Abstract
Background: A pace and ablate strategy may be performed in refractory atrial fibrillation with rapid ventricular response. Objective: We aimed to assess sex-related differences in patient selection and clinical outcomes after pace and ablate. Methods: In a retrospective multicentre study, patients undergoing AV junction ablation were studied. Sex-related differences in baseline characteristics, all-cause mortality, heart failure (HF) hospitalizations, and device-related complications were assessed. Results: Overall, 513 patients underwent AV junction ablation (median age 75 years, 50% men). At baseline, men were younger (72 vs. 78 years, p < 0.001), more frequently had non-paroxysmal AF (82% vs. 72%, p = 0.006), had a lower LVEF (35% vs. 55%, p < 0.001) and more frequently had cardiac resynchronization therapy (75% vs. 25%, p < 0.001). Interventional complications were rare in both groups (1.2% vs. 1.6%, p = 0.72). Patients were followed for a median of 42 months in survivors (IQR 22–62). After 4 years of follow-up, the combined endpoint of all-cause death or HF hospitalization occurred more often in men (38% vs. 27%, p = 0.008). The same was observed for HF hospitalizations (22% vs. 11%, p = 0.021) and all-cause death (28% vs. 21%, p = 0.017). Sex category remained an independent predictor of death or HF hospitalization after adjustment for age, LVEF and type of stimulation. Lead-related complications, infections, and upgrade to ICD or CRT occurred in 2.1%, 0.2% and 3.5% of patients, respectively. Conclusions: Pace and ablate is safe with a need for subsequent device-related re-interventions in 5.8% over 4 years. We found significant sex-related differences in patient selection, and women had a more favourable clinical course after AV junction ablation.
1. Introduction
Atrial fibrillation has shown a steep increase in recent years and is likely to further increase [1]. Despite significant advantages in catheter ablation [2], rhythm control by means of catheter ablation and/or medication is not attainable in a substantial proportion of patients with atrial fibrillation, in particular in patients with persistent, long standing and permanent atrial fibrillation [3,4]. For those with intractable symptoms or insufficient rate control, pace and ablate is a well-established treatment option, which is technically straight-forward and frequently results in immediate symptomatic benefit [5,6,7,8].
The pace and ablate approach received significant attention, when the recent APAF-CRT study showed that cardiac resynchronization therapy (CRT) followed by AV junction ablation improved all-cause mortality as well as the combination of all-cause mortality and heart failure (HF) hospitalizations, when compared to pharmacological therapy in patients with permanent atrial fibrillation and narrow QRS [5,9]. However, uncertainties regarding optimal patient selection and timing for this procedure remain. One of the concerns is the risk for subsequent device-related complications in pacemaker-dependent patients [10,11]. However, with a sample size of 63 patients in the intervention arm, APAF-CRT was too small to study the incidence of device-related complications in this particularly vulnerable subset of patients [9].
Sex- and gender-related bias in patient selection as well as differences in outcomes have been described for numerous medical procedures [12,13,14,15,16,17]. The impact on patient selection for and outcome after pace and ablate has not been studied to date. Therefore, we aimed to assess sex- and gender-related differences in patient selection and clinical outcomes in a large multicentre cohort of patients undergoing AV junction ablation for refractory atrial arrhythmias.
2. Methods
2.1. Study Population
Consecutive patients undergoing catheter ablation in Switzerland are prospectively enrolled into a national ablation registry [18]. For this retrospective multicentre analysis, consecutive patients undergoing AV junction ablation as part of a pace-and-ablate strategy for refractory atrial fibrillation between 2011 and 2019 at the two largest ablation centres in Switzerland were enrolled. Patient data were collected from the electronic health records systems. Patients with missing follow-up data were excluded from analysis.
The study was performed in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by local Ethics Committees. The authors had full access to and take full responsibility for the integrity of the data.
2.2. Baseline Evaluation
All patients underwent pre-procedural clinical evaluation including detailed medical history and standard blood tests. A detailed device history was obtained, including the type of device (pacemaker or ICD), the type of stimulation (RV only or biventricular), and the time since first device-implant. Transthoracic echocardiography was performed to assess the left ventricular ejection fraction (LVEF).
2.3. Ablation Procedure
The AV junction ablation procedures were performed in local anaesthesia and guided by fluoroscopy. The 3D electro-anatomical mapping systems were only exceptionally used. The selection of a non-irrigated or irrigated ablation catheter was based on the operator’s discretion.
2.4. Follow-Up
Follow-up data and vital status were obtained from the electronic health records. Hospitalisation for heart failure was adjudicated by the local investigators.
The primary endpoint of our analysis was a composite clinical outcome consisting of all-cause mortality or hospitalisation for heart failure during follow-up. Secondary endpoints were the individual components of the primary endpoint (all-cause mortality and hospitalisation for heart failure), device-related re-interventions during follow-up due to lead-complications, infections, or an upgrade to ICD or CRT.
2.5. Statistical Analysis
Categorical variables are reported as frequencies and percentages, for frequency comparisons we used chi-square tests. Continuous variables are reported as medians and interquartile ranges (IQR), comparisons between groups were performed with the Mann–Whitney U test. We additionally performed univariate and multivariate Cox regression models to investigate associations between sex category and outcomes. These associations are reported as hazard ratios (HRs) with 95% confidence intervals (CIs). We further illustrate incidences of endpoints using Kaplan–Meier curves, dichotomized by sex category. A p-value of <0.05 was considered statistically significant. Statistical analyses were performed using SPSS Statistics, IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0, Armonk, NY: IBM Corp.
