Recent Increases in Influenza-Related Hospitalizations, Critical Care Resource Use, and In-Hospital Mortality: A 10-Year Population-Based Study in South Korea

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Case Definition
2.3. Variables for Critical Care Resource Use
2.4. Variables for Outcomes
2.5. Data Analysis
3. Results
3.1. Study Population
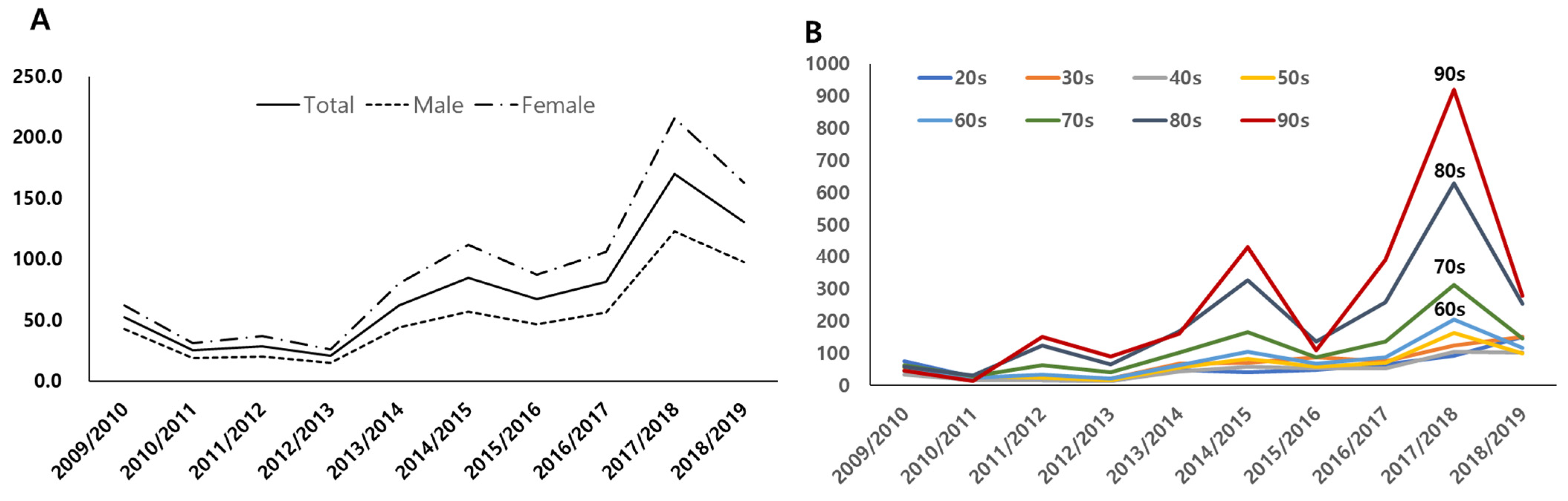
3.2. Incidence of Hospitalization
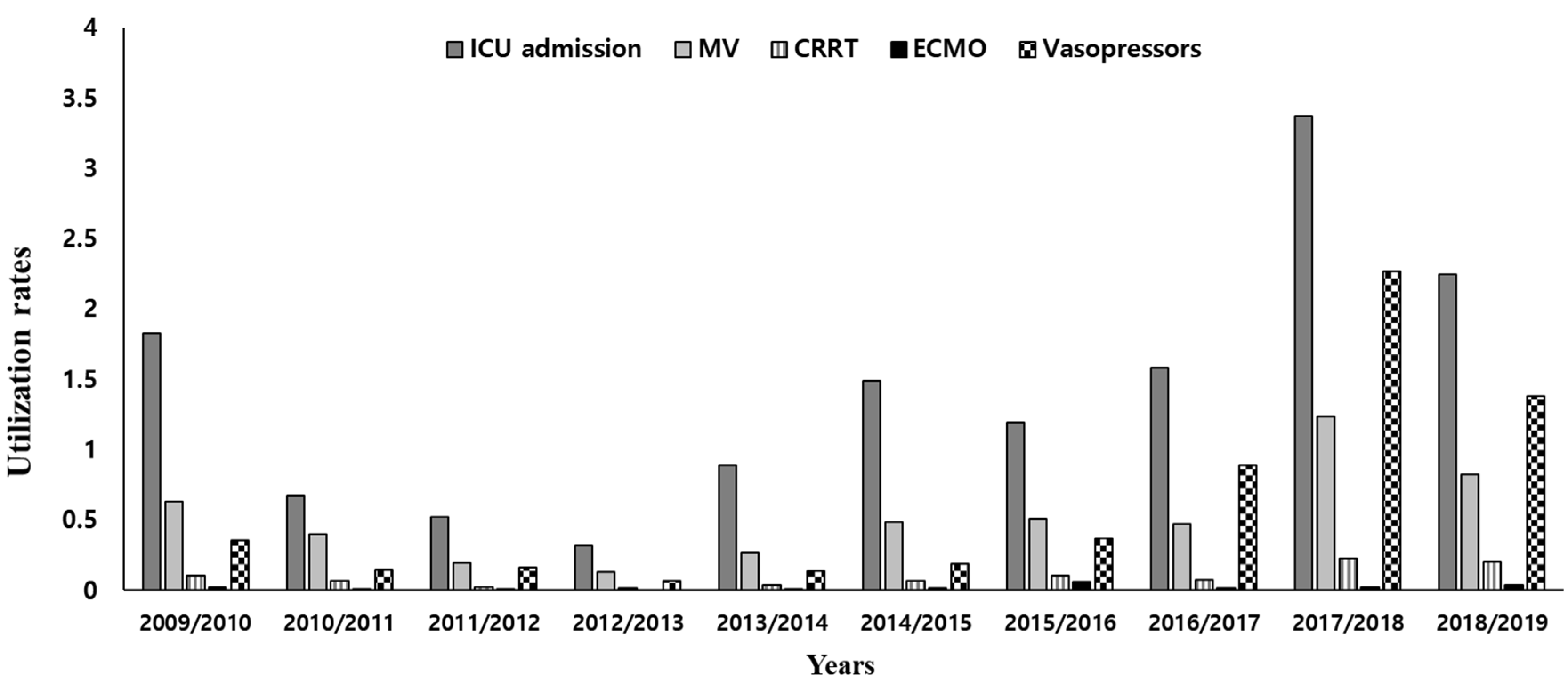
3.3. Critical Care Resource Use and Complications
3.4. Incidence Rates of ICU and In-Hospital Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Influenza Strategy 2019–2030. Available online: https://www.who.int/publications/i/item/9789241515320 (accessed on 5 December 2021).
- Gordon, A.; Reingold, A. The Burden of Influenza: A Complex Problem. Curr. Epidemiol. Rep. 2018, 5, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.; Park, J.Y.; Song, Y.; How, S.H.; Jung, K.S. Emerging respiratory infections threatening public health in the Asia-Pacific region: A position paper of the Asian Pacific Society of Respirology. Respirology 2019, 24, 