of Healthcare Access with Intensive Care Unit Utilization and Mortality in Patients of Hispanic Ethnicity Hospitalized With COVID-19. J. Hosp. Med. 2021, 16, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.; Buzon, J.; Kimmoun, A. Inotropes and vasopressors use in cardiogenic shock: When, which and how much? Curr. Opin. Crit. Care 2019, 25, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Chang, M.H.; Miranda-Valdes, Y.; Vest, K.; Kish, T.D. Impact of early home psychotropic medication reinitiation on surrogate measures of intensive care unit delirium. Ment. Health Clin. 2019, 9, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Devlin, J.W.; Skrobik, Y.; Gélinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef]
- Shehabi, Y.; Riker, R.R.; Bokesch, P.M.; Wisemandle, W.; Shintani, A.; Ely, E.W. Delirium duration and mortality in lightly sedated, mechanically ventilated intensive care patients. Crit. Care Med. 2010, 38, 2311–2318. [Google Scholar] [CrossRef] [PubMed]
- Renew, J.R.; Ratzlaff, R.; Hernandez-Torres, V.; Brull, S.J.; Prielipp, R.C. Neuromuscular blockade management in the critically Ill patient. J. Intensive Care 2020, 8, 37. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.J.; Deblock, H.; Erstad, B.; Gray, A.; Jacobi, J.; Jordan, C.; McGee, W.; McManus, C.; Meade, M.; Nix, S.; et al. Clinical Practice Guidelines for Sustained Neuromuscular Blockade in the Adult Critically Ill Patient. Crit. Care Med. 2016, 44, 2079–2103. [Google Scholar] [CrossRef] [PubMed]
- Lat, I.; Paciullo, C.; Daley, M.J.; Maclaren, R.; Bolesta, S.; McCann, J.; Stollings, J.L.; Gross, K.; Foos, S.A.; Roberts, R.J.; et al. Position Paper on Critical Care Pharmacy Services: 2020 Update. Crit. Care Med. 2020, 48, 813–834. [Google Scholar] [CrossRef] [PubMed]
- Newsome, A.S.; Jones, T.W.; Smith, S.E. Pharmacists Are Associated with Reduced Mortality in Critically Ill Patients. Crit. Care Med. 2019, 47, e1036–e1037. [Google Scholar] [CrossRef] [PubMed]
- Maves, R.C.; Downar, J.; Dichter, J.R.; Hick, J.L.; Devereaux, A.; Geiling, J.A.; Kissoon, N.; Hupert, N.; Niven, A.S.; King, M.A.; et al. Triage of Scarce Critical Care Resources in COVID-19 An Implementation Guide for Regional Allocation: An Expert Panel Report of the Task Force for Mass Critical Care and the American College of Chest Physicians. Chest 2020, 158, 212–225. [Google Scholar] [CrossRef] [PubMed]