3. Results
3.1. Study Population
Between 2011 and 2019, 513 AV junction ablations were performed in the two participating centres. Baseline and procedural characteristics are summarized in Table 1 and Table 2. Median age was 75 years (IQR 69–81), and 258 (50%) patients were women. Baseline differences between men and women were observed for age (72 vs. 78 years, p < 0.001), comorbidities such as coronary artery disease (47% vs. 24%, p < 0.001), and for the presence of persistent AF (82% vs. 72%, p < 0.001). No significant difference was present concerning symptom status with 48% of patients having NYHA class III or greater and 62% having EHRA class III or greater. LVEF was significantly lower in men at baseline (35% vs. 55%, p < 0.001) and median QRS-duration was significantly longer (122 ms vs. 96 ms, p < 0.001). While Beta-blocker and ACEI/ARB therapy were more frequently prescribed in men (88% vs. 81%, p = 0.03 and 71% vs. 63%, p = 0.04, respectively), no significant differences were noted among other medications.

Table 1.
Baseline characteristics of the patients.
Table 2.
Procedural characteristics.
3.2. Pace and Ablate as Primary or Secondary Treatment Strategy
Patient selection for primary ablation of the AV junction (without any preceding attempt at interventional rhythm control by means of pulmonary vein isolation) or secondary ablation of the AV junction (after failed previous attempts for atrial fibrillation ablation) was not different between men and women (primary strategy 76% vs. 77%, secondary strategy 24% vs. 23%, p = 0.94).