590–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rice, T.W.; Rubinson, L.; Uyeki, T.M.; Vaughn, F.L.; John, B.B.; Miller, R.R.; Higgs, E.; Randolph, A.; Smoot, B.E.; Thompson, B.T. Critical illness from 2009 pandemic influenza A virus and bacterial coinfection in the United States. Crit. Care Med. 2012, 40, 487–498. [Google Scholar] [CrossRef] [Green Version]
- Timmers, P.; Kerssens, J.J.; Minton, J.; Grant, I.; Wilson, J.F.; Campbell, H.; Fischbacher, C.M.; Joshi, P.K. Trends in disease incidence and survival and their effect on mortality in Scotland: Nationwide cohort study of linked hospital admission and death records 2001–2016. BMJ Open 2020, 10, e034299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, J.C.; Lee, I.K.; Huang, W.C.; Chen, Y.C.; Tsai, C.Y. Clinical Characteristics and Predictors of Mortality in Critically Ill Influenza Adult Patients. J. Clin. Med. 2020, 9, 1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Disease Burden of Influenza. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/flu/about/burden/index.html (accessed on 21 December 2021).
- Public Health England. Flu Annual Report: Winter 2019 to 2020. Available online: https://www.gov.uk/government/statistics/annual-flu-reports (accessed on 22 December 2021).