- Makam, A.N.; Nguyen, O.K.; Auerbach, A.D. Diagnostic accuracy and effectiveness of automated electronic sepsis alert systems: A systematic review. J. Hosp. Med. 2015, 10, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Page, N.; Baysari, M.T.; Westbrook, J.I. A systematic review of the effectiveness of interruptive medication prescribing alerts in hospital CPOE systems to change prescriber behavior and improve patient safety. Int. J. Med. Inform. 2017, 105, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Bright, T.J.; Wong, A.; Dhurjati, R.; Bristow, E.; Bastian, L.; Coeytaux, R.R.; Samsa, G.; Hasselblad, V.; Williams, J.W.; Musty, M.D.; et al. Effect of clinical decision-support systems: A systematic review. Ann. Intern. Med. 2012, 157, 29–43. [Google Scholar] [CrossRef] [PubMed]
- Jaspers, M.W.M.; Smeulers, M.; Vermeulen, H.; Peute, L.W. Effects of clinical decision-support systems on practitioner performance and patient outcomes: A synthesis of high-quality systematic review findings. J. Am. Med. Inform. Assoc. 2011, 18, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Alves-Conceição, V.; Rocha, K.S.S.; Silva, F.V.N.; Silva, R.D.O.S.; Cerqueira-Santos, S.; Nunes, M.A.P.; Martins-Filho, P.R.; Da Silva, D.T.; De Lyra, D.P. Are Clinical Outcomes Associated with Medication Regimen Complexity? A Systematic Review and Meta-analysis. Ann. Pharmacother. 2020, 54, 301–313. [Google Scholar] [CrossRef] [PubMed]
- Falch, C.; Alves, G. Pharmacists’ Role in Older Adults’ Medication Regimen Complexity: A Systematic Review. Int. J. Environ. Res. Public Health. 2021, 18, 8824. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Survivors (n = 243) | Non-Survivors (n = 74) | p-Value |
|---|---|---|---|
| Demographics | |||
| Age, median (IQR), y | 60.8 (48–73.5) | 65.8 (58–76) | 0.81 |
| Sex, No. (%) | |||
| Male | 134 (55) | 41 (55) | >0.99 |
| Race, No. (%) | |||
| White | 163 (67) | 42 (57) | 0.14 |
| Black | 19 (8) | 7 (9) | 0.83 |
| Hispanic | 25 (10) | 12 (16) | 0.24 |
| Asian | 4 (2) | 0 (0) | 0.61 |
| BMI, median (IQR) | 29 (23–32) | 28.5 (23–31.8) | 0.44 |
| Vital Signs | |||
| Systolic blood pressure (mm Hg) | 122.8 (108–133.7) | 107.1 (96.1–118.4) | 0.22 |
| Diastolic blood pressure (mm Hg) | 71.6 (62.3–80.4) | 64.2 (55.4–71.6) | 0.38 |
| Mean arterial pressure (mm Hg) | 88.7 (77.7–97.5) | 78.5 (69.4–86.4) | 0.22 |
| Heart rate (beats/min) | 88.7 (78–99.1) | 99.4 (86.2–113.5) | 0.82 |
| Respiratory rate (breaths/min) | 19.2 (16–21) | 25.2 (21.4–28) | 0.09 |
| Temperature (°C) | 98.2 (97.7–98.7) | 97.8 (96.8–99.2) | 0.74 |
| SaO2 (mm Hg) | 96.7 (95.1–98.7) | 93.9 (92.5–97) | 0.77 |
| Serum Laboratory Values | |||
| Sodium (mEq/L) | 136.3 (134–139) | 138.1 (134.6–143) | 0.58 |
| Potassium (mEq/L) | 4 (3.6–4.4) | 4.4 (3.9–4.9) | 0.16 |
| Chloride (mg/dL) | 103.9 (101–108) | 102.7 (98–108.5) | 0.35 |
| Carbon dioxide (mEq/L) | 23.6 (21–26) | 20.7 (14.2–25.9) | 0.96 |
| BUN (mg/dL) | 25.7 (12–30) | 38.7 (21.2–50) | 0.03 |
| SCr (mg/dL) | 1.5 (0.7–1.4) | 1.8 (0.9–2.5) | 0.05 |