3.3. Device Types Used for Pace and Ablate
In 359 cases (70%), a pacemaker or ICD had been implanted in a previous hospitalization. In the remaining cases, device implantation was performed immediately before AV junction ablation. Overall, CRT devices were more frequently implanted in men compared to women (53% vs. 17%, p < 0.001), as were ICDs (31% vs. 6%, p < 0.001).
3.4. Outcomes after Pace and Ablate
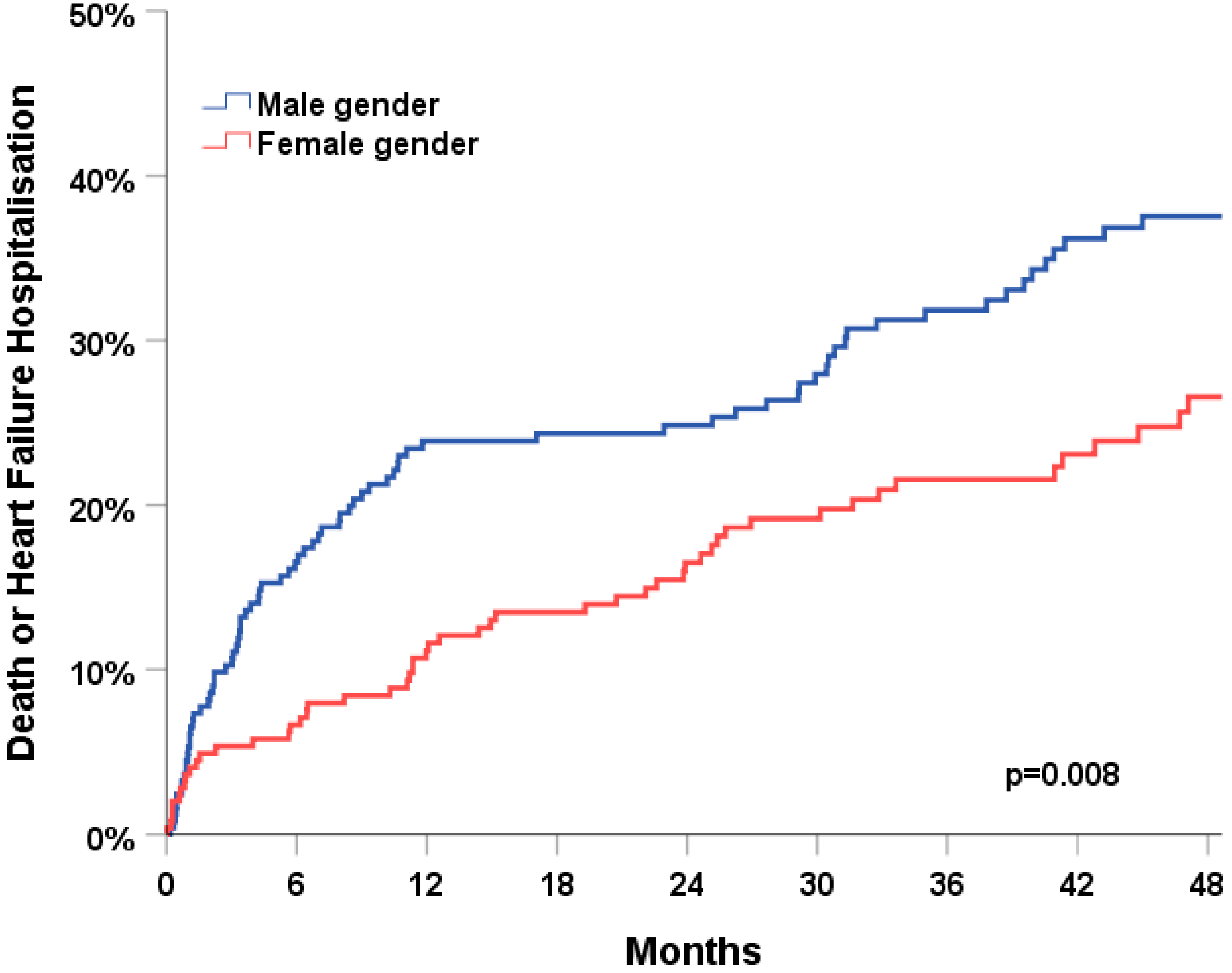
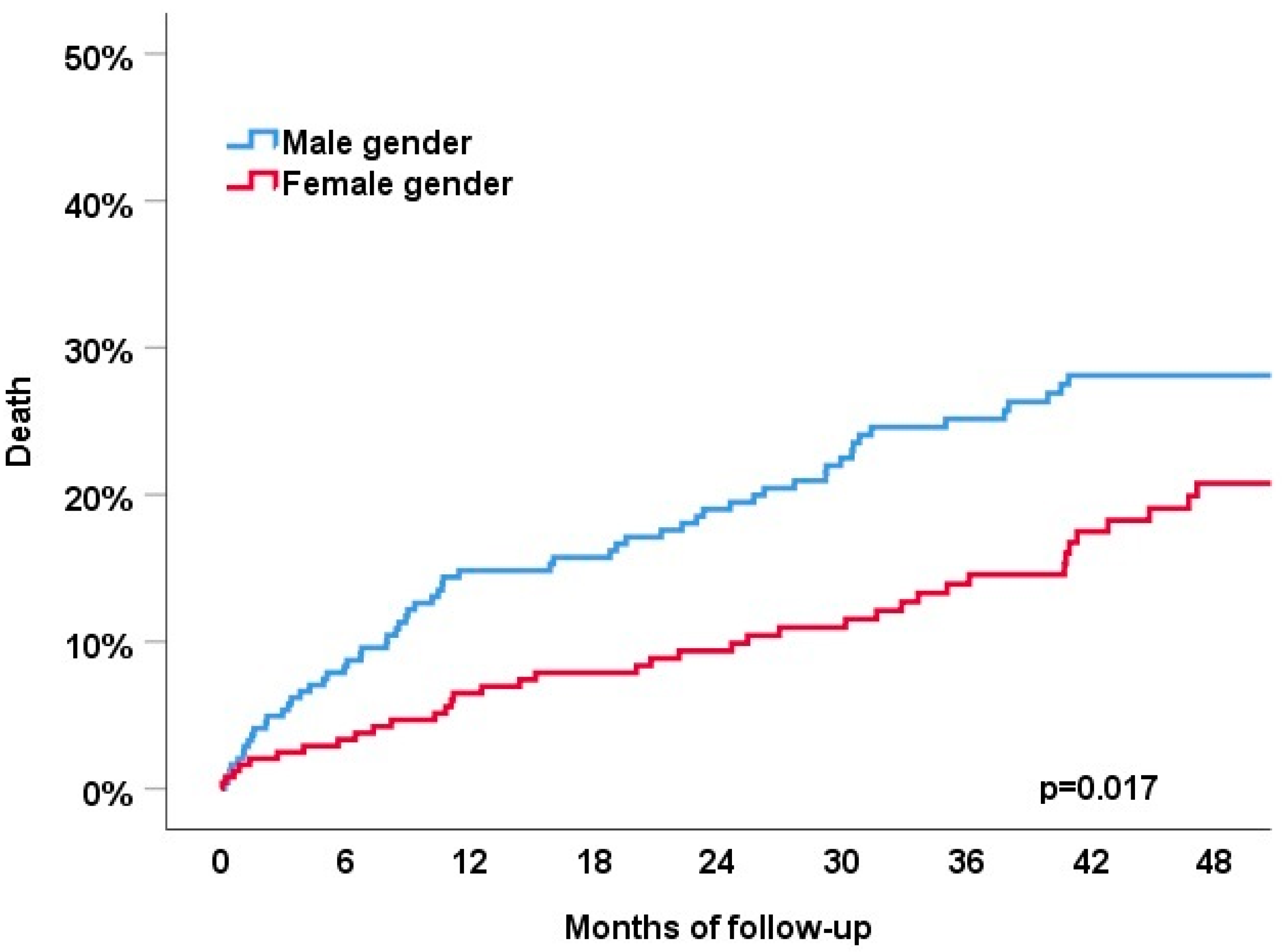
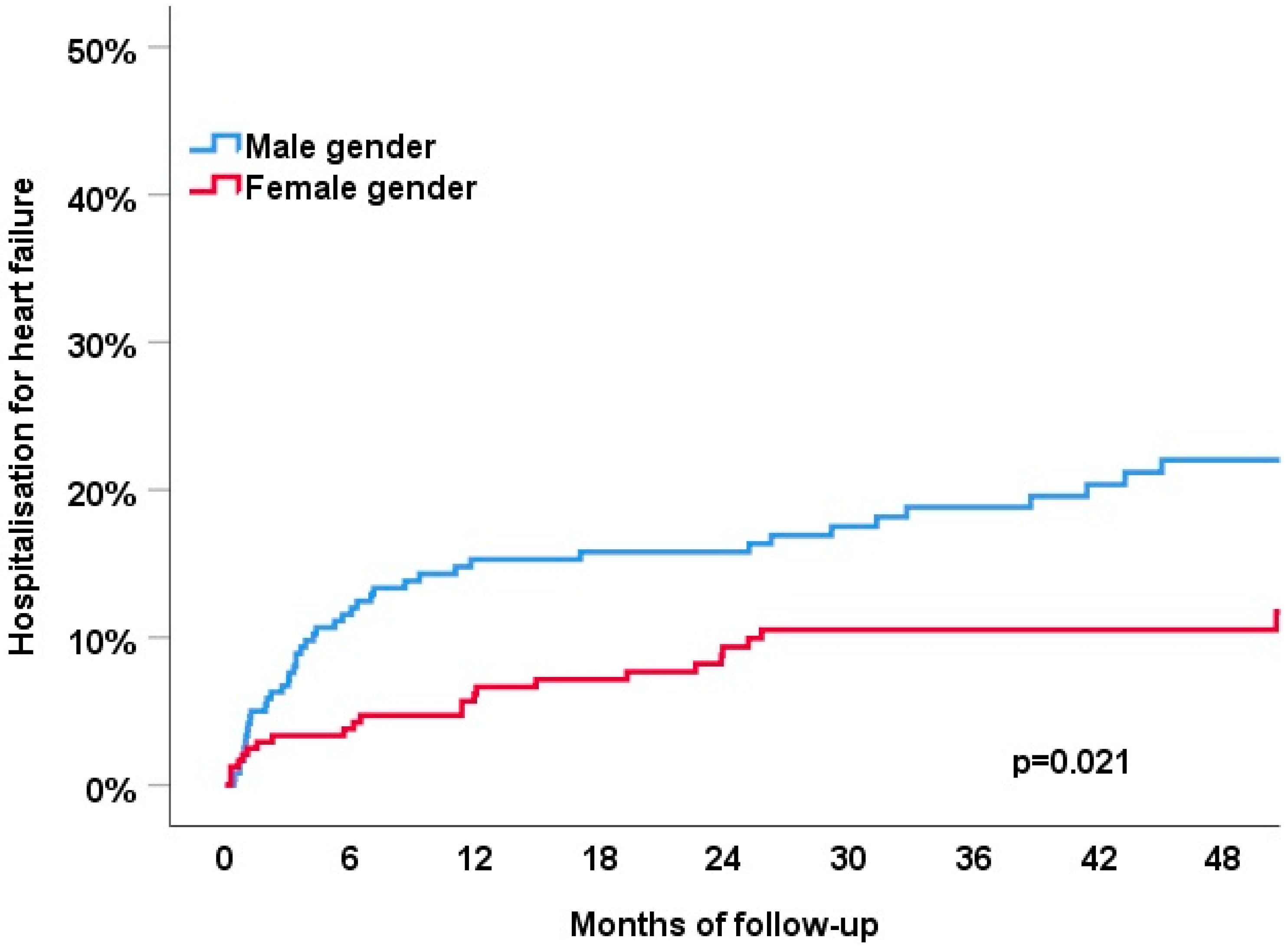
Patients were followed for a median of 42 months in survivors (IQR 22-62). After 4 years of follow-up, the primary endpoint of all-cause death or HF hospitalization had occurred in 32% of patients (Figure 1). The primary endpoint occurred significantly more frequently in men (38% vs. 27%, p = 0.008). The individual components of the primary endpoint showed a similar association with sex category: all-cause death occurred in 25% of the patients and was more common in men compared to women (28% vs. 21%, p = 0.017); HF hospitalizations occurred in 16% of the patients and were also more common in men compared to women (22% vs. 11%, p = 0.021); (Figure 2).