- O’Halloran, A.C.; Holstein, R.; Cummings, C.; Kirley, P.D.; Alden, N.B.; Yousey-Hindes, K.; Anderson, E.J.; Ryan, P.; Kim, S.; Lynfield, R.; et al. Rates of Influenza-Associated Hospitalization, Intensive Care Unit Admission, and In-Hospital Death by Race and Ethnicity in the United States From 2009 to 2019. JAMA Netw. Open 2021, 4, e2121880. [Google Scholar] [CrossRef]
- Byeon, K.H.; Kim, J.; Choi, B.Y.; Kim, J.Y.; Lee, N. Age-Period-Cohort Analysis of Influenza in Koreans: The National Health Insurance Research Database, 2009–2018. J. Korean Med. Sci. 2020, 35, e121. [Google Scholar] [CrossRef]
- Byeon, K.H.; Kim, J.; Choi, B.Y.; Kim, J.Y.; Lee, N. Factors Affecting the Incidence of Hospitalized Pneumonia after Influenza Infection in Korea Using the National Health Insurance Research Database, 2014–2018: Focusing on the Effect of Antiviral Therapy in the 2017 Flu Season. J. Korean Med. Sci. 2020, 35, e318. [Google Scholar] [CrossRef]
- Kim, Y.W.; Yoon, S.J.; Oh, I.H. The economic burden of the 2009 pandemic H1N1 influenza in Korea. Scand. J. Infect. Dis. 2013, 45, 390–396. [Google Scholar] [CrossRef]
- Suh, M.; Kang, D.R.; Lee, D.H.; Choi, Y.J.; Tchoe, B.; Nam, C.M.; Kim, H.J.; Lee, J.K.; Jun, B.Y.; Youm, Y.; et al. Socioeconomic burden of influenza in the Republic of Korea, 2007–2010. PLoS ONE 2013, 8, e84121. [Google Scholar] [CrossRef]
- Lee, Y.H.; Han, K.; Ko, S.H.; Ko, K.S.; Lee, K.U. Taskforce Team of Diabetes Fact Sheet of the Korean Diabetes, A. Data Analytic Process of a Nationwide Population-Based Study Using National Health Information Database Established by National Health Insurance Service. Diabetes Metab. J. 2016, 40, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Kim, K.H. Comparative study on three algorithms of the ICD-10 Charlson comorbidity index with myocardial infarction patients [article in Korean]. J. Prev. Med. Public Health 2010, 43, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Zhou, Y.; Fu, X.; Liu, X.; Huang, C.; Tian, G.; Ding, C.; Wu, J.; Lan, L.; Yang, S. Use of corticosteroids in influenza-associated acute respiratory distress syndrome and severe pneumonia: A systemic review and meta-analysis. Sci. Rep. 2020, 10, 3044. [Google Scholar] [CrossRef] [Green Version]
- Korea Ministry of Health and Welfare. Korea Health Law. Available online: http://law.go.kr (accessed on 10 November 2021).
- Korean Statistical Information Service. Available online: https://kosis.kr/eng/index/index.do (accessed on 30 December 2021).
- Korea Disease Control and Prevention Agency. Health Statistics. Available online: https://health.kdca.go.kr/healthinfo/biz/pblcVis/details.do?ctgrSn=71 (accessed on 12 August 2022).
- Choi, W.S. The National Influenza Serveillance System of Korea. Infect. Chemother. 2019, 51, 98–106. [Google Scholar] [CrossRef]
- Nguyen, A.M.; Noymer, A. Influenza mortality in the United States, 2009 pandemic: Burden, timing and age distribution. PLoS ONE 2013, 8, e64198. [Google Scholar] [CrossRef]
- Wu, S.; Wei, Z.; Greene, C.M.; Yang, P.; Su, J.; Song, Y.; Iuliano, A.D.; Wang, Q. Mortality burden from seasonal influenza and 2009 H1N1 pandemic influenza in Beijing, China, 2007–2013. Influenza Other Respir. Viruses 2018, 12, 88–97. [Google Scholar] [CrossRef]
- The Korean Disease Control and Prevention Agency. Infectious Disease Surveillance Year Book. 2010. Available online: http://www.kdca.go.kr/npt/biz/npp/portal/nppPblctDtaView.do?pblctDtaSeAt=1&pblctDtaSn=10 (accessed on 10 December 2021).