| Glucose (mg/dL) | 168.5 (110.5–198) | 219.5 (124–251.2) | 0.30 |
| Calcium (mg/dL) | 8.2 (7.7–8.7) | 8.1 (7.2–8.5) | 0.21 |
| Magnesium (mg/dL) | 1.9 (1.6–2.1) | 2.3 (1.9–2.5) | 0.12 |
| Phosphate (mg/dL) | 3.5 (2.8–4) | 6.1 (3.8–7.6) | 0.26 |
| White blood cell (×103/mL) | 11 (7.2–13.8) | 15.6 (8.4–19.4) | 0.51 |
| Hemoglobin (g/dL) | 10.2 (8.6–11.8) | 9.7 (8.1–11.6) | 0.31 |
| Hematocrit (%) | 31.8 (27.6–36.2) | 31.4 (24.9–36) | 0.35 |
| Platelets (×103/mL) | 211.3 (143–268) | 215.5 (128.5–271.8) | 0.57 |
| Lactate (U/L) | 3 (1.4–3.3) | 8.2 (3.1–13.5) | 0.41 |
| PT (s) | 17.6 (11.5–16.1) | 19.9 (13.3–27.8) | 0.56 |
| INR | 1.7 (1.1–1.6) | 2 (1.3–2.8) | 0.56 |
| Albumin (g/L) | 3.1 (2.8–3.5) | 2.8 (2.3–3.2) | 0.71 |
| Total bilirubin (mg/dL) | 1.3 (0.5–1.2) | 2.5 (0.5–1.2) | 0.87 |
| Urine Output every 6 h (mL/h) | 60.4 (7–96.5) | 56.5 (10.3–58.4) | 0.49 |
| eGFR (mL/min/1.73 m2) | 71.2 (42–99.2) | 50.3 (26.8–70.5) | 0.11 |
| Durations | |||
| Time on mechanical ventilation (h) | 34.6 (0–0) | 147.2 (4–197.5) | 0.08 |
| ICU length of stay (h) | 87.4 (21–86) | 191.4 (22–282.5) | 0.08 |
| Scoring Assessment on ICU admission | |||
| APACHE II | 17 (13–20) | 27.1 (21–32) | 0.01 |
| SAPS II | 12.5 (5–18) | 27.5 (18.2–35) | 0.039 |
| MRCI | 62.9 (34–84) | 81.1 (43–104.5) | 0.339 |
| MRC-ICU | 6 (3–8) | 8.6 (4–12) | 0.107 |
| GCS at admission | 13.1 (12–15) | 7.2 (3–11) | 0.351 |
| Lactic acidosis (E87.2) | 62 (26) | 39 (53) | <0.001 |
| Hypokalemia (E87.6) | 83 (34) | 19 (26) | 0.22 |
| Kidney failure (N17.9) | 63 (26) | 33 (45) | 0.004 |
| Hypo-osmolality hyponatremia (E87.1) | 63 (26) | 26 (35) | 0.16 |
| Was not resuscitated (Z66) | 35 (14) | 51 (69) | <0.001 |
| Acute myocardial infarction (I21.A) | 52 (21) | 26 (35) | 0.025 |
| Unspecified sepsis (A41.9) | 53 (22) | 23 (31) | 0.14 |
| Selected Features | Mortality OR (95% CI) | p-Value | Length of ICU Stay OR (95% CI) | p-Value | Mechanical Ventilation OR (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Model I | ||||||
| Age | 1.02 (1.0–1.05) | 0.12 | 1.02 (1.0–1.03) | 0.05 | - | - |
| Body mass index (BMI) | - | - | 1.02 (1.0–1.05) | 0.11 | - | |
| White | - | - | 0.59 (0.35–0.98) | - | - | - |
| Hispanic | 6.11 (2.84–13.85) | <0.001 | - | - | - | - |
| SAPS II at admission | 1.12 (1.07–1.18) | 0.001 | 1.04 (1–1.11) | <0.001 | 1.17 (1.13–1.21) | <0.001 |
| APACHE II at admission | 1.13 (1.05–1.21) | 0.002 | 0.92 (0.88–0.98) | 0.15 | - | - |
| CCI | - | - | 1.13 (1.0–1.32) | 0.14 | - | - |
| Model II | ||||||
| Age | 1.03 (1.02–1.05) | <0.001 | 1.01 (1.0–1.03) | 0.09 | - | - |
| Height | - | - | 1.14 (1.01–1.35) | 0.11 | 1.02 (1.04–1.46) | 0.03 |