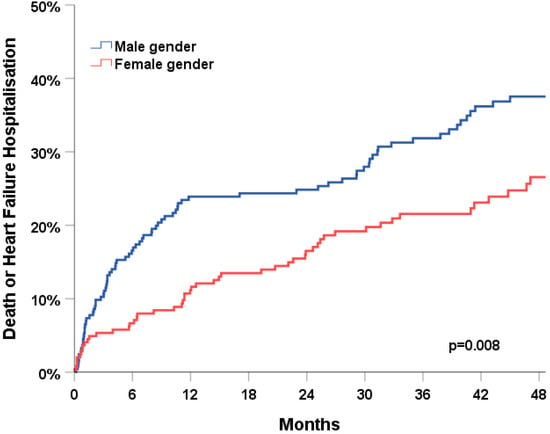
Figure 1.
Association of sex category with the combined clinical endpoint of all-cause death or heart failure hospitalisation during 4 years of follow-up.
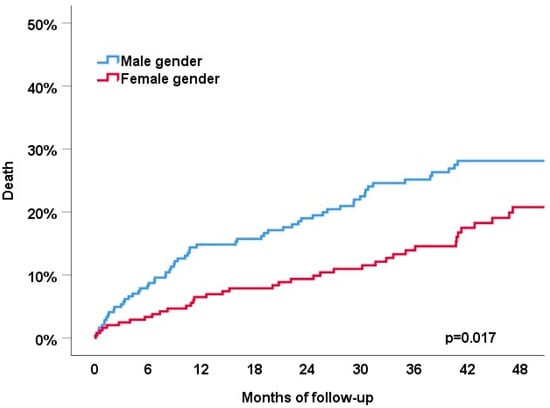
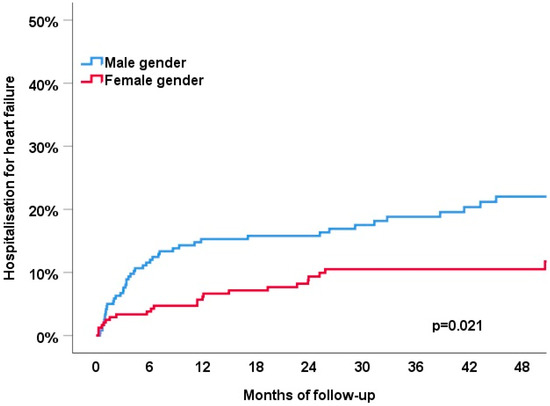
Figure 2.
Association of sex category with the all-cause death (top) and heart failure hospitalization (bottom) during 4 years of follow-up.
Male sex category remained an independent predictor of the combined endpoint of death or HF hospitalization after adjustment for age, LVEF and type of stimulation (HR 1.45 [1.0–2.1], p = 0.047, Table 3).
Table 3.
Univariate and multivariable Cox regression analysis to predict the primary endpoint of death or HF hospitalization.