- Li, J.; Wang, C.; Ruan, L.; Jin, S.; Ye, C.; Yu, H.; Zhu, W.; Wang, X. Development of influenza-associated disease burden pyramid in Shanghai, China, 2010-2017: A Bayesian modelling study. BMJ Open 2021, 11, e047526. [Google Scholar] [CrossRef]
- von der Beck, D.; Seeger, W.; Herold, S.; Günther, A.; Löh, B. Characteristics and outcomes of a cohort hospitalized for pandemic and seasonal influenza in Germany based on nationwide inpatient data. PLoS ONE 2017, 12, e0180920. [Google Scholar] [CrossRef] [Green Version]
- Baker, A.W.; Edmond, M.B.; Herwaldt, L.A.; Chen, L.F.; Srikantaswamy, S.; Sexton, D.J. Real-Time Surveillance of Influenza Morbidity: Tracking Intensive Care Unit Resource Utilization. Ann. Am. Thorac. Soc. 2017, 14, 1810–1817. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.; Ye, L.; Noorduyn, S.G.; Hux, M.; Thommes, E.; Goeree, R.; Ambrose, A.; Andrew, M.K.; Hatchette, T.; Boivin, G.; et al. Resource utilization and cost of influenza requiring hospitalization in Canadian adults: A study from the serious outcomes surveillance network of the Canadian Immunization Research Network. Influenza Other Respir. Viruses 2018, 12, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Viasus, D.; Pano-Pardo, J.R.; Pachon, J.; Campins, A.; López-Medrano, F.; Villoslada, A.; Fariñas, M.; Moreno, A.; Rodríguez-Baño, J.; Oteo, J.; et al. Factors associated with severe disease in hospitalized adults with pandemic (H1N1) 2009 in Spain. Clin. Microbiol. Infect. 2011, 17, 738–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferdinands, J.M.; Thompson, M.G.; Blanton, L.; Spencer, S.; Grant, L.; Fry, A.M. Does influenza vaccination attenuate the severity of breakthrough infections?A narrative review and recommendations for further research. Vaccine 2021, 39, 3678–3695. [Google Scholar] [CrossRef]
- Godoy, P.; Romero, A.; Soldevila, N.; Torner, N.; Jané, M.; Martínez, A.; A Caylà, J.; Rius, C.; Domínguez, A. Influenza vaccine effectiveness in reducing severe outcomes over six influenza seasons, a case-case analysis, Spain, 2010/11 to 2015/16. Eurosurveillance 2018, 23, 1700732. [Google Scholar] [CrossRef] [Green Version]
- Marin-Hernandez, D.; Schwartz, R.E.; Nixon, D.F. Epidemiological evidence for association between higher influenza vaccine uptake in the elderly and lower COVID-19 deaths in Italy. J. Med. Virol. 2021, 93, 64–65. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Estimated Flu-Related Illnesses, Medical Visits, Hospitalizations, and Deaths in the United States—2017–2018 Flu Season. Available online: https://www.cdc.gov/flu/about/burden/2017-2018.htm#:~:text=CDC%20estimates%20that%20flu%20burden,from%20flu%20(Table%201) (accessed on 10 July 2022).
- Lane, C.J.; Bhatnagar, M.; Lutrick, K.; Maves, R.C.; Weiner, D.; Olvera, D.R.; Uyeki, T.M.; Cobb, J.P.; Brown, J.C. ICU Resource Limitations During Peak Seasonal Influenza: Results of a 2018 National Feasibility Study. Crit. Care Explor. 2022, 4, e0606. [Google Scholar] [CrossRef]