| Weight | - | - | 0.95 (0.89–1.01) | 0.09 | 0.95 (0.89–1.01) | 0.1 |
| Body mass index (BMI) | - | - | 1.17 (1.0–1.41) | 0.06 | 1.18 (1.0–1.42) | 0.07 |
| White | - | - | 0.56 (0.33–0.93) | 0.03 | - | - |
| Hispanic | 5.74 (3.15- 10.79) | <0.001 | - | - | 1.84 (1.11–3.07) | 0.02 |
| MRCI score at 24 h | 1.01 (1–1.02) | 0.003 | 1.01 (1.0–1.02) | <0.001 | 1.01 (1.01–1.02) | <0.001 |
| MRCI score at 48 h | 1.01 (1–1.02) | 0.004 | - | 1.01 (1.0–1.02) | 0.03 | |
| CCI | - | - | 1.13 (1.0–1.32) | 0.13 | - | - |
| Model III | ||||||
| Age | 1.03 (1.02–1.05) | <0.001 | 1.01 (1.0–1.03) | 0.1 | - | - |
| White | - | - | 0.59 (0.35–0.99) | 0.04 | - | - |
| Hispanic | 6.44 (3.45–12.41) | <0.001 | - | - | 2.21 (1.29–3.85) | 0.004 |
| MRC-ICU at 24 h | 1.12 (1.06–1.19) | <0.001 | 1.17 (1.1–1.24) | <0.001 | 1.21 (1.14–1.29) | <0.001 |
| MRC-ICU at 48 h | 1.1 (1.04–1.17) | 0.002 | 1.05 (1.0–1.11) | 0.7 | 1.11 (1.05–1.18) | 0.001 |
| CCI | - | - | 1.14 (1.0–1.34) | 0.1 | 0.84 (0.65–1.07) | 0.155 |
| Model IV | ||||||
| Age | 1.04 (1.01- 1.08) | 0.017 | - | - | - | - |
| Hispanic | 6.23 (2.55- 16.41) | 0.001 | - | - | - | - |
| SAPS II at admission | 1.09 (1.04–1.15) | 0.001 | 1.04 (1–1.08) | 0.072 | 1.17 (1.11–1.23) | <0.001 |
| APACHE II at admission | 1.14 (1.05–1.23) | 0.002 | 0.94 (0.89–1) | 0.038 | - | - |
| MRCI at 24 h | - | - | 0.99 (0.98–1) | 0.134 | 0.97 (0.95–0.99) | 0.001 |
| MRC-ICU at 24 h | - | - | 1.1 (1–1.22) | 0.05 | 1.3 (1.13–1.51) | <0.001 |
| CCI | 0.79 (0.6–1.03) | 0.093 | - | - | 0.77 (0.58–1) | 0.052 |
| Anti-infectives | - | - | 2.27 (1.15–4.57) | 0.019 | - | - |
| Anticoagulants | 0.38 (0.1–1.42) | 0.139 | 2.26 (1.02–5.29) | 0.05 | - | - |
| Psychiatric agents | - | - | 1.8 (0.96–3.36) | 0.065 | 2.52 (1.01–6.64) | 0.05 |
| Pulmonary agents | - | - | - | - | 3.14 (1.34–7.66) | 0.01 |
| Cardiovascular agents | - | - | 2.81 (1.46–5.53) | 0.002 | 0.4 (0.15–0.98) | 0.05 |
| Diuretics | - | - | 3.35 (1.74–6.62) | <0.001 | - | - |
| Analgesics sedatives | - | - | - | - | 6.96 (1.73–36.07) | 0.012 |
| Vasopressors | 5.55 (2.12–15.26) | 0.001 | 3.49 (1.63–7.75) | 0.002 | 5.75 (2.4–14.48) | <0.001 |
| Paralytic agents | 3.38 (1.09–11.11) | 0.039 | - | - | - | - |
| Vitamins | - | - | 1.63 (0.88–3.03) | 0.122 | 0.25 (0.09–0.62) | 0.004 |
| Others | 2.54 (1.08–6.15) | 0.034 | - | - | - | - |
| AIC | AUC | Sensitivity | Specificity | |
|---|---|---|---|---|
| ICU Mortality | ||||
| Admission Model | 222.007 (217.45–222.15) | 0.88 (0.77–0.97) | 0.72 (0.60–0.82) | 0.89 (0.85–0.92) |
| MRCI Model | 313 (308–313) | 0.73 (0.54–0.89) | 0.73 (0.60–0.84) | 0.89 (0.85–0.93) |
| MRCI and SAPS II Model | 225 (220–225) | 0.88 (0.75–0.97) | 0.73 (0.63–0.83) | 0.89 (0.84–0.93) |