3.5. Device-Related Re-Interventions
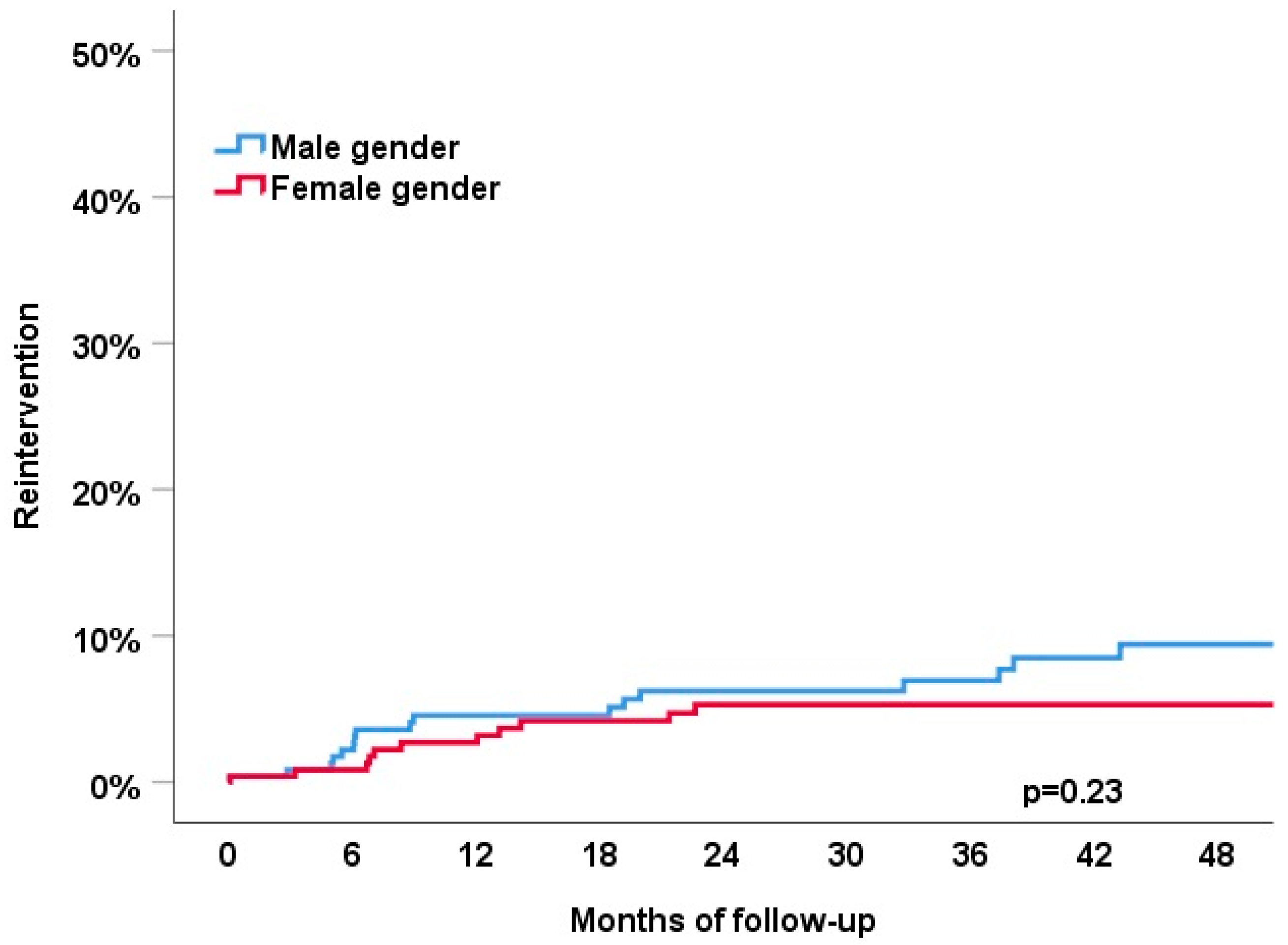
During follow-up, device-related re-interventions occurred in 5.8% of the patients: lead-related complications in 11 patients (2.1%) after a median of 362 days, infections in 1 patient (0.2%) after 1142 days, and upgrade to an ICD or CRT in 18 patients (3.5%) after a median of 238 days (Figure 3). No sex-related differences were observed (all p-values > 0.05).
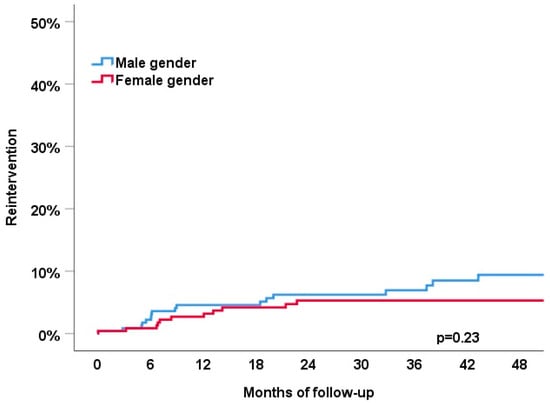
Figure 3.
Association of sex category with the device-related reinterventions (lead failure, infections or upgrade to ICD or CRT) during 4 years of follow-up.
4. Discussion
This study assessed sex- and gender-related differences in patient selection and long-term clinical outcomes in a large multicentre cohort of 513 patients undergoing AV junction ablation as part of a pace and ablate strategy for refractory atrial fibrillation. We report the following major findings:
First, the patient characteristics of men as compared to women chosen for pace and ablate differed significantly in our cohort. Men were younger, had a lower LVEF and a higher burden of comorbidities. Second, no sex and gender differences were observed in the use of pace and ablate as a primary treatment strategy or secondary after a prior failed atrial fibrillation ablation. Third, the primary endpoint of all-cause death or HF hospitalization occurred significantly more frequently in men compared to women during 4 years of follow-up (38% vs. 27%, p = 0.008). The better outcome in women was independent of age, LVEF and mode of stimulation. Fourth, the rate of device-related complications during 4 years of follow-up was 5.8%.
Our findings have clinical implications: In light of the ongoing increase in the worldwide incidence of atrial fibrillation, therapeutic options are necessary for patients in whom rhythm control or adequate rate and symptom control by means of medication and or catheter ablation cannot be achieved. For this patient group, the pace-and-ablate strategy is a well-established, though irreversible treatment option. The recent APAF-CRT trial showed that biventricular pacing and ablation was superior to pharmacological therapy in reducing mortality in patients with permanent AF [9]. In line with large registry data from Sweden [19], the mortality of AF patients in the control arm of APAF-CRT was over 40% after 4 years [9]. Using biventricular pacing and AV junction ablation, mortality could be reduced to 14% in APAF-CRT. The benefit of rate control and rate regularization provided by the pace and ablate strategy was confirmed in our study. The slightly higher mortality of 25% after 4 years observed in our cohort as similar to other studies [20,21] might be explained by two factors. First, the use of biventricular stimulation was only 35% in our cohort, and the non-physiological RV pacing likely has contributed to the higher mortality [22]. Second, the patients in our cohort were, on average, 3 years older compared to the intervention group in APAF-CRT [9].