- Gutierrez-Gonzalez, E.; Cantero-Escribano, J.M.; Redondo-Bravo, L.; San Juan-Sanz, I.; Robustillo-Rodela, A.; Cendejas-Bueno, E.; Influenza Working Group. Effect of vaccination, comorbidities and age on mortality and severe disease associated with influenza during the season 2016-2017 in a Spanish tertiary hospital. J. Infect. Public Health 2019, 12, 486–491. [Google Scholar] [CrossRef]
- Jung, C.H.; Son, J.W.; Kang, S.; Kim, W.J.; Kim, H.-S.; Kim, H.S.; Seo, M.; Shin, H.-J.; Lee, S.-S.; Jeong, S.J.; et al. Diabetes Fact Sheets in Korea, 2020: An Appraisal of Current Status. Diabetes Metab. J. 2021, 45, 1–10. [Google Scholar] [CrossRef]
- Choi, W.S.; Cowling, B.J.; Noh, J.Y.; Song, J.Y.; Wie, S.-H.; Lee, J.S.; Bin Seo, Y.; Lee, J.; Jeong, H.W.; Kim, Y.K.; et al. Disease burden of 2013-2014 seasonal influenza in adults in Korea. PLoS ONE 2017, 12, e0172012. [Google Scholar] [CrossRef]
- Meduri, G.U.; Golden, E.; Freire, A.X.; Taylor, E.; Zaman, M.; Carson, S.J.; Gibson, M.; Umberger, R. Methylprednisolone infusion in early severe ARDS: Results of a randomized controlled trial. Chest 2007, 131, 954–963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muthuri, S.G.; Venkatesan, S.; Myles, P.R.; Leonardi-Bee, J.; A Al Khuwaitir, T.S.; Al Mamun, A.; Anovadiya, A.P.; Azziz-Baumgartner, E.; Báez, C.; Bassetti, M.; et al. Effectiveness of neuraminidase inhibitors in reducing mortality in patients admitted to hospital with influenza A H1N1pdm09 virus infection: A meta-analysis of individual participant data. Lancet Respir. Med. 2014, 2, 395–404. [Google Scholar] [CrossRef] [Green Version]
- Mulpuru, S.; Li, L.; Ye, L.; Hatchette, T.; Andrew, M.K.; Ambrose, A.; Boivin, G.; Bowie, W.; Chit, A.; Dos Santos, G.; et al. Effectiveness of Influenza Vaccination on Hospitalizations and Risk Factors for Severe Outcomes in Hospitalized Patients With COPD. Chest 2019, 155, 69–78. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | 2009/2010 | 2010/2011 | 2011/2012 | 2012/2013 | 2013/2014 | 2014/2015 | 2015/2016 | 2016/2017 | 2017/2018 | 2018/2019 |
|---|---|---|---|---|---|---|---|---|---|---|
| No. of patients * | 20,465 | 9860 | 11,400 | 8247 | 25,301 | 34,986 | 27,951 | 34,240 | 71,944 | 55,758 |
| Proportion of patients (%) † | 0.05 | 0.03 | 0.03 | 0.02 | 0.06 | 0.08 | 0.07 | 0.08 | 0.17 | 0.13 |
| Age-adjusted hospitalization rate ‡ | 52.61 | 25.04 | 28.61 | 20.46 | 62.06 | 84.89 | 67.15 | 81.51 | 169.86 | 130.59 |
| Age, years # | 43.8 | 45.9 | 53.8 | 51.8 | 50.4 | 55.7 | 49.6 | 53.3 | 57.2 | 48.6 |
| Age groups (n) | ||||||||||
| 19–29 years | 5807 | 1987 | 1246 | 1023 | 3639 | 3038 | 3589 | 4810 | 6881 | 11,231 |
| 30–39 years | 3800 | 2168 | 2267 | 1754 | 5325 | 5381 | 6597 | 5669 | 9126 | 10,783 |
| 40–49 years | 3048 | 1548 | 1474 | 1266 | 3855 | 5073 | 4778 | 4564 | 8922 | 8517 |
| 50–59 years | 3715 | 2058 | 1878 | 1323 | 4440 | 6693 | 4755 | 5825 | 13,746 | 8440 |
| 60–69 years | 1948 | 989 | 1402 | 902 | 2855 | 5098 | 3533 | 4722 | 11,755 | 7118 |
| 70–79 years | 1628 | 811 | 1816 | 1212 | 3163 | 5229 | 2791 | 4454 | 10,613 | 5117 |