| MRC-ICU Model | 302 (297–302) | 0.75 (0.57–0.89) | 0.73 (0.62–0.83) | 0.89 (0.85–0.92) |
| MRC-ICU and SAPS II Model | 225 (221–225) | 0.88 (0.76–0.97) | 0.73 (0.62–0.84) | 0.90 (0.85–0.94) |
| Medication Model | 236 (232–236) | 0.88 (0.78–0.96) | 0.61 (0.48–0.73) | 0.86 (0.82–0.90) |
| Full Model | 226 (221–226) | 0.88 (0.77–0.97) | 0.73 (0.62–0.84) | 0.89 (0.85–0.92) |
| Length of ICU Stay | ||||
| Admission Model | 422.74 (421–423) | 0.68 (0.53–0.82) | 0.63 (0.5–0.70) | 0.62 (0.54–0.70) |
| MRCI Model | 431 (429–431) | 0.64 (0.48–0.78) | 0.65 (0.58–0.71) | 0.62 (0.55–0.71) |
| MRCI and SAPS II Model | 421 (419–422) | 0.69 (0.53–0.83) | 0.64 (0.57–0.70) | 0.62 (0.55–0.69) |
| MRC-ICU Model | 404 (402–405) | 0.70 (0.52–0.83) | 0.64 (0.56–0.74) | 0.61 (0.55–0.70) |
| MRC-ICU and SAPS II Model | 401 (399–402) | 0.71 (0.57–0.84) | 0.63 (0.57–0.70) | 0.62 (0.56–0.70) |
| Medication Model | 323 (320–324) | 0.82 (0.71–0.93) | 0.75 (0.69–0.81) | 0.74 (0.68–0.80) |
| Full Model | 402 (399–403) | 0.71 (0.56–0.84) | 0.64 (0.58–0.71) | 0.62 (0.54–0.70) |
| Need for Mechanical Ventilation | ||||
| Admission Model | 304.62 (300.23–305.0) | 0.85 (0.72–0.95) | 0.79 (0.70–0.86) | 0.8 (0.75–0.85) |
| MRCI Model | 408 (406–409) | 0.65 (0.48–0.80) | 0.79(0.69–0.86) | 0.80 (0.75–0.85) |
| MRCI and SAPS II Model | 308 (304–308) | 0.84 (0.73–0.94) | 0.77 (0.69–0.86) | 0.80 (0.75–0.85) |
| MRC-ICU Model | 365 (362–366) | 0.75 (0.62–0.873) | 0.78 (0.69–0.86) | 0.80 (0.76–0.84) |
| MRC-ICU and SAPS II Model | 290 (286–291) | 0.87 (0.77–0.96) | 0.78 (0.71–0.86) | 0.80 (0.75–0.86) |
| Medication Model | 273 (269–274) | 0.86 (0.75–0.96) | 0.8 (0.71–0.88) | 0.81 (0.76–0.86) |
| Full Model | 286 (281–286) | 0.87 (0.77–0.96) | 0.78 (0.70–0.86) | 0.80 (0.76–0.85) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Mamun, M.A.; Strock, J.; Sharker, Y.; Shawwa, K.; Schmidt, R.; Slain, D.; Sakhuja, A.; Brothers, T.N. Evaluating the Medication Regimen Complexity Score as a Predictor of Clinical Outcomes in the Critically Ill. J. Clin. Med. 2022, 11, 4705. https://doi.org/10.3390/jcm11164705
Al-Mamun MA, Strock J, Sharker Y, Shawwa K, Schmidt R, Slain D, Sakhuja A, Brothers TN. Evaluating the Medication Regimen Complexity Score as a Predictor of Clinical Outcomes in the Critically Ill. Journal of Clinical Medicine. 2022; 11(16):4705. https://doi.org/10.3390/jcm11164705
Chicago/Turabian StyleAl-Mamun, Mohammad A., Jacob Strock, Yushuf Sharker, Khaled Shawwa, Rebecca Schmidt, Douglas Slain, Ankit Sakhuja, and Todd N. Brothers. 2022. "Evaluating the Medication Regimen Complexity Score as a Predictor of Clinical Outcomes in the Critically Ill" Journal of Clinical Medicine 11, no. 16: 4705. https://doi.org/10.3390/jcm11164705