The rate of device-related early adverse events reported in APAF was 4.8% and consisted of lead dislodgements [9]. However, with only 63 patients in the intervention arm, the study was too small to provide information on the incidence of device-related re-interventions during follow-up. Based on large registry data from Scandinavia, the rate of major complications was already 5.6% after 6 months [11]. Given that device-related complications in pacemaker-dependent patients after AV junction ablation have a significant morbidity and mortality, the finding of only 5.8% device-related reinterventions after 4 years in our study was lower than expected and reassuring [10,11]. Furthermore, the majority of those reinterventions (3.5%) were upgrades without immediate device-related risk for the patients. Nevertheless, optimal implantation techniques (including the use of biventricular pacing or conduction system pacing) and measures to minimize device infections are important for all patients in need of a pacemaker or an ICD, but should particularly be considered for patients planned for a pace-and-ablate strategy [20,23,24].
The body of evidence about sex- and gender-related differences, but also sex- and gender-related bias in medicine and also cardiology is growing [12,13,14,15,16,17]. The relative contributions of sex-related (biology) and gender-related (behaviour) differences to the observed overall differences are often difficult to separate. The classification of patients in our study was based on sex. However, we cannot rule out that the observed differences were also partially affected by gender as well. In a recent study, Mohamed and co-workers reported that women are more frequently selected for CRT-P and men more frequently for CRT-D [16]. In our study, the selection of pace and ablate as a primary or secondary strategy (after failed PVI) did not differ between men and women. However, men significantly more often received biventricular simulation compared to women (53% vs. 17%). Given the significant differences in baseline characteristics, women and men in our study seemed to correspond to two main categories of patients who received a pace and ablate treatment: one category of patients with relatively few comorbidities and intolerable AF symptoms that were more often found in women, and another category of patients with a high burden of comorbidities and low LVEF more commonly found in men. In addition, women seem to be affected by more adverse effects of rate control medication as betablockers, in particular substances that are metabolised via Cyp2D6 [25]. These findings might reflect a sex-related bias in patient selection as well as differences in atrial fibrillation phenotypes in patients with heart failure with reduced ejection fraction and heart failure with preserved ejection fraction. Of important note, male sex category was independently associated with a negative clinical outcome even after adjustment for age, LVEF and type of stimulation. This, to our knowledge, is a new finding and necessitates further investigations.
Conduction system pacing by means of His bundle pacing or left bundle pacing has already remarkably affected the field of ventricular pacing and will do so even more so in the upcoming years. Given the advantages of conduction system pacing such as a shorter QRS width, more favourable LV remodelling compared to CRT [26,27] will likely make this the preferred approach in patients undergoing pace and ablate in the future [28].
5. Limitations
Potential limitations of the present study merit consideration. First, given the significant differences in baseline characteristics, residual confounding cannot be excluded and may have had some impact. Second, given that patient identification occurred via a prospective national ablation registry [18], the risk for introduction of a relevant bias seems low. Third, despite a sample size that was more than eight times larger than that of the intervention group in APAF-CRT, the number of patients with device-related re-interventions was too low to assess for predictors. Fourth, the lead position for RV and LV pacing was based on the implanting physician’s preference and, hence, was heterogeneous within the study sample. Since leads position may clearly impact on outcomes, this might have introduced a small bias.
6. Conclusions
A pace and ablate strategy in patients with refractory atrial fibrillation is safe. Subsequent device-related re-interventions are needed in 5.8% over 4 years. We found significant sex and gender differences in patient selection. Even after adjustment for age, LVEF and type of stimulation, women had a more favourable clinical course after AV junction ablation.
Author Contributions
Conceptualization, T.B., L.R., H.T. and T.R.; Data curation, T.B., M.K.-F., K.M., A.H., S.B. and M.K.; Formal analysis, T.B. and M.K.-F.; Investigation, T.B. and S.O.; Methodology, T.B., B.S., N.K. and T.R.; Project administration, T.B., M.K.-F., B.S., C.S. and T.R.; Resources, F.N., A.H., P.B., S.O., M.K., H.T., C.S. and T.R.; Software, J.S.; Supervision, T.R.; Validation, M.K.-F. and L.R.; Visualization, T.B.; Writing—original draft, T.B., M.K.-F. and T.R.; Writing—review & editing, T.B., M.K.-F., K.M., F.N., B.S., A.H., P.B., S.B., J.S., S.O., M.K., L.R., H.T., C.S., N.K. and T.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The utilized data is available from the corresponding author on request.
Conflicts of Interest
A. Haeberlin: Research grants from the Swiss National Science Foundation, the Swiss Heart Foundation, the University of Bern, the University Hospital Bern, the Velux Foundation, the Hasler Foundation, the Swiss Heart Rhythm Foundation, and the Novartis Research Foundation. He is Co-founder and CEO of Act-Inno, a cardiovascular device testing company. He has received travel fees/educational grants from Medtronic, Philips/Spectranetics and Cairdac without impact on his personal remuneration. F. Noti: Medtronic, Abbott: Travel fees, speaker fees, educational grant; Boston Scientific, Philips Spectranetics: Travel fees, educational grant; Biotronik: Institutional grant all for work outside the submitted study. B. Schaer: speaker’s bureau Medtronic. M. Kühne: personal fees from Bayer, Böhringer Ingelheim, Pfizer BMS, Daiichi Sankyo, Medtronic, Biotronik, Boston Scientific, Johnson & Johnson; research grants from Bayer, Pfizer BMS, Boston Scientific. L. Roten: speaker honoraria from Abbott/SJM and consulting honoraria from Medtronic. Ch. Sticherling: speaker honoraria from Biosense Webster, Boston Scientific and Medtronic and research grants from Biosense Webster, Daiichi-Sankyo, and Medtronic; proctoring for Medtronic (Cryoballoon) T. Reichlin: research grants from the Goldschmidt-Jacobson Foundation, the Swiss National Science Foundation, the Swiss Heart Foundation, the European Union [Eurostars 9799-ALVALE) and the Professor Max Cloëtta Foundation, all for work outside the submitted study. Speaker/consulting honoraria or travel support from Abbott/SJM, Astra Zeneca, Brahms, Bayer, Biosense-Webster, Biotronik, Boston-Scientific, Daiichi Sankyo, Medtronic, Pfizer-BMS and Roche, all for work outside the submitted study. Support for his institution’s fellowship program from Abbott/SJM, Biosense-Webster, Biotronik, Boston-Scientific and Medtronic for work outside the submitted study. All other authors report no conflict of interest related to this paper.