| 80–89 years | 473 | 283 | 1138 | 648 | 1794 | 3816 | 1729 | 3504 | 9117 | 3956 |
| ≥90 years | 46 | 16 | 179 | 119 | 230 | 658 | 179 | 692 | 1784 | 596 |
| Frequency of men (%) | 40.24 | 37.65 | 34.64 | 36.19 | 34.99 | 33.36 | 34.15 | 34.33 | 35.89 | 37.14 |
| Underlying comorbidities (%) | ||||||||||
| Diabetes mellitus | 2.19 | 2.94 | 3.61 | 4.27 | 3.46 | 4.82 | 3.97 | 4.07 | 4.56 | 3.46 |
| Cardiovascular disease | 0.57 | 0.61 | 1.22 | 1.32 | 0.83 | 1.21 | 1.04 | 1.12 | 1.43 | 1.13 |
| Cerebrovascular disease | 0.92 | 1.28 | 1.77 | 1.50 | 1.27 | 1.82 | 1.48 | 1.65 | 1.91 | 1.40 |
| Chronic lung disease | 1.91 | 3.04 | 4.68 | 4.22 | 3.48 | 4.40 | 4.05 | 3.78 | 4.01 | 3.40 |
| Chronic renal disease | 0.61 | 0.81 | 0.89 | 0.96 | 0.70 | 1.01 | 0.88 | 1.00 | 1.05 | 0.95 |
| Chronic liver disease | 1.63 | 2.33 | 2.99 | 2.89 | 2.09 | 3.31 | 3.31 | 2.93 | 2.95 | 2.02 |
| Cancer | 1.74 | 1.70 | 1.68 | 1.90 | 1.58 | 1.79 | 1.38 | 1.72 | 1.75 | 1.56 |
| Charlson comorbidity index # | 0.18 | 0.23 | 0.3 | 0.29 | 0.23 | 0.31 | 0.28 | 0.28 | 0.3 | 0.25 |
| Hospital types (%) | ||||||||||
| Tertiary hospital | 15.58 | 13.10 | 10.47 | 10.76 | 7.98 | 7.31 | 9.92 | 9.66 | 8.78 | 8.33 |
| General hospital | 50.35 | 47.24 | 47.73 | 47.54 | 46.03 | 48.59 | 51.32 | 47.29 | 47.97 | 50.25 |
| Hospital | 32.44 | 38.75 | 40.48 | 40.48 | 44.92 | 43.09 | 37.74 | 42.14 | 41.91 | 40.20 |
| Others | 1.63 | 0.90 | 1.32 | 1.22 | 1.08 | 1.01 | 1.02 | 0.92 | 1.34 | 1.22 |
| Influenaza vaccination (%) ‡‡ | 28.2 | 31.9 | 33.5 | 35.8 | 34.0 | 34.8 | 35.3 | 37.5 | 40.0 | 41.9 |
| Variables | n/Rate | 2009/2010 | 2010/2011 | 2011/2012 | 2012/2013 | 2013/2014 | 2014/2015 | 2015/2016 | 2016/2017 | 2017/2018 | 2018/2019 | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Myocardial infarct | n | 125 | 32 | 57 | 37 | 93 | 230 | 121 | 173 | 413 | 256 | <0.001 |
| rate *,† | 0.32 | 0.08 | 0.14 | 0.09 | 0.23 | 0.56 | 0.29 | 0.41 | 0.98 | 0.60 | ||
| Myocarditis | n | 17 | 1 | 6 | 10 | 12 | 13 | 3 | 8 | 14 | 20 | 0.123 |
| rate *,† | 0.04 | 0.00 | 0.02 | 0.02 | 0.03 | 0.03 | 0.01 | 0.02 | 0.03 | 0.05 | ||
| Cerebral infarct | n | 219 | 117 | 195 | 140 | 294 | 582 | 379 | 599 | 1299 | 651 | <0.001 |
| rate *,† | 0.56 | 0.30 | 0.49 | 0.35 | 0.72 | 1.41 | 0.91 | 1.43 | 3.07 | 1.52 | ||
| Cerebral hemorrhage | n | 188 | 76 | 148 | 82 | 228 | 401 | 242 | 339 | 717 | 331 | <0.001 |
| rate *,† | 0.48 | 0.19 | 0.37 | 0.20 | 0.56 | 0.97 | 0.58 | 0.81 | 1.69 | 0.78 | ||
| Liver failure | n | 377 | 163 | 159 | 92 | 250 | 468 | 304 | 295 | 1022 | 645 | <0.001 |
| rate *,† | 0.97 | 0.41 | 0.40 | 0.23 | 0.61 | 1.14 | 0.73 | 0.70 | 2.41 | 1.51 | ||
| Heart failure | n | 378 | 156 | 330 | 198 | 451 | 828 | 690 | 1059 | 2967 | 1619 | <0.001 |
| rate *,† | 0.97 | 0.40 | 0.83 | 0.49 | 1.11 | 2.01 | 1.66 | 2.52 | 7.00 | 3.79 | ||
| ICU death | n | 92 | 62 | 27 | 15 | 45 | 89 | 92 | 83 | 284 | 179 | <0.001 |
| rate *,† | 0.24 | 0.16 | 0.07 | 0.04 | 0.11 | 0.22 | 0.22 | 0.20 | 0.67 | 0.42 | ||