References
- Krijthe, B.P.; Kunst, A.; Benjamin, E.J.; Lip, G.Y.H.; Franco, O.H.; Hofman, A.; Witteman, J.C.M.; Stricker, B.H.; Heeringa, J. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur. Heart J. 2013, 34, 2746–2751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giaccardi, M.; Anselmino, M.; Del Greco, M.; Mascia, G.; Paoletti Perini, A.; Mascia, P.; De Ferrari, G.M.; Picano, E. Radiation awareness in an Italian multispecialist sample assessed with a web-based survey. Acta Cardiol. 2021, 76, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Van Gelder, I.C.; Groenveld, H.F.; Crijns, H.J.; Tuininga, Y.S.; Tijssen, J.G.; Alings, A.M.; Hillege, H.L.; Bergsma-Kadijk, J.A.; Cornel, J.H.; Kamp, O.; et al. Lenient versus strict rate control in patients with atrial fibrillation. N. Engl. J. Med. 2010, 362, 1363–1373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyse, D.G.; Waldo, A.L.; DiMarco, J.P.; Domanski, M.J.; Rosenberg, Y.; Schron, E.B.; Kellen, J.C.; Greene, H.L.; Mickel, M.C.; Dalquist, J.E.; et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N. Engl. J. Med. 2002, 347, 1825–1833. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Pokushalov, E.; Pentimalli, F.; Palmisano, P.; Chieffo, E.; Occhetta, E.; Quartieri, F.; Calo, L.; Ungar, A.; Mont, L.; et al. A randomized controlled trial of atrioventricular junction ablation and cardiac resynchronization therapy in patients with permanent atrial fibrillation and narrow QRS. Eur. Heart J. 2018, 39, 3999–4008. [Google Scholar] [CrossRef]
- Ganesan, A.N.; Brooks, A.G.; Roberts-Thomson, K.C.; Lau, D.H.; Kalman, J.M.; Sanders, P. Role of AV nodal ablation in cardiac resynchronization in patients with coexistent atrial fibrillation and heart failure a systematic review. J. Am. Coll. Cardiol. 2012, 59, 719–726. [Google Scholar] [CrossRef]
- Lim, K.T.; Davis, M.J.; Powell, A.; Arnolda, L.; Moulden, K.; Bulsara, M.; Weerasooriya, R. Ablate and pace strategy for atrial fibrillation: Long-term outcome of AIRCRAFT trial. Eur. Eur. Pacing Arrhythm. Card. Electrophysiol. J. Work. Groups Card. Pacing Arrhythm. Card. Cell. Electrophysiol. Eur. Soc. Cardiol. 2007, 9, 498–505. [Google Scholar] [CrossRef]
- Kay, G.N.; Ellenbogen, K.A.; Giudici, M.; Redfield, M.M.; Jenkins, L.S.; Mianulli, M.; Wilkoff, B. The Ablate and Pace Trial: A prospective study of catheter ablation of the AV conduction system and permanent pacemaker implantation for treatment of atrial fibrillation. APT Investigators. J. Interv. Card. Electrophysiol. Int. J. Arrhythm. Pacing 1998, 2, 121–135. [Google Scholar] [CrossRef]
- Brignole, M.; Pentimalli, F.; Palmisano, P.; Landolina, M.; Quartieri, F.; Occhetta, E.; Calo, L.; Mascia, G.; Mont, L.; Vernooy, K.; et al. AV junction ablation and cardiac resynchronization for patients with permanent atrial fibrillation and narrow QRS: The APAF-CRT mortality trial. Eur. Heart J. 2021, 42, 4731–4739. [Google Scholar] [CrossRef]
- Olsen, T.; Jorgensen, O.D.; Nielsen, J.C.; Thogersen, A.M.; Philbert, B.T.; Johansen, J.B. Incidence of device-related infection in 97 750 patients: Clinical data from the complete Danish device-cohort (1982–2018). Eur. Heart J. 2019, 40, 1862–1869. [Google Scholar] [CrossRef] [Green Version]
- Kirkfeldt, R.E.; Johansen, J.B.; Nohr, E.A.; Jorgensen, O.D.; Nielsen, J.C. Complications after cardiac implantable electronic device implantations: An analysis of a complete, nationwide cohort in Denmark. Eur. Heart J. 2014, 35, 1186–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaiser, D.W.; Fan, J.; Schmitt, S.; Than, C.T.; Ullal, A.J.; Piccini, J.P.; Heidenreich, P.A.; Turakhia, M.P. Gender Differences in Clinical Outcomes after Catheter Ablation of Atrial Fibrillation. JACC Clin. Electrophysiol. 2016, 2, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Sticherling, C.; Arendacka, B.; Svendsen, J.H.; Wijers, S.; Friede, T.; Stockinger, J.; Dommasch, M.; Merkely, B.; Willems, R.; Lubinski, A.; et al. Sex differences in outcomes of primary prevention implantable cardioverter-defibrillator therapy: Combined registry data from eleven European countries. Eur. Eur. Pacing Arrhythm. Card. Electrophysiol. J. Work. Groups Card. Pacing Arrhythm. Card. Cell. Electrophysiol. Eur. Soc. Cardiol. 2018, 20, 963–970. [Google Scholar] [CrossRef]
- Conen, D.; Arendacka, B.; Rover, C.; Bergau, L.; Munoz, P.; Wijers, S.; Sticherling, C.; Zabel, M.; Friede, T. Gender Differences in Appropriate Shocks and Mortality among Patients with Primary Prophylactic Implantable Cardioverter-Defibrillators: Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0162756. [Google Scholar] [CrossRef]
- Van Mieghem, N.M.; Reardon, M.J.; Yakubov, S.J.; Heiser, J.; Merhi, W.; Windecker, S.; Makkar, R.R.; Cheng, W.; Robbins, M.; Fail, P.; et al. Clinical outcomes of TAVI or SAVR in men and women with aortic stenosis at intermediate operative risk: A post hoc analysis of the randomised SURTAVI trial. EuroIntervention J. EuroPCR Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2020, 16, 833–841. [Google Scholar] [CrossRef]
- Mohamed, M.O.; Contractor, T.; Zachariah, D.; van Spall, H.G.C.; Parwani, P.; Minissian, M.B.; Rashid, M.; Martin, G.P.; Barker, D.; Patwala, A.; et al. Sex Disparities in the Choice of Cardiac Resynchronization Therapy Device: An Analysis of Trends, Predictors, and Outcomes. Can. J. Cardiol. 2021, 37, 86–93. [Google Scholar] [CrossRef]
- Tanaka, N.; Inoue, K.; Kobori, A.; Kaitani, K.; Morimoto, T.; Kurotobi, T.; Morishima, I.; Yamaji, H.; Matsui, Y.; Nakazawa, Y.; et al. Sex differences in atrial fibrillation ablation outcomes: Insights from a large-scale multicentre registry. Eur. Eur. Pacing Arrhythm. Card. Electrophysiol. J. Work. Groups Card. Pacing Arrhythm. Card. Cell. Electrophysiol. Eur. Soc. Cardiol. 2020, 22, 1345–1357. [Google Scholar] [CrossRef]
- Molitor, N.; Yalcinkaya, E.; Auricchio, A.; Burri, H.; Delacretaz, E.; Kuhne, M.; Menafoglio, A.; Reek, S.; Reichlin, T.; Herrera-Siklody, C.; et al. Swiss National Registry on Catheter Ablation Procedures: Changing Trends over the Last 20 Years. J. Clin. Med. 2021, 10, 3021. [Google Scholar] [CrossRef]
- Andersson, T.; Magnuson, A.; Bryngelsson, I.L.; Frobert, O.; Henriksson, K.M.; Edvardsson, N.; Poci, D. All-cause mortality in 272,186 patients hospitalized with incident atrial fibrillation 1995–2008: A Swedish nationwide long-term case-control study. Eur. Heart J. 2013, 34, 1061–1067. [Google Scholar] [CrossRef] [Green Version]
- Manuel, A.M.; Almeida, J.; Fonseca, P.; Monteiro, J.; Guerreiro, C.; Barbosa, A.R.; Teixeira, P.; Ribeiro, J.; Santos, E.; Rosas, F.; et al. Long-term outcomes after radiofrequency catheter ablation of the atrioventricular node: The experience of a Portuguese tertiary center. Rev. Port. De Cardiol. 2021, 40, 95–103. [Google Scholar] [CrossRef]
- Su, L.; Cai, M.; Wu, S.; Wang, S.; Xu, T.; Vijayaraman, P.; Huang, W. Long-term performance and risk factors analysis after permanent His-bundle pacing and atrioventricular node ablation in patients with atrial fibrillation and heart failure. Eur. Eur. Pacing Arrhythm. Card. Electrophysiol. J. Work. Groups Card. Pacing Arrhythm. Card. Cell. Electrophysiol. Eur. Soc. Cardiol. 2020, 22, ii19–ii26. [Google Scholar] [CrossRef]
- Stavrakis, S.; Garabelli, P.; Reynolds, D.W. Cardiac resynchronization therapy after atrioventricular junction ablation for symptomatic atrial fibrillation: A meta-analysis. Europace 2012, 14, 1490–1497. [Google Scholar] [CrossRef] [PubMed]
- Burri, H.; Starck, C.; Auricchio, A.; Biffi, M.; Burri, M.; D’Avila, A.; Deharo, J.C.; Glikson, M.; Israel, C.; Lau, C.P.; et al. EHRA expert consensus statement and practical guide on optimal implantation technique for conventional pacemakers and implantable cardioverter-defibrillators: Endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), and the Latin-American Heart Rhythm Society (LAHRS). Europace 2021, 23, 983–1008. [Google Scholar] [CrossRef] [PubMed]
- Tarakji, K.G.; Mittal, S.; Kennergren, C.; Corey, R.; Poole, J.E.; Schloss, E.; Gallastegui, J.; Pickett, R.A.; Evonich, R.; Philippon, F.; et al. Antibacterial Envelope to Prevent Cardiac Implantable Device Infection. N. Engl. J. Med. 2019, 380, 1895–1905. [Google Scholar] [CrossRef]
- Labbe, L.; Sirois, C.; Pilote, S.; Arseneault, M.; Robitaille, N.M.; Turgeon, J.; Hamelin, B.A. Effect of gender, sex hormones, time variables and physiological urinary pH on apparent CYP2D6 activity as assessed by metabolic ratios of marker substrates. Pharmacogenetics 2000, 10, 425–438. [Google Scholar] [CrossRef]
- Arnold, A.D.; Shun-Shin, M.J.; Keene, D.; Howard, J.P.; Sohaib, S.M.A.; Wright, I.J.; Cole, G.D.; Qureshi, N.A.; Lefroy, D.C.; Koa-Wing, M.; et al. His Resynchronization Versus Biventricular Pacing in Patients With Heart Failure and Left Bundle Branch Block. J. Am. Coll. Cardiol. 2018, 72, 3112–3122. [Google Scholar] [CrossRef]
- Vijayaraman, P.; Zalavadia, D.; Haseeb, A.; Dye, C.; Madan, N.; Skeete, J.R.; Vipparthy, S.C.; Young, W.; Ravi, V.; Rajakumar, C.; et al. Clinical outcomes of conduction system pacing compared to biventricular pacing in patients requiring cardiac resynchronization therapy. Heart Rhythm 2022, 19, 1263–1271. [Google Scholar] [CrossRef]
- Vijayaraman, P.; Hashimova, N.; Mathew, A.J.; Subzposh, F.A.; Naperkowski, A. Simultaneous conduction system pacing and atrioventricular node ablation via axillary vs femoral access. Heart Rhythm 2022, 19, 1019–1021. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).