| Hospital death | n | 135 | 89 | 61 | 30 | 91 | 216 | 169 | 184 | 610 | 314 | <0.001 |
| rate *,† | 0.35 | 0.23 | 0.15 | 0.07 | 0.22 | 0.52 | 0.41 | 0.44 | 1.44 | 0.74 | ||
| Median length of ICU stay ‡ | days | 10.0 | 9.0 | 11.0 | 12.0 | 10.0 | 11.0 | 12.0 | 9.0 | 10.0 | 10.0 | 0.003 |
| Median length of hospital stay ‡ | days | 5.0 | 5.0 | 4.0 | 4.0 | 4.0 | 4.0 | 4.0 | 4.0 | 4.0 | 4.0 | <0.001 |
| Variables | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Age | 1.089 | 1.086–1.093 | 1.090 | 1.085–1095 |
| Gender (male) | 1.835 | 1.676–2.008 | 1.491 | 1.339–1.660 |
| Years | ||||
| 2009/2010–2010/2011 | reference | reference | reference | reference |
| 2011/2012–2012/2013 | 0.625 | 0.489–0.798 | 0.350 | 0.265–0.462 |
| 2013/2014–2014/2015 | 0.687 | 0.578–0.817 | 0.487 | 0.399–0.596 |
| 2015/2016–2016/2017 | 0.767 | 0.648–0.907 | 0.383 | 0.312–0.468 |
| 2017/2018–2018/2019 | 0.979 | 0.845–1.133 | 0.378 | 0.315–0.453 |
| Charlson comorbidity index | 1.408 | 1.386–1.430 | 1.233 | 1.207–1.259 |
| Type of hospitals | ||||
| Hospitals * | reference | reference | reference | reference |
| General hospitals † | 4.949 | 4.223–5.800 | 1.944 | 1.645–2.298 |
| Tertiary hospitals ‡ | 15.993 | 13.546–18.883 | 2.365 | 1.955–2.860 |
| Others | 4.656 | 3.0370–7.1392 | 2.907 | 1.865–4.530 |
| Mechanical ventilation | 140.110 | 126.000–155.799 | 11.873 | 10.129–13.916 |
| CRRT | 284.161 | 229.745–351.467 | 7.233 | 5.398–9.693 |
| Use of vasopressors | 125.171 | 112.938–138.729 | 11.248 | 9.689–13.057 |
| Use of steroids | 4.568 | 4.030–5.177 | 0.900 | 0.761–1.065 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, T.H.; Lee, H.S.; Kim, N.-E.; Lee, K.J.; Kim, Y.K.; An, J.N.; Kim, J.-H.; Kim, H.W.; Park, S. Recent Increases in Influenza-Related Hospitalizations, Critical Care Resource Use, and In-Hospital Mortality: A 10-Year Population-Based Study in South Korea. J. Clin. Med. 2022, 11, 4911. https://doi.org/10.3390/jcm11164911
Hong TH, Lee HS, Kim N-E, Lee KJ, Kim YK, An JN, Kim J-H, Kim HW, Park S. Recent Increases in Influenza-Related Hospitalizations, Critical Care Resource Use, and In-Hospital Mortality: A 10-Year Population-Based Study in South Korea. Journal of Clinical Medicine. 2022; 11(16):4911. https://doi.org/10.3390/jcm11164911
Chicago/Turabian StyleHong, Tae Hwa, Hyung Seok Lee, Nam-Eun Kim, Kyu Jin Lee, Yong Kyun Kim, Jung Nam An, Joo-Hee Kim, Hyung Won Kim, and Sunghoon Park. 2022. "Recent Increases in Influenza-Related Hospitalizations, Critical Care Resource Use, and In-Hospital Mortality: A 10-Year Population-Based Study in South Korea" Journal of Clinical Medicine 11, no. 16: 4911. https://doi.org/10.3390/jcm11164911
APA StyleHong, T. H., Lee, H. S., Kim, N.-E., Lee, K. J., Kim, Y. K., An, J. N., Kim, J.-H., Kim, H. W., & Park, S. (2022). Recent Increases in Influenza-Related Hospitalizations, Critical Care Resource Use, and In-Hospital Mortality: A 10-Year Population-Based Study in South Korea. Journal of Clinical Medicine, 11(16), 4911. https://doi.org/10.3390/jcm11164911